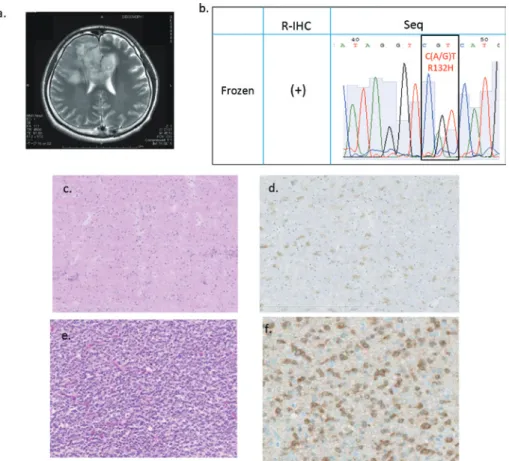
-1 FOR THE INTRAOPERATIVE DIAGNOSIS OF GLIOMAS
10
0
0
全文
(2)
(3)
(4)
(5)
(6)
(7)
(8)
(9)
(10)
図
関連したドキュメント
上海三造機電有限公司 Burmeister & Wain Scandinavian Contractor A/S TGE Marine Gas Engineering GmbH 三井E&S(中国)有限公司.. Mitsui E&S
ー コネクテッド・ドライブ・サービス ー Apple CarPlay プレパレーション * 2 BMW サービス・インクルーシブ・プラス(
[1] Feireisl E., Petzeltov´ a H., Convergence to a ground state as a threshold phenomenon in nonlinear parabolic equations, Differential Integral Equations 10 (1997), 181–196..
By the algorithm in [1] for drawing framed link descriptions of branched covers of Seifert surfaces, a half circle should be drawn in each 1–handle, and then these eight half
Tuncay, Oscillation theorems for a class of second order nonlinear differential equations with damping, Taiwanese Journal of Mathematics, 13 (2009), 1909- 1928..
In [24] he used this, together with Hendriks’ theorem, so show that if the fundamental group of a PD 3 complex splits as a free product, there is a corresponding split of the complex
のようにすべきだと考えていますか。 やっと開通します。長野、太田地区方面
We will give a different proof of a slightly weaker result, and then prove Theorem 7.3 below, which sharpens both results considerably; in both cases f denotes the canonical
