九州大学学術情報リポジトリ
Kyushu University Institutional Repository
Quantitative evaluation of bone-resorptive lesion volume in osteonecrosis of the femoral head using micro-computed tomography
馬場, 省次
http://hdl.handle.net/2324/4060038
出版情報:九州大学, 2019, 博士(医学), 課程博士 バージョン:
権利関係:©2019 Societe francaise de rhumatologie. Published by Elsevier Masson SAS. All rights reserved.
Availableonlineat
ScienceDirect
www.sciencedirect.com
Original article
Quantitative evaluation of bone-resorptive lesion volume in
osteonecrosis of the femoral head using micro-computed tomography
Shoji Baba , Goro Motomura
∗, Satoshi Ikemura , Yusuke Kubo , Takeshi Utsunomiya , Hiroyuki Hatanaka , Koichiro Kawano , Yasuharu Nakashima
DepartmentofOrthopaedicSurgery,GraduateSchoolofMedicalSciences,KyushuUniversity,3-1-1,Maidashi,Higashi-ku,Fukuoka,812-8582,Japan
a r t i c l e i n f o
Articlehistory:
Accepted4September2019 Availableonline12September2019
Keywords:
Osteonecrosisofthefemoralhead Boneresorption
Micro-CT Collapse
a b s t r a c t
ObjectivesToquantifythevolumeofbone-resorptivelesionsinpost-collapseosteonecrosisofthefemoral head(ONFH)usingmicro-computedtomography(micro-CT)andassesstheircharacteristicsinpost- collapseONFH.
MethodsWeinvestigated35femoralheadsresectedfrom35patientswithONFH(20menand15 women;meanage,47.2years).Oneachofsevencoronalhigh-resolutionmicro-CTslicesofthefemoral head,thebone-resorptiveareaswereextractedusingbonemicrostructuremeasurementsoftware.Next, thetotalbone-resorptivevolumeratio,definedastheratioofallbone-resorptivecross-sectionalareasto allfemoralheadcross-sectionalareasinallsevenslices,wascalculated.Associationsbetweentotalbone- resorptivevolumeratioandsex,age,ONFH-associatedfactors,patientworkloadlevels,ONFHstage,ONFH type,necroticvolumeonmagneticresonanceimaging,anddurationfromtheonsetofpaintosurgery wereanalyzed.Lesionlocationandtheassociationbetweenbone-resorptivelesionandcollapsewere alsoevaluated.
ResultsThemeantotalbone-resorptivevolumeratiowas7.0±6.0%,whichvariedsignificantlybyONFH stage(ARCOcollapsequantitation3A,3.5±2.1%;3B,6.8±3.0%;and3C,13.6±8.8%).ONFHstagewas independentlyassociatedwithtotalbone-resorptivevolumeratio(P<0.05).Furthermore,highbone- resorptivevolumeratioswerefoundintheanteriorfemoralheadandwereassociatedwithcollapse.
ConclusionsThisstudydemonstratedthatbone-resorptivevolumeinpost-collapseONFHwassignif- icantlyassociatedwiththediseasestage,whichwasmorewidespreadintheanteriorportionofthe femoralheadthanintheposteriorportion.
©2019Soci ´et ´efranc¸aisederhumatologie.PublishedbyElsevierMassonSAS.Allrightsreserved.
1. Introduction
Nontraumatic osteonecrosis of the femoral head (ONFH) is characterizedby femoralheadcollapseseveralmonthstoyears aftertheoccurrence ofosteonecrosis [1].Previous studieshave demonstratedthatacollapsedfemoralheadwithONFHinevitably involvesasubchondralfracture[2],whichmightbethemechanism ofcollapse initiation.Aftercollapse(ora subchondralfracture), somefemoralheadsmightpreservearelativelysphericalshape, whileothersmightbecomeseverelydeformed.Theshapeofthe femoralheadaftercollapseisessentialtoconsiderwhenselecting atherapeuticstrategy;however,thepathomechanismsofcollapse progressionremainunclear.
∗ Correspondingauthor.
E-mailaddress:[email protected](G.Motomura).
In post-collapse ONFH, bone-resorptive lesions can be seen withinthefemoralhead[3,4].BoneresorptioninONFHisconsid- eredtobecausedbyosteoclastsduringtheinitialphaseoftherepair process[5],whileboth theextentandlocation ofbone resorp- tionseem tobedifferentamong patientsin ONFH.Plenketal.
reportedthatthereareseveraltypesofrepairprocessesinONFH,in whichfemoralheadswithpredominantboneresorptionundergo moredestructionwithtime[4],suggestingthepossibleassociation betweenboneresorptionandcollapseprogression.
Ontheotherhand,tothebestofourknowledge,therehave been no studies that have quantitatively characterized bone resorptioninONFH.Withconventionalclinicalcomputedtomog- raphy(CT),detailedanalysisofbone-resorptivelesionsincluding their distribution and dimensions has been difficult. However, usingmicro-CTallowsustoevaluatethethree-dimensionalbone structureoftheentirefemoralheadindetailandquantitativelyat themicro-level[6–8].Therefore,thepurposesofthisstudywere https://doi.org/10.1016/j.jbspin.2019.09.004
1297-319X/©2019Soci ´et ´efranc¸aisederhumatologie.PublishedbyElsevierMassonSAS.Allrightsreserved.
76 S.Babaetal./JointBoneSpine87(2020)75–80
toquantifybone-resorptivelesionsusingmicro-CTandassessthe characteristicsofbone-resorptivelesionsinpost-collapseONFH.
2. Methods 2.1. Patients
Thisstudy was approved by the institutional review board.
Informedconsentwas obtainedfrom allindividualparticipants includedinthestudy.BetweenApril2012andAugust2017,77hips in67patientswithONFHunderwentprimaryjointreplacement surgery(totalhiparthroplastyorbipolarhemiarthroplasty)atour institution.Ofthese77hips,27wereexcludedfromthisstudyfor thefollowingreasons:21hipshadsevereosteoarthriticchanges, fourhipshadseverefemoralheaddeformityduetocollapse,and twohipshadeccentrically-locatednecroticlesions.Inaddition,five hipsinfivepatientstreatedwithabisphosphonateintakeforosteo- porosis wereexcluded.In 10 patientswho underwentbilateral jointreplacementsurgery,onehipineachpatientwasrandomly selectedforanalysistofulfillthestatisticalassumptionofindepen- dentobservation.Thus,weinvestigated35entirefemoralheads resectedfrom35patientswithONFH(20menand15women)with ameanageof47.3years(median46years,range18–81years).
FactorsassociatedwithONFHincludedcorticosteroiduse(>2gof prednisoloneoritsequivalentwithina3-monthperiod)in20hips andalcoholabuse(>320g/week)in15hips,whichwereclassified basedontheAssociationResearchCirculationOsseous(ARCO)eti- ologicclassificationcriteria[9,10].Inaddition,weclassifiedpatient workloadlevelsintothreegroups:lowactivity(unemployed)for 12hips,moderateactivity(workinanofficeenvironmentorthe hospitalityindustry,etc.)for17 hips,andhighactivity(nursing, workingforadeliveryserviceorinconstruction,etc.)forsixhips.
BasedontheARCOinternationalclassificationofosteonecrosis,all 35femoralheadswereclassifiedintostage3[11].Inthecurrent study,15femoralheadswith≤2mmofcollapseweredefinedas stage3A,12femoralheadswith2–4mmofcollapseasstage3B, andeightfemoralheadswith≥4mmasstage3C,byreferenceto theARCOquantitationofadomedepression[11].Eveninpatients
withnoobviousseveredeformityofthefemoralhead,weconsid- eredjointreplacementsurgerytobeindicatedwhentherewasan extensivenecroticlesionwithasubchondralfractureconfirmedon CTorbonemarrowedemasuggestiveofasubchondralfractureon magneticresonanceimaging(MRI)[12].Inaddition,thelocationof necroticlesionwasclassifiedusingtheJapaneseInvestigationCom- mitteeclassificationsystem[13]:typeC1(morethanthemedial two-thirdsoftheweight-bearingportionbut notextendinglat- erallytotheacetabularedge)in14hips,andtypeC2(extending laterallytotheacetabularedge) in21 hips.The meanduration fromtheonsetofpaintosurgerywas11.7±9.3months(median 7months,range 1–36months).Furthermore,thevolumeofthe necroticlesiononMRIwasdefinedasacombinednecroticangle usingthemodifiedKerboulmethod[14].Briefly,theanglesofthe femoralsurfacewithnecrosisonamid-sliceinT1-weightedcoronal andaxialviewsweremeasuredandsummed.Themeancombined necroticanglewas277.4±63.4(median262,range170–465).
2.2. Quantificationofbone-resorptivelesions
All35 sampleswerescanned withhigh-resolutionmicro-CT (RmCTT1,Rigaku,Tokyo,Japan)immediatelyaftersurgery.Micro- CTwasperformedatavoltageof60kV,currentof60A,voxelsize of133×133×133m3,andslicethicknessof0.4mm.Inthecur- rentstudy,abone-resorptiveareawasdefinedasaspace≥1mm indiameterandcoronalimagesofmicro-CTwereinvestigated.On eachcoronalmicro-CTslice,bone-resorptiveareaswereextracted usingbonemicrostructuremeasurement software(TRI/3D-BON, RatocSystemEngineering,Tokyo,Japan) followinga previously reportedmethod(Fig.1A–F)[8].Briefly,boneregionsincludingthe bonetrabeculaeand thecorticalshellweredepictedbybinariz- ingCTimagesusingabonethreshold(Fig.1B).Next,theentire regionwasdepicted(Fig.1C).Emptyregionsnotinvolvingbone weredepictedby subtracting thebone regionsfrom theentire region(Fig.1D). Inordertoidentifyemptyregionsof≥1mmin diameter,emptyregions<1mmindiameterwereclearedtoerode theallemptyregionsthree-dimensionallyby0.5mmdecrements fromtheirsurface(Fig.1E).Torestoretheoriginalshapeofthe
Fig.1.Quantificationofbone-resorptiveareasdefinedasspaces≥1mmindiameterusingbonemicrostructuremeasurementsoftware(TRI/3D-BON,RatocSystemEngi- neering,Tokyo,Japan).A.Acoronalmicro-CTimage;B.Boneregions,includingthebonetrabeculaeandthecorticalshell,aredepictedafterbinarizingCTimagesusinga bonethreshold;C.Theentireregionofafemoralheadisdepicted;D.Emptyregionsnotinvolvingbonearedepictedbysubtractingtheboneregionsfromtheentireregion;
E.Inordertoidentifyemptyregionsof>1mmindiameter,emptyregionslessthan1mmareclearedtoerodefromthesurfacethree-dimensionallyin0.5mmdecrements;
F.Torestoretheoriginalshapeoftheremainingemptyregionsintheaboveprocess,theirsurfacesaredilatedby0.5mmincrementsfromtheirsurface.Oftheremaining emptyregions,abone-resorptiveareaisdefinedasaregionconnectedtoanecroticlesion.
Fig.2. Distinguishingbetweenbone-resorptiveareasandbonedefectareas.
Bone-resorptiveareas(whitearrows)aredistinguishedfrombonedefectareas (whitearrowheads)causedbyasubchondralfractureorcollapsebasedonCTvalues.
remainingemptyregionsintheaboveprocess,theirsurfaceswere dilatedby0.5mmincrements(Fig.1F).Oftheremainingempty regions,abone-resorptiveareawasdefinedasaregionconnected toanecroticlesionanddistinctfromareasofbonedefectcausedby asubchondralfractureorcollapsebasedonCTvalues(Fig.2).The definitionofeachbone-resorptiveareawasbasedonconsensus amongthreeobservers(S.B.,T.U.,andH.H.);theyalsoconfirmed theareaofnecrosiswithMRI.Aftermicro-CT,allsampleswere madeaconfirmeddiagnosisofONFHbyahistopathologicaleval- uationbasedonpreviouslyreportedhistopathologicalcriteriaof ONFH[15,16].
2.3. Assessmentofbone-resorptivelesioncharacteristics
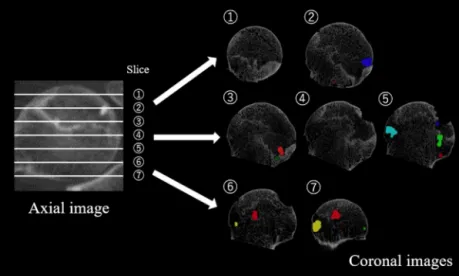
Inordertoquantitativelyassessthebone-resorptivevolumein theentirefemoralhead,atfirst,thecoronalslicesoffemoralhead weredividedequallyintosevenslices(Fig.3).Ineachslice,the cross-sectionalareaofthefemoralheadwasdefinedasthearea ofaconcentriccirclecenteredonthecenterofthefemoralhead.
Bothbone-resorptiveandfemoralheadcross-sectionalareaswere calculatedusingtheImageJsoftwareprogram(NationalInstitutes ofHealth,Bethesda,MD,USA).Themeanratioofbone-resorptive areastofemoralheadcross-sectionalareaswascalculatedforeach slice.Inaddition,thetotalbone-resorptivevolumeratioineach femoralheadwasdefinedastheratioofallbone-resorptiveareas toallfemoralheadcross-sectionalareasinsevenslices.Univariate
associationsbetweenthedegreeoftotalbone-resorptivevolume ratio and sex,age, associatedfactors of ONFH(steroidor alco- hol),stageandtypeofONFH,patientworkloadlevels,combined necroticangle,anddurationfromtheonsetofpaintosurgerywere analyzedfirst.Subsequently,afterconfirmingtheareaofnecrosis withMRI,theratioofthebone-resorptiveareatofemoralhead areainbothintra-necroticandextra-necroticlesionswereinves- tigated for each slice. Furthermore, thepresence or absenceof collapseinthesevensliceswasrecordedforall35femoralheads, andtherelationshipbetweenbone-resorptiveareasandfemoral headcollapsewasinvestigatedbycomparingbone-resorptiveareas betweensliceswithandwithoutcollapse. Inthecurrent study, collapsewasdefinedasabreakageofthefemoralheadcontour, includingasubchondralfracture.Finally,thecorrelationbetween collapseprogression rateandbone-resorptivevolumeratiowas investigatedusing31of35femoralheadsthatunderwentclinical CTforpreoperativeplanningatanaverageof72.7days(median 13days,range 1–837days)beforesurgery.Briefly,theprogres- sionofcollapseperdaywasdefinedasthedifferencebetweenthe collapsedepthoncorrespondingmid-coronalCTslicesbeforeand aftersurgerydividedbythenumberofdaysbetweenthetwoscans.
Collapse depthaftersurgery wasmeasuredusingthe micro-CT imagesofsurgicallyresectedfemoralheadsscannedimmediately aftersurgery.OneachofCTandmicro-CTimages,collapsedepth wasmeasuredasthedistancebetweentheconcentriccirclethat fitsthefemoralheadandthemaximumincursionintothefemoral headonthelinepassingthroughthecenterofthefemoralhead.
2.4. Statisticalanalysis
Dataareexpressedasmeans±SD.Allvariablesweretestedfor normalitywith theShapiro-Wilk test and for homoscedasticity withLevene’stest.Associationsbetweensex,associated factors, type of ONFH, and bone-resorptive volume ratio, respectively, were compared using Wilcoxonrank sumtest. The association between bone-resorptivevolume in slices with versus without collapsewasalsoinvestigatedusingWilcoxonranksumtest.The bone-resorptivevolumeratioforeachstageorpatientworkload levelwerecomparedusingSteel-Dwassmultiple-comparisontest.
Thecorrelationsbetweenage,durationfromtheonsetofpainto surgery, combined necrotic angle, and bone-resorptive volume ratio, respectively, were analyzed using Spearman’s correlation coefficient.The correlationbetweentheprogressionof collapse per day and bone-resorptive volume ratio was also analyzed
Fig.3. Methodsusedtoquantifythebone-resorptivevolumeoftheentirefemoralhead.
Inordertoquantitativelyassessthebone-resorptivevolumeintheentirefemoralhead,thecoronalslicesofafemoralheadaredividedequallyintosevenslices.Thetotal bone-resorptivevolumeratioineachfemoralheadisdefinedastheratioofallbone-resorptiveareastoallfemoralheadcross-sectionalareasinsevenslices.
78 S.Babaetal./JointBoneSpine87(2020)75–80
usingSpearman’scorrelationcoefficient.Significantfactorsasso- ciatedwithbone-resorptivevolume ratio wereidentified using multivariateanalysiswithstepwiseregressionthat includedall parameters. All statistical analyses were performed using the JMPsoftwareprogram(version13.0,SASInstituteInc.,Cary,NC, USA).P-valueslessthan0.05wereconsideredtobestatistically significant.
3. Results
Themeantotal bone-resorptivevolumeratiowas7.0±6.0%, whichwassignificantlydependentonONFHstage(3A,3.5±2.1%;
3B,6.8±3.0%;and3C,13.6±8.8%;P<0.05),whiledurationfrom theonset of pain tosurgery and patientworkload levelswere notassociatedwithbone-resorptivevolumeratio(Table1).Based onmultivariateanalysis,ONFHstagewasidentifiedtobeinde- pendently associated with total bone-resorptive volume ratio (P<0.01).
Withrespecttothelocationofbone-resorptiveareas,ahigh percentage of bone-resorptive cross-sectional areas tended to beseen in the anterior femoralhead (Fig.4). Therewas more bone-resorptive area in slice 1 than in slices 4–7 (P<0.01, respectively)andinslice2comparedwithslice6(P<0.05).Fur- thermore, most bone-resorptive areas in each slice and 81.9%
ofallbone-resorptiveareaswerefoundwithinnecroticlesions.
Meanbone-resorptive areain intra-necrotic lesions(5.9±7.1%) wassignificantlylargerthaninextra-necroticlesions(1.3±3.2%;
P<0.001).Inaddition,sliceswithfemoralheadcollapsewerealso more likely to befound in theanterior portion. Regarding the correlationbetweenbone-resorptivelesionsandfemoralheadcol- lapse,slices withcollapse hada significantlyhigher meanratio ofbone-resorptiveareas(9.4±10.6%)thansliceswithoutcollapse (2.9±3.3%;P<0.001;Fig.5A).Themeanprogression ofcollapse perdaywas87.1±115.9m(median26.8m,range0–400m).
Therewasasignificantpositivecorrelationbetweentheprogres- sionofcollapseperdayandbone-resorptivevolumeratio,(=0.59, P<0.001;Fig.5B).
4. Discussion
The current quantitative study demonstrated that bone- resorptive volume within the femoral head is significantly associatedwiththepost-collapsestageofONFH.Inaddition,the collapseprogressionrateandbone-resorptivevolumeratiowere positivelycorrelated. Thesefindings suggest that thedegree of boneresorptionmightincreaseascollapseprogresses.Ontheother hand,wefoundnootherfactorsinfluencingbone-resorptivevol- ume, including the duration from the onset of pain or patient workloadlevels.Althoughitremainsunclearwhetherboneresorp- tionisanantecedentphenomenontocollapseorasubchondral fracture, the current results suggested a cause-and-effect rela- tionship between bone resorption and collapse progression in post-collapseONFH.
Severalstudiessupporttherelationshipbetweenboneresorp- tionandcollapseprogression.Plenketal.reportedthatthereare severaltypesofrepairprocessesinONFH,inwhichfemoralheads withpredominantboneresorptionundergomoredestructionwith time[4].Karasuyamaetal.histopathologicallydemonstratedthat significantlymoreosteoclastsarepresentattheboundaryofthe necroticlesionwithcollapse versuswithoutcollapse[17].Inan animalstudy,increasedboneresorptionwasshowntobeassoci- atedwiththelossofstructuralintegrity,leadingtofemoralhead deformity [18]. Considering thesereports and ourfindings, we hypothesizethat the failure of mechanical stabilization due to excessiveboneresorptionmayleadtotheprogressionofcollapse.
Bisphosphonates,whichareosteoclastinhibitors,wereusedon atrialbasis topreventtheoccurrenceoffemoralheadcollapse basedontheconceptthatosteoclasticbone resorptioninitiates collapse [5]. Previous reports have indicated that bisphospho- nates may have the potential to postpone the progression of femoralheadcollapse[19–21],whichsuggeststhatboneresorp- tionmaybeacauseofcollapseprogression.However,tothebest ofourknowledge,therehavebeennostudiesthathavequanti- tativelycharacterizedbone-resorptivelesionsinONFH.Although wecannotconcludewhetherbone-resorptivelesionsareacause oraconsequenceoffemoralheadcollapseduetothedesignof thisstudy,thisisthefirststudythatquantitativelycharacterized
Table1
Univariateanalysisoftherelationshipbetweenbone-resorptivevolumeratioandpatientcharacteristics.
Bone-resorptivevolumeratio(%) P-value Correlationcoefficient
Mean±SD Median(IQR) Range
Sexa
Male 5.9±6.7 4.2(1.9–7.0) 0.5–31.2 <0.05
Female 8.4±4.7 6.7(4.7–12.3) 2.0–18.5
Associatedfactora
Steroid 7.4±4.8 6.7(3.3–11.2) 0.5–18.5 0.22
Alcohol 6.4±7.5 4.7(2.0–7.2) 1.3–31.2
JICtypea
C1 6.8±4.3 5.8(3.2–10.9) 1.9–15.2 0.56
C2 7.0±7.0 6.0(2.0–7.9) 0.5–31.2
ONFHstageb
3A 3.5±2.1 3.1(1.9–5.4) 0.5–7.2 3Avs3B:<0.01
3B 6.8±3.0 6.8(4.2–9.0) 1.6–11.9 3Avs3C:<0.01
3C 13.6±8.8 12.6(7.2–17.7) 2.0–31.2 3Bvs3C:<0.05
Workloadlevelsb
Low 9.1±4.7 7.8(6.1–12.2) 1.9–18.5 LowvsMod.:0.15
Moderate 6.4±7.3 3.4(2.0–7.9) 0.5–31.2 LowvsHigh:0.09
High 4.1±2.2 4.1(1.9–5.9) 1.6–7.2 Mod.vsHigh:0.92
Agec 0.27 0.19
Durationfromtheonsetofpaintosurgeryc 0.99 <0.01
Combinednecroticanglec 0.46 0.13
SD:standarddeviation;IQR:interquartilerange;JIC:JapaneseInvestigationCommittee;ONFH:osteonecrosisofthefemoralhead.
aWilcoxonranksumtest.
b Steel-Dwassmultiple-comparisontest.
c Spearman’scorrelationcoefficient.
Fig.4.Meanratioofbone-resorptivecross-sectionalareatofemoralheadcross-sectionalareaandpercentageofbone-resorptiveareainintra-necroticversusextra-necrotic lesionsbyslice.Themeanratioofbone-resorptiveareas(bargraph)andpercentageofsliceswithcollapse(linegraph)tendtobehigherintheanteriorportionofthe femoralhead.Thereismorebone-resorptiveareainslice1thaninslices4–7(P<0.01,respectively),aswellasinslice2versusslice6(P<0.05).Inaddition,withineach slice,mostbone-resorptiveareasarefoundinintra-necroticlesions.Thetotalbone-resorptiveareainintra-necroticlesions(5.9±7.1%)issignificantlylargerthanthetotal bone-resorptiveareainextra-necroticlesions(1.3±3.2%;P<0.001).
Fig.5. A.Theassociationbetweenbone-resorptivelesionandfemoralheadcollapse.
Themeanratioofbone-resorptiveareasinsliceswithcollapse(9.4±10.6%)issignificantlyhigherthanthatinsliceswithoutcollapse(2.9±3.3%,P<0.001);B.Thecorrelation betweentheprogressionofcollapseperdayandthebone-resorptivevolumeratio.Thereisasignificantpositivecorrelationbetweenthebone-resorptivevolumeratioand progressionofcollapseperday(=0.59,P<0.001).Thecurvedlineindicatesa95%confidenceellipsethatcontains95%ofthedata.
bone-resorptivelesionsinpost-collapseONFHanddemonstrateda possibleassociationbetweenbone-resorptivevolumeanddegree offemoralheadcollapseaswellasthecollapseprogressionrate.
Therefore,webelievethatthisstudyprovidesvaluableinformation forabetterunderstandingofbone-resorptivelesionsincollapsed femoralheadandservesasabasisforfutureinvestigationstopre- ventfemoralheadcollapseinpatientswithONFH.
Inthecurrentstudy,bone-resorptivelesionsweremorecom- monintheanteriorportionofthefemoralhead,andlesionlocation wassignificantlyassociatedwiththepresenceofcollapse.Since theanteriorportionofthefemoralheadissusceptibletomechan- icalstressduetothenatureofacetabularcoverage[22],itseems reasonablethatcollapse wasmore commonlyseenintheante- riorportionofthefemoralhead.Ontheotherhand,tothebest ofourknowledge,nostudieshavedemonstratedboneresorption beforecollapseinONFH.Althoughthecurrentstudyshowedsim- plybone-resorptivevolumeaftercollapse,wespeculatedthatbone
resorptionbeingpredominantlyintheanteriorportionmaybedue totheinfluenceofcollapse.
Themain limitationofthis studywastheinabilitytoassess time-dependentchangesinbone-resorptivevolumeprospectively.
Since we limited the subjects of the current study to whole femoral heads resected from patients with ONFH in order to assessthedetailedcharacteristicsofbone-resorptivelesionsusing micro-CT,thefindingsofthecurrentstudyreflectonlythestate of bone-resorptivelesionsatthetime ofsurgery. However,the current study demonstrated nosignificant correlation between duration fromtheonset ofpaintosurgeryand bone-resorptive volume. Therefore, we believe that this study provides useful information aboutboneresorptionin post-collapseONFH,even though evaluation occurred at one-time point. Second, regard- ingtherelationshipbetweenbone-resorptivevolumeandcollapse progressionrateperday,bone-resorptivelesionvolumeshouldbe ideallyassessedatbaselinetoevaluateitscausalrelationshipwith
80 S.Babaetal./JointBoneSpine87(2020)75–80
collapseprogression.However,itisnotpossibletoperformmicro- CT beforesurgery. Alternatively, we utilized clinicalCT images takenforpreoperativeplanning.Sincetheimagequalityofclinical CTscanswastoopoortoquantifythevolumeofbone-resorptive lesions,weassessedthecorrelationbetweencollapseprogression rateand bone-resorptivevolume of theresected femoralhead.
Althoughnotideal,webelievethecurrentresultsprovidevalu- abledatatosupportarelationshipbetweenboneresorptionand collapse progressionin post-collapse ONFH.Finally, thepatient agedistributionwaswideandwedidnotevaluatepatientactivi- tiesofdailyliving,whichmaybeassociatedwiththeprogression offemoralheadcollapse.Althoughthisstudydemonstratedthat patientageandworkloadlevelswerenotsignificantlycorrelated withbone-resorptivevolume,inafutureprospectivestudy,eval- uationofpatientactivityanddetailedexaminationbyagegroup shouldbeperformedtoelucidatethepathomechanism of bone resorptioninONFHusinghigh-resolutionradiologicalequipment invivo.
5. Conclusions
Thisstudydemonstratedthatbone-resorptivevolumeinpost- collapseONFHwassignificantlyassociatedwiththediseasestage andcollapseprogressionrate,whichwasmorewidespreadinthe anteriorportionofthe femoralhead thanin theposteriorpor- tion.Webelievethatthisstudyprovidesabetterunderstandingof boneresorptionincollapsedfemoralheadsandpotentialclinical therapeutictargetsforONFH.
Authors’contributions
Studydesign:S.B.andG.M.Acquisitionofdata:S.B,G.M,S.I., andY.N.Studyexecution:S.B.,Y.K., T.U.,H.H.,and K.K.Drafting ofthemanuscript:S.B.Revisionofthemanuscript:GM,SI, and YK.Approvalofthefinalversionofthemanuscript:S.B.,G.M.,S.I., Y.K.,T.U.,H.H.,K.K.,andY.N.Allauthorstakeresponsibilityforthe integrityofthedataanalysis.
Disclosureofinterest
Theauthorsdeclarethattheyhavenocompetinginterest.
Acknowledgements
We thank Junji Kishimoto, a statistician from the Digital MedicineInitiativeatKyushuUniversity,forhisadviceonthesta- tisticalanalysis.ThisworkwaspartiallysupportedbyGrants-in-Aid forScientificResearch(16K10906,16H07057,and19K09601)from theJapanSocietyforthePromotionofScience.
References
[1]OhzonoK,SaitoM,TakaokaK,etal.Naturalhistoryofnontraumaticavascular necrosisofthefemoralhead.JBoneJointSurgBr1991;73:68–72.
[2]MotomuraG,YamamotoT,YamaguchiR,etal.Morphologicalanalysisof collapsedregionsinosteonecrosisofthefemoralhead.JBoneJointSurgBr 2011;93:184–7.
[3]MurpheyMD,ForemanKL,Klassen-FischerMK,etal.Fromtheradiologic pathologyarchivesimagingofosteonecrosis:radiologic-pathologiccorrela- tion.Radiographics2014;34:1003–28.
[4]PlenkJrH,GstettnerM,GrossschmidtK,etal.Magneticresonanceimaging andhistologyofrepairinfemoralheadosteonecrosis.ClinOrthopRelatRes 2001;386:42–53.
[5]KenzoraJE,GlimcherMJ.Pathogenesisofidiopathicosteonecrosis:theubiqui- touscrescentsign.OrthopClinNorthAm1985;16:681–96.
[6]WangC,WangX,XuXL,etal.Bonemicrostructureandregionaldistributionof osteoblastandosteoclastactivityintheosteonecroticfemoralhead.PLoSOne 2014;9:e96361.
[7]MaJ-X,HeW-W,ZhaoJ,etal.Bonemicroarchitectureandbiomechanicsofthe necroticfemoralhead.ScientificReports2017:7.
[8]ChibaK,BurghardtAJ,OsakiM,etal.Three-dimensionalanalysisofsubchondral cystsinhiposteoarthritis:anexvivoHR-pQCTstudy.Bone2014;66:140–5.
[9]YoonBH,JonesLC,ChenCH,etal.Etiologicclassificationcriteriaofarcoon femoralheadosteonecrosispart1:glucocorticoid-associatedosteonecrosis.J Arthroplasty2019;34:163–8.
[10]YoonBH,JonesLC,ChenCH,etal.Etiologicclassificationcriteriaofarcoon femoralheadosteonecrosispart2:alcohol-associatedosteonecrosis.JArthro- plasty2019;34:169–74.
[11]JWM G. ARCOcommitteeon terminology andstaging. ARCO Newsletter 1993;5:79–82.
[12]TheruvathAJ,SukerkarPA,BaoS,etal.Bonemarrowoedemapredictsbone collapseinpaediatricandadolescentleukaemiapatientswithcorticosteroid- inducedosteonecrosis.EurRadiol2018;28:410–7.
[13]SuganoN,AtsumiT,OhzonoK,etal.The2001revisedcriteriafordiagnosis, classification,andstagingofidiopathicosteonecrosisofthefemoralhead.J OrthopSci2002;7:601–5.
[14]HaYC,JungWH,KimJR,etal.Predictionofcollapseinfemoralheadosteonecro- sis:amodifiedKerboulmethodwithuseofmagneticresonanceimages.JBone JointSurgAm2006;88:35–40.
[15]YamamotoT,IrisaT,SugiokaY,etal.Effectsofpulsemethylprednisolone onboneandmarrowtissues:corticosteroid-inducedosteonecrosisinrabbits.
ArthritisRheum1997;40:2055–64.
[16]MotomuraG,YamamotoT,MiyanishiK,etal.Combinedeffectsofananti- coagulantandalipid-loweringagentonthepreventionofsteroid-induced osteonecrosisinrabbits.ArthritisRheum2004;50:3387–91.
[17]KarasuyamaK,YamamotoT,MotomuraG,etal.Theroleofscleroticchanges inthestartingmechanismsofcollapse:ahistomorphometricandFEMstudy onthefemoralheadofosteonecrosis.Bone2015;81:644–8.
[18]KimHK,SuPH.Developmentofflatteningandapparentfragmentationfollow- ingischemicnecrosisofthecapitalfemoralepiphysisinapigletmodel.JBone JointSurgAm2002;84a:1329–34.
[19]GianakosAL,Moya-AngelerJ,DuggalS,etal.Theefficacyofbisphosphonates withcoredecompressionandmesenchymalstemcellscomparedwithbispho- sphonatesaloneinthetreatmentofosteonecrosisofthehip:aretrospective study.HSSJ2016;12:137–44.
[20]AgarwalaS,JainD,JoshiVR,etal.Efficacyofalendronate,abisphosphonate,in thetreatmentofAVNofthehip.Aprospectiveopen-labelstudy.Rheumatology 2005;44:352–9[Oxford].
[21]KangP,PeiF,ShenB,etal.Aretheresultsofmultipledrillingandalendronate forosteonecrosisofthefemoralheadbetterthanthoseofmultipledrilling?A pilotstudy.JointBoneSpine2012;79:67–72.
[22]IwasakiK,YamamotoT,MotomuraG,etal.Commonsiteofsubchondralinsuf- ficiencyfracturesofthefemoralheadbasedonthree-dimensionalmagnetic resonanceimaging.SkeletalRadiol2016;45:105–13.