A Case of Iliopsoas Abscess and Cerebellum Abscess Caused
by Misplacement of Central Venous Catheter
Aya Hiraoka,
1Yusuke Iki,
1Kazuya Odawara,
2Noriyuki Fumoto,
3Takeshi Morizane,
2and Hideo Tanaka
31 Postgraduate Clinical Training Center, Ehime Prefectural Central Hospital 2 Emergency and Critical Care Center, Ehime Prefectural Central Hospital 3 Department of Neurosurgery, Ehime Prefectural Central Hospital
A 64-year-old female was admitted due to iliopsoas abscess caused by misplacement of a central venous catheter (CVC) into the ascending lumbar vein (ALV). Despite removing the CVC and administering an antimicrobial agent, her general condition did not improve. Therefore, we performed a contrast-enhanced head computed tomography (CT) scan. The CT scan revealed a cerebellum abscess. Surgical cerebellum abscess drainage was thus performed urgently. We recommend using anteroposterior radiographs, J-guide wire catheter and ultrasound guidance to prevent misplacement. If misplacement of the CVC is suspected, it should be removed and a CT scan performed without hesitation as soon as possible.
Keywords: catheter misplacement, iliopsoas abscess, cerebellum abscess, ascending lumbar vein
Case Report
A 64-year-old female had been undergoing nasal feeding due to anorexia nervosa and depression for about a year at another hospital. One day, she developed fever approximately three weeks prior to admission at our hospital. She was diagnosed with urinary tract infection and treated with an antibiotic. CVC was inserted from the right femoral vein. Her fever reduced temporarily, although her inflammatory reaction worsened progressively. She developed fever again two days prior to admission at our hospital. She had progressive disturbance of consciousness. She was
brought to the emergency department of this hospital. She had a past medical history of atrialfibrillation. Initial vital signs were as follows: blood pressure of 116/83 mmHg, heart rate of 115 beats/min, respiratory rate of 15 breaths/min, SpO2of 97% on room air, body
temperature of 36.7°C, and the Glasgow Coma Scale was E2V1M1 (total 4/15). Physical examination revealed edema in her entire body, while other system examinations revealed nothing in particular. Laboratory studies were as follows: white blood cell (WBC) count 43,410/µl, hemoglobin (Hb) 10.8 g/dl, and C-reactive protein (CRP) 19.13 mg/dl. Cerebrospinal fluid (CSF)
Corresponding author: Aya Hiraoka
Postgraduate Clinical Training Center, Ehime Prefectural Central Hospital E-Mail: t401023h@yahoo.co.jp
Received for publication 18 November 2014 and accepted in revised form 23 January 2015 © 2015 The Japan Primary Care Association
General Medicine 2015, vol. 16, no. 2, p. 113–116.
Case Reports
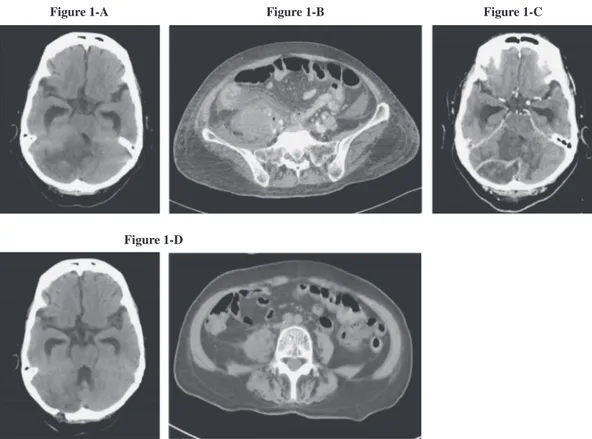
analysis was as follows: cells 1/µl, WBC 1/µl, protein 10 mg/dl, glucose 67 mg/dl. There was neither cardiac anomaly nor vegetation on echocardiography. Imaging findings on admission were as follows: Plain head CT scanning revealed a low density area in the cerebellar hemisphere and hydrocephalus due to press of fourth ventricle (Figure 1-A). Contrast-enhanced abdominal CT scan revealed swelling of the right iliopsoas muscle with gas and misplacement of the CVC (Figure 1-B). The patient was diagnosed with iliopsoas abscess caused by misplacement of the CVC into the ALV and hydrocephalus with cerebellum infarction. After the catheter was removed, antibiotic treatment consisting of linezolid (1200 mg/day) and cefozopran (4 g/day), and antihydropic treatment with glycerin (800 ml/day) (Figure 2) were initiated. Cultures of blood, spinal fluid, and the catheter tip were all negative, although iliopsoas muscle abscess drainage fluid was positive
only for Methicillin resistant Staphylococcus epidermi-dis (MRSE). On the 5th hospital day, a plain head CT scan showed progression of hydrocephalus. Ventricular drainage was performed. However hydrocephalus and disturbance of consciousness did not improve. On the 11th hospital day, a contrast-enhanced head CT scan revealed ring enhanced mass by contrast medium in a low density area of the cerebellar hemisphere (Figure 1-C). We diagnosed cerebellum abscess and performed surgical cerebellum abscess drainage. After the surgical drainage, her inflammatory reaction and consciousness state improved. On the 23th hospital day, a contrast-enhanced abdominal CT scan and head CT scan revealed that the iliopsoas muscle and cerebellum abscess had reduced (Figure 1-D). How-ever, the patient died due to aspiration pneumonia caused by vomiting on the 30th hospital day.
Figure 1. 1-A: Prain brain CT scan reveals low density area on right cerebellum and hydrocephalus due to pressure of ventriculus quartus. 1-B: Contrast-enhanced abdominal CT scan revealed a air image in swelling right iliopsoas and misplacement of the tip of the catheter. 1-C: Contrast-enhanced brain CT scan revealed ring enhanced by contrast medium in low density area of right cerebellum on the 11thhospital day. 1-D: The both iliopsoas and erebellum abscess are reduced on the 23th hospital day.
Figure 1-A Figure 1-B Figure 1-C
Figure 1-D
General Medicine 2015, vol. 16, no. 2
Discussion
About 50% of brain abscesses are caused by direct infection spreading from the otorhinolaryngologic region, and about 25% of brain abscesses are due to hematogenous infection spreading.1,2In our case, there was notable evidence of infection in the paranasal sinuses and oral cavity. We therefore considered hematogenous infection from the iliopsoas abscess as the cause of the cerebellum abscess. Iliopsoas abscess usually arises from the spread of infection of the digestive canal, urinary tract and orthopedics.3,4 We
suspect the cause of iliopsoas abscess in this case was misplacement of the CVC into the ALV. There are many reports of misplacement of the CVC in pediatric cases and left femoral vein approach cases.5 However there are few reports of adult cases and right femoral vein approach cases such as our case. Introduction of a catheter into the ALV is more likely to occur on the left side because of a lower degree of angulation between the iliac vein and the ALV.6,7There are some ways to avoid the serious complication associated with malpo-sition. Lateral deviation of catheters on the anteropos-terior radiographs represents cannulation of the ALV at the L4-L5 level.6Furthermore, the catheter may be safe-ly repositioned into the IVC with the use of a J-guide wire catheter8or by bedside ultrasound guidance.9
If a catheter is misplaced, it takes 14.8 days on average to be diagnosed.5 However, the elderly and mental
disorder patients usually find it difficult to personally
complain of symptoms. Therefore, we considered that it will take several days for such a condition to be diagnosed in our case. This suggests that it is important to remove the catheter and perform a CT scan without hesitation, if misplacement of the catheter or leakage of drug and infusionfluid from vessels into surrounding tissue is suspected. Dyspnea, pressure reduction, abdominal distension, low back pain and pleural effusion are remarkable symptoms that should trigger suspicion of misplacement of the catheter into the ALV and iliopsoas abscess formation.10
Conclusion
We reported a case of cerebellum abscess following iliopsoas abscess caused by misplacement of a CVC. Use of anteroposterior radiographs, J-guide wire catheters and ultrasound guidance has been reported as the way of reducing the risk of misplacement. We recommend removing the catheter and performing CT scans without hesitation, if catheter misplacement or leakage of drug and infusion fluid from vessels into surrounding tissues is suspected.
Conflict of interest: The authors have declared that no conflict of interest exists.
References
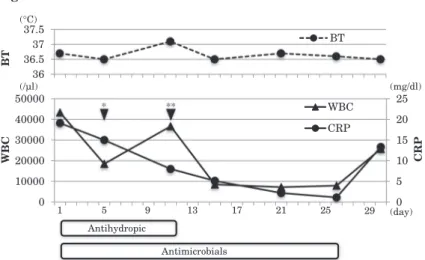
1 Okamura K, Shimazu M, Kobayashi S, et al: Case report Brain abscess at the site of cerebral infarction. Figure 2. The clinical course after admission.
36 36.5 37 37.5 BT BT 0 5 10 15 20 25 0 10000 20000 30000 40000 50000 CRP WBC WBC CRP Antihydropic Antimicrobials
BT: body temperature, WBC: white blood cells, CRP: C-reactive protein. *: ventricular drainage, **: cerebellum abscess drainage.
(day) 1 5 9 13 17 (mg/dl) (/µl) (°C) 21 * ** 25 29
A Case of Iliopsoas Abscess and Cerebellum Abscess Caused by Misplacement of Central Venous Catheter
Jpn J Neurosurg. 1998;7(10):644–647.
2 Takahashi K, Funayama Y, Fukushima K, et al: A case report of Crohn’s disease complicating with brain abscesses and splenic abscesses caused by infection of central venous catheter and subcutaneal port. Jpn J Gastroenterol Surg. 2005;38:1607–1611.
3 Ito I, Miura A: A case of type 2 diabetes mellitus complicated with left iliopsoas abscess caused by a left femoral vein catheter during treatment for right pyothorax and right subphrenic abscess. Nippon Ronen Igakkai Zasshi. 2011;48:180–184.
4 Yamamoto T, Yamakoshi M, Suzuki K, Yamamoto T, Shinagawa N, Ariga K: A case of psoas abscess associated in the elderly. Kansenshogaku Zasshi. 1996; 70(4):371–376.
5 Yamada M, Niwa K, Takahashi M, et al: IVH catheter inserted via the femoral vein inducing rectus abdominis muscle abscess formation via the inferior epigastric vein. J Jpn College Surg. 2007;32(6):914– 917.
6 Lavandosky G, Gomez R, Montes J: Potentially lethal misplacement of femoral central venous cathe-ters. Crit Care Med. 1996;24:65–68.
7 Gocze I, Muller-Wille R, Stroszczynski C, Schlitt HJ, Bein T: Accidental cannulation of the left ascending lumbar vein through femoral access-still often unrecognized. ASAIO J. 2012;58(4):435–437. 8 Harayama N, Isa Y, Arai H, et al: Two cases of extracorporeal membrane oxygenation catheter mis-placement in the ascending lumbar vein. J Jpn Soc Intensive Care Med. 2012;19:367–370.
9 Carrion E, Hertzog JH, Gunter AW, Lu T, Ruff C, Hauser GJ: Misplacement of femoral venous catheter into the ascending lumbar vein: repositioning using ultrasonographic guidance. Intensive Care Med. 2001; 27:240–242.
10 Tachimori A, Yamagata S, Ako E, et al: A case of ascites due to mislodging of a central venous catheter developed 20 days after its placement via the femoral vein. J Jpn Surg Assoc. 2009;70(7):2190–2194. General Medicine 2015, vol. 16, no. 2