Necrotizing Fasciitis of an Upper Extremity Starting as Pyogenic Flexor Tenosynovitis with a Horseshoe Appearance in the Hand: A Case Report
4
0
0
全文
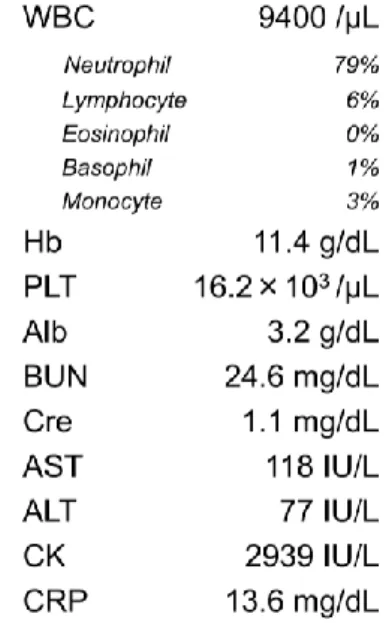
(2) Japanese Journal of Trauma and Emergency Medicine (Jpn J of Trauma & Emerg. Med.) Copyright © 2010 by The East Japanese Society for Trauma and Emergency Medicine Vol. 3 No. 2 Printed in Japan. Figure 1: Appearance of the left hand on arrival. The whole hand was swollen, especially the thumb and little finger.. Figure. 2:. Three. separate. incisions in the thumb (1), little finger (2), and the wrist (3). Bloody bullae were seen on the thumb, the little finger, and the thenar eminence.. Figure 3: Six months after the initial. debridement.. The. patient could use a pen with satisfactory flexion of the fingers.. induced asthma and colon cancer, which was. subcutaneous gas could be found in hand. surgically. No. radiographs. His condition was diagnosed as. medications were prescribed including steroids. pyogenic flexor tenosynovitis, and he was. for asthma. He had no predisposing factors for. admitted to our hospital 14 hours after onset of. infection such as smoking, diabetes mellitus, nor. the symptoms.. removed. two. years. before.. immunosuppression.. After a few hours of hospitalization, diffused. His temperature was 40.1 degrees Celsius.. blister, bloody vesicles and bullae rapidly formed. Blood pressure was 118/52 mmHg and pulse rate. on the thumb, thenar eminence, hypothenar. was 108 per minute. No obvious wounds could be. eminence, and little finger. Although the initial. found on his left arm. The left thumb and little. diagnosis was pyogenic flexor tenosynovitis, the. finger were markedly swollen with positive. rapid progression of erythematous margin up to. Kanavel’s. the distal forearm prompted the possibility of. four. cardinal. signs. (Figure. 1).. Laboratory data are shown in Table 1. No. necrotizing. 52. fasciitis.. A systemic. antibiotics. Jpn J of Trauma & Emerg. Med. 2012; 3(2); 51-54.
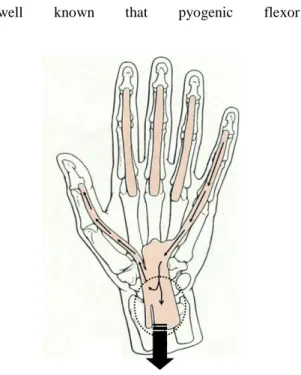
(3) Japanese Journal of Trauma and Emergency Medicine (Jpn J of Trauma & Emerg. Med.) Copyright © 2010 by The East Japanese Society for Trauma and Emergency Medicine Vol. 3 No. 2 Printed in Japan. therapy with 4.5 g/day of piperacillin-tazobactam. differ by a few percentages between the upper and. and 1800 mg/day of clindamycin were started. lower extremities; Mortalities of necrotizing. empirically, and emergency surgical debridement. fasciitis in the upper extremities and in the lower. was performed at 17 hours from the onset.. extremities are 50% and 46%, respectively.. Three separate incisions were made in the. Necrotizing fasciitis affecting a limb is, therefore,. thumb, the little finger, and from the distal. an emergency that requires prompt recognition. forearm to the wrist (Figure 2). Subcutaneous. and aggressive excision of affected tissues.. tissue was edematous and a large area of. Survival rate sharply declines with a delay in. antebrachial fascia of the flexors was necrotic.. surgery of more than twenty-four hours. The carpal tunnel was released for prevention of. case, we operated on the patient within 24 hours. carpal tunnel syndrome and debridement of the. after the onset with good result.. fascia was performed in the distal one-third of the. [7]. . In our. It is always difficult to decide to what extent a. forearm.. surgeon should perform debridement in severe. The antibiotics were switched. to 6 g/day of. soft tissue infection such as gas gangrene and. ampicillin and 1800 mg/day of clindamycin after. necrotizing fasciitis. It was decided not to explore. the surgery because Group A Streptococcus. the index, middle, and ring fingers based on the. (GAS) was confirmed by culture of the patient’s. distribution of the symptoms. The point of this. blood and excised tissue. Though systemic. case was that pain, swelling, and bullae formation. infectious condition was well controlled with. were mostly localized to the thumb and the little. intravenous antibiotics therapy, the pulp of the. finger, which implied a horseshoe abscess. It is. thumb and the whole little finger became necrotic.. well. known. that. pyogenic. flexor. A second surgery, amputation of the little finger and a kite flap from the index finger to cover the thumb pulp, was performed 25 days after the first surgery. The patient was discharged from the hospital on the day 73. Hand therapy was continued in the outpatient clinic. The patient regained satisfactory hand function without recurrence of infection at the latest follow-up (Figure 3).. Discussion Although 80% of necrotizing fasciitis occurs in the extremities, only 10.1% occurs in the upper extremities. [7]. .. And, while there is a significant. Figure 4: Schema of the anatomy of the synovial bursae and progression of the infection.. difference in the prevalences, mortalities only. 53. Jpn J of Trauma & Emerg. Med. 2012; 3(2); 51-54.
(4) Japanese Journal of Trauma and Emergency Medicine (Jpn J of Trauma & Emerg. Med.) Copyright © 2010 by The East Japanese Society for Trauma and Emergency Medicine Vol. 3 No. 2 Printed in Japan. tenosynovitis. sometimes. progresses. to. a. 1995;221(5):558-63; discussion 563-5.. horseshoe abscess. The reason for this progression is the existence of communication between. 3. Childers BJ, Potyondy LD, Nachreiner R,. synovial bursae. In 70% of individuals, synovial. Rogers. bursa of the thumb (radial bursa) and the little. Hendricks DL, Hardesty RA. Necrotizing. finger. fasciitis: A fourteen-year retrospective study. (ulnar. mid-palmar. bursa). bursa. connect. [8]. .. through. Therefore,. the. pyogenic. of. tenosynovitis of the thumb can easily spread to. FR,. 163. Childers. ER,. consecutive. Oberg. patients.. KC,. Am. Surg;68(2):109-16.. the little finger and vice versa. We assumed that pyogenic tenosynovitis of the thumb or the little. 4. Patel RR, Younai S, Narayanan K, Wahba H,. finger had progressed to a horseshoe abscess and. Stofman. finally to necrotizing fasciitis of the antebrachial. fasciitis of the hand: case report . Clin Infect. fascia through the Parona’s space. [9]. (figure 4).. GM.. Necrotizing. streptococcal. Dis. 1996;22(3):586-7.. Based on this assumption, we decided to explore only the thumb and the little finger, and not the. 5. Lesaffer J, Van Holder C, Haeck L. Necrotizing. other fingers. We believe that limiting the area of. fasciitis of the first ray caused by group A. debridement minimized the damage to the other. streptococcus.. fingers and our patient’s hand function could be. 2006;31(3):317-9.. J. Hand. Surg. Br.. spared. We reported a successful management of a case. 6. Tang WM, Ho PL, Fung KK, Yuen KY, Leon. of necrotizing fasciitis in an upper extremity that. JC. Necrotizing fasciitis of a limb. J Bone. started as a pyogenic flexor tenosynovitis. Joint Surg Br. 2001; 83: 709-14. showing a horseshoe appearance in a hand. We showed the possibility of treating the necrotizing. 7. Wong CH, Chang HC, Pasupathy S, Khin LW,. fasciitis with limited debridement based on its. Tan JL, Low CO. Necrotizing fasciitis:. pathoanatomy in detail.. clinical. presentation,. microbiology,. and. determinants of mortality. J Bone Joint Surg. References. Am. 2003;85-A(8):1454-60.. 1. P. Jarrett, M. Rademaker, M. Duffill. The 8. Jebson PJ. Deep subfascial space infections.. clinical spectrum of necrotizing fasciitis. A. Hand Clin. 1998;14(4):557-66.. review of 15 cases. Aus NZ J Med 1997;27(1):29-34.. 9. Hans-Martin Schmidt, Ulrich Lanz. Surgecal anatomy of the hand. Stuttgart, Germany:. 2. McHenry CR, Piotrowski JJ, Petrinic D,. George Thieme Verlag; 2004. p.26.. Malangoni MA. Determinants of mortality for necrotizing soft-tissue infections. Ann Surg. 54. Jpn J of Trauma & Emerg. Med. 2012; 3(2); 51-54.
(5)
図

関連したドキュメント
This study examined the influence of obstacles with various heights positioned on the walkway of the TUG test on test performance (total time required and gait parameters)
ABSTRACT XX Background. Pseudomesotheliomatous carcinoma of the lung ) PMCL * is characterized by diffuse pro- gression along visceral pleura, and has been confirmed histologically as
Tsujimoto, Yuichi; Satoh, Mototaka; Takada, Tsuyoshi; Honda, Masahito; Matsumiya, Kiyomi;. Fujioka, Hideki;
patient with apraxia of speech -A preliminary case report-, Annual Bulletin, RILP, Univ.. J.: Apraxia of speech in patients with Broca's aphasia ; A
Keywords: homology representation, permutation module, Andre permutations, simsun permutation, tangent and Genocchi
Lemma4.1.. This is not true if f is not positively homogeneous as the following example shows.. Let f be positively homogeneous. We shall give an example later to show that
When S satisfies the Type II condition, N is closed under both ordinary matrix product and Hadamard (entry-wise) product, and N becomes a commutative algebra (with unity element)
We show that a discrete fixed point theorem of Eilenberg is equivalent to the restriction of the contraction principle to the class of non-Archimedean bounded metric spaces.. We
