( g,T,3kYO, ,W, 2ii;l, ,Med,,8,o,il )
A Research Report Supported by Yayoi Yoshioka Award
ATRIAL NATRIURETIC PEPTIDE LEVELS AND ITS MOLECIULAR
FORM IN HUMAN CARDIAC TESSUE
Kiyoko NARUSE, Michiaki HIROEi), Mitsuhide NARUSE, Makoto NAGATA2),
Akimasa HASHIMOT03), Hitoshi KOYANAGI3), Morie SEKIGUCHI2),
Hiroshi DEMURA, Koushichiro HIROSAWA2)
and Kazuo SHIZUME
Department of Medicine, Institute of Clinical Endocrinology, i)Department of Radiology, 2)Department of Medicine, and 3)Department of Surgery, The Heart Institute of Japan,
Tokyo Women's Medical College
(Received March, 22th 1989)
Abstract
We investigated the levels and molecular form of atrial naturiuretic peptide (ANP) in human atrial tissue obtained frorn six autopsied patients without heart disease and 31 patients during
heart surgery. The levels of atrial ANP and its
three major variants -cr-hANP, B-hANP, and
7-hANP- were determined by a combination of
radioimmunoassay and high-performance gel
per-meation chromatography. The levels of right
atrial ANP were significantly higher in patients with mitral disease (12.2 ± 2.50 ptg/mg protein)
than that in the autopsy group or the patients with aortic disease, or atrial septal defect. These increased ANP levels were mainly accounted for by an increase in B-hANP. Both total ANP and
B-hANP levels in the right atrium correlated with the presence of atrial fibrillation and with right atrial, pulmonary arterial, and pulmonary capil-lary wedge pressures.
These results suggest that human atrium
responds to an imposed hemodynamic overload by
increasing ANP production and by a shift to the B-hANP form. This -dimeric peptide could be used
as a marker indicating adaptation to chronic pathologic conditions.
Introduction
The recent discovery of atrial natriuretic
poly-peptides (ANP) in human atrial tissue spurred
many studies, which have made it clear that the heart is a part of the endocrine system involved in the maintenance of body-fluid homeostasis (for review, see refereneesi}N4)>. ANP acts to correct
disturbances in body fluid volume and blood
pressure through potent natriuretic, diuretic, and vasodilator effects, and also by interacting with other regulatory system such as the renin-angiotensin-aldosterone system5)N8) and vasopres-sin9)lo).
Atrial ANP has been reported to be composed of
at least three major components: 7-human ANP
(7-hANP), a 126-amino-acid peptide; a-human ANP (a-hANP), a 28-amino-acid residue of the
carboxy-terminal of xhANP; and B-hANP, which is an
antiparallel dimer of cr-hANPii)i2). The
compo-nents 7-hANP and cr-hANP have been
charac-terized respectively as a prohormone and a major secretory form. The pathophysiologic significance
of B-hANP, which has a unique structure and a biologic activity different from or-hANP in its dura-tion and magnitudei2), is not known.
The present study was undertaken to
inves-tigate the biochemical changes in ANP production
in overloaded heart and the pathophysiologic significance of the different ANP molecular forms, especially B-hANP. We measured the levels of
total immunoreactive ANP and its moiecular
autopsy and open heart surgery.
Methods
Tissue collectionHuman right and/or left atrial tissues were
obtained at autopsy from six patients with a mean
age of 60 ± 3 years, who died of noncardiac
disease: a 61-year-old man with thyroid and
esophageal cancer, 52-year-old and 70-year-old
men with esophageal cancer, a 53-year-old man
with liver cirrhosis, a 64-year-old man with lung cancer, and a 68-year-old man with a dissecting
aneurysm, respectively. None of them had left
ventricular hypertrophy as judged from electro-cardiograms and/or chest radiographs. All autop-tic specimens were obtained within 3 hours after death.
Surgical specimens were obtained at the time of open heart surgery from 31 patients. The mitral disease group consisted of nine patients: six with
predominant mitral stenosis and three with
predominant mitral regurgitation. These patients ranged in age from 46 to 63 years with a mean age
of 55 ± 2 years. The group with aortic valve disease consisted of eight patients, ranging in age from 34 to 68 years with a mean of 51 ± 5 years. Seven had aortic regurgitation and one had aortic
stenosis. The group with atrial septal defect
(ASD) consisted of seven patients, ranging in age from 19 to 61 years with a mean of 43 ± 6 years. Surgical specimens were also obtained from seven patients with miscellaneous cardiac diseases (left atrial aneurysm, tetralogy of Fallot with atrial
septal defect, congenital pulmaonary stenosis with ventricular septal defect, ventricular septal defect, endocardial cushion defect, tricuspid re-gurgitation, and left atrial myxoma) (Table 1). A small portion (approximately 5 mg) of the
right atrial appendage was incised during
can-nulation for cardiopulmonary bypass. A small amount of the left atrial appendage was also
trimed in some patients to provide access to the mitral valve according to routine operative
pro-cedure and to prevent postoperative thrombus
formation. The tissues obtained were immediately
frozen and stored at -800C until extracted.
Blood samples were also obtained from a
peripheral vein in some of the patients before
cardiac surgery. Blood samples were collected in chilled tubes containing sodium
ethylenediamine-tetraacetate (Na2EDTA) (4 mM) and aprotinin
(500 kallikrein inactivator units/ml). The samples
were separated by centrifugation at 40C, and
plasma was stored at -700C until assayed.
Extraction of ANP
Atrial ANP was extracted in 1 M acetic acid containing 20 mM HCI after boiling for 10 min. Tissues were homogenized with a Polytron
hom-ogenizer (Brinkman Company, Westbury, NY),
centrifuged at 15,OOO g for 60 min at 40C, and the
clear supernatant was stored at -300C until
subjected to radioimmunoassay (RIA) or chro-matography.
Plasma ANP was extracted by the method
described previouslyi3}. In brief, 1 ml of each plasma was first acidified with acetic acid and then applied to a Sep-Pak Cis (Waters Associates, Milford, MA) cartridge. The adsorbed peptide was eluted with 2 ml of a mixture of acetonitrile and O.4% acetic acid (3:2). The eluates were evapo-rated, lyophilized, dissolved in the assay buffer,
and subjected to RIA or to the following
chro-matographic procedure.
High-performance gel permeation
chro-matography (HP-GPC)
Immunoreactive ANP components of a different molecular weight wefe separated and determined
by a combination of RIA and HP-GPC using a
TSK-GEL G2000 SW column (7.5 × 600 mm; Toyo Soda, Tokyo). The column was eluted with 10 mM trifluoroacetic acid containing O.2 M sodium chloride and 30% acetonitrile as a solvent at a flow rate of O.3 ml/min. Under the conditions
em-pioyed, the retention times of the standard
sub-stances used for molecular weight calibration
were as follows: 43.7 ± O.1 niin for bovine serum albumin, 48.2 ± O.1 min for carbonic anhydrase, 55.8 ± O.1 min for cytochrome C, 67.6 ± O.3 min
for synthetic B-hANP (Protein Research
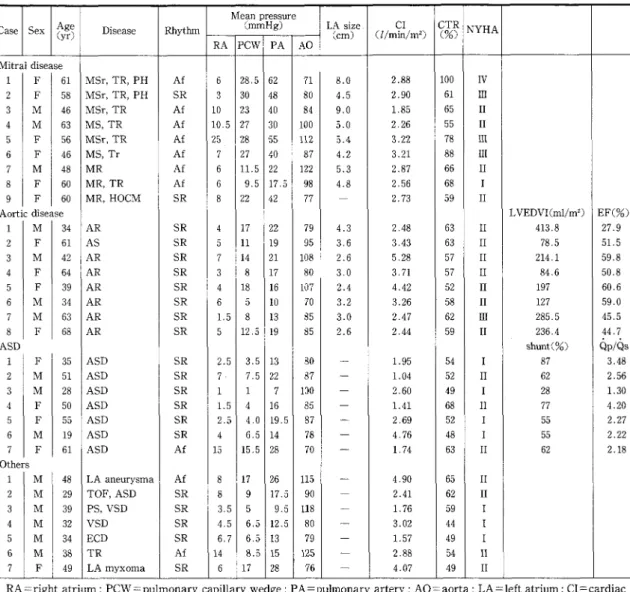
Table 1 Clinical characteristics and hemodynamic variables
Case Sex Age Disease Rhythm
Mean (mmHg)pressure LAsize. (cm) CI (llminlm2) CTR(%)
NYHA
(yr)RA
PCW
PA AO Mitraldisease 1 F 61 MSr,TR,PH Af 6 28,5 62 71 8.0 2.88 100 IV 2 F 58 MSr,TR,PH SR 3 30 48 80 4.5 2.90 61 III 3M
46 MSr,TR Af 10 23 40 84 9.0 1.85 65 II 4M
63MS,TR
Af 10.5 27 30 100 5.0 2.26 55 II 5 F 56 MSr,TR Af 25 28 55 1!2 5.4 3,22 78 lll 6 F 46 MS,Tr Af 7 27 4e 87 4.2 3,21 88 III 7M
48MR
Af 6 11.5 22 122 5.3 2,87 66 II 8 F 60MR,TR
Af 6 9.5 17.5 98 4.8 2,56 68 I 9 F 60MR,HOCM
SR 8 22 42 77-
2,73 59 IIAorticdisease LVEDVI(ml/m2) EF(%)
1
M
34AR
SR 4 17 22 79 4.3 2.48 63 II 413,8 27.9 2 F 61 AS SR 5 11 19 95 3,6 3.43 63 II 78.5 51,5 3M
42AR
SR 7 14 21 108 2.6 5.28 57 II 214.1 59,8 4 F 64AR
SR 3 8 17 80 3.0 3,71 57 II 84.6 50.8 5 F 39AR
SR 4 18 16 107 2.4 4,42 52 II 197 6e.6 6M
34AR
SR 6 5 10 70 3.2 3.26 58 II 127 59.0 7M
63AR
SR L5 8 13 B5 3,O 2.47 62 llI 285.5 45,5 8 F 68AR
SR 5 12.5 19 B5 2.6 2.44 59 II 236.4 44,7 ASD shunt(O/.) QplQs 1 F 35 ASD SR 2.5 3.5 13 80T
1.95 54 I 87 3.48 2M
51 ASD SR 7・ 7,5 22 87-
1,e4 52 II 62 2.56 3M
28 ASD SR 1 1 7 100-
2,60 49 I 28 1.30 4 F 50 ASD SR L5 4 16 85-
1.41 68 II 77 4.20 5 F 55 ASD SR 2,5 4.0 19,5 87-
2.69 52 I 55 2.27 6M
19 ASD SR 4 6.5 14 78-
4.76 48 I 55 2.22 7 F 61 ASD Af 15 15.5 28 70-
1.74 63 II 62 2.18 Others 1M
48 LAaneurysma Af 8 17 26 115-
4.90 65 II 2M
29 TOF,ASD SR 8 9 17.5 90-
2.41 62 II 3M
39 PS,VSD SR 3.5 5 9.5 118"
1.76 59 I 4M
32 VSD SR 4.5 6,5 12.5 80 rm 3.02 44 I 5M
34 ECD SR 6,7 6.5 13 79-
1.57 49 I 6M
38TR
Af 14 8.5 15 125L
2.88 54 II 7 F 49LAmyxoma
SR 6 17 28 767
4.07 49 IIRA ==right atrium ; PCW=pulmonary capillary wedge ; PA=pulmonary artery ; AO=aorta ; LA= left atrium ; CI=cardiac index ; CTR-cardiothoracic ratio ; NYHA=New York Heart Association ; MSr =:mitral stenosis with mild mitral regur-getation ; TR== tricuspid regurregur-getation ; PH --pulmonary hypertension ; MS=mitral stenosis ; Tr=imild tricuspid
regurgeta-tion; MR=mitral regurgetaregurgeta-tion; HOCM=hypertrophic obstructive cardiomyopathy; AR=aortic regurgetaregurgeta-tion; AS=
aortic stenosis ; ASD=atrial septal defect ; TOF=tetralogy of Fallot ; PS=pulmonary stenosis, VSD=ventricular septal
defect; ECD==endocardial cushion defect; Af=:atrial fibrillation; SR=sinus rhythm; LVEDVI=left ventricular
end-diastolic volume index ; EF=ejection fraction ; QpfQs=ratio of pulmonary to systemic blood flow.
(Protein Research Foundation), and 82.4 ± O.1 min
for angiotensin I. The eluates was evaporated,
lyophilized, dissolved in the assay buffer, and subjected to RIA.
Radioimmunoassay of ANP
Immunoreactive ANP was determined by the
RIA method as described previouslyi3) except for
the anti-ANP antiserum. In brief, a-hANP was
radioiodinated by the chloramine-T method, and the iodinated tracer was purified by high-per-formance liquid chromatography on a ptBondapak Cis column (Waters Associates, Milford, MA). The antiserum used in this study was raised in New Zealand white rabbits using or-hANP as antigen'`).
It was used at a final dilution of 1:4 × 10`, yielding a maximum binding of approximately 35% of the
quantity of i25I-ANP. The crossreactivity with
a-rat ANP and B-hANP was 16% and 90% on a molar
basis, respectively. The crossreactivity with
an-giotensin II, arginine vasopressin, ACTH,
so-matostatin, vasoactive intestinal peptide, and
thyroglobulin was less than O.OOOI%.
The assay buffer in RIA was O.1 M Tris acetate,
pH 7.4, containing O.1% bovine serum albumin
(Amersham, Arlington Heights, IL) and 1 mM
Na2EDTA. The RIA incubation mixture consisted Table 2 Atrial and plasma ANP levels
AtrialANP(#g/mgprotein)
Patients Rightatrium Leftatrium
PlasmaANP
(pg/ml)Total 7-hANP S-hANP a-hANP Total 7-hANP fi-hANP
a-hANP
Autopsy 1.5e O.84 1,23 2.82 O.95 2,99 3.54 8.46 17,6 10,0 25.9 9.22 14,8 17.9 2.66 O.89 1.31 O.42 2,13 O.09 O.17 5.87 10.3 4,O 1.91 O.51 O.78 1.94 O.90 28.8 8.15 1.33 1.02 1.06 O.78 O,64 2.27 1,14 O.55 1.10 I,40 0,20 O.32 3,13 1,33 2.48 1.57 1.21 O.45 2.45 1.50 O,71 O.56 0.97 O.31 O.59 O.04 O.08 e.56 1,17 3.53 1,29 O.35 O.59 O.13 O.65 1.89 1.07 O.47 O.38 O.87 O.40 O.52 1.02 0,32 O.20 O.10 1.06 O.34 2.64 O,30 6,6I 14.6 7.48 22.7 8.18 11.5 13.7 1.62 0.25 O.14 O.07 1.32 O,02 O.05 4.63 8.87 O.16 e.4o O.15 O.10 1.64 O.12 23.4 4.54 O.80 0.42 O.19 O,11 O.05 O,68 O.02 O.03 O.Ol O.02 O.07 n,d, n.d. n.d. n.d. n.d. n.d. n,d. n,d. n.d. 0.05 O.02 O,04 O.Ol n.d. 0.01 e.o2 O.11 n,d. e.os O.15 0.01 O,04 O.03 O.04 O,52 e,49 n,d. 0.04 O,02 O.07 O.02 O,14 1.69 1.15 1.50 4.18 3.77 3.18 O.36 9.15 3.23 I,94 10,O 1.83 5.04 9,39 r---"-"--O.I2-2.13 O.72 O.43 O.94 1.81 2.24 1.21 O.28 1.08 O,21 0.29 O.29 O,20 O,35 1.68 O.95 O,43 0.19 1.95 1.23 1,25 o.e3 7,48 2.69 1.34 9.01 1.51 4.2I 6.60 n,d, O.14 O.19 O,13 O.13 O.17 O.03 n.d. n.d. n,d. n.d, n.d. n,d. 0.56 rm
of 100 pt1 of standard or-hANP, 100 pt1 of diluted antiserum (1:8,OOO), 100 pt1 of i25I-a-hANP (ap-proximately 10,OOO cpm) and 200 ptl of the assay buffer. The mixture was incubated for 24 h at 40C.
Antibody-bound and free tracer peptide were
separated by the addition of anti-rabbit
immu-noglobulin antiserum (1:20), normal rabbit serum
(1:200), and 15% polyethylene glycol in assay
buffer. The sensitivity of the RIA was 2 pg/tube, with 50% displacement at 30 pg/tube.
Protein concentration
The protein cencentration of the extract was measured by the Bradford dye-binding methodi5)
using crystalline bovine serum albumin as a
standard.
Cardiac catheterization
Right-sided and left-sided cardiac catheteriza-tion were performed with a No. 7F thermodilucatheteriza-tion
Swan-Ganz catheter (Edwards Laboratories,
Santa Ana, CA), which was inserted into the right internal jugular vein or the antecubital vein for right-sided catheterization, and the radial or fem-oral artery for left-sided catheterization. All
pressures -mean right atrial, mean pulmonary arterial, mean pulmonary capillary wedge, and mean aortic- were measured in each position.
Other hemodynamic parameters measured
in-cluded heart rate, cardiac index, left ventricular end-diastolic volume index, and ejection fraction (in patients with aortic disease), and left-to-right shunt and the ratio of pulmonary to systemic
blood flow (Qp/Qs ratio) (in patients with ASD).
Cardiac output was determined by thermodilu-tion. In addition, left atrial size was assessed by echocardiography using either the M-mode
echo-cardiographs or a two-dimentional estimate. Statistical analysis
Data are expressed as micrograms per
mil-ligram protein (mean ±SE), and were analyzed by
an unpaired and/or paired t-test. Regression analyses employed the linear and multivariate
least squares methods. Differences between
groups were considered to be significant at
P<O.05.
Results
The clinical characteristics and various hemo-dynamic data of each patient are shown in Table 1 and are in summarized in table 3. Seven of the nine patients with mitral disease also had atriai fibrillation. All except one (for whom data were not available) had left atrial enlargement accord-ing to echocardiography (in our laboratory, a value greater than 3.0 cm is considered enlarged). The right atrial pressure, pulmonary capillary wedge pressure, and/or mean pulmonary arterial pres-sure were elevated in most of the patients with mitral disease. The left ventricular end- diastolic volume index (204.6 ± 39.6 ml/m2 body surface area) was elevated and the ejection fraction (49.9 ± 3.8%) was abnormally low in patients with
aortic valve disease. The left-to-right shunt was 60 ± 6% and the Qp/Qs ratio (2.57 ± O.31) was
significantly elevated compared with normal
values (less than 1.5) in patients with ADS. As shown in Table 3, the pulmonary capillary
wedge pressure and pulmonary arterial pressure were significantly higher in patients with mitral disease than in patients with aortic disease or
ASD. In addition, although the cardiothoracic ratio (CTR) determined from chest radiographs
was abnormally high in all three cardiac disease groups, it was significantly higher in patients with mitral disease than in the other two groups. The atrial levels of total ANP and of its molec-ular variants are shown in Table 2. Right atrial
ANP levels were determined in all 31 patients
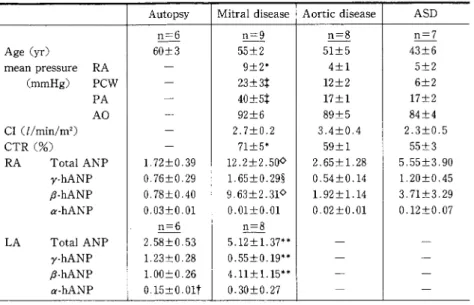
examined. As summarized in Table 3, the atrial total ANP level in mitral disease was 12.2 ± 2.50 ptg/mg protein, which was significantly higher
than in the autopsy, aortic disease, and ASD groups. Of the miscellaneous cardiac disease
group, the patient with left atrial aneurysm had the highes・t atrial ANP levels.
Immunoreactive ANP in the atrial tissue
con-sisted of three major components. The first major peak was located at the elution position of cyto-chrome C with a molecular weight of 12.6 kilo-daltons, and was regarded as 7-hANP. The second
Table 3 Summary of the clinical, hemodynamic data and atrial ANP levels Autopsy Mitraldisease Aorticdisease
ASD
Age(yr) rneanpressureRA
(mmHg)PCW
PA
AO
CI(llmin/m2) CTR(O/.)RATotalANP
v-hANPP-hANP
a-hANPLATotalANP
7-hANPP-hANP
cr-hANPn=6
60±3 n==9 55±2 9±2. 23±3t 40±5t 92±6 2.7±O.2 71±5. 12,2±2,50e 1,65±O,29g 9.63±2.31Q O.Ol±O.Ol n=8 5.12±1.37-. O.55±O.19** 4.11±1.15** O.30±O.27n=8
51±5 4±1 12±2 17±1 89±5 3.4±O,4 59±1 2.65±1.28 O,54±O.14 1.92±1.14 O.02±O.Ol ---rn=7
43±6 5±2 6±2 17±2 84±4 2.3±O.5 55±3 5,55±3,90 1.20±0,45 3,71±3.29 O.12±O,07-m--Values are the means±SE. ANP levels are expressed as "gfmg protein, 'p<O.05 1 tp<O,O05 vs corresponding values in aortic disease and ASD. gp<O.05 i ep<O,Ol vs corresponding values in autopsy,
tp<O.05 i "p<O.Ol vs corresponding right atrial values. Abbreviations as in Table 1,
and third major peaks were located at the elution posi・tions of synthetic B-hANP and a-hANP, re-spectively. In the patients studied, atrial tissue always contained 7-hANP or B-hANP as the pre-dominant variant (Fig. IA, B).
The atrial 7-hANP level in the mitral disease group was 1.65 ± O.29 ptg/mg protein, which was significantly higher than in the autopsy and aortic disease groups (Table 3). The atrial B-hANP level in mitral disease was about 12 times higher than in the autopsy group. Atrial 6-hANP levels in the
aortic disease and ASD groups were not signi-ficantly different from those in the autopsy group.
Immunoreactive ANP corresponding to a-hANP
was not detected in most of the patients with mitral disease. In addition, there was no signifi-cant difference in atrial a-hANP levels among the different disease states. On the whole, total ANP levels in the right atrium showed a significant
correlation with B-hANP levles (r=O.992,
P<O.OOI).
ANP levels in the right atrium did not differ from those in left atrium in the autopsy group. In
ISO e n e loo 2g : 50 (A)' gk il
-a
zz
rt qt ==t
:・ " " 2・i III
(B)2:
i:- E. {・ {・SII l Iii
tooo 7soB
e
-a va 50o az
(
250 O 3o 4o so 6o 7o so go 3o 4o so 6o 7o eo go O Retention time{min> Retention tlrne(min)Fig. 1 Representative HP-GPC gel filtration patterns of immunoreactive ANP from human atrial tissue (A) y-hANP-predominant type (patient 3 of the autopsy group). (B) B-hANP-predominant type (patient 4 of the
mitral disease group),
the mitral
atrium had
disease group, however, the
significantly higher levels of right
ANP, 7-hANP, and B-hANP than the left atrium. In addition, the plasma ANP level determined
from seven mitral disease patients was 131 ± 33.9
pg/ml, which is significantly higher than the
normal value for healthy subjects as found in our laboratory (22 ± 5 pg/ml).
Various clinical features were examined to
ascertain which had contributed to the increase of atrial total ANP and each ANP variant. When the subjects were divided into two groups on the basis
? 30 :. 9 4 a E -a 3 2o se y s S S 10 ・E-E RHYTHM o
-o
.oo
: . . ;o
fotaL B-hANP lbtat B-hANP
hANP hANP
SR Af
(n=21) (n=10)
Fig. 2 RelationshipsbetweenrightatrialtotalhANPand
B-hANP levels and cardiac rhythm
Abbreviations as in Table 1. Mean is shown by bar, e : mitral disease, O: aortic disease, A: ASD, A: others.
tP<O.OOI vs corresponding values in patients with SR,
s
L* :
L*
:4:
-th
d ? 30 t's
J9 2o Sa : 10 t CTR gi
: . . s .-*
i o . N : : . -!-* . Ro
Totat B-hANP lbteL B-hANP
hANP hANP
E60ete 60eie<
(n=17) <n=14>
Fig. 3 RelationshipsbetweenrightatrialtotalhANPand B-hANP levels and CTR
Abbreviations as in Table 1. Mean is shown by bar. O: mitral disease, O: aortic disease, A: ASD, A: others, EP<O.Ol vs corresponding values in patients with CTR less than 60%,
of either age (more than 50 and less than 50 years old) or clinical severity according to the New York
Heart Association (NYHA) classification, no
statistically significant differences in atrial ANP levels were found. In contrast, the presence of atrial fibrillation (Fig. 2) and an increased CTR (Fig. 3) correlated respectiveiy with increased levels of total ANP and of B-hANP.
Of the various hemodynamic parameters, right atrial ANP levels showed a significant positive correlation with the right atrial pressure (r= O.654, p<O.OOI) (Fig. 4), pulmonary arterial pres-sure (r==O.468, P<O.Ol), and pulmonary capillary wedge pressure (r=O.447, P<O.O05). B-hANP levels also showed a similar positive correlation with these hemodynamic parameters (Fig. 5). In addi-tion, the presence of atrial fibrillaaddi-tion, elevated
rt 3o g 4 g -a-:. 20 :. E i :pt 10 E . s
I・
.o
O 10 20 30
Righ± atriaL pressure (mmHg)
Fig. 4 Relationships between right atrial total hANP
levels and right atrial pressure
e: mitral disease, O: aortic disease, A: ASD, A:others.
Regression line calculated by least squares analysis.
O ..o: 4: rt 3o 6.de -,k i' 2o
E
l iO ,T' o . o : . i t': . .e lo 2e 3o
Right etriat pressure CmmHg)
Fig. 5 Relationships between right atrial B-hANP levels
and right atrial pressure
e: mitral disease, O: aortic disease, A: ASD, A: others. Regression line calculated by least squares analysis.
pulmonary arterial pressure, and elevated CTR
correlated with the right atrial 7-hANP levels. Although right atrial ANP levels tended to cor-relate negatively with cardiac index, the relation was not statistically significant. There was no significant correlation between right atrial ANP levels and mean arterial pressure.
In contrast to the right atrial ANP levels, left atrial ANP levels did not correlate significantly
with any of the hemodynamic parameters inves-tigated. Although the left atrial ANP levels tended to show even a negative correlation with left atrial size, the relation was not statistically significant.
Discussion
The present study demonstrates that the atrial ANP levels are markedly elevated in patients with
mitral disease compared to patients with
non-cardiac disease, aortic disease, or ASD. Atrial pressure, which has been reported to be an im-portant factor regulating ANP secretioni6)Ni8), was significantly elevated in mitral disease but not in aortic disease or ASD. Therefore, we suggest that the increased atrial ANP levels could be the result of increased atrial pressure. The finding that
plasma ANP levels were also elevated suggests
that increased atrial pressure stimulates atrial production of ANP in mitral disease.
This conclusion is further supported by the
strong correlation observed between atrial ANP levels and right atrial pressure. We also found a less prominent but significant correlation of right
ANP levels with pulmonary arterial pressure
(r=O.468, P<O.Ol) and pulmonary capillary wedge
pressure (r=O.447, P<O.O05), suggesting that pressures in these areas could also stimulate
production of ANP in the right atrium. This
possibility is supported by findings of increased plasma ANP levels in hypoxia-induced pulmonary hypertension in ratsi9) and in patients with congen-ital pulmonary disease20}. In addition, we recently reported that plasma ANP levels correlate with
pulmonary arterial pressure in patients with
angina pectoris2i), which suggests that pulmonary arterial pressure may have some role in
modula-ting ANP secretion in certain pathologic states. The existence of vagal afferent fibers arising from
the nerve endings near the pulmonary
capil-laries22) indicates that central nervous system
mediated reflexes might be involved in the in-teraction between pulmonary arterial pressure
and ANP secretion. However, there is a significant correlation among right atrial, pulmonary
arte-rial, and pulmonary capillary wedge pressures, which can obviously be attributed to the
back-ward effect of the increased left atrial pressure. The correlation of right atrial ANP levels with
pulmonary arterial and pulmonary capillary
wedge pressures, therefore, may only reflect this pressure relation.
Another factor that correlates with increased right atrial ANP levels is the presence of atrial
fibrillation. Both fixed and paroxysmal atrial fibrillation is known to be associated with an increased plasma ANP levelsi3)23)24). It is possible that atrial fibrillation stimulates the production of ANP in the atrium as well as its secretion. Among the patients in this study, atrial fibrillation was mainly observed in patients with mitral disease, in whom atrial pressures are increased. In addi-tion, patient 7 with ASD and patient 1 with a left atrial aneurysm, who had the highest atrial ANP levels in their respective disease groups, exhibited both elevated atrial pressure and atrial fibrilla-tion. Therefore, it cannot be excluded that creased atrial ANP levels are related to the in-creased atrial pressure rather than to the presence of atrial fibrillation. Of the patients with mitral regurgitation, however, patients 7 and 8, who had atrial fibrillation, showed atrial ANP levels
sev-eral times higher than in patient 9, who had regular sinus rhythm, although atrial and
pul-monary arterial pressures were more elevated in patient 9 than in patients 7 and 8. This finding gives further support to the notion that atrial fibrillation is one of the important conditions
affecting ANP production. We cannot conclude
from the present study, however, whether atrial fibrillation itself can stimulate ANP production in the absence of chronically increased atrial
pres-sure, nor can we suggest the mechanism by which
this irregular movement of atrial wall might
affect ANP production.
The finding in patient 6 with tricuspid regur-gitation is interesting. Although this patient had increased atrial pressure and atrial fibrillation,
atrial ANP levels were no higher than in the
autopsy group. At least two possible explanations for this finding must be considered. First,
monary capillary wedge pressure and/or
pul-monary arterial pressure (which were in the
normal range in this patient) may be more critical than right atrial pressure in stimulating right
atrial ANP production. However, in our series ANP ieveis correlated most strongly with right
atrial pressure. An alternative explanation
in-volves the duration of increased right atrial pressure. In our mitral disease group, the duration of the disease estimated from the history ranged from 8 months to 36 years, with an average of 17 years. Although there was no direct correlation between the duration and the ANP levels, patient
9 who had the shortest duration also had the
lowest atrial ANP levels, and patient 5 who had the longest duration had the highest atrial ANP ieveis. The duration of disease in the patient with tricuspid regurgitation -estimated at 3 years from the history- might be too short to induce increased atrial ANP levels.
The clinical severity of congestive heart failure was determined according to the NYHA Funcional
Classification, which has been reported to cor-relate with plasma ANP levels25}"'27). Eight patients
fell in class I, 18 in class II, 4 in class III, and 1 in
class IV. Although the atrial ANP level in the class III and IV patients (9.02 ± 3.60 ptg/mg protein) was higher than in the class Iand II patients (5.09 ± 1.43 ug/mg protein), the difference was not sta-tisticaily significant. The reason for the
discre-pancy with the previous studies25)'J27) is not
known. However, in the present study,
classifi-cantion according to NYHA was determined
within 1 week before the heart surgery, and
therefore could have been influenced by
treat-ments including medication, and restriction of
diet and excercise since admission to the hospital.
The immunoreactive ANP in our specimens
comprised three major components corresponding
to 7-hANP, B-hANP, and or-hANP, in agreement with previous findingsii)i2). In the autopsy group, who died of noncardiac disease, atrial 7-hANP and B-hANP levels were almost identical, and the a-hANP level was much lower. In contrast, in eight of the nine patients with mitral disease, atrial
ANP was composed mainly of B-hANP. B-hANP
was also the predominant molecular form in the atrium of the patients with other cardiac diseases in whom atrial ANP levels were high: patients 4, 7, and 8 with aortic disease, patient 7 with ASD, and the patient with a left atrial aneurysm. There was a significant correlation between total ANP
and B-ANP levels. Furthermore, 6-hANP levels correlated with the same clinical feature and hemodynamie variables as the total ANP levels
-the presence of atrial fibrillaiton, and right atrial, pulmonary arterial, and pulmonary capil-lary wedge pressures. These results indicated that B-hANP becomes the main molecular form of ANP in chronically overloaded hearts.
6-hANP, an antiparallel dimer of a-hANP, was
reported to have a biological activity different from a-hANP. Its natriuretic activity is weaker but longer-lasting than that of a-hANP, whereas its hypotensive effect is comparabie to that of ev-hANPi2}. Such a dimeric peptide with bioactivity has never been found in the tissue of any other animal species. How and why B-hANP is increased
in the chronically overloaded atrium is not
known. However, it seems improbable that
B-hANP is produced from two a-B-hANP molecules,
since the disulfide linkage between the two cys-teine residues at positions 7 and 23 is chemically stable. Therefore, we suggest that the dimeric form may be generated before the disulfide linkage is formed in the or-hANP molecule- i.e., early in ANP processing. If so, we predict the presence of
an immunoreactive ANP with higher molecular
weight than y-hANP. Consistent with this hy-pothesis, we have sometimes found on HP-GPC a very small peak of immunoreactive ANP with an
apparent molecular weight of 25,OOO daltons, although further studies are required to elucidate the nature of this high-moleuclar-weight ANP.
It has been reported the B-hANP is rapidly converted to a-hANP in the plasma28)29). It is not known, however, whether B-hANP itself is also
secreted into the circulation. We have compared
the molecular form of atrial ANP with that of
plasma in seven patients with mitral disease in
whom a B-hANP was the predominant molecular
form in the atrium. In six of the seven patients,
B-hANP was present as a minor component in
addition to a-hANP in the plasma. Thus, all the
patients with B-hANP in their plasma also had B-hANP in their atrial tissue29).
We recently reported the molecular form of
plasma ANP before and after atrial pacing at 150 beats/min for 30 min in two patients with sick
sinus syndrome29). Plasma ANP was increased
significantly by atrial pacing, and the increase involved B-hANP as well as cr-hANP. In addition, B-hANP has been found in the plasma of patients with renal and heart disease30). Taken together, these results suggest that B-hANP is secreted into the circulation under certain conditions. 6-hANP
could be a precursor substance that quickly
supplies two molecules of a-hANP, or it might exhibit unique biological activities without being
converted to or-hANP. Whichever its mode of
action, an increase in B-hANP may mark
adap-tation to a chronic hemodynamic overload.
ANP is also produced in the left atrium.
Although both right and left atrial pressures were elevated above normal to a'similar extent in the mitral disease group, right atrial ANP levels were two times higher than in the left atrium. Fur-thermore, left atrial ANP levels did not correlate with any of the factors that correlated with right atrial ANP levels. It is noteworthy that not even pulmonary capillary wedge pressure or left atrial size correlated with left atrial ANP level. In fact, there was an insignificant negative correlation between left atrial size and left atrial ANP level (r= -O.469). The exact explanation for this finding is not known. However, it can be anticipated that
histologic deterioration and fibrosis of the tissue may be more prominent in the left atrium than in the right atrium in mitral disease in which left atrial pressure is primarily increased. Extensive tissue destruction may reduce the number of the atriocytes that produce ANP.
Another factor that should be taken into
ac-count is the difference of the conditions under which the left and right atrial tissue specimens
were taken. The right atrial appendage was
trimmed during cannulation for cardiopulmonary bypass, whereas the left atrial appendage was trimmed after the completion of the
cardiopul-monary bypass. Accordingly, the hemodynamic
conditions could be quite different when the left atrial tissue was obtained, and the value of
cor-relating left atrial ANP levels with the
hemo-dynamic variables determined before surgery may be limited.
It has been reported that normal rat ventricle can adapt to an imposed systoilc load by
decreing the proportion of Vi isomyosin and the as-sociated ATPase activity, resulting in a lower
velocity of muscle shortening and probably a more
energy-efficient contraction3i). More recent
studies32)33) have found that human atrial tissue, which is biochemically similar to rat ventricle in isomyosin distribution, has a similar capacity to alter the ratio of Vi to V3 isomyosins in response to hemodynamic loads. The increase in ANP and its
molecular shift to B-hANP could be another
adaptation performed by the atrial tissue in the pressure/volume overloaded heart. In contrast to the myosin isozymes34), changes in ANP molecular form may reflect hemodynamic overload of longer duration (although this will not necessarily hold in advanced stages of cardiac disease, as seen in the left atrium in our mitral disease group). Taken together, these findings lead to the intriguing hypothesis that human atrial tissue adapts to overload conditions through two dif-ferent mechanisms-an increase in ANP
produc-tion accompanied by a shift to the B-hANP form,
and changes in isomyosin distribution. The
the peripheral tissues, whereas the isomyosin
ratio affects the heart directly. In addition, our findings give further support to the clinical im-portance of performing a biochemical analysis of the atrial tissue specimen to evaluate the bio-chemical adaptation of the failing heart, although more comparative studies of biopsied atrial tissue are needed.
Acknowledgement
The authors thank Dr. M. Takeishi and the staff of
the Department of Pathology I and Dr. A. Kajita and the
staff of the Department of Pathology II, Tokyo Women's
Medical College for their assistance in obtaining autoptic
tissue specimens and Ms. Fumiko Numata and Ms. Yuko
Kato for their able technical assistance.
This work was supported in part by a Grant-in-Aid for Scientific Research of the Yayoi Yoshioka Award, a
Grant-in Aid for Scientific Research from the Ministry of
Education, Science, and Culture, Japan, and by a research grant from the Foundation for Growth Science
in Japan.
References
1) Cantin M, Genest J: The heart and the atrial uretic factor. Endocrine Rev 6: 107-127, 1985
2) Cole BR, Needleman P: Atriopeptins; velume regulatory hormones, Clin Res 33: 389-394, 1985
3) DeBold AJ: Atrial natriuretic factor: a hormone
produced by the heart. Science 230: 767--770, 1985
4) Laragh JH: Atrial natriuretic hormone, the
aldosterone axis, and blood pressure-electrolyte eostasis. N Engl J Med 313: 1330-1340, 1985
5) Burnett JC Jr, GrangerJP, Opgenorth TJ: Effects
of synthetic atrial natriuretic factor on renal function and renin release. Am J Physiol 247: F863-F866, 1984
6) Maack T, Marion DN, Camargo MJF et al: Effects
of auriculin (atrial natriuretic factor) on blood pressure,
renal function, and the renin-aldosterone system in dogs. Am J Med 77: 1069-1075, 1984
7) Atarashi K, Mulrow PJ, Franco-Saenz R et al: Inhibition of aldosterone production by an atrial
extract. Science 24: 992-994, 1984
8) Kudo T, Baird A: Inhibition of aldosterone production in the adrenal glomerulosa by atrial natriuretic factor.
Nature 312: 756-757, 1984
9) Samson WK: Atrial natriuretic factor inhibits
dration and hemorrhage-induced vasopressin release, Neuroendocrinology 40: 277-279, 1985
10) Obana K, Naruse, M, Inagami T et al: Atrial
natriuretic factor inhibits vasopressin secretion from
rat posterior pituitary, Biochem Biophys Res Commun 132: 1088-1094, 1985
11) Kangawa K, Matsuo H: Purification and complete amino acid sequence of a-human atrial' natriuretic polypeptide (a-hANP). Biochem Biophys Res Commun 118: 131-139, 1984
12) Kangawa K, Fukuda A, Matsuo H: Structural identification of beta- and gamma-human atrial
uretic polypeptides (B- and 7-hANP). Nature 313: 397-400, 1985
13) Naruse M, Naruse K, Obana K et al:
tive a-human atrial natriuretic polypeptide in human plasma. Peptides 7; 141-145, 1986
14) Yoshinaga K, Yamaguchi K, Abe K et al: mination of atrial natriuretic polypeptide (ANP) in human plasma. Biomed Res 7: 173-179, 1986
15) Bradford MM: A rapid and sensitive method for the
quantitation of microgram quantities of protein ing the principle of protein-dye binding. Ann Biochem
72: 248-254, 1976
16) Dietz JR: Release of natriuretic factor frorn rat
lung preparation by atrial distension. Am J Physiol 247: RI093--RI096, 1984
17) Lange RE, Th61ken, H, Ganten D et al: Atrial
natriuretic factor-a circulating hormone stimulated by volume loading. Nature'314: 264-266, 1985
18) Sato F, Kamoi K, Wakiya Y et al: Relationship
between plasma atrial natriuretic peptide levels and
atrial pressure in man. J CIin Endocrinol Metab 63: 823-827, 1986
19) Mckenzie JC, Tanaka T, Inagami T et al:
tions in atrial and plasma atrial natriuretic factor (ANF)
content during development of hypoxia-induced
monary hypertension in the rat. Proc Sco Exp Biol Med
181: 459-463, 1986
20) Lang RE, Unger T, Ganten D et.al: a-atrial
natriuretic peptide concentrations in plamsa of children with congenital heart and pulmonary diseases, Br MedJ
291: 1241, 1985
21) Naruse K, Naruse M, Honda T et al: Atrial
triuretic peptide correlates with pulmonary arterial pressure and cardiac output. Peptides 8: 285-290, 1987 22) Paintal AS: Mechanism of stimulation of type J monary receptors. J Physiol 203: 511-532, 1969
23) Yamaji T, Ishibashi M, Nakaoka H et al: Possible
role for atrial natriuretic peptide in polyuria associated
with paroxysmal atrial arrhythmia. Lancet i: 1211, 1985 24) Roy D, Paillard F, Cassidy D et al: Atrial natriuretic factor during atrial fibrillation and supraventricular tachycardia. J Am Coll Cardial 9: 509-514, 1987
25) Nakaoka H, Imataka K, Amano M et al: Plasma
levels of atrial natriuretic factor in patients with
congestive heartfailure. N Engl J Med 313: 892-983, 1985
26) Shenker Y, Sider RS, Ostafin EA et al: Plamsa
levels of immunoreactive atrial natriuretic factor in
healthy subjects and in patients with edema. J CIin Invest 76: 1684-1687, 1985
Plasma atrial natriuretic peptide in cardiac disease and during infusion in healthy volunteers. Lancet ii:66−69,
1985
28)Itoh H, Nakao K, Shiono S et a1:Conversion ofβ一
human atrial natriuretic polypeptide intoα一human
atrlal natriuretic polypeptide in human plasma in vitro.
Biochem Biophys Res Commun 143:560−569,1987 29)Naruse M, Naruse K, Hifumi S et al:Molecular
heterogeneity of immunoreactive ANP in human
plasma. Biologically active atrial peptides. ASH sym−
posium series 2:183−186,1988
30)Miyata A, Toshimori T, Hashiguchi T et al:
Molecular forms of atrial natriuretic polypeptides cir−
culating in human plasma. Biochem Biophys Res Commun l42:461−467,1987
31)Mercadier JJ, Lompre AM, Wisnewsky C et ah
Myosin isoenzymatic changes in several models of rat
cardiac hypertrophy. C重rc Res 49:525−532,1981
32)Gorza L, Mercadier JJ, Schwartz K et al:Myosin types in the human heart. An immunofluorescence
study of normal and hypertrophied atrial and ventri−
cular myocardium. Circ Res 54:694−702,1984 33)Yazaki Y, Tsuchimochi H, Kuroo M et al:Dis・ tribution of myosin isozymes in human atrial and
ventricular myocardium:comparison in normal and
overloaded heart. Eur Heart∫5(suppL F):103−110,1984
34)Buttr韮ck PM, Malhotra A, Brodman R et al: Myosin isoenzyme distribution in overloaded human
atrial tissue. Circualtion 74:477−483,1986