2014.5.20
慈恵
ICU勉強会
麻酔部 レジデント
3年 亀田慎也
Introduc3on
Ø 広範囲の中大脳動脈領域梗塞や半球梗塞は脳浮腫を起こし、
脳ヘルニアからやがて死を迎える。
Ø 悪性中大脳動脈領域梗塞
(
malignant middle-‐cerebral-‐artery infarc3on)
は、
ICUにおける内科的治療を行っても約80%が脳ヘルニア
を起こし、
1週間以内に死亡する。
Ø 内科的治療の有用性に対する十分なEvidenceは存在しない。
Arch Neurol 1984;41:26-‐9.
Arch Neurol 1996;53:309-‐15.
Stroke 1984;15:492-‐6.
Stroke 2007;38:3084-‐94.
Introduc3on
Ø 減圧開頭術+硬膜形成術は浮腫組織の頭蓋外への膨張
を可能にし、致命的な脳の偏位やヘルニアを予防すること
が出来る。
Ø これまでに悪性中大脳動脈領域梗塞に対する減圧開頭術
の有用性に関する前向き研究がなされて来た。
3Lancet Neurol 2009;8:949-‐58.
DEMICAL
Stroke. 2007;38:2506-‐2517.
• 減圧開頭群は死亡率が52.8%低下。有意差あり
• 機能予後は統計学的有意差なし(mRS≦3)
悪性中大脳動脈領域梗塞に対する
早期減圧開頭術の有用性について検討
ランダム化後6時間以内
or 発症30時間以内に施行
Ø フランス, 多施設, 前向き RCT
Ø
18-‐55歳, 24時間以内発症の悪性脳梗塞 38人
Ø 減圧開頭術
+内科的治療群 vs 内科的治療群
Ø
Primary outcome : mRS≦3(発症後6ヶ月)
5
Stroke. 2007;38:2518-‐2525.
• 減圧開頭群は死亡率が有意に低い
• 機能予後はmRS≦3で分けた場合は有意差無し
mRS≦4で分けた場合は有意差有り
悪性中大脳動脈領域梗塞に対する
減圧開頭術の死亡率と機能予後との関係を検討
Ø ドイツ, 多施設, 前向き RCT
Ø
18-‐60歳, 発症12-‐36時間以内の悪性脳梗塞 32人
Ø 減圧開頭術+内科的治療群 vs 内科的治療群
Ø
Primary outcome : 30日死亡率と発症6ヶ月のmRS≦3
• 減圧開頭群は死亡率が有意に低い
• 機能予後は有意差無し
悪性中大脳動脈領域梗塞に対する
発症
4日以内の減圧開頭術の有用性について検討
Ø オランダ, 多施設, 前向き RCT
Ø
18-‐60歳, 発症96時間以内の悪性脳梗塞 64人
Ø 減圧開頭術+内科的治療群 vs 内科的治療群
Ø
Primary outcome : 発症1年後のmRS≦3
Lancet Neurol 2009; 8: 326–33
7
Lancet Neurol 2007; 6: 215–22
Ø
DECIMAL, DESTINY, HAMLET に登録された患者
Ø
18-‐60歳(平均年齢40代) 93人
Ø 多施設, Meta-‐analysis
Ø
Primary outcome:発症1年後のmRS≦4(0-‐4 vs. 5-‐6)
Ø
Secondary outcome:発症1年後のmRS≦3(0-‐3 vs. 4-‐6)
Lancet Neurol 2007; 6: 215–22
• 発症1年後の死亡率:
71% → 22%
•
mRS:5の割合:減圧開頭群 4% vs. 内科的治療群 5%
•
mRS:2-‐3の割合:
減圧開頭群 43% vs. 内科的治療群 21.5%
⇒
減圧開頭群の方が機能予後が良い
Introduc3on
減圧開頭術を受けた
50歳以上のうち
•
Uhlら ⇒ 12%: 比較的機能予後良好
37%:死亡 or 重篤な障害
•
Guptaら⇒80%:死亡 or 重篤な障害
Ø これまでの研究は対象が60歳以下であり、61歳以上の
高齢患者に対しても同様の結果が得られるか不明
Ø 臨床では61歳以上が約50%を占める
J Neurol Neurosurgery Psychiatry 2004;75:270-‐4.
Stroke 2004;35:539-‐43.
Neurosurg Focus 2009;26(6):E3.
Decompressive Surgery for the Treatment of Malignant
InfarcGon of the Middle Cerebral Artery Ⅱ
(
DESTINY Ⅱ
)
Design
Ø 前向き、 無作為、非盲検、多施設、比較試験
Ø 減圧開頭群:内科的治療群≒1:1に割り付け
11• 発症
48時間以内に無作為化
• 治療開始は無作為化
6時間以内に開始
• 減圧開頭群は内科的治療も受けた
Ø ドイツ
13施設
Ø 期間:2009年8月〜2013年3月
Pa3ents
Ø 年齢61歳以上
Ø 発症48時間以内かつ治療開始前で、片側の急性中大
脳動脈領域梗塞の臨床症状を有する患者
Ø
NIHSSが劣位半球で14点以上、優位半球で19点以上
Ø 基底核を含む中大脳動脈領域の3分の2以上の梗塞
<除外項目>
•
mRS>1, Barthel index<95, GCS<6点
•
対光反射
(-‐)
•
梗塞領域の二次性占拠性血腫
(+)
•
他の脳病変、手術禁忌
•
3年以上の寿命が見込めない症例
Treatment
発症
48時間以内かつ無作為化後6時間以内に開始
13Ø
Conserva3ve treatment
(内科的治療)
⇒各参加施設の
ICUで脳卒中に対して行われている治療
Ø
Surgical treatment
⇒減圧開頭術と硬膜形成術
• 浸透圧療法 -‐ マンニトール、グリセロール、高張HES
• 挿管、人工呼吸器管理⇒過換気
• 緩衝液(Trimethamin)
• 鎮静
• 血圧管理
• 血糖管理 etc
挿管の適応:
GCS<8, pO2<60mmHg, pCO2>48mmHg
嚥下・咳嗽反射の低下、上気道閉塞の危険性
• 最低直径12cm
Outcomes & Endpoints
Ø
Primary endpoint:
Ø
Secondary endpoints:
無作為化後
6ヶ月後(±14日)、12ヶ月後(±14日)
•
6ヶ月後のmodified Rankin scale(mRS) 0-‐4の割合
•
12ヶ月生存率
•
NIHSS score
•
mRS
• 日常生活の活動度(Barthel Index)
•
QOL評価(SF-‐36、EQ-‐5D)
• うつ状態の評価(HDRS)
• 有害事象、外科的合併症
• 患者満足度
Sta3s3cal analysis
Ø
Primary endpoint解析:two sided significance level of 5%
Ø 中間解析:Whitehead’s triangular test
Ø 結果:odds比、bias補正95%信頼区間
Ø
Sample size:最大160人、検出力90%
15
Whitehead’s triangular test
(Preliminary analysis set)
⇒
Primary endpoint解析において
有益、有害、無益が明らかである
場合は即刻中止。
Primary endpointでmRS≦4の割合が
減圧開頭群:
31.0%、内科的治療群:8.6%と仮定
(対数
odds比:1.56)
DESTINY II – Supplemental analyses 4
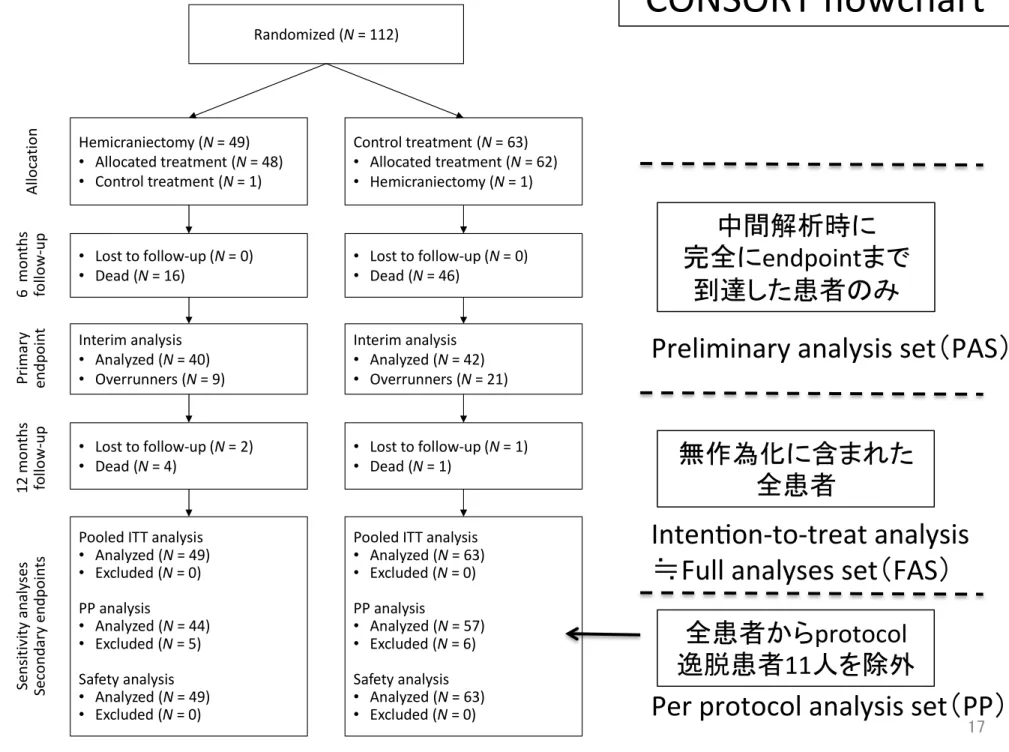
Figure S1. CONSORT flowchart.
Of 112 patients randomized 63 were allocated to receive conservative (control) treatment alone, 49 were allocated to receive additional DH. Of the 63 patients in the control group one patient was treated by DH because of continuous deterioration of consciousness and the decision of the
treating physician to perform DH. One patient in the surgical group did not receive DH because of a revised decision of the relatives after randomization indicating that DH was no treatment option. No patient was lost to follow-up for the primary endpoint analysis after 6 months. For the analyses of the secondary endpoints at 12 months two patients in the DH group and one patient in the control group were lost to follow-up; one patient´s legal representative withdraw consent of further follow-up, two patients refused contact for reasons not given. Five DH patients and six control patients were excluded from the per protocol analysis. Reasons for exclusion were crossover to the other treatment in two patients, one from each treatment group. The other patients were excluded because follow-up visits were substantially outside the time frame (more than 4 weeks for 6 months visit, more than 8 weeks for 12 months visit).
Randomized (N = 112) Hemicraniectomy (N = 49) • Allocated treatment (N = 48) • Control treatment (N = 1) Control treatment (N = 63) • Allocated treatment (N = 62) • Hemicraniectomy (N = 1) Interim analysis • Analyzed (N = 40) • Overrunners (N = 9) Interim analysis • Analyzed (N = 42) • Overrunners (N = 21) • Lost to follow-up (N = 0) • Dead (N = 16) • Lost to follow-up (N = 0) • Dead (N = 46)
Pooled ITT analysis • Analyzed (N = 49) • Excluded (N = 0) PP analysis • Analyzed (N = 44) • Excluded (N = 5) Safety analysis • Analyzed (N = 49) • Excluded (N = 0)
Pooled ITT analysis • Analyzed (N = 63) • Excluded (N = 0) PP analysis • Analyzed (N = 57) • Excluded (N = 6) Safety analysis • Analyzed (N = 63) • Excluded (N = 0) • Lost to follow-up (N = 2) • Dead (N = 4) • Lost to follow-up (N = 1) • Dead (N = 1) A llo ca tio n 6 m o n th s fo llo w -u p Pr im ar y en d p o in t 12 m o n th s fo llo w -u p Se n si ti vi ty a n al ys e s Se co n d ar y e n d p o in ts 17
Preliminary analysis set(PAS)
Inten3on-‐to-‐treat analysis
≒
Full analyses set(FAS)
Per protocol analysis set(PP)
中間解析時に
完全に
endpointまで
到達した患者のみ
無作為化に含まれた
全患者
全患者から
protocol
逸脱患者
11人を除外
CONSORT flowchart
Study pa3ents
2009年9月〜2012年3月の期間
延べ
112人
<内訳>
患者登録は効果安全性評価委員会
の勧告により
Primary endpointの
6ヶ月の時点で
中止
された
⇒
82人
減圧開頭
40人
内科的治療
42人
6ヶ月時点で評価中の患者
⇒
30人
減圧開頭
9人
内科的治療
21人
両群間の患者特性に大きな差無し
Demographic and Clinical Characteris3cs of the Pa3ents at Baseline.DESTINY II – Supplemental analyses 4
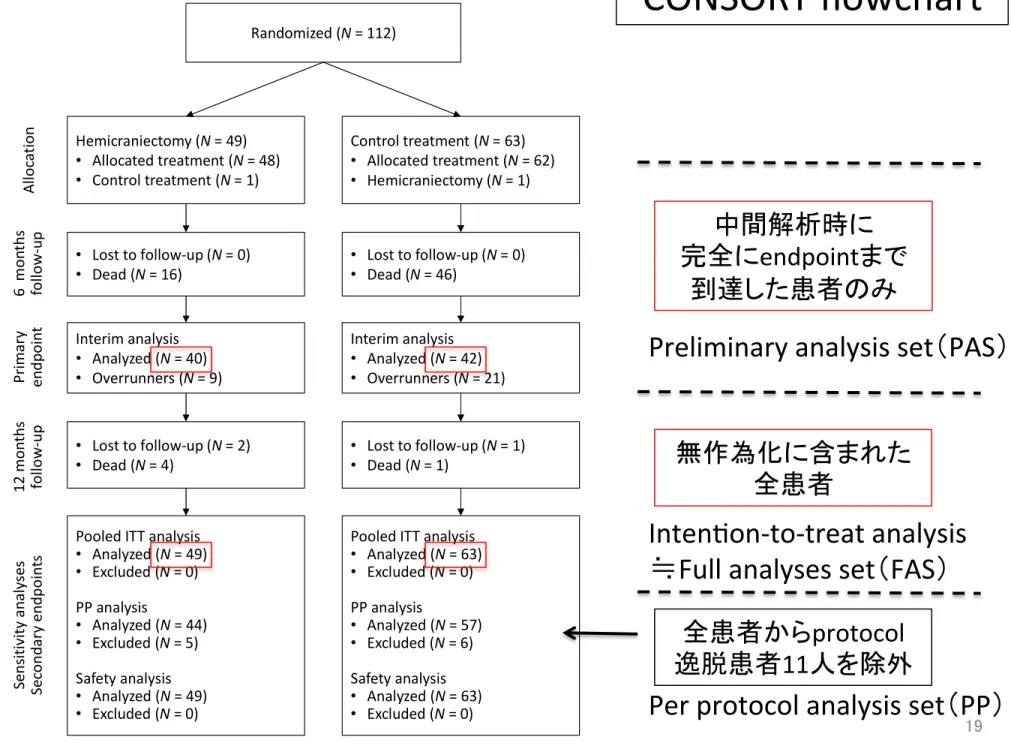
Figure S1. CONSORT flowchart.
Of 112 patients randomized 63 were allocated to receive conservative (control) treatment alone, 49 were allocated to receive additional DH. Of the 63 patients in the control group one patient was treated by DH because of continuous deterioration of consciousness and the decision of the
treating physician to perform DH. One patient in the surgical group did not receive DH because of a revised decision of the relatives after randomization indicating that DH was no treatment option. No patient was lost to follow-up for the primary endpoint analysis after 6 months. For the analyses of the secondary endpoints at 12 months two patients in the DH group and one patient in the control group were lost to follow-up; one patient´s legal representative withdraw consent of further follow-up, two patients refused contact for reasons not given. Five DH patients and six control patients were excluded from the per protocol analysis. Reasons for exclusion were crossover to the other treatment in two patients, one from each treatment group. The other patients were excluded because follow-up visits were substantially outside the time frame (more than 4 weeks for 6 months visit, more than 8 weeks for 12 months visit).
Randomized (N = 112) Hemicraniectomy (N = 49) • Allocated treatment (N = 48) • Control treatment (N = 1) Control treatment (N = 63) • Allocated treatment (N = 62) • Hemicraniectomy (N = 1) Interim analysis • Analyzed (N = 40) • Overrunners (N = 9) Interim analysis • Analyzed (N = 42) • Overrunners (N = 21) • Lost to follow-up (N = 0) • Dead (N = 16) • Lost to follow-up (N = 0) • Dead (N = 46)
Pooled ITT analysis • Analyzed (N = 49) • Excluded (N = 0) PP analysis • Analyzed (N = 44) • Excluded (N = 5) Safety analysis • Analyzed (N = 49) • Excluded (N = 0)
Pooled ITT analysis • Analyzed (N = 63) • Excluded (N = 0) PP analysis • Analyzed (N = 57) • Excluded (N = 6) Safety analysis • Analyzed (N = 63) • Excluded (N = 0) • Lost to follow-up (N = 2) • Dead (N = 4) • Lost to follow-up (N = 1) • Dead (N = 1) A llo ca tio n 6 m o n th s fo llo w -u p Pr im ar y en d p o in t 12 m o n th s fo llo w -u p Se n si ti vi ty a n al ys e s Se co n d ar y e n d p o in ts 19
Preliminary analysis set(PAS)
Inten3on-‐to-‐treat analysis
≒
Full analyses set(FAS)
Per protocol analysis set(PP)
中間解析時に
完全に
endpointまで
到達した患者のみ
無作為化に含まれた
全患者
全患者から
protocol
逸脱患者
11人を除外
CONSORT flowchart
Primary endpoint at 6 months
Full analysis set(FAS)
≒Inten3on-‐to-‐treatにおいて
odds比 2.91
95%CI:1.06-‐7.49
P=0.04
Preliminary analysis set(PAS)
≒中間解析において
odds比 3.97
95%CI:1.39-‐8.76
P =0.01
減圧開頭群の方が重篤な後遺症を残さずに生存できる(
mRS≦4)
DESTINY II – Supplemental analyses 4
Figure S1. CONSORT flowchart.
Of 112 patients randomized 63 were allocated to receive conservative (control) treatment alone, 49 were allocated to receive additional DH. Of the 63 patients in the control group one patient was treated by DH because of continuous deterioration of consciousness and the decision of the
treating physician to perform DH. One patient in the surgical group did not receive DH because of a revised decision of the relatives after randomization indicating that DH was no treatment option. No patient was lost to follow-up for the primary endpoint analysis after 6 months. For the analyses of the secondary endpoints at 12 months two patients in the DH group and one patient in the control group were lost to follow-up; one patient´s legal representative withdraw consent of further follow-up, two patients refused contact for reasons not given. Five DH patients and six control patients were excluded from the per protocol analysis. Reasons for exclusion were crossover to the other treatment in two patients, one from each treatment group. The other patients were excluded because follow-up visits were substantially outside the time frame (more than 4 weeks for 6 months visit, more than 8 weeks for 12 months visit).
Randomized (N = 112) Hemicraniectomy (N = 49) • Allocated treatment (N = 48) • Control treatment (N = 1) Control treatment (N = 63) • Allocated treatment (N = 62) • Hemicraniectomy (N = 1) Interim analysis • Analyzed (N = 40) • Overrunners (N = 9) Interim analysis • Analyzed (N = 42) • Overrunners (N = 21) • Lost to follow-up (N = 0) • Dead (N = 16) • Lost to follow-up (N = 0) • Dead (N = 46)
Pooled ITT analysis • Analyzed (N = 49) • Excluded (N = 0) PP analysis • Analyzed (N = 44) • Excluded (N = 5) Safety analysis • Analyzed (N = 49) • Excluded (N = 0)
Pooled ITT analysis • Analyzed (N = 63) • Excluded (N = 0) PP analysis • Analyzed (N = 57) • Excluded (N = 6) Safety analysis • Analyzed (N = 63) • Excluded (N = 0) • Lost to follow-up (N = 2) • Dead (N = 4) • Lost to follow-up (N = 1) • Dead (N = 1) A llo ca tio n 6 m o n th s fo llo w -u p Pr im ar y en d p o in t 12 m o n th s fo llo w -u p Se n si ti vi ty a n al ys e s Se co n d ar y e n d p o in ts 21
Preliminary analysis set(PAS)
Inten3on-‐to-‐treat analysis
≒
Full analyses set(FAS)
Per protocol analysis set(PP)
中間解析時に
完全に
endpointまで
到達した患者のみ
無作為化に含まれた
全患者
全患者から
protocol
逸脱患者
11人を除外
CONSORT flowchart
Per protocol analysis set
(
sensi3vity analysis)
odds比 3.61
95%CI:1.20-‐9.80
P =0.024
protocolに従って
減圧開頭群
5人と内科的治療群6人を除外
<理由>
• 他の研究に参加している 2人
•
follow-‐upの時期が期間外 9人
Hemicraniectomy in Middle-Cerebral-Artery Stroke
n engl j med 370;12 nejm.org march 20, 2014
1097
(Table S6 in the Supplementary Appendix).
Infec-tions were more frequent in the hemicraniectomy
group. In addition, 23 complications related to
initial hemicraniectomy and bone-flap
reimplan-tation were reported: 5 hemorrhages, 10 cases of
pain requiring pharmacologic treatment, 1
hygro-ma, 1 incident related to anesthesia, and 6
non-specified events, 5 of which were classified as
serious adverse events. The most frequent serious
adverse events in the control group were nervous
system disorders (mainly herniation and brain
edema). Causes of death are listed in Table 3. An
increased rate of early death due to herniation in
the control group was the only major difference
between the two treatment groups.
Discussion
The DESTINY II trial was stopped for reasons of
efficacy after the reductions in deaths and severe
disability at 6 months had become significant.
This treatment effect remained stable after
inclu-sion of all randomly assigned patients and after
12 months of follow-up.
The question of an age limit for
hemicraniec-tomy in patients with malignant
middle-cerebral-artery infarction is controversial among
neurolo-gists and neurosurgeons. The uncertainty about
whether surgery is beneficial in older patients
with stroke, for whom the overall prognosis is
poorer than that for younger patients with stroke,
Hemicraniectomy Group (N=49) Percent Percent Control Group (N=63) Control Group (N=62) 0 7 32 28 33 19 32 6 43 3 15 13 70 5 11 8 76 20 40 60 80 100 0 20 40 60 80 100
Modified Rankin Score
3 4 5 6
Modified Rankin Score
3 4 5 6 Hemicraniectomy Group (N=47)
A
B
6 Months 12 MonthsFigure 1. Functional Outcome after Hemicraniectomy and after Conservative Treatment Alone According to
the Modified Rankin Score.
The primary end point was survival without severe disability, defined as a score of 0 to 4 on the modified Rankin scale (range, 0 to 6, with 0 indicating no symptoms and 6 indicating death). The results shown are the probability estimates for all patients who underwent randomization (the intention-to-treat population). Panel A shows the bias-corrected distribution of scores on the modified Rankin scale at 6 months. Panel B shows the raw distribution of Rankin scores at 12 months.
The New England Journal of Medicine
Downloaded from nejm.org at THE JIKEI UNIVERSITY SCHOOL OF MEDICINE on March 22, 2014. For personal use only. No other uses without permission. Copyright © 2014 Massachusetts Medical Society. All rights reserved.
Hemicraniectomy in Middle-Cerebral-Artery Stroke
n engl j med 370;12 nejm.org march 20, 2014
1097
(Table S6 in the Supplementary Appendix).
Infec-tions were more frequent in the hemicraniectomy
group. In addition, 23 complications related to
initial hemicraniectomy and bone-flap
reimplan-tation were reported: 5 hemorrhages, 10 cases of
pain requiring pharmacologic treatment, 1
hygro-ma, 1 incident related to anesthesia, and 6
non-specified events, 5 of which were classified as
serious adverse events. The most frequent serious
adverse events in the control group were nervous
system disorders (mainly herniation and brain
edema). Causes of death are listed in Table 3. An
increased rate of early death due to herniation in
the control group was the only major difference
between the two treatment groups.
Discussion
The DESTINY II trial was stopped for reasons of
efficacy after the reductions in deaths and severe
disability at 6 months had become significant.
This treatment effect remained stable after
inclu-sion of all randomly assigned patients and after
12 months of follow-up.
The question of an age limit for
hemicraniec-tomy in patients with malignant
middle-cerebral-artery infarction is controversial among
neurolo-gists and neurosurgeons. The uncertainty about
whether surgery is beneficial in older patients
with stroke, for whom the overall prognosis is
poorer than that for younger patients with stroke,
Hemicraniectomy
Group (N=49)
Percent
Percent
Control Group
(N=63)
Control Group
(N=62)
0
7
32
28
33
19
32
6
43
3
15
13
70
5 11
8
76
20
40
60
80
100
0
20
40
60
80
100
Modified Rankin Score
3
4
5
6
Modified Rankin Score
3
4
5
6
Hemicraniectomy
Group (N=47)
A
B
6 Months
12 Months
Figure 1.
Functional Outcome after Hemicraniectomy and after Conservative Treatment Alone According to
the Modified Rankin Score.
The primary end point was survival without severe disability, defined as a score of 0 to 4 on the modified Rankin
scale (range, 0 to 6, with 0 indicating no symptoms and 6 indicating death). The results shown are the probability
estimates for all patients who underwent randomization (the intention-to-treat population). Panel A shows the
bias-corrected distribution of scores on the modified Rankin scale at 6 months. Panel B shows the raw distribution of
Rankin scores at 12 months.
The New England Journal of Medicine
Downloaded from nejm.org at THE JIKEI UNIVERSITY SCHOOL OF MEDICINE on March 22, 2014. For personal use only. No other uses without permission.
Copyright © 2014 Massachusetts Medical Society. All rights reserved.
Primary endpointの機能予後
Ø
mRS:0-‐2 ⇒ 両群共に
0%
Ø
mRS:5 ⇒ 減圧開頭群
28
% vs. 内科的治療群 13%
DESTINY II – Supplemental analyses 10
Figure S6. Survival in the two groups.
Secondary endpoints
12ヶ月生存率(Kaplan-‐Meier)
減圧開頭群
59.0%
(
23/39, 95%CI:42.1 – 74.4%)
内科的治療群
22.0%
(
9/41, 95%CI:10.6 – 37.6%)
減圧開頭群
57.4%
(
27/47, 95%CI:42.2 – 71.7%)
内科的治療群
24.2%
(
15/62, 95%CI:14.2 – 36.7%)
FAS
PAS
内科的治療群で大きく最初に低下するが
T h e ne w e ngl a nd jou r na l o f m e dicine
n engl j med 370;12 nejm.org march 20, 2014
1096
Table 2. Secondary Outcomes at 12 Months.*
Outcome Hemicraniectomy Group (N = 49) Control Group (N = 63) P Value Intention- to-Treat
Population Surviving Patients
no. of patients/total no. (%)
Modified Rankin scale score <0.001 0.73 0–2 0/47 0/62
3 3/47 (6) 3/62 (5) 4 15/47 (32) 7/62 (11) 5 9/47 (19) 5/62 (8) 6 20/47 (43) 47/62 (76)
NIHSS total score <0.001 0.70 17–42 7/22 (32) 3/10 (30)
8–16 14/22 (64) 4/10 (40) 0–7 1/22 (5) 3/10 (30)
Barthel index score 0.002 0.34 60–100 3/27 (11) 5/13 (38) 0–55 24/27 (89) 8/13 (62) SF-36 score† <0.001 0.86 Mental component 51–100 10/25 (40) 6/12 (50) 26–50 14/25 (56) 6/12 (50) 0–25 1/25 (4) 0/12 Physical component <0.001 0.43 26–100 11/25 (44) 5/12 (42) 0–25 14/25 (56) 7/12 (58) Hamilton Depression Rating Scale
score ‡ <0.001 0.97 0–19 18/18 (100) 5/6 (83)
20–52 0/18 1/6 (17)
EQ-5D visual-analogue scale score§ <0.001 0.94 51–100 6/22 (27) 2/10 (20)
26–50 10/22 (45) 5/10 (50) 0–25 6/22 (27) 3/10 (30)
* There were 27 known survivors in the surgery group and 15 known survivors in the control group.
† Both the mental-component and physical-component summary scores of the Medical Outcomes Study 36-Item Short-Form Health Survey (SF-36) range from 0 to 100, with higher scores indicating greater well-being. In this study, no pa-tients had a mental-component summary score higher than 75 and no papa-tients had a physical-component summary score higher than 50.
‡ Scores on the Hamilton Depression Rating Scale range from 0 to 52, with higher scores indicating greater severity of symptoms and scores higher than 19 indicating severe depression.
§ Scores on the EuroQoL Group 5-Dimension Self-Report Questionnaire (EQ-5D) visual-analogue scale range from 0 (worst quality of life) to 100 (best quality of life).
The New England Journal of Medicine
Downloaded from nejm.org at THE JIKEI UNIVERSITY SCHOOL OF MEDICINE on March 22, 2014. For personal use only. No other uses without permission. Copyright © 2014 Massachusetts Medical Society. All rights reserved.