Contribution of systemic inflammation and
nutritional status to the relationship between
tooth loss and mortality in a
community-dwelling older Japanese population:
a mediation analysis of data from the
Tsurugaya project
著者
Takako Hiratsuka, Takamasa Komiyama, Takashi
Ohi, Fumiya Tanji, Yasutake Tomata, Ichiro
Tsuji, Makoto Watanabe, Yoshinori Hattori
journal or
publication title
Clinical Oral Investigations volume
volume
24
page range
2071-2077
year
2019-09-04
URL
http://hdl.handle.net/10097/00129146
Relationship between status of dentition and incident functional disability in an elderly Japanese population: prospective cohort study of the Tsurugaya Project
Takamasa Komiyama, DDS, PhD1, Takashi Ohi, DDS, PhD1 , 2, Yoshitada
Miyoshi, DDS, PhD1, Takahisa Murakami, DDS, PhD3, Akito Tsuboi,
DDS, PhD4, Yasutake Tomata, PhD5, Ichiro Tsuji, MD, PhD5, Makoto
Watanabe, DDS, PhD6, Yoshinori Hattori, DDS, PhD1
1Division of Aging and Geriatric Dentistry, Department of Oral
Function and Morphology, Tohoku University Graduate School of Dentistry, Sendai, Japan
2Japanese Red Cross Ishinomaki Hospital, Ishinomaki, Japan
3Division of Public Health, Hygiene and Epidemiology, Faculty of
Medicine, Tohoku Medical and Pharmaceutical University, Sendai, Japan
4Department of Community Medical Supports, Tohoku Medical
Megabank Organization, Tohoku University, Sendai, Japan
5Division of Epidemiology, Department of Health Informatics and
Public Health, Tohoku University School of Public Health, Graduate School of Medicine, Sendai, Japan.
6Department of Social Welfare, Faculty of General Welfare, Tohoku
Fukushi University, Sendai, Japan
Takamasa Komiyama: Department of Aging and Geriatric Dentistry, Tohoku University Graduate School of Dentistry, 4-1Seiryo-machi,
Aoba-ku, Sendai, Miyagi 980-8575, Japan. Phone number: 81-22-717-8396, Fax number: 81-22-717-8396. E-mail address: [email protected]
Short title:
Relationship between status of dentition and incident functional disability
Keywords: Prospective cohort study; Dental status; Elderly; Incident
ABSTRACT
Purpose: The purpose of this study was to examine whether the status
of dentition is associated with incident functional disability in elderly people.
Methods: This prospective cohort study targeted community-dwelling
Japanese adults of age ≥ 70 years (N = 838). Participants were classified into the following four groups in accordance with Miyachi’s Triangular Classification, which represents the status of dentition on the basis of numbers of remaining teeth and occlusal supports: Zone A, ≥ 10 occlusal supports; Zone B, 5–9 occlusal supports; Zone D, ≤ 4 occlusal supports and ≥ 11 remaining teeth and Zone C, ≤ 10 remaining teeth. Incident functional disability was defined by the first certification of long-term care insurance in Japan. Data regarding age, sex, body mass index, medical history, smoking, alcohol consumption, education, depressive symptoms, cognitive impairment, social support, history of fall, and subjective masticatory ability were collected.
Results: During follow-up for 5,185 person-years, 305 participants
experienced functional disability. Considering the follow-up data of ≥ 3 years from baseline, participants in Zones C (hazard ratio [HR], 1.98; 95% confidence interval [CI], 1.26–3.11) and D (HR, 2.50; 95%CI, 1.54–4.01) were found to be more likely to develop functional disability than those in Zone A (P for trend = 0.002).
Conclusions: Status of dentition was associated with incident
this study suggest that maintenance of remaining teeth and retention of occlusal supports contribute to the prevention of functional disability.
1. Introduction
In Japan, life expectancy has continued to increase in common with other industrialized countries, with Japan having the longest life expectancy in the world. However, in Japan, the difference between life expectancy and healthy life expectancy—which is defined by non-deterioration of living functions—is approximately 8.8 years [1]. It is necessary to prevent disease onset and deterioration of living functions and make health recommendations to enable elderly people to live independent and healthy lives.
A growing number of epidemiological studies have shown that tooth loss is related to cerebrovascular diseases [2–6], cognitive impairment [7–10], falls [11], and depressive symptoms [12], which are all major causes of functional disability among elderly Japanese [13]. Furthermore, several studies have demonstrated the association of tooth loss with future onset of functional disability [14–16]. It is possible that decline in masticatory ability due to tooth loss plays an important role in incident functional disability. On the other hand, some studies have shown that dentition status—including occlusal support and difficulty of prosthodontic care, which cannot be expressed solely on the basis of number of teeth—is associated with decrease in masticatory ability [17, 18]. Therefore, we hypothesized that if difficulty of prosthodontic care varied depending on the dentition status, it would appear as a difference in the recovery of masticatory ability, and the risk of functional disability by means of frailty and disease brought about by poor nutrition.
Miyachi’s Triangular Classification [19] is widely used for evaluation of dentition status in prosthodontic clinical settings [18]. This classification was adopted as a part of a multi-axis assessment protocol for determining treatment difficulty in prosthodontic care, which was recommended by the Japan Prosthodontic Society [20]. The concept of this classification is to categorize patients requiring prosthodontic care into four categories according to degree of difficulty on the basis of number of remaining teeth and occlusal support. This classification also shows that restoration of the effect of masticatory ability by prosthodontic treatment differs according to category of the partially edentulous arch [19].
In the present study, we aimed to determine whether the status of dentition evaluated using Miyachi’s Triangular Classification was associated with incident functional disability in an 8-year prospective cohort study involving a community-dwelling elderly population.
2. Methods
2.1. Study population
This study was conducted as a part of the Tsurugaya Project, a comprehensive geriatric assessment (CGA) process involving the measurement of physical, mental, and social functions among community-dwelling elderly people in Tsurugaya district, a suburban area of Sendai in northern Japan [21, 22]. Clinical dental examination and an oral-health questionnaire survey were also conducted as components of the CGA process [23].
The flow diagram of this study is shown in Fig. 1. The study design and complete details of this project have been described elsewhere [21–23]. Briefly, all 2,925 inhabitants of age ≥ 70 years as of March 2003 were invited to participate in a health survey. Among these residents, 948 (32.4%) participated in the baseline survey conducted in July 2003, and 924 of these respondents agreed to participate in this study. In the follow-up survey, 79 participants who had already been certified by long-term care insurance (LTCI) and 7 further participants with missing oral health data were excluded. Consequently, the final analysis included 838 participants. The study protocol was approved by the institutional review board of Tohoku University Graduate School of Medicine.
2.2. Oral examination
Oral examination was performed by five trained dentists who had received sufficient calibration. They determined the numbers of remaining teeth and occlusal supports [23]. Residual root teeth were excluded from the total number of remaining teeth. Subjective masticatory ability was evaluated using the masticatory index scale [23], which inquires of the participants whether they can chew 10 types of food (fish, rice, fish sticks, fish paste, arum root paste, chicken, apples, Chinese cabbage, rice crackers, and peanuts). Participants were accordingly categorized as those who could masticate all these foods and those who had difficulty masticating one or more of the foods.
2.3. Classification of status of dentition
Status of dentition was evaluated in accordance with Miyachi’s Triangular Classification (Fig. 2), which is based on the number of teeth and occlusal supports present [18, 20]. The number of remaining teeth was defined as the total number of teeth remaining in the oral cavity, excluding third molars and residual root teeth. With regard to occlusal supports, the presence of a pair of the same type of teeth—excluding third molars and residual root teeth—in the maxillary and mandibular jaws on the ipsilateral side was considered to account for one occlusal support; the total number of such pairs was counted to determine the number of occlusal supports. Participants were categorized into four categories of dentition status on the basis of numbers of remaining teeth and occlusal supports as follows: Zone A, ≥ 10 occlusal supports; Zone B, 5–9 occlusal supports; Zone C, ≤ 10 remaining teeth; and Zone D, ≤ 4 occlusal supports and ≥ 11 remaining teeth.
2.4. Other measurements
Participants were administered a questionnaire, which included questions on medical history (stroke, myocardial infarction, and hypertension), smoking status, alcohol consumption, duration of education, and a history of falls occurring within the previous 6 months. Body mass index (BMI) was calculated as the ratio of weight (in kg) and height (in m2). Depressive symptoms were measured using the
Japanese version of the 30-item Geriatric Depression Scale [24], with scores ≥ 11 indicating depressive symptoms. Cognitive function was
evaluated on the basis of Mini-Mental State Examination (MMSE) scores [25], with MMSE scores ≥ 26 indicating normal cognition and scores < 26 indicating slight cognitive impairment [22]. Physical function was assessed using the Timed-Up-and-Go test [26], which measures the time (in s) taken for subjects to rise from a standard arm chair, walk 3 m, turn around, walk back to the chair, and sit down; participants were categorized into quartiles on the basis of their scores in this test. The following questions assessed the levels of social support available to participants: Do you have someone (1) with whom you can consult when you are in trouble? (2) with whom you can consult when your physical condition is poor? (3) who can help with your daily housework? (4) who can take you to a hospital when your physical condition is not good? and (5) who can take care of you when you are ill in bed? On the basis of their responses, participants were classified as having restricted (responding no to at least one question) or unrestricted (responding yes to all questions) social support [22].
2.5. Follow-up and outcome
The primary outcome of this study was onset of functional disability, which was defined by the first certification of LTCI. This criterion has been used in previous epidemiological studies [15, 27, 28] and is considered as an index of healthy life expectancy in Japan. Every citizen of age ≥ 40 years pays insurance premiums, and every person of age ≥ 65 years is eligible to receive formal caregiving service. Eligibility for LTCI certification is adjudged upon application from elderly individuals
or their caregivers and is determined by (i) on-site assessment of the current physical and mental status of individuals and their utilization of medical procedures, using a standardized questionnaire developed by the Ministry of Health, Labour and Welfare, followed by computerized analysis and (ii) a subsequent needs-assessment performed by a Municipal Certification Committee comprising physicians, nurses, and other experts in health and social services, who are appointed by the local mayor [29].
Information on LTCI (including care level and dates of relocation from Sendai city and death) was obtained from the Sendai Municipal Authority. The observation period was from the time of baseline survey in 2003 until either the date of approval for LCTI certification or June 30, 2011. Cases were censored if the participants had relocated from Sendai or died.
2.6. Statistical analysis
Baseline characteristics of the study participants were evaluated in accordance with dentition status, using the Wilcoxon rank-sum test for continuous variables and Fisher ’s exact test for categorical variables. Kaplan–Meier survival analysis and the log-rank test evaluated the cumulative incidences of functional disability according to dentition status. Cox proportional hazards models were used to calculate hazard ratios (HRs) and 95% confidence intervals (CIs) for the onset of functional disability.
The statistical models were developed as follows. First, a univariate model was created (Model 1). Second, because age and sex were significant confounders the relationship of oral health status and incident functional disability in previous studies [15, 16], age and sex were added to Model 1 (Model 2). In the final model, BMI, medical history (hypertension, stroke, myocardial infarction, and joint diseases), smoking status (never, former, or current), alcohol consumption (never, former, or current), extent of formal education (< 18 or ≥ 18 years), depressive symptoms (Geriatric Depression Scale score < 11 or ≥ 11), cognitive impairment (MMSE score < 26 or ≥ 26), physical function (timed “Up-and-go” test score quartile), social support, history of fall within the previous 6 months, and subjective masticatory ability (which were all conceivable confounders) were added to Model 2 (Model 3).
The proportional hazards assumption for the models was checked by describing log-minus-log-transformed Kaplan–Meier curves of incident functional disability on the basis of dentition status [30]. Visual inspection of this graphical depiction suggested the follow-up period be divided into two time intervals (< 3 and ≥ 3 years after baseline survey), and two different HRs were obtained.
All data analyses were performed using SPSS software ver. 21.0 for Windows (IBM SPSS Japan, Tokyo, Japan). For all tests, P values < 0.05 were considered to indicate statistical significance. Categorical variables that included missing data were recorded by reassigning missing values into separate “missing” categories to maximize the
number of participants included in the analysis and thereby maximize statistical power.
3. Results
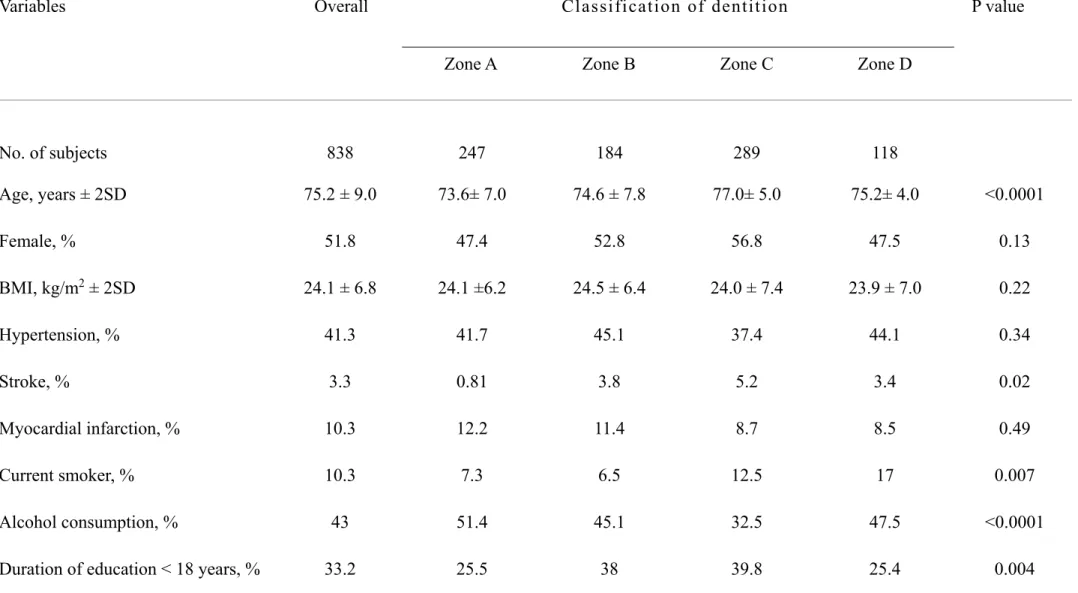
Table 1 presents the baseline characteristics of the study participants according to dentition status. The numbers of participants assigned to Zones A–D were 247 (29.5%), 184 (22.0%), 184 (14.1%), and 289 (34.5%), respectively. Age, history of stroke, smoking status, alcohol consumption, extent of education, physical function, history of falls occurring within the previous 6 months, and subjective masticatory ability were all significantly associated with status of dentition.
Over a follow-up period of 5,185 person-years (median, 7.8 years per participant; interquartile range, 4.8–7.9 years), 65 participants had died, and 29 had relocated from Sendai. Incident functional disability was identified in 305 participants (36.4%) on the basis of first certification of LTCI. Fig. 3 presents the Kaplan–Meier survival curves for cumulative incidence of functional disability. Cumulative incidences of functional disability among participants in Zones A–D were 21.6%, 34.9%, 51.2 %, and 47.6%, respectively. There were significant differences in rate of functional disability among the four states of dentition (log-rank test, P < 0.001).
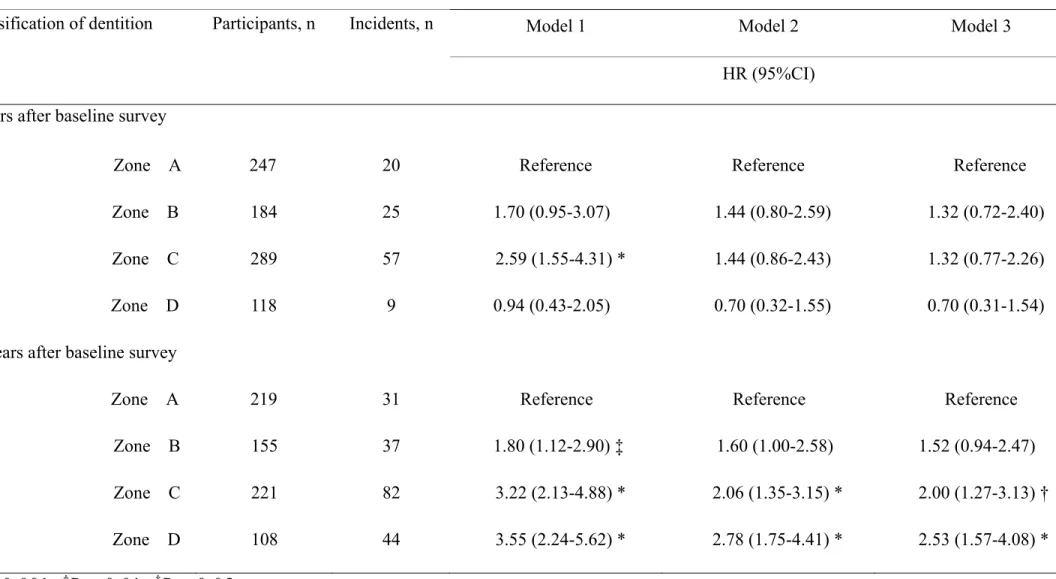
Table 2 presents the relationship between the status of dentition and incident functional disability determined by time-dependent Cox proportional hazard analysis. Considering data recorded within 3 years of the baseline survey, in the crude model (model 1; Table 2),
participants in Zone D exhibited a significantly higher risk of functional disability than those in Zone A. However, in the adjusted models (models 2 and 3), there were no longer any significant differences in risk of functional disability among the four states of dentition (Table 2). Considering data recorded 3 years or later after the baseline survey, participants in Zones C (HR, 1.98; 95%CI, 1.26–3.11) and D (HR, 2.50; 95%CI, 1.54–4.01) exhibited a significantly greater risk of functional disability than those in Zone A, even after adjustment for conceivable covariates (model 3; Table 2; P for trend = 0.002).
4. Discussion
This prospective cohort study demonstrated that the status of dentition evaluated on the basis of numbers of remaining teeth and occlusal supports, in accordance with Miyachi’s Triangular Classification, was associated with incident functional disability in a community-dwelling elderly population. Individuals in Zones C (few teeth and occlusal supports) and D (relatively high number of teeth and few occlusal supports) were more likely to develop functional disability than those in Zone A (relatively stable occlusion). Furthermore, this relationship did not change even after adjustment for possible confounders, including age, sex, BMI, medical history, smoking status, alcohol consumption, extent of formal education, depressive symptoms, cognitive impairment, physical functioning, extent of social support, history of fall, and subjective masticatory ability.
In this study, denture wearers were categorized as follows: Zone A (41, 16.6%), Zone B (114, 62.0%), Zone C (279, 96.5%), and Zone D (115, 97.5%). We thought that non-denture wearers in Zones C and D would be particularly affected by the relationship between status of dentition and the incidence of functional disability. However, when we performed a subgroup analysis that excluded non-denture wearers in Zones C and D, the relationship between status of dentition and the incidence of functional disability did not change (data not shown).
In the present study, interestingly, the HR for incident functional disability in Zone D (HR [95%CI], 2.50 [1.54–4.01]) was higher than that in Zone C (HR [95%CI], 1.98 [1.26–3.11]), even though individuals in Zone D possessed a greater number of teeth than those in Zone C. This finding suggests that the relationship between tooth loss and functional disability is not dose-dependent but is mediated by the number of occlusal supports. Because most patients in Zone D have non-vertical stop occlusion, they are generally recognized as being difficult to treat and likely to experience a higher level of discontent with their prosthesis and greater inconvenience than others. Miyachi stated that individuals in Zone D might have a number of teeth but would have lost their occlusal support and that teeth that were not involved in occlusal support were more likely to augment the burden on the residual ridge under dentures [19]. In contrast, patients in Zone C tend to maintain a functionally stable condition despite losing almost all occlusal supports [19]. In order to maintain proper masticatory function and prevent
functional disability, it might be important to retain teeth with occlusal supports rather than just retaining teeth.
A possible pathway that explains the relationship between the status of dentition and incident functional disability is the increased risk of malnutrition due to deterioration of masticatory function [31]. Decline in nutritional status has been reported to be associated with cerebrovascular diseases [32], cognitive impairment [33], and frailty [34], which are all major causes of functional disability in Japan. In a cohort study involving 349 subjects of 70 years of age, the number of food items that the subjects could chew was significantly lesser in Zones B, C, and D than in Zone A [18]. The present findings, too, confirmed that objective masticatory ability (maximum occlusal force) of participants in Zones C (median[N] ± SD, 153.9 ± 135.9) and D (median[N] ± SD, 279.1 ± 203.1) was significantly lower than that for participants in Zone A (median[N] ± SD, 662.1 ± 372.6, Wilcoxon rank sum test: p< 0.001). In elderly people, differences in the status of dentition may be associated with general health through changes in nutrient intake and nutritional status.
Dysfunction of body balance due to loss of occlusal supports is also a possible pathway by which status of dentition is related to onset of functional disability. A previous study has shown that loss of occlusal supports is associated with a short one-leg standing time with open eyes, which reflects body balance [35]. In agreement with this previous finding, in the present study, the scores of the functional reach test—a clinical measure of body balance—were significantly lower among
participants in Zones C (median[cm] ± SD, 24.0 ± 19.0) and D (median[cm] ± SD, 25.0 ± 17.6) than among those in Zone A (median[cm] ± SD, 26.3 ± 19.0, Wilcoxon rank sum test: p< 0.001). Decline in balance function has been reported to be a risk factor for falling, which is one of the major causes of functional disability in Japan [36].
In the present study, since there was a violation of the proportional hazards assumption, the follow-up period was divided into two intervals (< 3 and ≥ 3 years). Consequently, no association was observed between status of dentition and onset of functional disability over short-term follow-up. The present study targeted community-dwelling elderly people who were relatively healthy and did not require long-term care. Therefore, it is presumed that the status of dentition affects the onset of functional disability not instantly but over time later in life.
The present study has some limitations. First, the response rate was not high (32.4%). Since this study was conducted as a CGA process in a public facility, the participants may have been healthier and had greater health awareness than others not included in the assessment. With regard to oral status, the mean number of remaining teeth (15.2) among participants of the Tsurugaya project in 2003 was higher than that (12.1) among participants of a national survey conducted in Japan in 2005 [37]. Therefore, though the selection bias in the present study does not affect the association between the status of dentition and incident functional disability, it needs to be considered when generalizing the present findings. Furthermore, since the number of
elderly participants with oral health impairment was limited, it is possible that the association between status of dentition and functional disability was underestimated in this study. Second, the present study did not survey changes in the status of dentition. Sato et al. [18] reported that in 70-year-old community-dwelling elderly subjects, classification of the various states of dentition in accordance with Miyachi’s Triangular Classification demonstrated different numbers of remaining teeth and occlusal supports and changes in masticatory ability 10 years from the baseline. Therefore, to clarify the impact of status of dentition on functional disability, future studies should assess the time course of both status of dentition and masticatory performance. Third, the present study might not have been completely free from detection bias. To receive LCTI certification, it is essential for some elderly individuals or their caregivers to contact the municipal government for application. In this study, some elderly individuals with disability may not have been certified, and the degree of this bias remains unverified. Fourth, we could not obtain information about causes for the incidence of functional disability. Therefore, it was not possible to state whether the status of dentition was associated with a particular type of disability or onset of disease (physical function, cognitive function, onset of cerebrovascular disease, etc.). Future studies are required to survey causes for the incidence of functional disability.
Although the present study had some limitations, the status of dentition evaluated in accordance with Miyachi’s Triangular Classification system was independently associated with incident functional disability in a community-dwelling elderly Japanese population. The present findings suggest that both maintenance of remaining teeth and retention of occlusal supports contribute to prevention of functional disability.
Conflict of interest: None.
Funding: This study was supported by Health Sciences Research Grants
(H21-Choju-Ippan-001, H22-Junkankitou-Ippan-001 and JSPS KAKENHI Grant Number JP17H06533) from the Ministry of Health, Labour and Welfare, Japan. The sponsor played no part in design, methodology, subject recruitment, data collections, analysis, or preparation of this paper.
Author contributions: Komiyama, Ohi, Tomata, Watanabe, and Tsuji:
study concept and design. Ohi, Miyoshi, Murakami, Tsuboi, Tomata, Tsuji, Watanabe, and Hattori: data collection. Komiyama, Ohi, Miyoshi, Murakami, Tsuboi, Tomata, Tsuji, and Hattori: data analysis and interpretation. Komiyama, Ohi, and Hattori: writing the first draft of the manuscript. Komiyama, Ohi, Tsuboi, Tomata, Tsuji, and Hattori: critical revisions for important intellectual content. All authors read and approved the final manuscript.
References
[1] World Health Organization. Healthy life expectancy(HALE) at birth, http://www.who.int/gho/mortality_burden_disease/life_tables/hale/en/; 2005 [accessed 29 August 2017].
[2] Joshipura KJ, Hung HC, Rimm EB, Willett WC, Ascherio A. Periodontal disease, tooth loss, and incidence of ischemic stroke. Stroke 2003;34:47–52.
[3] Abnet CC, Qiao YL, Dawsey SM, Donq ZW, Taylor PR, Mark
SD. Tooth loss is associated with increased risk of total death and death from upper gastrointestinal cancer, heart disease, and stroke in a Chinese population-based cohort. Int J Epidemiol 2005;34:467–74.
[4] Heitmann BL, Gamborg M. Remaining teeth, cardiovascular morbidity and death among adult Danes. Prev Med 2008;47:156–60. [5] Choe H, Kim YH, Park JW, Kim SY, Lee SY, Jee SH. Tooth loss, hypertension and risk for stroke in a Korean population. Atherosclerosis 2009;203:550–6.
[6] You Z, Cushman M, Jenny NS, Howard G. Tooth loss, systemic
inflammation, and prevalent stroke among participants in the reasons for geographic and racial difference in stroke (REGARDS)
study. Atherosclerosis 2009;203: 615–9.
[7] Stein PS, Desrosiers M, Donegan SJ, Yepes JF, Kryscio RJ. Tooth loss, dementia and neuropathology in the Nun study. J Am Dent Assoc 2007;138:1314–22.
[8] Kaye EK, Valencia A, Baba N, Spiro A 3rd, Dietrich T, Garcia
older men. J Am Geriatr Soc 2010;58:713–8.
[9] Tsakos G, Watt RG, Rouxel PL, de Oliveira C, Demakakos
P. Tooth loss associated with physical and cognitive decline in older adults. J Am Geriatr Soc 2015;63:91–9.
[10] Yamamoto T, Kondo K, Hirai H, Nakade M, Aida J, Hirata Y. Association between self-reported dental health status and onset of dementia: A 4-year prospective cohort study of older Japanese adults from the Aichi gerontological evaluation study (AGES)
project. Psychosom Med 2012;74:241–8.
[11] Yamamoto T, Kondo K, Misawa J, Hirai H, Nakade M, Aida J et al. Dental status and incident falls among older Japanese: A prospective cohort study. BMJ Open 2012;2: e001262.
[12] Anttila SS, Knuuttila ML, Sakki TK. Relationship of depressive symptoms to edentulousness, dental health, and dental health
behavior. Acta Odontol Scand 2001; 59:406–12.
[13] Ministry of Health, Labour and Welfare, Japan. Comprehensive survey of living conditions 2010. Ministry of Health, Labour and Welfare, Japan, http://www.mhlw.go.jp/english/database/db-hss/cslc-report2010.html; 2017 [accessed 29 August 2017].
[14] Shimazaki Y, Soh I, Saito T, Yamashita Y, Koga T, Miyazaki H, et al. Influence of dentition status on physical disability, mental
impairment, and mortality in institutionalized elderly people. J Dent Res 2001;80:340–5.
[15] Aida J, Kondo K, Hirai H, Nakade M, Yamamoto T, Hanibuchi T, et al. Association between dental status and incident disability in an older
Japanese population. J Am Geriatr Soc 2012;60:338–43.
[16] Komiyama T, Ohi T, Miyoshi Y, Murakami T, Tsuboi A, Tomata Y, et al. Association between tooth loss, receipt of dental care, and functional disability in an elderly Japanese population: The Tsurugaya Project. J Am Geriatr Soc 2016; 64:2495–502.
[17] Ikebe K, Matsuda K, Murai S, Maeda Y, Nokubi T. Validation of the Eichner index in relation to occlusal force and masticatory performance. Int J Prosthdont 2010;23:521–4.
[18] Sato N, Ono T, Kon H, Sakurai N, Kohno S, Yoshihara A, et al. Ten-year longitudinal study on the state of dentition and subjective
masticatory ability in community-dwelling elderly people. J Prosthodont Res 2016;60:177–84.
[19] Miyachi T. Defective dentition and prosthodontic treatment: clinical level, pattern and speed on the case study. Tokyo: Ishiyaku Publishers Inc; 2011.
[20] Kuboki T, Ichikawa T, Baba K, Hideshima M, Sato Y, Wake H, et al. A multi-centered epidemiological study evaluating the reliability of the treatment difficulty indices developed by the Japan Prosthodontic
Society. J Prosthdont Res 2012;56:71–86.
[21] Hozawa A, Ebihara S, Ohmori K, Kuriyama S, Ugajin T, Koizumi Y, et al. Increased plasma 8-isoprostane levels in hypertensive subjects: The Tsurugaya Project. Hypertens Res 2004;27:557–61.
[22] Kuriyama S, Hozawa A, Ohmori K, Shimazu T, Matsui T, Ebihara S, et al. Green tea consumption and cognitive function: a cross-sectional study from the Tsurugaya project. Am J Clin Nutr 2006;83:355–61.
[23] Ohi T, Sai M, Kikuchi M, Hattori Y, Tsuboi A, Hozawa A, et al. Determinants of the utilization of dental services in a community-dwelling elderly Japanese population. Tohoku J Exp Med 2009;218:241– 9.
[24] Blink TA, Yesavage JA, Lum O, Heersema PH, Adey M, Rose TL. Screening tests for geriatric depression. Clin Gerontol 1982;1:37–44. [25] Folstein MF, Folstein SE, McHugh PR. ‘Mini-mental state’. A practicalmethod for grading the cognitive state of patients for the clinician. J Psy-chiatr Res 1975;12:189–98.
[26] Podsiadlo D, Richardson S. The timed “Up & Go”: a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc
1991;39:142–8.
[27] Kondo N, Kawachi I, Hirai H, Kondo K, Subramanian SV, Hanibuchi T, et al. Relative deprivation and incident functional disability among older Japanese women and men: prospective cohort study. J Epidemiol Community Health 2009;63:461–7.
[28] Nitta A, Hozawa A, Kuriyama S, Nakaya N, Ohmori-Matsuda K, Sone T, et al. Relationship between peripheralarterial disease and incident disability among elderly Japanese: The Tsuru-gaya Project. J Atheroscler Thromb 2010;17:1290–6.
[29] Matsuda S, Yamamoto M. Long-term care insurance and integrated care for the aged in Japan. Int J Integr Care 2001;1:e28.
[30] Aparasu RR, Chatterjee S, Mehta S, Chen H. Risk of death in dual-eligible nursing home residents using typical or atypical antipsychotic agents. Med Care 2012;50:961–9.
[31] Sheiham A, Steele JG, Marcenes W, Lowe C, Finch S, Bates CJ, et al. The relationship among dental status, nutrient intake, and nutritional status in older people. J Dent Res 2001;80:408–13.
[32] Imamura T, Doi Y, Arima H, Yonemoto K, Hata J, Kubo M, et al. LDL cholesterol and the development of stroke subtypes and coronary heart disease in a general Japanese population: the Hisayama study. Stroke 2009;40:382–8.
[33] Tucker KL. Nutrient intake, nutritional status, and cognitive function with aging. Ann N Y Acad Sci 2016;1367:38–49.
[34] Bollwein J, Diekmann R, Kaiser MJ, Bauer JM, Uter W, Sieber CC, et al. Dietary quality is related to frailty in community-dwelling older adults. J Gerontol A Biol Sci Med Sci 2013; 68:483–9.
[35] Okuyama N, Yamaga T, Yoshihara A, Nohno K, Yoshitake Y, Kimura Y, et al. Influence of dental occlusion on physical fitness decline in a healthy Japanese elderly population. Arch Gerontol Geriatr 2011; 52:172–6.
[36] Tinetti ME, Doucette J, Claus E, Marottoli R. Risk factors for serious injury during falls by older persons in the community. J Am Geriatr Soc 1995;43:1214–21.
[37] Ministry of Health, Labour and Welfare. The survey of dental disease in 2005. Ministry of Health, Labour and Welfare, Japan,
http://www.mhlw.go.jp/toukei/list/62-17c.html; 2017 [accessed 29 August 2017].
Table 1 — Population characteristics according to classification of dentition.
Variables Overall Classification of dentition P value
Zone A Zone B Zone C Zone D
No. of subjects 838 247 184 289 118 Age, years ± 2SD 75.2 ± 9.0 73.6± 7.0 74.6 ± 7.8 77.0± 5.0 75.2± 4.0 <0.0001 Female, % 51.8 47.4 52.8 56.8 47.5 0.13 BMI, kg/m2 ± 2SD 24.1 ± 6.8 24.1 ±6.2 24.5 ± 6.4 24.0 ± 7.4 23.9 ± 7.0 0.22 Hypertension, % 41.3 41.7 45.1 37.4 44.1 0.34 Stroke, % 3.3 0.81 3.8 5.2 3.4 0.02 Myocardial infarction, % 10.3 12.2 11.4 8.7 8.5 0.49 Current smoker, % 10.3 7.3 6.5 12.5 17 0.007 Alcohol consumption, % 43 51.4 45.1 32.5 47.5 <0.0001
Depressive symptoms, % 24.7 20.2 25.5 29.1 22 0.18
Cognitive impairment, % 9.1 6.5 8.2 11.8 9.3 0.46
Physical function (4th quartile), % 24.5 17.4 22.8 31.1 25.4 0.003
Restricted social support, % 33.5 33.2 33.7 34 33.1 0.99
Fall within the previous 6 months, % 13.3 7.7 16.3 17 11 0.005
Decline in subjective chewing ability, %
30.8 10.1 20.1 51.6 39.8 <0.0001
P values were determined using the Wilcoxon rank-sum test for continuous variables and Fisher’s exact test for categorical variables.
Table 2 — Relationship between classification of dentition and incident disability (N = 838).
Classification of dentition Participants, n Incidents, n Model 1 Model 2 Model 3
HR (95%CI) < 3 years after baseline survey
Zone A 247 20 Reference Reference Reference
Zone B 184 25 1.70 (0.95-3.07) 1.44 (0.80-2.59) 1.32 (0.72-2.40)
Zone C 289 57 2.59 (1.55-4.31) * 1.44 (0.86-2.43) 1.32 (0.77-2.26)
Zone D 118 9 0.94 (0.43-2.05) 0.70 (0.32-1.55) 0.70 (0.31-1.54)
≥ 3 years after baseline survey
Zone A 219 31 Reference Reference Reference
Zone B 155 37 1.80 (1.12-2.90) ‡ 1.60 (1.00-2.58) 1.52 (0.94-2.47)
Zone C 221 82 3.22 (2.13-4.88) * 2.06 (1.35-3.15) * 2.00 (1.27-3.13) †
Zone D 108 44 3.55 (2.24-5.62) * 2.78 (1.75-4.41) * 2.53 (1.57-4.08) *
*P < 0.001; †P < 0.01; ‡P < 0.05.
Model 2: Model 1 + age and sex.
Model 3: Model 2 + medical history, body mass index, smoking, alcohol consumption, duration of education, depressive symptoms, cognitive impairment, physical function, restricted social support, fall within the previous 6 months, and subjective chewing ability.
HR: hazard ratio; CI: confidence interval.
Legends to Figures
Fig. 1 — Flow diagram of participant selection for the study.
Fig. 2 — Miyachi’s Triangular Classification. Zone A: occlusal supports ≥ 10; Zone B:
occlusal supports ≥ 5; Zone C: occlusal supports ≤ 4, number of teeth ≤ 10; Zone D: occlusal supports ≤ 4, number of teeth ≥ 11.
Fig. 3 — Kaplan–Meier curves showing cumulative incidence of functional disability in
accordance with classification of dentition. Log-rank test, P < 0.0001.
Fig. 1.
Residents of age ≥ 70 years living in Tsurugaya district N = 2,925
Participants in the baseline survey N = 948
Participants providing written informed consent N = 924
Long-term care needed at the time of baseline survey N = 79
Missing baseline information N = 7
Participants included in follow-up survey N = 838
Incident functional disability N = 305
Death N = 65
Migration N = 29
Fig. 2.
28
20
14
10
5
0
0
5
10
14
Number of remaining teeth
Zone C
Zone B
Zone D
Zone A
Fig. 3. 0 10 20 30 40 50 60 0 1 2 3 4 5 6 7 8 Cum ulative incidence ratio (%)
Follow-up time (years)
Zone D Zone C Zone B Zone A