IRUCAA@TDC : Treatment of periodontal defects with enamel matrix derivative: clinical evaluation at early healing stages.
10
0
0
全文
(2) 85. Bull Tokyo Dent Coll (2010) 51(2): 85–93. Clinical Report. Treatment of Periodontal Defects with Enamel Matrix Derivative: Clinical Evaluation at Early Healing Stages Atsushi Saito, Hiroki Hayakawa*, Kei Ota*, Koushu Fujinami, Masahiko Nikaido** and Takemi Makiishi Division of Conservative Dentistry, Department of Clinical Oral Health Science, Tokyo Dental College, 2-9-18 Misaki-cho, Chiyoda-ku, Tokyo 101-0061, Japan * Division of General Dentistry, Department of Clinical Oral Health Science, Tokyo Dental College, 2-9-18 Misaki-cho, Chiyoda-ku, Tokyo 101-0061, Japan ** Nikaido Dental Office, 3-5-12-4F Nihonbashi, Chuo-ku, Tokyo 103-0027, Japan. Received 15 January, 2010/Accepted for publication 3 February, 2010. Abstract The aim of this retrospective clinical study was to evaluate the treatment of intrabony periodontal defects with enamel matrix derivative (EMD) during the early stages of healing. Sixteen patients aged 38–77 years with a clinical diagnosis of chronic periodontitis were subjected to data analysis. A total of 25 teeth with various osseous defects received regenerative therapy with EMD, and were followed for a minimum of 6 months. Post-operative healing was uneventful in the majority of cases. Treatment of the intrabony defects with EMD led to a statistically significant improvement in the mean value of probing depth at 3 months compared with that at baseline (p⬍0.001). Mean values of attachment gain at 3 and 6 months were of clinical significance: 3.6Ⳳ1.8 mm and 3.2Ⳳ1.5 mm, respectively. Reduction in probing depth was achieved with minimal recession of gingival margin and was sustained over a time course of 6 months. A progressive increase in radiopacity, suggestive of initial signs of bone-fill, was observed by 6 months. In summary, the results suggest that treatment of intrabony defect with EMD induces favorable periodontal healing with a high level of predictability. Key words:. Periodontal regeneration— Periodontitis— Enamel matrix derivative (EMD)—Intrabony defects. Introduction. ally leads to tooth exfoliation. In recent years, a number of new treatment procedures have been introduced in attempts to regenerate lost periodontal tissues. An attractive way of promoting periodontal regeneration is to try to mimic the events that took place during the. Periodontitis, one of the most common infectious diseases in humans25), is characterized by gingival inflammation, as well as loss of connective tissue and alveolar bone, which eventu85.
(3) 86. Saito A et al.. development of the periodontal tissues4). One such example is treatment with an enamel matrix derivative (EMD). EMD represents an extracellular matrix derivative that seems to control and promote periodontal regeneration. EMD is derived from porcine tooth buds and is available in a commercial formulation (Emdogain® Gel, Biora AB, Malmö, Sweden). This product is composed primarily of acidic extracted amelogenins in an aqueous viscous solution of propylene glycol alginate6). The activities of EMD on epithelial cells suggest a potential desirable inhibitory effect on epithelial downgrowth during the early regenerative stages10). Since its introduction, extensive research regarding EMD has been carried out. EMD has demonstrated the ability to encourage periodontal regeneration in both animal studies and clinical trials10,22). The clinical significance of EMD therapy, however, is still under debate, and its scientific base has yet to be firmly established15). While it is imperative to evaluate the efficacy of a treatment modality in longitudinal studies, it is equally important to understand the healing process during early periods. It is assumed that EMD has an effect on the critical steps of periodontal wound healing that occur during the early healing phase9). In our teaching hospital, surgical treatment with EMD has been the treatment of choice for patients requesting periodontal regenerative therapy. In the practice of evidence based medicine, it is important to integrate individual clinical expertise with the best available external clinical evidence from systematic research16). Toward this end, it is necessary to evaluate the clinical outcomes in one’s own practice setting. The aim of the present study was to evaluate the clinical outcomes of periodontal regenerative surgery with EMD during the early stages of healing.. Methods 1. Subjects The study participants were selected from. a patient population at Suidobashi Hospital, Tokyo Dental College, with clinical diagnosis of moderate to advanced chronic periodontitis. Written informed consent was obtained from all patients. The following criteria were used for inclusion and data analysis in the present study: 1) no serious systemic complications or history of allergies; 2) periodontal pockets with a probing depth (PD) of ⱖ6 mm; 3) osseous defects estimated to be at least 4 mm deep and 2 mm wide (largest width). A total of 16 patients (12 women and 4 men) with a mean age of 56.7 years (range; 38 to 77) were subjected to data analysis. 2. Initial periodontal therapy After systemic and oral assessments, a periodontal treatment plan was formulated for each patient. Initial periodontal therapy consisting mainly of oral hygiene instructions, fullmouth scaling and root planing, and occlusal adjustment (if trauma from occlusion was present) was performed by three clinicians. 3. Clinical parameters At least 4 weeks after the initial therapy, re-evaluation was performed. The following baseline clinical parameters were recorded prior to the surgery. PD was measured using a Williams probe with a force of 0.25 N by the examiner and rounded up to the nearest millimeter. Clinical attachment level (CAL) was measured from the cemento-enamel junction to the apical depth of periodontal probe penetration. PD, CAL and gingival recession were registered at six sites. Tooth mobility was recorded using Miller’s index11). The presence or absence of supragingival dental plaque was recorded by the Plaque Control Record (PCR) of O’Leary et al.13). Postoperative re-evaluations were performed at 3 and 6 months after surgery. 4. Radiographic examination Intraoral radiographs were obtained with a paralleling cone technique. Subjective evaluation was used to detect potential changes in radiographical images..
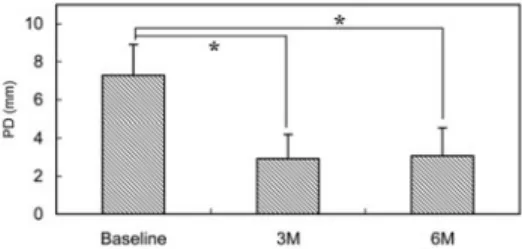
(4) 87. Short-term Outcomes of EMD Therapy. 5. Periodontal regenerative therapy An individualized treatment plan, with alternatives, was presented to the patient. Informed consent to the proposed surgical intervention was obtained from each patient. If other dental pathologies or conditions were present, they were treated prior to or concurrently with the regenerative therapy. Surgical interventions were implemented between January 2008 and June 2009. Interventions ranged from localized to quadrant surgery, with at least one tooth in the quadrant having intrabony defects matching the abovementioned criteria. Regenerative therapy with EMD was performed by the standard procedure as described previously17). Briefly, a fullthickness periodontal flap (papilla preservation technique) was employed to gain access to the root surface for scaling and root planing. In localized procedures, a vertical releasing incision was made on the buccal aspect, at least one tooth distant from the lesion. Following debridement, sites were acid-etched with 36% ortho-phosphoric acid for 15 seconds in order to remove smear layers. After the sites were thoroughly rinsed with sterile saline, 0.3 ml or 0.7 ml EMD solution (Emdogain® Gel) was applied, in accordance with the manufacturer’s instructions. No attempt was made to use bone graft or other supplementary modalities. The flaps were immediately replaced and sutured with monofilament, non-resorbable sutures. Either modified vertical mattress or interrupted sutures were used to obtain complete closure of the interdental soft tissues. Postoperative instructions were subsequently given to the patients. Patients received an oral antibiotic (typically 300 mg/d cefdinir) and a non-steroidal antiinflammatory drug for 3 to 5 days. They were advised to use a mouth rinse twice daily. The sutures were removed after 10 to 14 days. After suture removal, patient plaque control with the roll brushing technique utilizing an ultra-soft toothbrush was resumed at the surgically treated sites. Any adverse reactions or patient perceptions (i.e., pain, bleeding, or swelling, as obtained by interview) during the first week postsur-. gery were assessed and recorded. 6. Supportive periodontal therapy Meticulous supragingival professional tooth cleaning was also performed biweekly for the first 6 weeks postsurgery. Thereafter, patients were recalled once a month. They received supportive periodontal therapy, consisting mainly of oral hygiene instruction and professional plaque control. 7. Data management and statistical analysis The deepest site of the defect was used for evaluating the clinical changes in the primary outcome variables PD and CAL. For statistical analysis of the quantitative data, a software package (InStat version 3.10 for Windows, GraphPad Software, La Jolla, CA, USA) was used. p-values less than 0.01 were considered statistically significant.. Results None of the patients showed any healing complications with the initial periodontal therapy. During the initial therapy, an effort was made to obtain an optimal level of oral hygiene by patient self-care, as well as professional care. A total of 25 sites (18 molars, 3 premolars, 4 canines) in 16 patients received regenerative therapy with EMD and were followed up for at least 6 months. The mean PD of the sites at baseline was 7.3Ⳳ1.6 mm, and the defect type included 1 to 3-wall intrabony defects (1-wall: 3 sites, 2–3-wall: 22 sites). The majority of defects treated demonstrated good flap closure during the first and second postoperative week. Examples of the patients’ perceptions of healing during the first week postoperatively are listed in Table 1. The frequency of no perceived pain or swelling was 52%. Post-operative healing, thereafter, was uneventful in the vast majority of patients. A statistically significant improvement in mean PD was already observed at 3 months postsurgery (Fig. 1). Mean PD reductions in the recorded sites at 3 and 6 months.
(5) 88. Saito A et al.. Table 1 Patient perceptions during first week postoperatively Perceptions. Prevalence (% surgery events)*. No remarkable distress Minor pain Minor swelling Minor bleeding Sore spot in gum. 52 20 8 8 16. * Frequencies do not add up to 100% as multiple answers were allowed.. Fig. 1 Change in PD (meanⳲSD). n⳱25 *p⬍0.001, Friedman test with Dunn post test. Table 2 Frequency distribution of CAL gains at 6 months CAL gain (mm) ⬍2 2–3 4–5 ⱖ6. Prevalence (%) 16 48 28 8. Fig. 2 Change in CAL (meanⳲSD). n⳱25 *p⬍0.001, Friedman test with Dunn post test. Fig. 4 Change in tooth mobility (meanⳲSD). n⳱25. Fig. 3 Contribution of gingival recession and clinical attachment gain in reduction of PD.. were 4.4Ⳳ1.4 mm (range 3 to 8 mm) and 4.2Ⳳ1.2 mm (range 3 to 7 mm), respectively. The reduction in PD was maintained during the 6 months observation period, with no significant change. A statistically significant change in CAL was also observed at 3 months postsurgery (Fig. 2). Mean CAL gains in the recorded sites at 3 and 6 months were 3.6Ⳳ1.8 mm (range 0 to 7 mm) and 3.2Ⳳ1.5 mm (range 0 to 7 mm), respectively. The CAL gain was maintained during the 6 months observation period, with no significant change. Table 2. shows the frequency distribution of CAL gains at 6 months. Twelve sites demonstrated a CAL gain of 2 to 3 mm and 7 sites a gain of 4 to 5 mm. No significant correlation was found between the baseline PD and CAL gain at 6 months (r⳱0.4388, p⳱0.0282, by Spearman rank correlation). The reduction in PD was achieved with minimal recession of the gingival margin (Fig. 3). There was no significant change in tooth mobility during the observation period (Fig. 4), although it was typical to find a transient increase in mobility immediately after surgery. When the relationship between the baseline tooth mobility and CAL gain was assessed, no significant difference in CAL gain was found between teeth without mobility and teeth.
(6) 89. Short-term Outcomes of EMD Therapy. a. b. c. d. Fig. 5 a: 64-year-old woman with generalized chronic periodontitis. Clinical appearance of tooth #46 during surgery with EMD. Note extensive intrabony defect extending from furcation to distal root area. b: Radiographic view at initial visit, showing vertical bone loss as well as furcation involvement. c: Radiographic view at 3 months, showing slight change in radiopacity in distal aspect of #46. d: Radiographic view at 6 months, suggesting further resolution of intrabony component of defect. Lamina dura reformation is not observed.. with mobility (ⱖ1, Miller index, p⳱0.2249, Mann-Whitney U test). No apparent adverse reactions were recorded as a result of multiple applications of EMD within the same patient. The clinical and radiographic appearances of representative cases are shown in Figs. 5 and 6.. Discussion In the present study, periodontal surgery with EMD resulted in significant PD reductions and CAL gains at treated sites during the early healing period. Although it is generally recommended to wait for 6 months before taking any clinical measurements after EMD. treatment 5), we performed careful probing (0.25 N) to assess soft tissue healing at early stages. An improvement in PD was detected as early as 3 months postoperatively. The observed improvement in PD at 6 months (approximately 4.3 mm; 59% of the baseline PD) was in accordance with the results from a multi-center study of 956 cases in Japan20). The mean CAL gain at 6 months was of clinical significance (3.4 mm; 40% of the baseline attachment level). A meta analysis of clinical studies on the management of angular osseous defects with EMD10) revealed a PD reduction of 4.0 mm (50% of the baseline PD) and CAL gain of 3.2 mm (33% of the original attachment level) for a total of 317 lesions during an observation period ranging from 6 to 12.
(7) 90. Saito A et al.. a. b. c Fig. 6 a: 69-year-old woman with generalized chronic periodontitis. Note extensive intrabony defect surrounding distal root. b: Radiographic view at initial visit, showing vertical bone loss at distal root as well as furcation involvement. c: Radiographic view at 6 months, showing distinctive increase in radiopacity in distal root and furcation area.. months. In their international multi-center study, Tonetti et al.21) reported a mean CAL gain of 3.1 mm at 1 year. Previous study by our group evaluated the long-term clinical. outcomes of treatment with EMD in a private practice setting17). The mean CAL gain at 6 months was 3.6 mm, which was significantly greater than that (2.2 mm) observed in our study on guided tissue regeneration utilizing bioresorbable membrane26). The results of the present study were comparable to those of earlier studies reporting the efficacy of EMD therapy. In this study, 8 teeth showed mobility at 6 months postoperatively. During the 6 months observation period, no significant change in tooth mobility was observed (Fig. 4). Moreover, no significant difference in CAL gain was found in relation to tooth mobility. It has been suggested that mobile teeth are at greater risk of future attachment loss when compared to teeth without mobility23). Although it is not clear if this is the case for teeth with regenerative therapy, more attention should be paid to mobile teeth during the maintenance period. It was typical to find a slight improvement in radiopacity at as early as 3 months postoperatively (Fig. 5c). Signs of possible bone-fill were generally more apparent at 6 months. Sculean et al.19) reported the formation of new attachment at 6 months following EMD treatment of advanced intrabony lesions. In their study using histological analysis in humans, the formation of new attachment was not always followed by bone regeneration, although the newly formed cementum was predominantly of a cellular character. Heijl et al.7) reported that distinct radiographical bone-fill was observed as early as 5 months after surgery with EMD, and further bone gain may be expected for as long as 3 years. Radiographic imaging provides evidence for bone-fill rather than true regeneration, and the present report is based solely on clinical cases, with no histological evidence. However, based on the theoretical basis of this procedure and the cumulative evidence presented by many studies, it seems sound to assume that the results do demonstrate initial signs of regeneration. In the present study, wound healing immediately following EMD application appeared to be favorable, with few adverse events, as judged by patient perceptions as well as clini-.
(8) 91. Short-term Outcomes of EMD Therapy. cal observations. EMD may influence softtissue healing, which may cause better postoperative patient perceptions, in addition to its capability of promoting periodontal regeneration1,12,18,24). Lack of pain, improved healing of the soft tissues and limited inflammation of the operated areas have been common clinical observations following EMD therapy8,9). Ozcelik et al.14) reported that patient perceptions on the immediate post-operative period were significantly better in the non-surgery and surgery with EMD groups when compared with the surgery group. On the other hand, Zetterström et al.27) and Hagenaars et al.5) reported no differences in post-surgical healing and patient perceptions, between surgeries with EMD and flap operations. Further controlled studies are needed in order to clarify whether application of EMD induces an added healing effect on soft tissues during the early postoperative period. While the majority of cases in the present study demonstrated clinically favorable healing, it is noteworthy that 4 sites (16%) demonstrated a CAL gain of less than 2 mm. In particular, a case of tooth #37, which had poor prognosis, exhibited a particularly unfavorable outcome by 6 months. The CAL gain once confirmed at 3 months was subsequently lost, showing a PD of 7 mm at 6 months. The wide and deep 1-wall intrabony defect, which extended to the root apex, was likely to be the main cause for the poor outcome in this tooth. An occlusal overload without canine guidance might have contributed as well. These findings call for even more careful judgment based on the prognosis. With regard to possible sensitization to EMD, Froum et al.3) reported a lack of clinical adverse reactions following separate applications of EMD in the same individual. The results from our study also support this, since no adverse reactions were observed in patients after multiple applications of EMD. Like all research, the methods used in this study warrant some consideration. Since the size of the patient sample was small, no attempts were made to differentiate location of surgical sites or defect types in the data. analysis. Type of osseous defect has been shown to be important determinant in EMD treatment2). Since this was not a prospective case-controlled study, no control (flap surgery only or with placebo) data were available. Furthermore, a standardized reproducible method or computer-assisted subtraction was not utilized for analysis of intraoral radiographs. The evaluation of subgingival microflora was not performed in the patients in the present study. The effect of subgingival microflora on EMD treatment is another area that needs to be investigated. In summary, results presented in this report, of a 3 to 6 month observation period, demonstrate that periodontal surgery with EMD results in a clinically relevant reduction in PD and a gain in attachment with early signs of bone-fill. Within the limitation of the present study, treatment of intrabony defect with EMD appears to be capable of inducing favorable periodontal healing with a high level of predictability.. Acknowledgements The authors thank the dental hygienists at the Section of Dental Hygiene, Suidobashi Hospital, for their collaborative periodontal care.. References 1) Cortellini P, Tonetti MS (2007) A minimally invasive surgical technique with an enamel matrix derivative in the regenerative treatment of intra-bony defects: a novel approach to limit morbidity. J Clin Periodontol 34:87–93. 2) Froum S, Lemler J, Horowitz R, Davidson B (2001) The use of enamel matrix derivative in the treatment of periodontal osseous defects. A clinical decision tree based on biologic principles of regeneration. Int J Periodontics Restorative Dent 21:437–449. 3) Froum S, Weinberg M, Novak J, Mailhot J, Mellonig J, Van Dyke T, McClain P, Papapanou PN, Childers G, Ciancio S, Blieden T, Polson A, Greenstein G, Ykuna R, Wallace ML, Oatters.
(9) 92. 4). 5). 6) 7). 8). 9). 10). 11) 12). 13) 14). 15). Saito A et al.. M, Wagener C (2004) A multicenter study evaluating the sensitization potential of enamel matrix derivative after treatment of two infrabony defects. J Periodontol 75:1001–1008. Gestrelius S, Lyngstadaas SP, Hammarström L (2000) Emdogain — periodontal regeneration based on biomimicry. Clin Oral Invest 4:120–125. Hagenaars S, Louwerse PHG, Timmerman MF, Van der Velden U, Van der Weijden GA (2004) Soft-tissue wound healing following periodontal surgery and Emdogain® application. J Clin Periodontol 31:850–856. Hammarström L (1997) Enamel matrix, cementum development and regeneration. J Clin Periodontol 24:658–668. Heijl L, Heden G, Svardstrom G, Ostgren A (1997) Enamel matrix derivative (Emdogain®) in the treatment of intrabony periodontal defects. J Clin Periodontol 24:705–714. Jepsen S, Heinz B, Jepsen K, Arjomand M, Hoffmann T, Richter S, Reich E, Sculean A, Gonzales JR, Bodeker RH, Meyle J (2004) A randomized clinical trial comparing enamel matrix derivative and membrane treatment of buccal class II furcation involvement in mandibular molars. Part I: Study design and results for primary outcomes. J Periodontol 75:1150– 1160. Jepsen S, Topoll H, Rengers H, Heinz B, Teich M, Hoffmann T, Al-Machot E, Meyle J, JervoeStorm PM (2008) Clinical outcomes after treatment of intra-bony defects with an EMD/ synthetic bone graft or EMD alone: a multicentre randomized-controlled clinical trial. J Clin Periodontol 35:420–428. Kalpidis CDR, Ruben MP (2002) Treatment of intrabony periodontal defects with enamel matrix derivative: a literature review. J Periodontol 73:1360–1376. Miller SC (1950) Textbook of Periodontia, 3rd ed., p.125, Blakiston, Philadelphia. Murphy KG, Gunsolley JC (2003) Guided tissue regeneration for the treatment of periodontal intrabony and furcation defects. A systematic review. Ann Periodontol 8:266–302. O’Leary TJ, Drake RB, Naylor JE (1972) The plaque control record. J Periodontol 43:38. Ozcelik O, Haytac MC, Seydaoglu G (2007) Immediate post-operative effects of different periodontal treatment modalities on oral health-related quality of life: a randomized clinical trial. J Clin Periodontol 34:788–796. Rösing CK, Aass AM, Mavropoulos A, Gjermo P (2005) Clinical and radiographic effects of enamel matrix derivative in the treatment of intrabony periodontal defects: A 12-month longitudinal placebo-controlled clinical trial. 16). 17). 18). 19). 20). 21). 22). 23). 24). 25) 26). 27). in adult periodontitis patients. J Periodontol 76:129–133. Sackett DL, Rosenberg WM, Gray JA, Haynes RB, Richardson WS (1996) Evidence based medicine: what it is and what it isn’t. BMJ 312 (7023):71–72. Saito A, Nanbu Y, Nagahata T, Yamada S (2008) Treatment of intrabony periodontal defects with enamel matrix derivative in private practice: A long-term retrospective study. Bull Tokyo Dent Coll 49:89–96. Sanz M, Tonetti MS, Zabalegui I, Sicilia A, Blanco J, Rebelo H, Rasperini G, Merli M, Cortellini P, Suvan JE (2004) Treatment of intrabony defects with enamel matrix proteins or barrier membranes: results from a multicentre practice-based clinical trial. J Periodontol 75:726–733. Sculean A, Donos N, Windisch P, Brecx M, Gera I, Reich E, Karring T (1999) Healing of human intrabony defects following treatment with enamel matrix proteins or guided tissue regeneration. J Periodont Res 34:310–322. Sueda T, Hoshino J, Yamamura N (2004) Survey on results of Emdogain® use in multiple dental clinics. J Jpn Soc Periodontol 46:152– 160. (in Japanese) Tonetti MS, Lang NP, Cortellini P, Suvan JE, Adriaens P, Dubravec D, Fonzar A, Fourmousis I, Mayfield L, Rossi R, Silvestri M, Tiedemann C, Topoll H, Vangsted T, Wallkamm B (2002) Enamel matrix proteins in the regenerative therapy of deep intrabony defects. J Clin Periodontol 29:317–325. Trombelli L (2005) Which reconstructive procedures are effective for treating the periodontal intraosseous defect? Periodontol 2000 37:88–105. Wang HL, Burgett FG, Ramf jord S (1994) The influence of molar furcation involvement and mobility on future clinical periodontal attachment loss. J Periodontol 65:25–29. Wennström JL, Lindhe J (2002) Some effects of enamel matrix proteins on wound healing in the dento-gingival region. J Clin Periodontol 29:9–14. Williams RC, Offenbacher S (2000) Periodontal medicine: the emergence of a new branch of periodontology. Periodontol 2000 23:9–12. Yamanouchi K, Nakagawa T, Seida K, Saito A, Yamada S, Hiwatashi K, Setoguchi T, Chuman M, Sueda T (1994) Clinical study on the effect of absorbable membrane applied to guided tissue regeneration technique. J Jpn Soc Periodontol 36:884–894. (in Japanese) Zetterström O, Andersson C, Eriksson L, Fredriksson A, Friskopp J, Heden G, Jansson B, Lundgren T, Nilveus R, Olsson A, Renvert.
(10) Short-term Outcomes of EMD Therapy. S, Salonen L, Sjöström L, Winell A, Östrgren A, Gestrelius S (1997) Clinical safety of enamel matrix derivative (Emdogain®) in the treatment of periodontal defects. J Clin Periodontol 24:697–704.. Reprint requests to: Dr. Atsushi Saito Division of Conservative Dentistry, Department of Clinical Oral Health Science, Tokyo Dental College, 2-9-18 Misaki-cho, Chiyoda-ku, Tokyo 101-0061, Japan E-mail: [email protected]. 93.
(11)
図
関連したドキュメント
We present sufficient conditions for the existence of solutions to Neu- mann and periodic boundary-value problems for some class of quasilinear ordinary differential equations.. We
infectious disease society of America clinical practice guide- lines: treatment of drug-susceptible
(Recent result: Yes, but consistent quantum gravity is delicate.) Early universe cosmology: Observations of cosmic microwave background, maybe even earlier stages with
As can be seen, the sacred sites associated with Nichiren that are listed in regional chronicles and records of famous places are based on the en- tries found in Shinpen
Begin applications prior to or in the early stages of disease development, and continue as needed throughout the season at a 2- to 3-week interval, up to and including the day
Daoxuan 道 璿 was the eighth-century monk (who should not be confused with the Daoxuan 道宣 (596–667), founder of the vinaya school of Nanshan) who is mentioned earlier in
Amount of Remuneration, etc. The Company does not pay to Directors who concurrently serve as Executive Officer the remuneration paid to Directors. Therefore, “Number of Persons”
N 9 July 2017, the United Nations Educational, Scientific and Cultural Organization (UNE- SCO) inscribed “Sacred Island of Okinoshima and Associated Sites in the Munakata
