ContentslistsavailableatScienceDirect
Lung Cancer
j o ur n a l ho me p ag e : w w w . e l s e v i e r . c o m / l o c a t e / l u n g c a n
Plasma epidermal growth factor receptor mutation testing with a chip-based digital PCR system in patients with advanced non-small cell lung cancer
Norimitsu Kasahara
a,i, Hirotsugu Kenmotsu
a,∗,1, Masakuni Serizawa
b,∗∗,1,
Rina Umehara
b, Akira Ono
a, Yasushi Hisamatsu
a,f, Kazushige Wakuda
a, Shota Omori
a, Kazuhisa Nakashima
a, Tetsuhiko Taira
a,g, Tateaki Naito
a, Haruyasu Murakami
a,
Yasuhiro Koh
h, Keita Mori
c, Masahiro Endo
d, Takashi Nakajima
e, Masanobu Yamada
i, Masatoshi Kusuhara
b, Toshiaki Takahashi
aaDivisionofThoracicOncology,ShizuokaCancerCenter,Japan
bDrugDiscoveryandDevelopmentDivision,ShizuokaCancerCenterResearchInstitute,Japan
cClinicalTrialCoordinationOffice,ShizuokaCancerCenter,Japan
dDivisionofDiagnosticRadiology,ShizuokaCancerCenter,Japan
eDivisionofDiagnosticPathology,ShizuokaCancerCenter,1007Shimonagakubo,Nagaizumi-chou,Suntou-gun,Shizuoka,411-8777,Japan
fDepartmentofMedicalOncologyandHematology,OitaUniversityFacultyofMedicine,1-1Idaigaoka,Hasamamachi,Yufu,Oita,879-5593,Japan
gDivisionofRespiratoryMedicine,MinamiKyushuNationalHospital,1882Kida,Kajiki-chou,Aira,Kagoshima,899-5293,Japan
hThirdDepartmentofInternalMedicine,WakayamaMedicalUniversity,811-1Kimiidera,Wakayama,Wakayama,641-8509,Japan
iDepartmentofMedicineandMolecularScience,GunmaUniversityGraduateSchoolofMedicine,3-39-15,Showa-machi,Maebashi,Gunma371-8511, Japan
a r t i c l e i n f o
Articlehistory:
Received16July2016 Receivedinrevisedform 17December2016 Accepted2February2017
Keywords:
Liquidbiopsy
Epidermalgrowthfactorreceptormutation DigitalPCR
CirculatingfreeDNA Non-smallcelllungcancer
a b s t r a c t
Objectives:Epidermalgrowthfactorreceptor(EGFR)mutationtestingisacompaniondiagnostictodeter- mineeligibilityfortreatmentwithEGFRtyrosinekinaseinhibitors(EGFR-TKIs)innon-smallcelllung cancer(NSCLC).Recently,plasma-basedEGFRtestingbydigitalpolymerasechainreaction(dPCR),which enablesaccuratequantificationoftargetDNA,hasshownpromiseasaminimallyinvasivediagnostic.
Here,weaimedtoevaluatetheaccuracyofaplasma-basedEGFRmutationtestdevelopedusingchip- baseddPCR-baseddetectionof3EGFRmutations(exon19deletions,L858Rinexon21,andT790Min exon20).
Materials andmethods:Forty-nine patientswith NSCLC harboringEGFR-activating mutationswere enrolled,andcirculatingfreeDNAs(cfDNAs)wereextractedfromtheplasmaof21and28patients beforetreatmentandafterprogressionfollowingEGFR-TKItreatment,respectively.
Results:UsingreferencegenomicDNAcontainingeachmutation,thedetectionlimitofeachassaywas determinedtobe0.1%.Thesensitivityandspecificityofdetectingexon19deletionsandL858Rmuta- tions,calculatedbycomparingthemutationstatusinthecorrespondingtumors,were70.6%and93.3%, and66.7%and100%,respectively,showingsimilarresultscomparedwithpreviousstudies.T790Mwas detectedin43%of28cfDNAsafterprogressionwithEGFR-TKItreatment,butinnocfDNAsbeforethe startofthetreatment.
Conclusion:Thischip-baseddPCRassaycanfacilitatedetectionofEGFRmutationsincfDNAasaminimally invasivemethodinclinicalsettings.
©2017ElsevierB.V.Allrightsreserved.
Abbreviations: ARMS,amplificationrefractorymutationsystem;BEAMing,beads,emulsions,amplificationandmagnetics;cfDNA,circulatingfreeDNA;CI,confidence interval;ddPCR,dropletdigitalpolymerasechainreaction;dPCR,digitalpolymerasechainreaction;EGFR,epidermalgrowthfactorreceptor;EGFR-TKI,epidermalgrowth factorreceptortyrosinekinaseinhibitors;JAK2,Januskinase2;NSCLC,non-smallcelllungcancer;PFS,progression-freesurvival;RR,responserate;SD,standarddeviation.
∗Correspondingauthorat:DivisionofThoracicOncology,ShizuokaCancerCenter,1007Shimonagakubo,Nagaizumi-chou,Suntou-gun,Shizuoka411-8777,Japan.
∗∗ Correspondingauthorat:DrugDiscoveryandDevelopmentDivision,ShizuokaCancerCenterResearchInstitute,1007Shimonagakubo,Nagaizumi-chou,Suntou-gun, Shizuoka411-8777,Japan.
E-mailaddresses:[email protected](H.Kenmotsu),[email protected](M.Serizawa).
1 Bothofthecorrespondingauthorsequallycontributedtothisstudy.
http://dx.doi.org/10.1016/j.lungcan.2017.02.001 0169-5002/©2017ElsevierB.V.Allrightsreserved.
1. Introduction
Epidermalgrowthfactor receptor (EGFR)mutationtesting is essentialfortreatmentdecisionsforpatientswithadvancednon- smallcell lung cancer(NSCLC). EGFRtyrosine kinaseinhibitors (EGFR-TKIs),includinggefitinib,erlotinib,andafatinib,areeffective againstpatientswithNSCLCharboringEGFR-activatingmutations, suchasexon19deletionsortheL858Rmutationinexon21[1–6].
However,mostpatientswithNSCLCtreatedwithEGFR-TKIseven- tuallyacquireresistance. TheT790MmutationinEGFR exon20 causesapproximately50%ofacquiredresistancetoEGFR-TKIsin patients[7,8].Recently,thethird-generationEGFR-TKIosimertinib, whichspecificallytargetsEGFRT790M,wasapprovedforusein somecountriesincludingtheUSandJapan,andtheimportance ofserialbiopsiesfordetectingT790Misincreasing,assuchinfor- mationdeterminestheappropriatenessofosimertinibtreatment [9,10].However,repeatedbiopsiesaresometimeshighlyinvasive andcanbedifficulttoperformwithoutcomplications[11].
Recently, some studies have reported the efficacy of EGFR- activatingmutation analysiswith circulating free DNA (cfDNA) extractedfromtheplasmaofpatientswithNSCLC[12–21].More- over, EGFR-activating mutation analysis with cfDNA was also approvedasacompaniondiagnosisforselectingpatientseligible fortreatmentwithgefitinibandosimertinibintheEuropeanUnion.
However,sometechnicallimitationsfordetectingEGFRmutations withcfDNAhave beenreported.For example,thequantityand qualityofcirculatingtumor-derivedDNAvarieswidelybetween patients[22].Moreover,thedetectablepercentageofthetumor- derivedDNAfractionincfDNAcanreachaslowas0.01%[23].The digitalpolymerasechainreaction(dPCR),whichenablesaccurate copy-numberquantificationoftarget moleculesfromlow-input DNA,isthoughttobeapromisingtechnologyforovercomingthe abovelimitationsinmutationtestingwithcfDNA[24].Thehigh performanceofdPCRisachievedbycompartmentalizinga sam- pleatthelevelofasingleDNAmoleculebydistributingasample intothousandsof separatePCRreactions. Accordingly,thetotal copynumberoftargetscanbedeterminedbycountingthepos- itiveandnegativepartitions.dPCRplatformsareclassifiedinto3 typesbasedonthecompartmentalizationmethodused,including dropletdigital PCR (ddPCR)[20,25–30],BEAMing (beads,emul- sions,amplificationandmagnetics)PCR[19,20,31],andchip-based dPCR[30,32,33].Plasma-basedEGFRmutationtestingwithddPCR hasbeenevaluatedinmanyinstitutes.However,chip-baseddPCR hasnotbeenwidelyevaluated.
Thenewchip-baseddPCRsystem,QuantStudio3D(QS3D)Digi- talPCRSystem(ThermoFisherScientific,Waltham,MA,USA),was launched.Theconventionalchip-basedBioMarkdPCRsystem(Flu- idigm,SanFrancisco,CA,US)compartmentalizesDNAinto9,180 micropores[32,33],whereastheQS3DDigitalPCRsystemcompart- mentalizesDNAinto20,000micropores,whichiscomparabletothe compartmentalizationabilityoftheddPCRplatform,QX100/QX200 Droplet DigitalPCR System(Bio-Rad, Hercules, CA,US)broadly usedinstudiesforliquidbiopsy[25–29].Moreover,bothPCRand detectionprocessescanbeconsecutivelyperformedwithinaher- meticallysealedreactionchamberintheQS3DDigitalPCRsystem;
however,thisisnotpossiblewiththeddPCRsystem.Thisfeatureof theQS3DDigitalPCRsystemofferstheadvantageofrequiringfewer pipettingprocess thanthose neededforddPCR.Together,these propertiescontributetothereducedriskofcross-contamination.
TheQS3DDigitalPCRsystemrunseachchipindividually,indicat- ingsuitabilityoftheQS3DDigitalPCRsystemforclinicalsettings insmallinstitutionswithoutvastamountsofsamples.In previ- ouslystudies,thisQS3DDigitalPCRsystemhasbeenusedtodetect DNAmutationsinJanuskinase2(JAK2)[34]andcoagulationfac- torVgenes[35],microRNAs[36],andviralDNA[37],butnotEGFR mutations.
Therefore, this study aimed to evaluate plasma-based EGFR mutationanalysisinpatientswithadvancedNSCLC,usingthisnew chip-baseddPCRsystem,QS3DDigitalPCRSystem.
2. Materialandmethods 2.1. Patients
Allpatientsamplesusedinthisstudywerecollectedfromour previousprospectivestudytoevaluateplasmaEGFRmutationtest- ingwiththeRNaseH-dependentPCRandblockingoligo-dependent PCR methods[38].Thepresent studywasdesigned toevaluate theperformanceoftheQS3DDigitalPCRSysteminplasma-based EGFRmutationanalysis,usingcfDNAsamplesarchivedinthatpre- viousstudy[38].To beeligibleforourpreviousstudy,patients needed tohave beendiagnosed with advanced-stage NSCLCor post-operativerecurrenceandtohaveanEGFR-activatingmutation intheirtumors,asconfirmedbytheScorpionARMS(amplification refractorymutationsystem)method[39].In ourpreviousstudy [38],49patientswereenrolledfromOctober2013toMarch2014, andtumorstagingwasevaluatedaccordingtotheSeventhEdi- tionof TNMinLungCancer[40].Clinicalfactorsat thetimeof bloodsamplingwereobtainedfromthepatients’medicalrecords.
Basedonthetimingofbloodsampling,patientsweredividedinto 2groups.Onegroupincluded21patientsenrolledbeforethestart ofEGFR-TKItreatment,andtheothergroupincluded28patients whoshoweddiseaseprogressionafterEGFR-TKItreatment.Writ- teninformedconsentwasobtainedfromallpatients.Thisstudy wasconductedinaccordancewiththeprovisionsoftheDeclara- tionofHelsinkiandwasapprovedbytheInstitutionalReviewBoard ofShizuokaCancerCenter(approvalnumber#20-50-27-2-3).
2.2. Chip-baseddPCR
PlasmasamplesandDNAextractionaredescribedintheSupple- mentaryMaterialsandMethods.dPCRwasperformedontheQS3D DigitalPCRSystem(ThermoFisherScientific),whichwascomposed ofaProFlexPCRsystem,aQS3DdigitalPCRchiploader,andaQS3D chipscanner(allfromThermoFisherScientific).
TodetectthemostcommondeletionsinEGFRexon19,apair ofprimersand2TaqManprobesweredesigned,basedonYung’s report[32](Supplementary Fig.1).Asareferenceprobe,a VIC- labeledprobewasdesignedagainstaregionneighboringtheexon 19deletionsitesthatlacksreportedmutations.Awild-type-specific FAMprobewasdesignedagainsttheregionwheremostexon19 deletionsoccur.Insamplesharboringexon19deletions,theFAM probecannotanneal;thus,onlyVICfluorescenceisdetected.The sequencesoftheamplificationprimersandTaqManprobesused aregiveninSupplementaryTable1.TodetecttheL858RandT790M mutations,predesignedTaqManprobeandprimersets,AHRSRSV (EGFR6224)andAHRSROS(EGFR6240),respectively,werepur- chasedfromThermoFisherScientific.
2.3. Assessmentofthedetectionlimitforeachmutation
Thedetectionlimitofeachassaywasdefinedasthelowesttarget concentrationthatcouldbespecificallydetected(i.e.,withnofalse- positivedetectionintheabsenceofthetarget)andwasdetermined using20ngsampleoneachof2chipscontainingHDxReference StandardDNA(HorizonDiscovery,Cambridge,UK),whichwasval- idatedusingaddPCRsystemofBio-Rad.Thereferencestandard DNAsusedincludedHD251E746-A750(registeredintheCOS- MICdatabaseasthemostfrequentexon19deletion[http://cancer.
sanger.ac.uk/cancergenome/projects/cosmic/]),HD254forL858R, andHD258forT790M.EachreferencemutantDNAcontainseach mutantsequenceatafrequencyof50%.EachreferencemutantDNA
Table1
Patientcharacteristics.
Allpatients (n=49)(%)
Patientsbefore startofEGFR-TKI treatment (n=21)(%)
PatientswithPD afterEGFR-TKI treatment (n=28)(%) Age,years
median 67 74 65
range 42–89 50–89 42–81
Sex
Male 20(41) 7(33) 13(46)
Female 29(59) 14(67) 15(54)
Smokinghistory
Never 28(57) 16(76) 12(43)
Current/Former 21(43) 5(24) 16(57)
Histology
Adenocarcinoma 49(100) 21(100) 28(100)
EGFRmutation
Ex19del 34(69) 14(67) 20(71)
L858R 15(31) 7(33) 8(29)
Stage
IIIB/IV 41(84) 18(86) 23(82)
Postoperativerecurrence8(16) 3(14) 5(18) EGFR-TKI,epidermalgrowthfactorreceptortyrosinekinaseinhibitor;PD,progres- sivedisease;Ex19deletion,exon19deletionmutation;L858R,L858Rmutationin exon21.
wasseriallydilutedwiththecorrespondingwild-typeEGFRrefer- enceDNA(HD709,HorizonDiscovery)to50%,10%,5%,1%,0.5%, 0.1%,0.05%,or0.01%. Weregarded theperformance ofdPCRas adequateonlyiftheseriallydilutedDNAcopiesweredetected,as expected.Theaveragecopynumberdetectedinthepresenceof wild-typeEGFRreferenceDNA(i.e.,negativecontrol)plus3stan- darddeviations(SD)wasusedasthecut-offvalueforeachmutation site.
2.4. Statisticalanalysis
Thesensitivityand specificityofthechip-baseddPCRassays indetectingEGFRmutationswereevaluatedbycomparingresults obtainedwiththeScorpionARMSmethodusingthecorresponding tumorsamples(thereferencemethod).The95%confidenceinter- vals(CI)forthesensitivityandspecificitywerecomputedusing theClopperandPearsonmethod[41].Fisher’sexacttestwasused toexaminewhetherthetestresultscorrelatedwithclinicopatho- logicalcharacteristics.Progression-freesurvival(PFS)wasdefined asthedurationbetweentheinitiationofEGFR-TKItherapyandthe onsetofprogressivediseaseordeathfromanycause.PFSwascalcu- latedaccordingtotheKaplan–Meiermethodandcomparedusing thelog-ranktest.Correlation coefficients werecalculated using Spearman’srankanalysis.P<0.05wasconsideredstatisticallysig- nificant.StatisticalanalyseswereperformedusingJMPsoftware, version12.0.1for Windows(SAS Institute, Cary,NC,US)and R software,version3.1.3(http://www.r-project.org).
3. Results
3.1. Patientcharacteristics
Thepatientcharacteristicsare shownin Table1.Thirty-four patientswithNSCLCharboredanexon19deletionand15patients presentedtheL858Rmutationintheirtumorsamples,asdetected using the Scorpion ARMS method. Twenty-one blood samples werecollectedfrompatientswhohad never beentreatedwith EGFR-TKIs,and 28 blood sampleswere collectedfrompatients with progressive disease after treatment with EGFR-TKIs. The patientshadamedianageof67years (range42–89years),and 29patients(59%)werefemale.Twenty-eightpatients(57%)were never-smokers,and 21 (43%) had a smoking history. Forty-one
Table2
ComparisonofEGFRexon19deletionandL858RstatusincfDNAandpairedtumor samples.
Tumortissue
PlasmacfDNA + – Sensitivity Specificity Concordance Exon19del
+ 24 1 70.6% 93.3% 77.6%
− 10 14
L858R
+ 10 0 66.7% 100.0% 89.8%
− 5 34
cfDNA,circulatingfreeDNA;Ex19del,exon19deletionmutation;L858R,L858R mutationinexon21;M+,mutationpositive;M-,mutationnegative.
patients(84%)hadstageIIIBorstageIVdisease,and8patients(16%) hadpost-operativerecurrence.Alllungtumorswereclassifiedhis- tologicallyasadenocarcinoma.
3.2. Determinationofassayperformance
Afterpreparing7 serialdilutionsof genomicDNA harboring an EGFR mutant in genomic DNA with wild-type EGFR (range:
50%–0.01%mutantEGFR), westably detectedthetargetedEGFR mutationsatafrequencyaslowas0.1%(SupplementaryFig.2).
Experimentswererepeatedover3separatedays.Todeterminethe cut-offvalue,referenceDNA withwild-typeEGFRwasanalyzed 8times usingamplificationprimers andeach mutation-specific probe.Theaveragecopynumbersforthewild-typereferenceDNA (plus3SDs),whichwereusedasthecut-offvalues,were1.6,2.1, and0copies/assayforexon19deletions,L858R,andT790M,respec- tively. Supplementary Fig.3A shows comparisons betweenthe expectedmutationfrequencyin20ngofDNAloadedinto2separate chipsvs.theobservedcopynumbersofEGFRmutations.Mutant alleleswerestablydetectedusingthesecut-off values,downto aprevalenceof0.1%(SupplementaryFig.3A).Wealsoevaluated thecopynumberofEGFRmutationsinplasmasamplesusingthese determinedcut-offvalues.Apositivelinearrelationshipbetween theexpected and observedmutation frequencies wasobserved overarangeof0.1–50%duringtestingforallmutantsexamined.
Regressionanalysisshowedcoefficientsofdetermination(R2)of 0.9976,0.9952,and0.9961withdetectionoftheexon19deletion mutant,L858R,andT790M,respectively(SupplementaryFig.3B).
3.3. EGFRmutationtestinginclinicalplasmacfDNAsamples
Among49 patients, themedian concentrationof cfDNA iso- latedpermlofplasmaacrossallsampleswas35.1ng/ml(range 12.2–139.5).Twenty-fiveplasmasampleswereidentifiedaspos- itiveforanexon19deletion,basedonthecut-offcopynumber (>1.6),and10wereidentifiedaspositiveforL858R(cut-offcopy number>2.1),asshowninFig.1andSupplementaryTable2.Only 1plasmasamplewaspositiveforbothanexon19deletionand L858R,althoughonlytheL858Rmutationwasdetectedinthecorre- spondingtumortissue.ThesensitivityandspecificityofeachdPCR assaycalculatedbycomparisonwiththecorrespondingtumorsam- pleswere70.6%(24/34;95%CI,52.5%–84.9%)and93.3%(14/15;
95%CI,68.1%–99.8%)forexon19deletion,and66.7%(10/15;95%
CI,38.4%–88.2%)and100%(34/34;95%CI,89.7%–100%)forL858R (Table2).Theoverallconcordanceratebetweentheplasmaand tumortissueswas77.6%(38/49;95%CI,63.4%–88.2%)forexon19 deletionand89.8%(44/49;95%CI,77.8%–96.6%)forL858R.
Twelvesampleswereidentifiedaspositive(cut-offcopynum- ber>0)fortheT790Mmutation(Fig.1andSupplementaryTable 2).AllplasmasampleswiththeT790Mmutationwereobtained frompatientsshowingprogressionafterEGFR-TKItreatment(43%;
Fig.1.DistributionofEGFRmutant-allelecopynumbersperassayinplasmasam- ples.Intheexon19deletionassay,thecopynumbersdetectedinplasmasamples rangedfrom1.0to610.7copies/assay,and25plasmasampleswerescoredasposi- tiveusingacut-offvalueof1.6copies/assay.IntheL858Rassay,thecopynumbers detectedinplasmarangedfrom4.6to5380.4copies/assay,and10sampleswere scoredaspositiveforL858Rusingacut-offvalueof2.1copies/assay.IntheT790M assay,thecopynumbersmeasuredinplasmasamplesrangedfrom4.6to267.2 copies/assay,and12plasmasampleswerescoredaspositiveusingacut-offvalue of0copies/assay.Thedashedlineshowstheaveragecopynumbersfornegativesam- plesplus3×SDasthecut-offvalue.Exon19del,exon19deletion;L858R,L858R mutationinexon21;T790M,T790Mmutationinexon20.
12/28),withtheT790Mmutationnotbeingobservedinpatient samplesobtainedbeforeEGFR-TKItreatment.
In28 patientswithprogressive diseaseaftertreatmentwith EGFR-TKIs, 11 out of 12 patients with NSCLC and detectable EGFRT790Mintheplasmaunderwentre-biopsy,5ofwhichalso presentedtheT790Mmutationintheirre-biopsysamples(Supple- mentaryTables2and3).Inaddition,9outof16patientswithNSCLC lackingdetectableT790Mintheplasmaunderwentre-biopsy,and 2patientspresentedT790Mintheirre-biopsysamples(Supple- mentaryTables2and3).
Amongthe25patientswithanexon19deletionintheplasma, thepercentmutationrateintheplasmarangedfrom0.3%to45.4%
(median2.3%).Amongthe10patientswithdetectableL858Rinthe plasma,thepercentmutationrateintheplasmarangedfrom0.5%
to70.8%(median2.4%),including1patientwhohadbothanexon 19deletionandtheL858Rmutation.Amongthe12patientswith detectableT790Mintheplasma,thepercentmutationrateinthe plasmarangedfrom0.5%to11.6%(median1.4%).Nostatistically significantrelationshipsbetweentheamountofinputcfDNAand thecopynumbersofeachEGFRmutationwereobserved(Supple- mentaryFig.4).
3.4. AssociationbetweenEGFRmutationdetectionand extra-thoracicmetastaticdisease
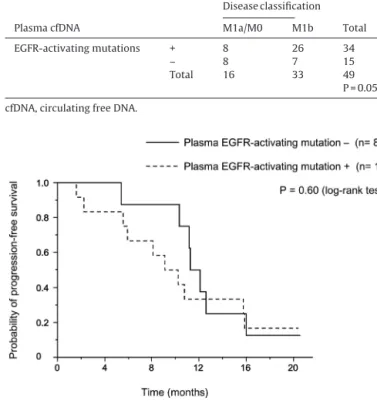
Amongallpatients,therelationshipbetweenthedetectionof EGFRmutationsincfDNAandtheexistenceofextra-thoracicmetas- taseswasevaluated.EGFR-activatingmutationstendedtobemore frequentlydetectedintheplasmaofpatientswithextra-thoracic metastaticdisease(M1b)thaninpatientswithdiseaseconfined tothethoraciccavity(M1a/M0;p=0.053;Table3).Nodifference inthedetectionoftheEGFRT790Mmutationintheplasmawas observedbetweenpatientswithM1a/M0andM1bdiseaseclassi- fications(p=0.29).
Table3
RelationshipbetweenEGFR-activatingmutationsandNSCLCclassification.
Diseaseclassification
PlasmacfDNA M1a/M0 M1b Total
EGFR-activatingmutations + 8 26 34
– 8 7 15
Total 16 33 49
P=0.053 cfDNA,circulatingfreeDNA.
Fig.2. Progression-freesurvival(PFS)of20patientswithNSCLCwhoenrolledin thisstudybeforethestartofEGFR-TKItreatment.ThemedianPFSwas9.7months inpatientswithdetectableEGFR-activatingmutationsintheplasma(dashedline), and11.7monthsinpatientswithoutdetectableEGFR-activatingmutationsinthe plasma(solidline;p=0.60).
3.5. PlasmaEGFRmutationstatusatpre-treatmentvs.clinical outcomes
Amongthe21patientswhoenrolledbeforethestartofEGFR-TKI treatment,20patientsweretreatedwithEGFR-TKIsafterplasma sampling.Nostatisticallysignificantdifferencewasobservedinthe responserate(RR)andPFSfollowingEGFR-TKItreatmentbetween patientswithdetectable(n=12) and undetectable(n=8)EGFR- activatingmutationsintheplasma(RR: 87.5vs.66.7%,p=0.60;
medianPFS:11.7vs.9.7months,p=0.60;Fig.2).
4. Discussion
Toourknowledge,thisisthefirststudytoevaluatetheper- formance of detection assays for exon 19 deletion, L858R, and T790MinplasmasamplesusingtheQS3DDigitalPCRSystem.EGFR mutationswerestablydetectedataprevalenceaslowas0.1%,indi- catingconsistencywithdatafromapreviousstudyfordetection ofJAK2V617Fmutationinmyeloproliferativeneoplasmswiththe QS3DDigitalPCRsystem[34].ThedetectionlimitsofddPCR,using theQX100/QX200DropletDigitalPCRSystemwereestimatedas 0.01–0.04%[25–29].Similarly,thedetectionlimitofBEAMingPCR wasestimatedas0.01%[31],andthatofchip-baseddPCRusing theBioMarksystemwas0.03–0.1%[32,33](Table4).Asshownin Table4,weobservedsimilarsensitivityandspecificitycomparedto theotherdPCRassays.Theseresultsindicatedthatthelowerdetec- tionlimitdidnotcorrelatewiththesensitivityandspecificityin detectingEGFRmutationsinplasma.Thisdiscrepancymighthave resultedfromtheuseofdifferenttypesofDNA,suchasplasmid andhumangenomicDNA,whendeterminingthelowerdetection limit.Moreover,itispossiblethatdifferencesinthedesignofthe primersandprobes,aswellasthecut-offvalueselected,alsocaused thedifferencesintheresults.
Table4
PerformancecomparisonwithotherPCRmethodsforevaluatingEGFRmutationsin plasma.
Method Detection
limit(%)
Sensitivity (%)
Specificity (%) Allele-specificPCR(Cobas)[18–21] 0.1 60.7–84.3 96.4–97.0
BEAMingPCR[19,20,30] 0.01 72.7–87.0 96.8–100
DropletdPCR[25–29] 0.01–0.04 66.7–84.3 95.8–100
Chip-baseddPCR[31,32] 0.03–0.1 78.9 100
Thisstudy 0.1 66.7–70.6 93.3–100
dPCR,digitalPCR.
EGFR-activating mutations tended to be more frequently detectedintheplasmaofpatientswithextra-thoracicmetastatic disease (M1b) than in patients with limited thoracic disease (M1a/M0; p=0.053; Table3).These resultsare consistentwith thoseofpreviousstudiesandsuggestthatthetumorburdenor metastaticstatusmayinfluencethedetectionofEGFRmutations intheplasma[15,19,20,42].Althoughnostatisticallysignificant differenceswereobservedintheRRandPFSfollowingEGFR-TKI treatment between patients with or without detectable EGFR- activatingmutationsintheirplasma,patientswithEGFR-activating mutationsintheplasmaappearedtohaveinferiorPFS(Fig.2).These resultsmighthavebeeninfluencedbythemetastaticstatus.
WhilealowfrequencyofdenovoT790Mmutationsintumor sampleswasreportedin onestudy[43],anotherstudyshowed theexistenceoftheT790Mmutationinapproximatelyhalfofthe tumorsamplestestedafterprogressionwithEGFR-TKItreatment [8].In thepresentstudy,T790M mutationswereonlydetected inplasmasamplesofpatientsshowingdiseaseprogressionafter EGFR-TKItreatment, and thefrequency of T790M detection in plasma samples was 43%, similar to data from previous dPCR studies showing that 28.6%–66.7% of patients withNSCLC had detectableT790Mintheplasma[19,20,26,28,29,33].Twoprevious reportsshowedthattheclinicalresponseratesforthird-generation EGFR-TKIs in patients positive for the T790M mutation in the plasmawerenearlyidenticaltothatinpatientswithpositivetis- suesamples[19,20].TheseresultssuggestthatplasmaT790Mcan serveasabiomarkerfortheuseofthird-generationEGFR-TKIs;
thus,itwillbecomemoreimportanttotestfor thepresenceof plasmaT790Minfutureclinicalsettings.
Thisstudyhassomelimitations.Firstly,wecouldnotperform thecomparisonassaywiththesamecfDNAsamplesbetweenthe QS3DDigitalPCRsystemandotherdPCRplatforms.Instead,inthis study,weperformedtheassessmentofassayperformanceofthis QS3DDigitalPCRassaywithcommerciallyavailablecertifiedref- erenceDNA materialswhose mutant allelecopy numberswere validatedusingaddPCRsystemofBio-Rad(SupplementaryFigs.
2and3).Secondly,becauseenoughmatchingtumorsampleswere notavailabletoevaluatetheQS3DDigitalPCRassay,thedetec- tionofEGFR-mutationsbydPCRwasperformedonlywithplasma samplesand notwithtissue samples.Thesensitivityand speci- ficityoftheassayswerecalculatedaccordingtotheEGFRmutation statusoftumorsamples,asfirstdeterminedusingtheScorpion ARMSmethod.Thirdly,differencesoccurredinthetimingbetween bloodsamplingandtumortissuesamplingforsomepatients.The prevalenceof EGFR-activating mutations in the plasma can be influencedbytreatmentwithEGFR-TKIsorcytotoxicchemother- apies[25]. Thetime course mayalsohave an influenceonthe levelofEGFR-activatingmutationsdetectedintheplasma.Accord- ingly,wecouldnotevaluatetheconcordanceofT790Mmutations betweenplasmaandtissuesamples.TheleveloftheT790Mmuta- tionpresentinplasmamaychangefollowingEGFR-TKItreatment [25].In thisstudy,T790Mmutationswereonlydetectedinthe plasmaofpatientsshowingprogressionafterEGFR-TKItreatment;
thus,theT790Mmutationstatusinthecorrespondingtumorsam-
plesatthetimeofbloodsamplingisunclear.However,thisisalso generallyalimitationinclinicalsettings.Theselimitationsmight alsobe associated withthecausesowing towhich the perfor- manceoftheQS3DDigitalPCRsystemwassimilartothatofthe conventionalchip-basedBioMarkdPCRsystem(Fluidigm),which hasfewermicroporescomparedtotheQS3DDigitalPCRsystem [32],althoughapreviousstudyreportedthatthenumberofparti- tionsimpactsthemeasurementprecisionanddynamicrange[44].
Toovercometheabove-mentionedlimitations,prospectivestudies withtime-matchedbloodandtissuesamplesobtainedfrommore patientswithlungadenocarcinomaarenecessaryforfurthereval- uationoftheperformanceoftheEGFRmutation-detectionsystem developedinthisstudy.
5. Conclusion
We evaluated dPCR assays for detecting EGFR mutations in plasmasamplesofpatientswithNSCLCusingtheQS3DDigitalPCR System.ThissystemshowedsimilarperformancetootherdPCR assays.OurresultsindicatedthatEGFRmutationtestingwithcfDNA usingchip-baseddPCRcanbeusefulasaminimallyinvasivemon- itoringmethodinclinicalsettings.
Conflictofinterest
Theauthorshavethefollowingconflictsofinteresttodeclare:H.
K.,Y.H.,M.Y.,andT.T.receivedresearchgrantsfromAstraZeneca.
K.K.H.K.,H.M.,Y.K.,M.Y.,andT.T.receivedspeakingfeesfrom AstraZeneca.K.K.H.K.,Y.K.,andM.Y.receivedresearchgrants fromBoehringerIngelheim,Japan.H.K.,H.M.,Y.K.,M.Y.,andT.
T.receivedspeakingfeesfromBoehringerIngelheim,Japan.Y.H., Y.K.,M.Y.,andT.T.receivedresearchgrantsfromChugaiPharma- ceuticalCo.,Ltd.H.K.,A.O.,S.O.,H.M.,M.Y.,andT.T.received speakingfeesfromChugaiPharmaceuticalCo.,Ltd.H.K.,A.O.,and S.O.receivedspeakingfeesfromTaihoPharmaceuticalCo.,Ltd.T.
T.receivedresearchgrantsfromEliLilly JapanK.K.H.K.andA.
O.receivedspeakingfeesfromEliLillyJapanK.K.T.T.received researchgrantsfromPfizerJapan,Inc.
Acknowledgement
ThisworkwassupportedbytheJapanSocietyforthePromotion ofScienceKAKENHIGrantNumber15K21688(A.O.).
AppendixA. Supplementarydata
Supplementarydataassociatedwiththisarticlecanbefound,in theonlineversion,athttp://dx.doi.org/10.1016/j.lungcan.2017.02.
001.
References
[1]M.Maemondo,A.Inoue,K.Kobayashi,S.Sugawara,S.Oizumi,H.Isobe,A.
Gemma,M.Harada,H.Yoshizawa,I.Kinoshita,Y.Fujita,S.Okinaga,H.Hirano, K.Yoshimori,T.Harada,T.Ogura,M.Ando,H.Miyazawa,T.Tanaka,Y.Saijo,K.
Hagiwara,S.Morita,T.Nukiwa,North-EastJapanStudyG,Gefitinibor chemotherapyfornon-small-celllungcancerwithmutatedEGFR,NewEngl.
J.Med.362(2010)2380–2388.
[2]T.Mitsudomi,S.Morita,Y.Yatabe,S.Negoro,I.Okamoto,J.Tsurutani,T.Seto, M.Satouchi,H.Tada,T.Hirashima,K.Asami,N.Katakami,M.Takada,H.
Yoshioka,K.Shibata,S.Kudoh,E.Shimizu,H.Saito,S.Toyooka,K.Nakagawa, M.Fukuoka,Gefitinibversuscisplatinplusdocetaxelinpatientswith non-small-celllungcancerharbouringmutationsoftheepidermalgrowth factorreceptor(WJTOG3405):anopenlabel,randomisedphase3trial,Lancet Oncol.11(2010)121–128.
[3]R.Rosell,E.Carcereny,R.Gervais,A.Vergnenegre,B.Massuti,E.Felip,R.
Palmero,R.Garcia-Gomez,C.Pallares,J.M.Sanchez,R.Porta,M.Cobo,P.
Garrido,F.Longo,T.Moran,A.Insa,F.DeMarinis,R.Corre,I.Bover,A.Illiano, E.Dansin,J.deCastro,M.Milella,N.Reguart,G.Altavilla,U.Jimenez,M.