( g,7,3kyo,,W, 2?,,Me9,8,o,il )
A Research Report Supported by Itoe Okamoto Award
GROWTH HORMONE TREATMENT IN
TURNER'S SYNDROME
Kazue TAKANO, Naomi HIZUKA and Kazuo SHIZUME
Department of Medicine, Institute of Clinical Endocrinology Tokyo Women's Medical College
(Received May lst, 1986)
Abstract
Twenty-one patients with Turner's syndrome
were treated with pituitary derived hunian growth
hormone (p-hGH) andlor methionyl human growth
hormome (m-hGH) for 1-2 years. Plasma
non-esterified fatty acid (NEFA) (mean ± SEM)
in-creased significantly from O.52 ± O.06 to 1.30 ±
O.09 mEgA at 4 hrs. after 4 IU of hGH administra-tion (p<O.OOI). Basal plasma somatonedin C (SM-C) levels were within the normal range; however,
they increased significantly at 24 hrs. after three daily injections of 4 IU of hGH (basal, O.92 ± O.14; 24 hrs., 1.39 ± O.16; 48 h, 1.68 ± O.19; 72h, 1.91 ±
O.22 Ulml; p<O.OOI). For the long-term treatment, the patients were given 4-16 IU of hGH for 1-2
years. The height increased 5.5 ± 1.2 and 5.1 ± O.6
cmlyear in the first and the second year of the
treatment, respectively. These values were greater than pretreatment value of 3.6 ± O,8 cm/year
(p<O.OOI). Antibody against hGH was observed in 60% of the patients at the end of 12 months of m-hGH treatment. Otherwise there were.no signifi-cant changes in physical, blood or urine
examina-tions.
These results indicate that hGH treatment is useful for the acceleration of growth velocity in
pa-ients with Turner's syndrome.
Introduction
Turner's syndrome is a genetic disorder with
many physical abnormalities. Short stature is one
of them. For the treatment of short stature, an-abolic steroids, low doses of estrogen andlor hGH have been usedi)'v5). Human GH treatment has not been systematically employed because of the lack
of hGH supply. Recently Raiti6) reported the effec-tiveness of hGH treatment in American patients
with Turner's syndrome.
Since the success of hGH synthesis by recom-binant DNA technology7), several investigators
have reported the properties and biological
activ-ities of methionyl hGH (m-hGH) in man and
animals8)NiS). We previously reported the growth
promoting effects of m-hGH in 62 patients with
pituitary dwarfismi4),is).
In this paper, we investigated the growth re-sponse and antigenicity of m-hGH and p-hGH in pa-tients with Turner's syndrome.
Materials and Methods
Growth hormone preparations:
Pituitary derived human growth hormone
(p-hGH; Crescormon@) and synthetic human growth
hormone (m-hGH, Somatonorm@) were obtained
from KabiVitrum, Stockholm, Sweden. Each vial
contained 4 IU of hGH, 40 mg of glycine and 1 mg of Na-phosphate.
Patients and study design:
Twenty-one patients with Turner's syndrome,
aged 7-13 years, were investigated. Informed con-sent was obtained from each patient and her par-ents, and the experimental protocol was approved by the Human Subjects Investigation Committee of 662
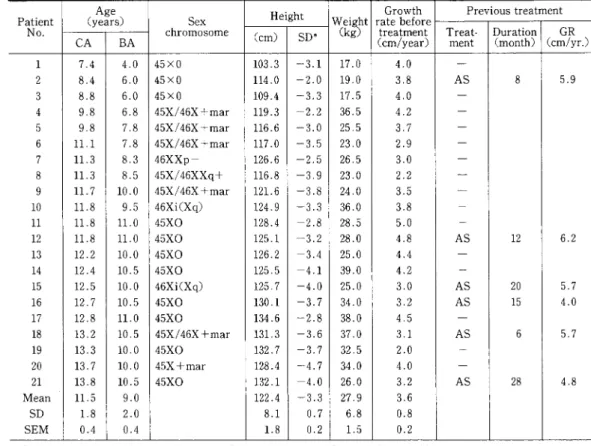
-Table 1 Clinical findings
Age Height Growth Previoustreatment
Patient (years) Sex Weight ratebefore
GR
No.
CA
BA
chromosome (cm) SD* (kg) (cm/year)treatment Treat-ment Duration(month) (cm/yr.)1 7.4 4.0 45×O 103.3 -3.1 17.0 4.0
m
2 8,4 6.0 45×O 114.0 -2.0 19.0 3,8AS
8 5.9 3 8,8 6.0 45×O 109.4 -3.3 17.5 4,O-4 9.8 6.8 45X/46X+mar 119.3 -2.2 36.5 4.2
-5 9.8 7,8 45X/46X+mar 116.6 -3.0 25.5 3.7
-6 11.1 7,8 45X/46X+mar 117.0 -3.5 23,O 2.9
-7 11.3 8,3
46XXp-
126.6 -2.5 26,5 3.0-8 11.3 8.5 45Xf46XXq+ 116.8 -3.9 23,O 2,2 un 9 11.7 10.0 45Xf46X+mar 121.6 -3.8 24,O 3,5
-10 11.8 9.5 46Xi(Xq) 124.9 -3.3 36.0 3.8 -11 11.8 11.0 45XO 128.4 -2.8 28.5 5.0 T
12 11.8 11,O 45XO 125.1 -3.2 28,O 4.8
AS
12 6.213 12.2 10.0 45XO 126.2 -3.4 25,O 4.4
-14 12.4 10.5 45XO 125,5 -4,1 39,O 4.2
-15 12.5 10.0 46Xi(Xq) 125.7 -4.0 25,O 3,O
AS
20 5.716 12.7 10.5 45XO 130.1 -3.7 34.0 3,2
AS
15 4,O17 12.8 11.0 45XO 134.6 -2.8 38.0 4.5
-18 13,2 10.5 45X/46X+mar 131.3 -3.6 37.0 3,1
AS
6 5.719 13,3 10.0 45XO 132.7 -3.7 32.5 2.0 T
20 13,7 10,O
45X+mar
128.4 -4.7 34,O 4.0-21 13.8 10.5 45XO 132.1 -4.0 26,O 3.2
AS
28 4,8Mean 11.5 9.0 122.4 -3.3 27,9 3,6
SD 1.8 2.0 8.1 O.7 6,8 O.8
SEM
O.4 O.4 1.8 O.2 1.5 O,2CA : chronological age, BA : bone age, GR : growth rate, 'SD of Japanese girls of similar age group.
AS: anabolic steroid,
our department. Table 1 gives the individual data for the clinical findings used in this study. The diagnosis of Turner's syndrome was established by sex chromosome analysis. Four patients (Nos. 12,
15, 18 and 21) were under the treatment with
anabolic steroid (stanozolol, 1 mglday). Two
pa-tients (Nos. 2 and 16) had been treated with anabolic steroid previously, but the treatment later
was switched to m-hGH. Three patients (Nos. 5, 7 and 17) were firstly treated with p-hGH for 8-9 months and then switched to m-hGH. Five patients
(Nos. 1, 3, 8, 9 and 10) were treated with p-hGH for 2 years and 6 patients (Nos. 4, 6, 11, 14, 19 and 20)
were treated with m-hGH for one year. One patient (No. 13) had been treated with a previous prepara-tion of m-hGH for 6 months and then the treatment
was switched to the same preparation used others. Glucose (1.75 gfkg BW) was administered to
evaluate glucose metabolism before and one year
after hGH treatment. The acute lipolytic effect of hGH was examined by measuring non-esterified fatty acid (NEFA) before and 4 hrs. after the
injec-tion of m-hGH. The short-term effect of hGH on somatomedin generation was studied by measuring
SM-C by RIA at 24 hrs. after three daily injection
of m-hGH. For the long-term treatment, each pa-tient received 4-16 IU of p-hGH or m-hGH by im or sc injection in 2-4 divided doses per week for 1-2 years.
During the treatment, vital signs, height, body weight were checked regularly by the same phy-sician at the same time of the day. The antibody
against hGH were measured once a month or two
months during the treatment as previously des-cribedi4). Bone age was evaluated before and one
and two years after the treatment according to the
-663-standards of Greulich & Pylei6). Student's t-test
and paired t-test were used for statistical analysis.
Results
Plasma non-esterified fatty acid (NEFA) (mean ±
SEM) increased significantly from O.52 ± O.06 to
1.30 ± O.09 mEqA at 4 hrs. after the first
admin-istration of 4 IU of m-hGH (p<O.OO1). Mean plasma
SM-C levels were O.92 ± O.14, 1.39 ± O.16, 1.68 ± O.19 and 1.91 ± O.22 Ulml at O, 24, 48 and 72 hrs. after the three daily injections of 4 IU of m-hGH. The latter three values were significantly greater than the basal one (p<O.OOI).
The dosages of hGH administered, the changes in body height, bone age and body weight are
shown in Table 2. The height increased between
3.4 and 7.8 cmlyear with a mean of 5.5 ± 1.2
cmlyear during the first year of the treatment. During the second year, the height increased
be-tween 4.3 and 5.6 cmlyear with a mean of 5.1 ± O.6
cm/year. These two mean values were greater than that of pretreatment (p<O.OOI). Bone age did not accelerat during the treatment. There was no rela-tionship between the growth rate on the one hand and the chronological age, bone age, dosages of
hGH administered or sex chromosome pattern on the other.
The antibody against hGH did not appear in pa-tients treated with p-hGH, however, did appear in
those treated with m-hGH. The positive percent
and the titer of hGH antibody in patients treated with m-hGH for one year are shown in Fig. 1 and 2,
together with those in pituitary dwarfs treated with
the same batch of m-hGH for one year. The anti-body appeared 2 months after the treatment in 4 of 15 patients; 8 and 9 patients had antibody after 6
and 12 months of the treatment, respectively. After
12 months of the treatment, the titer of antibody
Table 2 Dose of hGH, growth rate during the treatment, and bone age and body weight before and at the end of the lst and the 2nd year of treatment.
.patlent
hGH
Growthrate (cmlyear) Bone age(year) Bodyweight(kg)No. U/kg/w Before lstyr. 2ndyr. Before lstyr. 2ndyr, Before lstyr, 2ndyr.
1 O,94 4,e 6.3 5,5 4.0 5.5 7,O 17,O 22.0 25,O
2 O.84 3.8 6.0
m
6,O 7.0-
19,O 23.0-3 O,46 4.0 4.1 5,1 6,O
-
9.0 17.5 20.0 22.0 4 O,44 4,2 7.8-
6.8 8.0 rm 36.5 41.0m
5 O,63 3,7 7,O 5.6 7.8 8.5 ne 25.5 28.0-6 O.70 2.9 5,2
-
7.8 8.8-
23.0 27.0-7 O.60 3.0 6.9 5.5 8,3 10.0
-
26.5 30.0T
8 O.52 2.2 4,O 4.5 8.5 9.0 10.0 23.0 25.5 29.09 O.67 3.5 4.5 5.9 10.0 11,O 12.0 24.0 26,O 28,5
10 O.22 3.8 4.5 4.4 9.5 10.0 11,6 36,O 40.0 43.0
11 O.56 5.0 4.9
T
11,O 12,O-
28,5 35,OT
12 O.57 4.8 6.4*
-
11.0 11.0m
28.0 31,O-13 O.64 4.4 6.4 4,3 10.0 10.0 10,O 25.0 27.0 31,5
14 O,41 4.2 5.4
-
10,5 12.0-
39.0 39.5-15 O,64 3,O 5.6*
-
10.0 11.5L
25.0 31,O-16 O,47 3.2 3.7
-
10,5 11.5T
34.0 38,O-17 O.42 4.5 6.5
-
11.0 11.0-
38.0 38,5+
18 O.43 3.1 6.0*
-
10,5 11.0-
37.0 41.0-I9 O.49 2.0 4.3
r
10,O 10,5-
32.5 32.5-20 O.47 4.0 3.4 rm 10,O 10.5
-
34,O 34.5N
21 O.62 3.2 5.5*
u
10.5 11,O-
26.0 31.5-Mean O.56 3.6 5,5 5.1 9.1 10.0 9.9 27.9 31.5 29.8
SD O.16 O.8 1,2 O.6 2.0
L7
1,8 6.8 6,5 7.2SEM
O.03 O.2 O,3 O.2 O.4 O.4 O.7 1.5 1,4 3.0'combination therapy of hGH and stanozolol
-x $ 1OO
5 so
8
ts 608 4o
!
< 20
=
2o
PIT.DWARF(N=21) TURNER' S SYNDROME ( N=15 ) E vF
sl
O2468 10 12
MONTHS OF m-hGH TREATMENT
Fig. 1 hGH antibody appearance in Turner's syndrome
and in pituitary dwarfs by Somatonorm treatrnent,
140 TURNER'S SYNDROME ( N=15 )
O 20 40 60 80 100
130 120 PIT.DWARFS ( N=21 ) 110E
oL"
H,M, BA: 9 m-hGH 4 v/w n lo3 < lo2 S lolsO
-10 10.5 1 1.0 %(-) [ ]
lo gas]
1 o2 e.1 o' .:. :.:. 1 o` ..1 o5Fig. 2 Titer of hGH antibody at 12 month treatment of Somatonorm in patients with Turner's syndrome and in
pituitary dwarfs.
was 10 (No. 4) in one patient; in 4 (Nos. 13, 14, 16 and 20) it was 102; in 3 (Nos. 5, 11 and 12) it was 10s; and in one (No. 15) 104. Thus the titers of
anti-hGH antibody varied between 10 and 104,
Before and during the treatment with hGH, no
remarkable changes in glucose metabolism, blood
count, urinalysis or routine blood chemistries were noted.
Discussion
We have investigated the effect of hGH on
growth in 21 patients with Turner's syndrome for
one and two years. Since the m-hGH and p-hGH
have the same growth promoting effect in patients with hGH deficiency, the effect of both hGH pre-parations combined together in this study.
Four-teen patients showed accelerated growth from a
pretreatment height velocity of 3.5 ± O.9 (SD) to
6.0 ± 1.0 (SD) cmtyear during the first year of the
treatment. One patient (No. 13) had been treated with a previous batch of m-hGH (No. 82412) and her height increased 7.0 cmlyear (Fig. 3). Even
10 11 12 13
AGE,YEARS
Fig. 3 Effects of m-hGH on height increase and the
duction of anti-hGH antibody in a patient (No, 13) with Turner's syndrome, At the age of 12.2 ('), the m-hGH
paration was changed from batch No. 82412 to 81000,
ECP contents in these batches were 220 and 3 ng per vial, respectively.
though she had already antibody against hGH at the beginning of the new batch (No. 81000), her height increased 3.4 cm during 6 months, which corresponded to 6.8 cmlyear. A low dose of anab-olic steroid together with m-hGH seemed to
im-prove the effect on growth increase. Four patients had growth increases of 6.4, 5.6, 6.0 and 5.5 cm/year when m-hGH was given together with a
low dose of anabolic steroid. These values were
similar to those of 6.2, 5.7, 5.7 and 4.8 cmlyear,
re-spectively, obtained during previous treatment
with anabolic steroid alone. Bone age did not accel-erate in these patients during the treatment.
There are only few reports on the effects of hGH in Turner's syndome. Almqvist et al.i) reported short-term effects of hGH in metabolic balance studies on 3 such patients and observed that
phy-siological doses of hGH (40-120 "giCkg body
weight) produced anabolic responses in these
pa-tients, Hutchings et al.2) and Tanner et al.S) treated 2 and 5 patients with Turner's syndrome for 4 months and 1 year, respectively, and observed
mean height increases from 3.2 to 6.8 cmlyear and
2.9 to 3.9 cmlyear, respectively. Stahnkes) treated
8 patients with XO sex chromosomes with hGH at a dose of 12 IU!week for 6 months. Their mean pre-treatment growth rate was 2.56 ± O.34 cmlyear;
during the treatment, 2 of them showed increased
growth rates of around 6 to 8 cmlYear. These 2 pa-tients were younger ones. The rest of the papa-tients had a growth rate of 2.2 ± O.53 cmlyear. Raiti6) re-ported the treatment with pituitary hGH (O.6
U/kglweek) in 57 patients with Turner's syndrome for 6 and 12 months. Thirty-five patients were
treated for 6 months and their height increased by 3.31 cm, which corresponded to 6.62 cmlyear.
Twenty-two patients were treated for 12 months and their height increased by 5.89 cmlyear. These
two values were greater than the pretreatment value of 3.18 cmlyear. The mechanism of the effect of hGH treatment is not clear at this moment. How-ever, it is partly based on a mechanism similar to that of gigantism in prepubertal children with
GH-producing tumours.
The antigenicity of m-hGH was previously
re-portedi4)・i5). The cause of this antigenicity was con-sidered mostly to be a minute amount of E. coli pro-tein (ECP). The m-hGH used in this study
con-tained very small amounts of ECP; 3 nglvial (Dr. Fryklund at KabiVitrum AB, personal
communica-tion). However, in 9 of 15 patients (60CIJb), antibody
against hGH was appeared after 12 months of
treatment. The incidence is greater than that for pituitary dwarfism treated with pituitary GH (5-20C)6), but similar to that observed in pituitary dwarfism treated with the same batch of m-hGHis). The mean height increase in 8 patients with
anti-body titers of more than 102 was 5.4 ± O,5 cmlyear, which did not differ from that in 13 patients, 5.5 ±
O.3 cmlyear, with titers less than 10. Thus, the antibody against hGH seems to have no effect on
growth during the treatment.
These data indicate that hGH treatment is useful for the acceleration of growth velocity in patients
with Turner's syndrome. However, long-term
follow up studies are necessary to conclude the
effect of m-hGH and antibody against hGH on
growth response.
Acknowledgements
This study was partly supported by grants from
the Foundation for Growth Science and Itoe
Okamoto'award. The authors appreciate the supply
of m-hGH from KabiVitrum AB
Sweden.
in Stockholm,
References
1) Almqvist, S., Hall, K., Lindstedt, S., sten, J., Luft, R. and Sj6berg, H.; Effects of
short-term administration of physiological doses of human growth hormome in three patinets with
Turner's syndrome. Acta Endocrinol (Copenh) 46
451--464 (1964)
2) Hutchings, J., Escamilla, R., Li C. and
sham, P.: Li human growth hormone administration in gonadal dysgenesis. Amer J Dis Child 109 318'"321 (1965)
3) Tanner, J., Whitehouse, R., Hughes, P. and Vince, F.: Effect of human growth hormone ment for 1 to 7 years on growth of 100 children with
growth hormone deficiency, low birthweight,
herited smallness, Turner's syndrome and other plaints. Arch Dis Child 46 745-782 (1971)
4) Ross, J., Cassorla, F., Skerda, M., Valk, I., Loriaux, D. and Cutler, G.: A preliminary study
of the effect of estrogen dose on growth in Turner's syndrome. New Engl J Med 309 1104-- 1106 (1983)
5) Stahnke, N.: Human growth hormone treatment in
short children without growth hormone deficiency. New Engl J Med 3 10 925--926 (1984)
6) Raiti, S.: The committee on growth horrnone; Growth-stimulating effects of human growth mone therapy in Turner's Syndrome: in ``Human
Growth Hormone'' edited by S. Raiti and A. Tolman, Plenum Med. Book Co. New York p. 109-113 (1986)
7) Goeddel, D.V., Heyneker, H.L., Hozumi, T., Arentzen, R., Itakura, K., Yansura, D.G.,
Ross, M.J., Miozzari, G., Crea, R. and
Seeburg, P.H.: Direct expression in Escherichia
coli of a DNA sequence coding for human growth mone. Nature 281 544--548 (1979)
8) Olson, K.C., Fenno, J., Lin, N., Harkins, R.N., Snider, C., Kohr, W.H., Ross, M.J.,
Fodge, D., Prender, G. and Stebbing, N.:
Purified human growth hormone from E. coli is
biologicaly active. Nature 293 408--411 (1981)
9) Hizuka, N., Hendricks, C.M., Pavlakis, G.N.,
Hamer, D.H. and Gorden, P.: Properties of human growth hormone polypeptides: purified from pituitary extracts and synthesized in monkey kidney
cells and bacteria. J CIin Endocrinol Metab 55
545--550 (1982)
10) Rosenfeld, R.G., Aggarwal, B.B., Hints, R.L. and Dollar, L.A.: Recombinant DNA-derived
ionyl human growth hormone is similar in membrane binding properties to human pituitary growth
mone. Biochem Biophys Res Commun 106202−209 (1982a)
11)Rosenfeld, R.G., Wilson, D.M., Donar, LA.,
Bennett, A. and Hints, R.L:Both human
pituitary growth hormone and recombinant DNA− derived human growth hormone cause insulin resis−
tance at a postreceptor site. J CIin Endocrinol Metab
1033∼1038(1982b)
12)Frigeri, LG., Robel, G. and Stebbing, N.= Bacteria−derived human growth hormone lackes lipo−
1ytic activity in rat adipose tissue. Biochem Biophys
Res Commun 1041041−1046(1982)
13)Hintz, R.L, Rosenfeld, R.G., Wilson, D.M.,
Bennett, A., Finno, J., McClellan, B. and Swift, R.:Biosyn亡hetic methionyl hyman grow亡h
hormone is biologically active in adult man. Lance l
1276−1279(1982)
14)Takano, K., Shizume, K., Hizuka, N.,Hibi,1.,
Kato, K., Kohno, H., Kondo, T., Ogawa, M., Okada, Y., Sudo, M., Suwa, S. and Takahara,
J.:Treatment of idiopathic pituitary dwarfism with methionyl hurnan growth hormone. Endocrinol Japon
30523−527(1983)
15)Takano, K.,Shizume, K., Hizuka, N.,Okuno, A.,Umino, T., Kobayashi, Y., Kusano, S.,
Nakalima, H., Irie, M., Hibi,1., Kato, K.,
Suwa, S., Koshimizu, T., Ogawa, M., Sudo, M.,Imura, H., Okada, Y., Kondo, T., Hashimoto, K., Miyao, M., Kohno, H., Iwatani, N. and Ono, S.:Treatment of pituitary dwarfism with methiQnyl human growth hormone in Japan. Endocrinol Jpn, submitted,1986
16)Greulich, W.W. and Pyle,1.S.:Radiographic Atlas of Skeletal Development of the Hand and Wrist,2ed. Stanford University Press, Stanford (1959) ターナー症候群へのヒト成長ホルモン治療の試み 東京女子医科大学 内分泌疾患総合医療センター内科 三月ノ カ ズ エ ヒヅカ ナオミ シズメ カズオ