Clinicopathological distinction of two categories of oral squamous cell carcinoma of the tongue: de novo vs. sequential types
8
0
0
全文
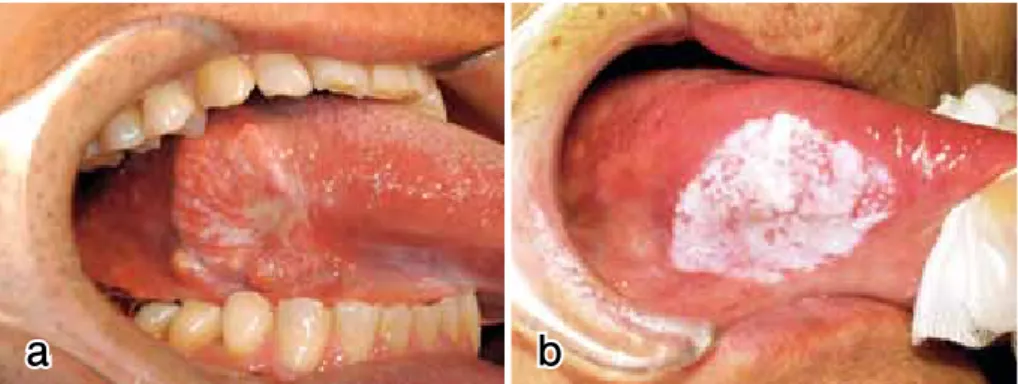
(2) 82 Saito et al. studies and in pathology textbooks, has been its occurrence in older men who drink alcohol and smoke (2-3, 5-8). In recent years, however, we have noticed from our dental hospital services that a special type of oral cancer has been increasing in number, predominantly in older females who lack smoking and drinking habits. Also, contradictory to the established concept of oral cancer mentioned above (9-16), there are often local recurrences as well as multiple occurrences. Typical and conventional oral cancers are presented as indurative masses with exophytic as well as intrinsic growths frequently associated with ulceration (17-19). The other type of oral cancer we have recently noticed tends to be clinically diagnosed as one of three conditions: homo geneous leukoplakia, non-homogeneous leukoplakia with an obscure lesional margin, or erythroplakia (20-22). It is histopathologically characterized as superficial squamous cell carcinoma (SCC), which is usually surrounded by such precursor lesions as carcinoma in-situ (CIS) and epithelial dysplasia (13-16). We wanted to examine such newly recognized types of oral cancer to elucidate if there is any clinicopathological difference between them and conventional and invasive SCCs. In this study, we limited our examination to tongue cancer cases because they are the most frequent among oral cancers in this country as well as in many areas in the world (2-3, 5-7, 23-26) and because we wanted to simplify the comparison between the two types. Using tongue squamous cell carcinoma samples, we analyzed their clinicopathological characteristics to determine whether or not we could estab lish a new disease entity among the oral cancers diagnosed as squamous cell carcinoma. Our approach was different from that of previous trials, in which oral squamous cell carcinomas were categorized by differentiation, malignant potentials, or invasiveness of carcinoma cells (17-18). Instead, we intended to separate at least one particular subtype of oral cancer from the mixture of different subtypes of them to apply appropriate treatment for each type of oral cancer based on more scientific evidence.. Materials and methods Patients and clinical records Cases of primary malignant tumors of the tongue were collected from the patient records of the Department of Oral and Maxillofacial Surgery, Niigata University Hospital, from the 38-year period between 1970 and 2007. The patients’ clinical data included age, sex, tumor location and size, histopathological diagnosis, local recurrence, multiple occurrence, lymph node metastasis, distant metastasis, smoking or alcohol drinking habits, and the use of prosthetic appliances. Tumor size, local recurrence, multiple occur rence, and lymph node metastasis were determined from the case description as well as from actual image records, such as ultrasound (US), computed tomography (CT), and magnetic resonance imaging (MRI). Distant metastases were confirmed by autopsies in some cases, but most were determined by simple radiogram and bone scan. Dental. Two clinicopathological categories of tongue SCC status, such as missing teeth and treatment with crownbridge, was confirmed by panoramic radiographs, while patient denture-wearing status was assessed using clinical records. Detailed smoking and drinking histories, including consumption amounts, frequency of use, and duration, were not obtainable from the patient records, so smoking and drinking were simply counted as habitual or not. Histopathological evaluation Cases definitely diagnosed as SCC were selected, and those with uncertain diagnoses or other types of malignancies, such as salivary or mesenchymal tumors, were excluded. Surgical, biopsy, or autopsy specimens for the cases men tioned above were collected from the surgical pathology files of the Oral Pathology Section, Department of Surgical Pathology, in the same hospital. Hematoxylin and eosin (HE)-stained tissue sections were screened by two patholo gists, independently, for confirming the following character istics: the depth and width of cancerous foci, and the presence of CIS and epithelial dysplasia in their surroundings of SCC. The tongue carcinoma cases were then divided into two groups: conventional invasive SCC without precancerous backgrounds (de novo type), and superficial carcinomas arising from precancerous lesions (sequential type). The diagnoses of CIS and epithelial dysplasia were dependent on criteria proposed by the Working Committee on New Histopathological Criteria for Borderline Malignancies of the Oral Mucosa, the Japanese Society of Oral Pathology (9-10), or by the Oral Pathology Section, Department of Surgical Pathology in the hospital (11-16). Statistical analysis All data were statistically analyzed using Dr. SPSS II for Windows (version 11.0, SPSS Inc., Chicago, IL, USA), a statistical software package. The average score for a patient’s age was calculated using a t test, and the clinicopathological items, such as sex, location, size, local recurrence, multiple occurrence, lymph node metastasis, distant metastasis, tumor type, smoking and drinking habits, and prosthetic appliance usage, were studied using the Chisquare test with Fisher’s exact test. P<0.05 was considered statistically significant.. Results Histopathology There were 119 patients with primary SCC of the tongue. Of the 119 patients, 44 (37.0%) were diagnosed as having conventional invasive SCC without precancerous background (de novo type), and 75 (63.0%) had superficial carcinomas arising from precancerous lesions (sequential type). As shown in Fig. 1a, de novo type cases clinically presented as an indurative mass with exophytic as well as intrinsic growths, frequently associated with ulceration. In contrast, sequential cases were clinically recognized as erythroplakia, homogeneous leukoplakia, or non-homoge neous leukoplakia with obscure lesional margins (Fig. 1b)..
(3) Oral Med Pathol 16 (2012) 83. a. b. Fig. 1. Two different types of squamous cell carcinoma of the tongue: de novo type (a) and sequential type (b). Out of the 119 patients, 44 (37.0%) had conventional invasive carcinomas without precancerous backgrounds (de novo type, a) and 75 (63.0%) had superficial carcinomas arising from precancerous lesions, such as epithelial dysplasia (sequential type). De novo type carcinomas presented as an indurative mass with exophytic as well as intrinsic growth, which was frequently associated with ulceration (b). In contrast, sequential type carcinomas were recognized as homogeneous leukoplakia, erythroplakia, or nonhomogeneous leukoplakia with obscure lesional boundaries (b).. Histologically, the distinction between the de novo type and the sequential type was more conspicuous. In the de novo type, carcinoma cell nests invaded deeply into the muscle layer with extravert and lateral growths. Eventually, the invading front was clearly formed against normal epithelia in the lateral direction, and granulation tissue-like stromal reaction was prominent against the muscle tissue in the deeper direction (Fig. 2a). Since there was no precan cerous lesion around the carcinoma cell nests, their growths were considered to be de novo, which was designated as de novo type. In the sequential type, invasive SCC foci were shown to be located in the central part of the surgically removed specimens, and they were gradually continuous from widespread CIS or dysplastic epithelial lesions in the periphery. When CIS foci in the 75 cases were histologically separated according to the classification by Kobayashi et al. (13), there were 9 basaloid, 4 verrucous and 62 acanthotic types, as multiple CIS foci with different histological types were found in the same case. In addition to the epithelial characteristics, neighboring CIS/dysplastic lesions often. a. accompanied a dense band-like infiltration of lymphoid cells in the subepithelial zone (Fig. 2b). Since this type of carcinoma seemed to arise from the background of its precursor lesions, which could be considered to be sequential, this type of carcinoma was designated as sequential type. Age and sex Out of the 119 patients, 66 were males (55.5%) and 53 females (45.4%) with an overall male-to-female ratio of 1.25:1. Their ages ranged from 21 to 84 years and the average was 59.1 years (male 59.2, female 59.0, respectively). Among the 44 patients with de novo type, there were 28 males (63.6%) and 16 females (36.4%) with a male-tofemale ratio of 1.75:1. In contrast, in the 75 patients with sequential type, there was no difference in gender between 38 males and 37 females (Table 1, Fig. 3). The mean age of the de novo patients was 54.0 years, ranging from 24 to 84 years (male 56.6 years vs. female 49.3 years), while that of the sequential patients was 62.1 years, ranging from 24 to 84 years (male 61.0 years vs. female 63.2. b. Fig. 2. Histological comparison of two different types of squamous cell carcinoma of the tongue: de novo type (a) and sequential type (b). In de novo type carcinomas (a), carcinoma cell nests invaded deeply into the muscle layer with extravert and lateral growths. Eventually, the invading front was clearly formed against normal epithelia in the lateral direction, and granulation tissue-like stromal reaction was prominent towards the muscle tissue in the deeper direction. There were no precancerous lesions around the carcinoma cell nests. In sequential type carcinomas (b), invasive foci appeared to have developed gradually from surrounding precursor lesions, such as carcinoma in-situ (CIS) or epithelial dysplasia. The neighboring CIS/dysplastic lesions were often accompanied with a dense band-like infiltration of lymphoid cells in the subepithelial zone..
(4) 84 Saito et al.. Two clinicopathological categories of tongue SCC Table 1. Clinical summary of squamous cell carcinoma of the tongue by histological types squamous cell carcinoma types P value for clinical matters de novo (n=44) sequential (n=75) difference number ratio number ratio between de novo and sequential of cases (%) of cases (%) sex. male female location lateral sublingual tumor size T1 T2 T3 T4 T1+T2 subtotal T3+T4 subtotal lymph nodes metastasis yes no local recurrences yes no multiple occurrences yes no distant metastasis yes no. 28 16. 63.6 36.4. 38 37. 50.7 49.3. 0.05<. 41 3. 93.2 6.8. 67 8. 89.3 10.7. 0.05<. 13 17 4 10 30 14. 29.6 38.6 9.1 22.7 68.2 31.8. 27 39 4 5 66 9. 36.0 52.0 5.3 6.7 88.0 12.0. 0.05< 0.05< 0.05< <0.02 <0.02 <0.02. 20 24. 45.5 54.5. 12 63. 16.0 84.0. <0.001. 7 37. 15.9 84.1. 11 64. 14.7 85.3. 0.05<. 0 44. 0.0 100.0. 8 67. 10.7 89.3. 0.05<. 4 40. 9.1 90.9. 6 69. 8.0 92.0. 0.05<. years) (Fig. 3). The sequential patients were generally older than the de novo patients, and the difference was statistically significant (P=0.003). Location Both de novo and sequential tumors arose mostly on the lateral margin of the tongue (41 de novo, 93.2% vs. 67 sequential, 89.3%). Among the sequential cases, the sublingual occurrence was more frequent (8, 10.7%) than the de novo (3, 6.8%), although the difference was not statistically significant (Table 1). Size Concerning the TNM clinical staging, 13 de novo (29.6%) and 27 sequential (36.0%) types were categorized as T1; 17 (38.6%) and 39 (52.0%) as T2; 4 (9.1%) and 4 (5.3%) as T3; and 10 (22.7%) and 5 (6.7%) as T4, respectively. When T1+T2 cases were compared with T3+T4 cases, T1+T2 (66, 88.0%) were more common than T3+T4 (9, 12.0%) in sequential patients, while in de novo patients, T3+T4 accounted 31.8% (14 cases) against 68.2% (30 cases) of T1+T2. The difference between the de novo and sequential in terms of these two categorized clinical stages (T1+T2 vs. T3+T4) was statistically significant (P=0.015) (Table 1).. Lymph node metastasis Twenty patients with de novo type (45.5%) had cervical lymph node metastases, while only 12 patients (16.0%) with sequential type did. The difference was statistically significant (P=0.001) (Table 1). Local recurrences Seven patients with de novo type (15.9%) developed local recurrences within 24 months. On the other hand, 11 patients with sequential type (14.7%) developed local recurrences (Table 1). Multiple occurrences Eight patients with sequential type (10.7%) had additional SCC foci in the other sites from their primary ones within the oral cavity, which appeared at the same time and/or in delayed timings. However, no patients with de novo type had multiple foci (Table 1). Distant metastasis Four patients out of the 44 patients with de novo type (9.1%) had distant metastases in the lung (3/4, 75%) and bone marrow (1/4, 25%), while 6 patients with sequential type (8.0%) were shown to have metastatic foci in the lung (3, 50%) as well as in bones (3, 50%). There was no difference in metastatic potential between the two types (Table 1)..
(5) Oral Med Pathol 16 (2012) 85. a. 25. number of patients. 20. 15. 10. 5. 0. b. 20-29. 30-39. 40-49. 50-59 age. 60-69. 70-79. 80-89. 20-29. 30-39. 40-49. 50-59 age. 60-69. 70-79. 80-89. 25. number of patients. 20. 15. 10. 5. 0. Fig. 3. Age and sex distribution of patients with squamous cell carcinoma of the tongue by histological types: de novo type (a) and sequential type (b). Open square ( ), total; closed square ( ), male; dotted square ( ), female. A total of 119 patients with squamous cell carcinoma of the tongue were analyzed in this study. There were 66 male (55.5%) and 53 female (45.4%) patients with an overall male-to-female ratio of 1.25:1. Their ages ranged from 21 to 84 years, and the average was 59.1 years (male 59.2, female 59.0, respectively). There were 44 de novo and 75 sequential carcinomas. Among the 44 patients with de novo type (a), there were 28 males (63.6%) and 16 females (36.4%), with a male-to-female ratio of 1.75:1. In contrast, in the 75 patients with sequential type (b), there was no difference in gender between the 38 males and 37 females. The mean age of the de novo patients was 54.0 years (range 24-84 years; male 56.6 years vs. female 49.3 years), while that of the sequential patients was 62.1 years (range 24-84 years, male 61.0 years vs. female 63.2 years). The sequential patients were generally older than de novo patients, and the difference was statistically significant (P = 0.003).. Prosthetic appliances Dental conditions, such as wearing dentures and crowns and bridges, were compared between the patients with de novo and sequential types, as summarized in Table 2. The dental conditions were categorized into four groups: 1) both dentures and crown bridges; 2) dentures and/or crown bridges; 3) crown bridges and/or dentures; 4) neither dentures nor crown bridges. Group 1 was found in 7 de novo types (25.0%) and in 17 sequential types (44.7%) among. male patients. The difference was not statistically significant. Among the female patients, group 1 was found in 5 de novo types (31.3%) and in 15 sequential types (40.6%). Group 2 was found in 13 de novo types (46.4%) and in 23 sequential types (60.5%) among male patients. Among the females, group 2 was seen in 7 de novo types (43.7%) and in 24 sequential types (64.9%). Group 3 was found in 19 de novo types (67.9%) and in 28 sequential types (73.6%) among male patients. Among the females, group 3 was seen in 12 de. Table 2. Prosthetic appliances among patients with squamous cell carcinoma of the tongue male P value for female prosthetics de novo (n=28) sequencial (n=38) difference de novo (n=16) sequencial (n=37) between de crown/ case case case case novo and dentures % % % % bridges number number number number sequential + + / -. + / + -. 7 13 19 3. 25.0 46.4 67.9 10.7. 17 23 28 4. 44.7 60.5 73.6 10.5. 0.05< 0.05< 0.05< 0.05<. 5 7 12 2. 31.3 43.7 75.0 12.5. 15 24 27 1. 40.6 64.9 73.0 2.7. P value for difference between de novo and sequential 0.05< 0.05< 0.05< 0.05<.
(6) 86 Saito et al.. Two clinicopathological categories of tongue SCC. Table 3. Smoking and alcohol drinking habits among patients with squamous cell carcinoma of the tongue male P value for female habits de novo (n=28) sequencial (n=38) difference de novo (n=16) sequencial (n=37) between de case case case case novo and smoking drinking % % % % number number number sequential number + + / -. + / + -. 17 21 23 1. 60.7 75.0 82.1 3.6. 22 26 30 4. 57.9 68.4 78.9 10.5. novo types (75.0%) and in 27 sequential types (73.0%). Group 4 was found in 3 de novo types (10.7%) and in 4 sequential types (10.5%) among male patients. Among female patients, group 4 was found in 2 de novo types (12.5%) and in one sequential type (2.7%) among the female patients. In terms of prosthetic appliance types, there was no statistically significant difference between histological types both in male and female patients. Smoking and alcohol drinking The relationships between cigarette smoking and alcohol drinking habits were analyzed for gender and histopatho logical types, as summarized in Table 3. Four groups were categorized by the combination of smoking and drinking habits as follows: 1) both smoking and drinking; 2) smoking and/or drinking; 3) drinking and/or smoking; 4) neither smoking nor drinking. Among the male patients, group 1 was seen in 17 de novo types (60.7%) and in 22 sequential types (57.9%) with no difference. In the female patients, group 1 was seen in 5 de novo types (31.3%) and in 1 sequential type (2.7%). The difference between the two types was statistically significant (P=0.007). There was no difference in the group 2 distribution between de novo (21, 75.0%) and sequential (22, 57.9%) types among the male patients. However, in the female patients, group 2 was found in 7 de novo types (43.7%) and 1 sequential type (2.7%), and the difference was statistically significant (P<0.001). Group 3 was found in 23 de novo (82.1%) and in 30 sequential (78.9%) types among the male patients, showing no difference between the two types. In contrast, 7 de novo types (43.7%) were more frequent than 4 sequential types (10.8%) in group 2 female patients, and the difference was statistically significant (P=0.001). Group 4 was seen in 1 de novo (3.6%) and 4 sequential (10.5%) types among the male patients, which showed no difference. However, 7 de novo types (43.7%) were obviously less than 33 sequential type (89.2%) in group 4 female patients, and the difference was statistically significant (P=0.001). The results indicated that the male patients with de novo types had both smoking and drinking habits more frequently than did the female patients of sequential type.. Discussion In this study, we proposed for the first time a new concept of distinction of two types of SCC of the tongue, de novo type and sequential type, based on their clinical and. 0.05< 0.05< 0.05< 0.05<. 5 7 7 7. 31.3 43.7 43.7 43.7. 1 1 4 33. 2.7 2.7 10.8 89.2. P value for difference between de novo and sequential <0.01 <0.001 <0.01 <0.001. histopathological characteristics. SCCs of the tongue have been considered to be one single disease entity, although they are classified due to the degree of differentiation of carcinoma cells (17) or according to their modes of invasion (27). However, these classification systems have been used solely to evaluate individual cases within the one disease entity of SCC. In contrast, the present study has provided new insight concerning the disease entity itself. From both clinical and pathological points of view for its precise treatment, it is now obvious that the sequential type SCC should be separated from conventional and invasive SCC, which we called the de novo type in this study. Clinical and macroscopic characteristics of the sequential type might be summarized as superficial SCCs with white or erosive appearances. According to the surface nature— white, red, or patchy white and red—many of the sequential type SCC cases tended clinically to be diagnosed as socalled homogenous leukoplakia, erythroplakia, or nonhomogenous leukoplakia. Induration of the surrounding mucosa was not conspicuous. At a histopathological level, they were located in the central portion of surgically removed specimens and surrounded by CIS and/or epithelial dysplasia. It is thus reasonable to consider that they arise in the background of CIS and/or epithelial dysplasia. Although no definite description of this kind of oral SCC as a separate disease entity has previously appeared in print, malignant transformed examples of oral leukoplakia have been docu mented in the literature (28-30). Regarding the esophagus, however, there have been some developing concepts similar to ours (31-33). Since the sequential type SCC has now been shown to be always associated with such precursor lesions as CIS and epithelial dysplasia, it seems appropriate to consider the lesion as a lesional complex including different sequential stages from precancerous lesions to franklyinvasive SCC (9-10, 13-15). In contrast, de novo type SCCs could be clinically characterized by their exophytic growth, which was frequently associated with ulceration. They were usually accompanied with induration in the surrounding mucosa. Histopathologically, their proliferation was not only extro vert but also introvert in horizontal and vertical directions into the muscle layer, resulting in fibrous granulation tissue reaction in the invading front, which was considered to be the reason for the induration (34, 35). Thus, there was a clear front formation between the SCC foci and their surrounding normal epithelia in the lateral direction. Granulation tissuelike stromal reactions were prominent towards the muscle.
(7) Oral Med Pathol 16 (2012) 87 tissue in the deeper direction. Since there was no definite association with precancerous lesions around the SCC nests, this type of growth was possibly considered to be de novo. It should be possible to take the de novo type as an advanced stage of the sequential type, because there was a definite difference in the size factor between the two types in the present study. In the present series, however, there was no direct evidence for the sequential precancerous lesions around the de novo type SCC foci, and we have come to use the term de novo for such conventional and invasive SCC cases. The distinction of the two types was also supported by another clinical characteristic. The patients with sequential type were more prevalent among older females than were those with de novo type. The fact that such a definite tendency in gender and age distribution of the sequential type exists must be emphasized, because the conventional wisdom is that oral cancer tends to occur in the males in their sixth and seventh decades (1-4). Based on the present results on the location of lesions, most of the cases were found in the lateral margin of the tongue, which was also the case in most previous studies (18, 19). Accordingly, we investigated the relationship between dental conditions and the other variables. Although there was a tendency that prosthetic-appliance wearers were more frequently found among the female patients with sequential type SCC, there were no significant differences in terms of different status of wearing prosthetic appliances between the two types. It is, therefore, necessary to analyze dental conditions from different aspects and in greater detail, looking at such factors as occlusional changes due to attrition, missing of teeth, dentition, ill-fitting dentures, broken teeth, or xerostomia, which are associated with or without aging, because there have been no actual investi gations performed along these lines (7, 8, 36). Smoking and drinking have been believed to be dependently and synergistically associated with an increased risk of oral cancer (24-26, 37-40), and the risk tends to increase with increased frequencies of exposure to smoke and alcohol, as well as with amounts of consumption (33, 41-42). However, in the present study, interestingly, the prevalence of smoking and drinking habits in the female patients with sequential type SCC was significantly lower than in their male counterparts, or in the patients with de novo type SCC. Therefore, it is obvious that smoking and drinking were not risk factors for the female patients with sequential type SCC. In conclusion, the distinction of the two different disease categories of squamous cell carcinoma of the tongue, de novo and sequential, among the Japanese population has been disclosed by the present study. In order to provide better clinical intervention, clinicians, healthcare providers, and pathologists should pay greater attention to the sequential type SCC, which tends to arise in older female individuals who neither smoke and nor drink alcohol, and which tends to recur and occur in multiple sites.. Acknowledgments This study was supported in part by Grants-in-Aid for Scientific Research from the Japan Society for the Promotion of Science.. References 1. Statistics and Information Department, the Minister’s Secretariat, Ministry of Health, Labor and Welfare, Health and Welfare Statistics Association. Vital Statistics of Japan 2005. Yamatosogo Publishing, Tokyo, 2005; 292-307. 2. Moore SR, Johnson NW, Pierce AM, et al. The epidemiology of mouth cancer: a review of global incidence. Oral Dis 2000; 6: 65-74. 3. Moore SR, Johnson NW, Pierce AM, et al. The epidemiology of tongue cancer: a review of global incidence. Oral Dis 2000; 6: 75-84. 4. Su WZ, Tohnai I, Kawamura T, et al. Trends in site-specific mortality from oral and pharyngeal cancer among Japanese males, 1950-94. Oral Oncol 1999; 35: 9-16. 5. Sawair FA, Al-Erynani K, Al-Surhy A, et al. High relative frequency of oral squamous cell carcinoma in Yemen: qat and tobacco chewing as its aetiological background. Int J Environ Health Res 2007; 17: 185-95. 6. Mathew Iype E, Pandey M, Mathew A et al. Squamous cell carcinoma of the tongue among young Indian adults. Neoplasia 2001; 3: 273-7. 7. Gorsky M, Silverman S. Denture wearing and oral cancer. J Prosthetic Dent 1984; 52: 164-6. 8. Lockhart PB, Norris CM Jr, Pulliam C. Dental factors in the genesis of squamous cell carcinoma of the oral cavity. Oral Oncol 1998; 34: 133-9. 9. The Working Committee on New Histopathological Criteria for Borderline Malignancies of the Oral Mucosa, The Japanese Society for Oral Pathology. Guidelines for histopathological diagnosis of borderline malignancies of the oral mucosa. A Preliminary Proposal 2005. Yamazaki Publishing, Niigata, 2005. 10. The Working Committee on New Histopathological Criteria for Borderline Malignancies of the Oral Mucosa, The Japanese Society for Oral Pathology. Oral Carcinoma inSitu (JSOP) Catalog, Histopathological Variations. Sunashobo Publishing, Tokyo, 2007. 11. Syafriadi M, Cheng J, Jen KY, et al. Two-phase appearance of oral epithelial dysplasia resulting from focal proliferation of parabasal cells and apoptosis of prickle cells. J Oral Pathol Med 2005; 34: 140-9. 12. Syafriadi M, Ida-Yonemochi H, Ikarashi T, et al. Carcinoma in-situ of the oral mucosa has definite tendency towards keratinization. Oral Med Pathol 2003; 8: 43-4. 13. Kobayashi T, Maruyama S, Cheng J, et al. Histopathological varieties of oral carcinoma in situ: Diagnosis aided by immunohistochemistry dealing with the second basal cell layer as the proliferating center of oral mucosal epithelia. Pathol Int 2010; 60: 156-66. 14. Funayama A, Cheng J, Maruyama S, et al. Enhanced expression of podoplanin in oral carcinomas in situ and squamous cell carcinomas. Pathobiology 2011; 78: 171-80. 15. Mikami T, Cheng J, Maruyama S, et al. Emergence of.
(8) 88 Saito et al.. Two clinicopathological categories of tongue SCC. keratin 17 vs. loss of keratin 13: Their reciprocal immuno histochemical profiles in oral carcinoma in situ. Oral Oncology 2011; 47: 497-503. 16. Alvarado CG, Maruyama S, Cheng J, et al. Nuclear translocation of β-catenin synchronized with loss of E-cadherin in oral epithelial dysplasia with a characteristic two-phase appearance. Histopathology 2011; 59: 283-91. 17. Johnson N, Franceschi S, Ferlay J, et al. Squamous cell carcinoma. In: Barnes L, Eveson JW, Reichart P, Sindransky D, eds. WHO Classification of Tumours, Pathology and Genetics of Head and Neck Tumours. IARC Press, Lyon, 2005; 168-75. 18. Shafer WG, Hine MK, Levy BM, Tomich CE. Malignant tumors of epithelial tissue origin. A Textbook of Oral Pathology. WB Saunders Company, Philadelphia, 1983; 110-37. 19. Pindborg JJ, Reichart PA, Smith CJ, et al. Histological Typing of Cancer and Precancer of the Oral Mucosa. Springer, New York, 1997. 20. Waldron CA, Shafer WG. Oral carcinoma in situ. Oral Surg Oral Med Oral Pathol 1975; 39: 227-38. 21. Lumerman H, Freedman P, Kerpel S. Oral epithelial dysplasia and the development of invasive squamous cell carcinoma. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1995; 79: 321-9. 22. Weijers M, Snow GB, van der Waal JE, et al. The clinical relevance of epithelial dysplasia in the surgical margins of tongue and floor of mouth squamous cell carcinoma: an analysis of 37 patients. J Oral Pathol Med 2002; 31: 11-5. 23. Haya-Fernandez MC, Bagan JV, Murillo-Cortes J, et al. The prevalence of oral leukoplakia in 138 patients with oral squamous cell carcinoma. Oral Dis 2004; 10: 346-8. 24. Andrea J, Schulten EA, Kostense PJ, et al. Tobacco and alcohol related to the anatomical site of oral squamous cell carcinoma. J Oral Pathol Med 1993; 22: 459-62. 25. Barasch A, Morse DE, Krutchkoff DJ, et al. Smoking, gender, and age as risk factors for site-specific intraoral squamous cell carcinoma. A case-series analysis. Cancer 1994; 73: 509-13. 26. Castellsague X, Quintana MJ, Martinez MC, et al. The role of type of tobacco and type of alcoholic beverage in oral carcinogenesis. Int J Cancer 2004; 108: 741-9. 27. Yamamoto E, Kohama G. Mode of invasion, bleomycin sensitivity and clinical course in squamous cell carcinoma of the oral cavity. Cancer 1983; 15: 2175-80. 28. Haya-Fernandez MC, Bagan JV, Murillo-Cortes J, et al. The prevalence of oral leukoplakia in 138 patients with oral squamous cell carcinoma. Oral Dis 2004; 10: 346-8. 29. Hseu SS, Wabg WC, Chen CH, et al. Malignant Received November 11, 2011. transformation in 1458 patients with potentially malignant oral mucosal disorders: a follow-up study based in a Taiwanese hospital. J Oral Pathol Med 2007; 36: 25-9. 30. Schepman KP, van der Meij EH, Smeele LE, et al. Malignant transformation of oral leukoplakia: a follow-up study of a hospital-based population of 166 patients with oral leukoplakia from the Netherlands. Oral Oncol 1998; 34: 270-5. 31. Takubo K, Aida J, Sawabe M et al. Early squamous cell carcinoma of the oesophagus: the Japanese viewpoint. Histopathology 2007; 51: 733-42. 32. Kanamoto A, Yamaguchi H, Nakanishi Y, et al. Clinico pathological study of multiple superficial oesophageal carcinoma. Brit J Surg 2007; 87: 1712-5. 33. Lewin KJ, Appelmen HD. Superficial squamous cell carcinoma. Atlas of Tumors of the Esophagus and Stomach. Armed Forces Institute of Pathology, Washington DC, 1995; 58-63. 34. Ikarashi T, Ida-Yonemochi H, Oshiro K, et al. Intraepithelial expression of perlecan, a basement membrane-type heparan sulfate proteoglycan reflects dysplastic changes of the oral mucosal epithelium. J Oral Pathol Med 2004; 33: 87-95. 35. Ahsan MS, Yamazaki M, Maruyama M, et al. Differential expression of perlecan receptors, α-dystroglycan and integrin β1, before and after invasion of oral squamous cell carcinoma. J Oral Pathol Med 2011; 40: 552-9. 36. Velly AM, Franco EL, Schlecht N, et al. Relationship between dental factors and risk of upper aerodigestive tract cancer. Oral Oncol 1998; 34: 284-91. 37. Morse DE, Psoter WJ, Cleveland D, et al. Smoking and drinking in relation to oral cancer and oral dysplasia. Cancer Causes Control 2007; 18: 919-29. 38. Franceschi S, Talamini R, Barra S, et al. Smoking and drinking in relation to cancers of the oral cavity, pharynx, larynx, and esophagus in northern Italy. Cancer Res 1990; 50: 6502-7. 39. Blot WJ, McLaughlin JK, Winn DM, et al. Smoking and drinking in relation to oral and pharyngeal cancer. Cancer Res 1988; 48: 3282-7. 40. De Stefani E, Boffetta P, Oreggia F, et al. Smoking patterns and cancer of the oral cavity and pharynx: a case-control study in Uruguay. Oral Oncol 1998; 34: 340-6. 41. Zheng T, Holford T, Chen Y, et al. Risk of tongue cancer associated with tobacco smoking and alcohol consumption: a case-control study. Oral Oncol 1997; 33: 82-5. 42. Dahlstrom KR, Little JA, Zafereo ME, et al. Squamous cell carcinoma of the head and neck in never smoker-never drinkers: A descriptive epidemiologic study. Head Neck 2008; 30: 75-84. Accepted January 5, 2012.
(9)
図

関連したドキュメント
Neovastat (AE-941) in refractory renal cell carcinoma patients: report of a phase II trial with two dose levels. Phase I/II trial of the safety and efficacy of shark cartilage in
学位授与番号 学位授与年月日 氏名
Recently, we reported that the CSC markers epithelial cell adhesion molecule (EpCAM) and CD90 are expressed independently in primary HCCs and cell lines, and CD90 + cells share
10 Ma tsud a S, e t a l: Comparison of transthoracic esophag ecto my with de fin itiv e chemoradio the rapy as initia l trea tmen t for pa tien ts with e sophagea l squamous cell ca
Suppose the group A possesses a nice subgroup G of countable length equipped with a valuation produced by the restricted height valuation on A such that A/G is a weakly n-summable
If Φ is a small class of weights we can define, as we did for J -Colim, a2-category Φ- Colim of small categories with chosen Φ-colimits, functors preserving these strictly, and
This conjecture is not solved yet, and a good direction to solve it should be to build first a Quillen model structure on the category of weak ω-groupoids in the sense of
Kwak, J.H., Kwon, Y.S.: Classification of reflexible regular embeddings and self-Petrie dual regular embeddings of complete bipartite graphs. Kwon, Y.S., Nedela, R.: Non-existence
