A Clinicopathologic Study of Breast Cancer
Patients during Pregnancy
Kotaro Iijima,
Masataka Yoshimoto,
Jun Horiguchi,
Tetsunari Oyama,
Yasuo Morishita,
Fujio Kasumi
and Goi Sakamoto
Background & Aims: The purpose of this study was to investigate the influence of pregnancy on breast cancer prognosis by analyzing clinical and pathological features of young patients with breast cancer in relation to last birth. M ethod: A total of 622 young breast cancer patients under 35 years of age undergoing surgical treatment between 1960 and 1990 at Cancer Institute Hospital were included in this study. The patients were classified into four groups; group A patients who were diagnosed during pregnancy or within one year after delivery,group B patients who were diagnosed from one to three years after delivery, group C patients who were diagnosed three years or more after delivery, and group D patients who were nulliparous. All four groups were examined from the viewpoint of clinical and pathological findings with regard to age, disease duration, first childbirth, clinical stage, histopath-ological type, lymph node metastasis, and survival. Furthermore, nuclear grade and immunohisto-chemical staining of both estrogen receptor (ER) and factor-VIII were examined in early-stage breast cancer patients. Result : The incidence of early-stage(0,I and II) breast cancer was significantly(p< 0.05) lower in group A (69%) than in groups C (88%) and D (85%). The incidence of nodal involve-ment decreased from group A (61%), B (59%), C (51%) to D (43%) in that order. The incidence of nodal involvement in group D was significantly (p<0.05) lower than that in groups A and B. The positive rate of estrogen receptor increased from group A (50%), B (56%) to C (72%) in that order. Disease-free survival was significantly (p<0.05) more favorable in group D than in groups A and C. The similar result was obtained in patients with clinically early-stage breast cancer. Conclusion : Patients who developed breast cancer during pregnancy or within less than one year postpartum have a poor prognosis among patients under 35 years old. Patients having no childbirth history generally have a high risk factor of developing breast cancer,however,breast cancer patients without childbirth history under 35 years old result in a favourable prognosis.(Kitakanto Med J 2006;56:93∼99)
Key Words: Breast cancer, pregnancy, young women, estrogen receptor, prognosis
Introduction
Breast cancer is the most common disease in women when categorized by the affected organs. Some reports have been published that breast cancer during pregnancy has a poor prognosis. The reasons for this are the delay in detection due to breast develop-ment in pregnancy and the impact of the hormone
environment of pregnancy on breast cancer. In the past,breast cancer associated with pregnancy was treat-ed as advanctreat-ed breast cancer. In recent years, how-ever,breast cancer during pregnancy is generally treat-ed in the same way as ordinary breast cancer and continuation with pregnancy is promoted.
The type of breast cancer during pregnancy that is likely affected by pregnancy varies in definition, but
1 Department of Thoracic and Visceral Organ Surgery,Gunma University Graduate School of Medicine,Maebashi,Gunma 371-8511,Japan 2 Department of Breast Surgery,Cancer Institute Hospital,Tokyo 135-8550 Japan 3 Department of Breast Pathology, Cancer Institute Hospital, Tokyo 135-8550, Japan 4 Department of Tumor Pathology , Gunma University Graduate School of Medicine, Maebashi, Gunma 371-8511, Japan
Received : January 16, 2006 Accepted : January 24, 2006
Address: KOTARO IIJIMA Department of Thoracic and Visceral Organ Surgery,Gunma University Graduate School of Medicine3-39-22 Showa-machi, Maebashi, Gunma 371-8511, Japan
tions were involved in the calculation, the differences between institutions in treatment and diagnosis would make it difficult to obtain meaningful results. There-fore, a large number of breast cancer patients from a single medical institution should be used in order to investigate the correlation between pregnancy and childbirth, and the clinicopathological factors which might influence the impact of pregnancy on breast cancer.
Patients and M ethods
The subjects of this study included 622 breast cancer patients aged 35 or less out of 8,780 primary breast cancer patients who received surgical treatment between 1960 and 1990 at the Cancer Institute Hospi-tal. These patients were classified into four groups by pregnancy and childbirth history: group A patients who had been pregnant or were less than one year postpartum at the time of surgery(49 patients, 7.9%), group B patients who were one year or more but less than three years postpartum prior to surgical treatment
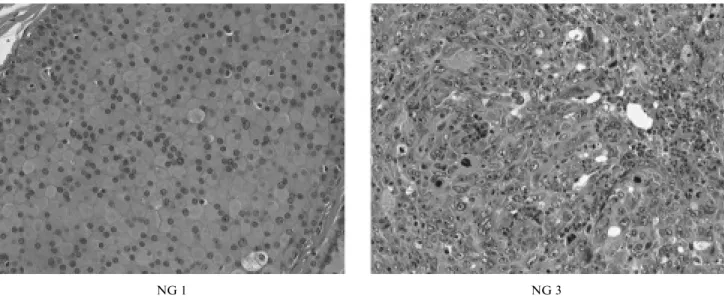
Using hematoxylin and eosin (HE) staining speci-mens, NG was determined by nuclear atypia and mitotic counts (Figure 1).
Nuclear atypia: Score 1; nuclei were uniform and chromatin were not prominent,Score 3; nuclei varied in size and had prominent irregularities in form, and Score 2; between scores 1 and 3.
Mitotic counts: Observation was made of tumor cells at a high magnification. Score 1; less than five mitoses in 10 high-magnification fields,Score 3; 11 or more mitoses in 10 high-magnification fields,Score 2; between scores 1 and 3.
Calculation of NG : The scores for nuclear atypia and mitotic counts were added. Tumors were classified into three categories according to the added scores, NG1; three points or less, NG2; four points, and NG3; five points or more.
Immunohistochemical staining
Using formalin-fixed and paraffin-embedded spec-imen, a thinly sliced specimen (4μm) was placed on a
Figure 1 Histological nuclear grade
Nuclear grade (NG) was determined using the HE stain slides. Shown on the left was NG 1. Nuclei were relatively uniform and few mitoses were seen. On the right was NG 3.Size of nuclei was random and mitoses prominently increased.
silane-coated slide glass. After deparaffinization, it was treated for 30 minutes in 0.3% hydrogen peroxide and rinsed using 10mM phosphate-buffered saline (PBS). For antigen retrieval, the specimen was micr-owaved for 10 minutes using 0.1mM citrate-phosphate buffer or 20% zinc sulfate solution (Bio-Rad Labora-tories, Hercules, CA). After cooling and treatment for 30 minutes using normal horse serum,the primary monoclonal antibody was incubated at 4 degrees over-night. ER (Immunotech, Marseilles, France) was diluted 8 times and Factor-VIII (DAKO, Glostrup, Denmark) was diluted 50 times. The specimen was treated for 30 minutes using the anti-biotin mouse antibody in a 500-time dilution of streptavidin
(DAKO, Glostrup, Denmark), then stained in 3,3 -diamino-benzidine tetrahydrochloride solution and counterstained using hematoxylin. With respect to ER, those tumor nuclei with 10% or more staining were determined to be positive (Figure 2). With respect to Factor-VIII, four locations were chosen under a low magnification (×100) where capillary vessels converged inside the tumor. Stained capillary vessels (Figure 3) in these locations were counted under a high magnification (×400). The average of four locations was counted and used as microvessel count (MVC).
Positive Negative
Figure 2 Immunohistochemical staining for estrogen receptor
On the left was an example of estrogen receptor negative with virtually no nucleus being stained. On the right was a positive example, with many nuclei clearly stained.
Figure 3 Immunohistochemical staining for factor VIII
Shown on the left was an example of a relatively low microvessel count(MVC)with thinly scattered staining of newly formed vessels. On the right was an example of a high MVC, with many newly formed vessels being stained.
Statistical analysis
The comparison among groups was conducted using the chi-square test. Survival curves were calcu-lated by the Kaplan-Meier method and the statistical differences between the survival curves were evaluated using the generalized Wilcoxon test. A value assigned for determining a significance was p<0.05.
Results
There was no significant difference in age and disease duration among the four groups. In groups A, B,and C,which had childbirth histories,there were no statistically significant differences in the age of first childbirth or number of childbirths. Group A patients had a significantly(p<0.01)lower proportion of T1 tumor (≦2.0cm) compared to groups C patients (Table 1). The incidence of clinical stages up to stage
II was 69% in group A, which was significantly(p< 0.05) lower compared to groups C and D. There was no statistically significant difference in clinical stages among groups B, C and D (Table 1). Pathological lymph node metastasis was observed in 61% of group A,in 59% of group B,in 51% of group C,and in 43% of group D. The incidence of lymph node metastasis was significantly(p<0.05)lower in group D compared to groups A and B (Table 1). Ductal carcinoma in situ (DCIS) was observed in one patient (2.0%) of group A (49 patients),which was low,compared to the other groups; 10 of 106 patients(9.4%)in group B,17 of 269 patients (6.3%) in group C, and 15 of 198 patients (7.6%) in group D. However, histologial distribution among all groups showed no statistically significant difference (Table 1). NG, ER and MVC were examined in patients with up to stage II breast
III-IV 15 17 31 29 p<0.05 (A vs D) Nuclear grade 1 19 44 142 80 2 9 17 33 37 3 8 20 45 39 NS unknown 13 25 49 42 Histology DCIS 1 10 17 15 Papillotubular 15 31 77 49 Solid-tubular 11 24 46 52 Scirrhous 17 35 107 66 Others 5 6 22 16 NS
Values=mean±SEM, NS ; not significant, DCIS ; ductal carcinoma in situ
Table 2 ER status and MVC
Group A B C D p ER negative 18 34 60 75 positive 18 44 153 81 positivity(%) 50 56 72 52 p 0.05 (C vs A, B, D) MVC 60 51 53 63 NS
cancer. With regard to the NG,the incidence of grade 1 was 52.8% in group A,54.3% in group B,64.5% in group C and 51.3% in group D. There was no signifi-cant difference in NG among the four groups (Table 1).
The incidence of ER positivity was 50% for group A, 56% for group B, 72% for group C and 52% for group D. Group C had a significantly (p<0.05)
higher ER positivity than group A,B and D (Table 2). MVC was 60 for group A,51 for group B,53 for group C and 63 for group D. There was no statistically significant difference among the four groups.
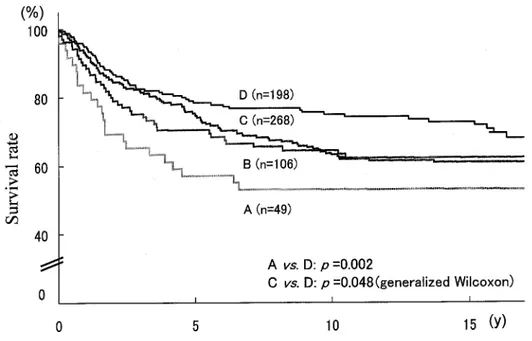
In all disease stages, the prognosis of group D patients was most favourable, and there was a signifi-cant(p<0.05)difference in the survival curves between groups A and C and between groups C and D (Figure
Figure 5 Survival rate in patients with stage I and II breast cancer
Patients in group A (one year or less postpartum) had the poorest prognosis and those in group D (no childbirth history) had the most favourable prognosis. There were significant differences in the survival curves between groups A and D and between groups C (one to three years postpartum) and D.
Figure 4 Survival rate in all patients
Patients in group A (one year or less postpartum) had the poorest prognosis and those in group D (no childbirth history) had the most favourable prognosis. There were significant differences in the survival curves between groups A and D and between groups C (one to three years postpartum) and D.
patients had significantly more advanced-stage breast cancer compared to those of the other groups, and in regard to histological type,the incidence of DCIS was lower in group A, without a significant difference.
In the portion of the study evaluating patients up to clinical stage II, group A patients had the lowest ER positivity. There are some studies of ER in breast cancer during pregnancy. We demonstrated that breast cancer patients during pregnancy were more likely to have axillary node-positive and ER-negative tumors. Our findings are consistent with those obser-ved by other investigators. Patients with ER-nega-tive tumors are considered to have a poor prognosis compared to those with ER-positive tumors. The ligand-binding assay to determine ER positivity may be less accurate in the hormonal circumstances of pregnancy because of the competitive blocking of the receptor sites resulting from hyperestrogenemia. Thus,we used immunohistochemical methodologies to determine the ER hormone status.
Lymphovascular invasion is common in the major-ity of breast cancer in young women. However, neovascular formation in pregnant women with breast cancer is unknown. MVC is meaningful as a factor in neovascular formation, and it has been reported that patients with a high MVC have a poor prognosis. In our study, MVC was higher in group A than in groups B and C, which was not a statistically signifi-cant. From these findings,breast cancer during preg-nancy(less than one year postpartum) has not only a larger number of advanced cases but also tumors with greater malignancy.
Group B had the second highest number of advanced patients next to group A. When disease stages were matched (up to stage II),the survival rate in group B was the similar with group C,although the ER positive rate was lower in group B. The difference in the survival rate between groups A and B may be explained by the following reason. Since breast can-cer is affected during its subclinical stage by the high
births is considered to be risk factors in developing breast cancer. However,these factors did not indicate the prognosis of breast cancer.
The mammary glands are in an undeveloped state in women who have not given birth. Morphological observation indicates that the lobules differentiate and acquire the capacity for lactation only through preg-nancy and childbirth. Childbirth history creates a different environment for breast cancer development, and cancers which develop with or without childbirth history differ in biological properties. The prognosis is reported to be poor for such early-onset breast cancer compared to cancer in other age groups. The patient age in this paper was limited to 35 or less in order to examine childbirth history in relation to survival.
In this study, the impact of pregnancy on breast cancer was examined from the viewpoint of time since childbirth. There were many advanced patients in the so-called breast cancer during pregnancy patients. The patients who developed cancer during pregnancy or up to one year after birth had a poor prognosis even when the disease stage was matched. The patients three years or less postpartum might have been affected by pregnancy in ER,however,there was no significant difference in prognosis between those who developed the disease three years or less and those who developed it more than three years postpartum. The patients without childbirth history were found to have a good prognosis.
In summary, patients of 35 years old or less who developed breast cancer during pregnancy or within less than one year postpartum may have a poor progno-sis. Patients with no childbirth history generally have a high risk factor of developing breast cancer. How-ever,our present study indicates breast cancer patients with no childbirth history may have a favourable prognosis.
References
1. Bonnier P, Romain S, Dilhuydy JM, et al. Influence of pregnancy on the outcome of breast cancer: A case-control study. Int J Cancer 1997; 72: 720-727.
2. Phillips KA,Milne RL,Friedlander ML,et al. Prognosis of premenopausal breast cancer and childbirth prior to diagnosis. J Clin Oncol 2004; 22: 699-705.
3. Rosenberg L,Thalib L,Adami HO,et al. Childbirth and breast cancer prognosis. Int J Cancer 2004; 111: 772-776. 4. Middleton LP,Amin M,Gwyn K,et al. Breast carcinoma in pregnant women : Assessment of clinicopathologic and immunohistochemical features. Cancer 2003; 98: 1055 -1060.
5. Gallenberg MM, Loprinzi CL. Breast cancer and preg-nancy. Semin Oncol 1989 ; 16: 369-376.
6. Clark RM,Reid J. Carcinoma of the breast in pregnancy and lactation. Int J Radiat Oncol Biol Phys 1978; 4: 693 -698.
7. Petrek JA, Dukoff BA, Rogatko A. Prognosis of preg-nancy-associated breast cancer. Cancer 1991; 67: 869 -872.
8. Nugent P, OConnell TX. Breast cancer and pregnancy. Arch Surg 1985; 120: 1221-1224.
9. King RM, Welch JS, Martin JK, et al. Carcinoma of the breast associated with pregnancy. Surg Gynecol Obstet
1985; 160: 228-232.
10. Ishida T, Yokoe T, Kasumi F, et al. Clinicopathologic characteristics and prognosis of breast cancer patients as-sociated with pregnancy and lactation : Analysis of case -control study in Japan. Jpn J Cancer Res 1992; 83: 1143 -1149.
11. Kroman N, Mouridsen HT. Prognostic influence of preg-nancy before, around, and after diagnosis of breast cancer. The Breast 2003; 12: 516-521.
12. Aziz SA, Pervez S, Khan S, et al. Case control study of prognostic markers and disease outcome in inflammatory carcinoma breast: A unique clinical experience. Breast J 2001; 7: 398-404.
13. Takei H, Iino Y, Horiguchi J, et al. Angiogenesis and stromal fibronectin expression in invasive breast carcinoma. Int J Oncol 1998; 12: 517-523.
14. Rosen PP,Lesser ML,Kinne DW,et al. Breast carcinoma in women 35 years of age or younger. Ann Surg 1984; 199 : 133-142.
15. Kollias J, Elston CW, Ellis IO, et al. Early-onset breast cancer-histopathological and prognostic considerations. Br J Cancer 1997; 75: 1318-1323.
16. Gajdos C, Tartter PI, Bleiweiss IJ, et al. Stage 0 to stage III breast cancer in young women. J Am Coll Surg 2000; 190: 523-529.