Pre-treatment guidelines and considerations for
an improved quality of life
Rehabilitation concepts
for edentulous patients.
無歯顎患者のための補綴修復コンセプト
Date of issue: January 2013 © Nobel Biocare Services AG, 2013
3 Rehabilitation concepts for edentulous patients
Introduction Comprehensive range of treatment solutions from the pioneer of osseointegration 4
The edentulous patient – social and functional implications 5
Planning Pre-treatment guidelines and considerations:
– Oral examination of the patient 6
– Bone resorption pattern 7
Maxilla:
– Treatment in the maxilla requires evaluation of available alveolar bone 8
– Grafting and delayed loading 10
– Transition line 11
– Considerations for the placement of 4 versus 6 implants 12
Mandible:
– Treatment of the edentulous mandible 13
3D treatment planning with NobelClinician™ 14
Guided surgery with NobelGuide® 15
Loading of implants 16
Immediate Function Clinical guideline – Immediate Function with TiUnite® implants 17
Clinical cases Mild/moderate bone resorption:
– Immediate loading for full-arch rehabilitation using NobelClinician™ 20
– Failing dentition in both arches 22
Moderate bone resorption:
– All-on-4® concept with NobelGuide® in maxilla and fl ap approach in mandible 24
Moderate/severe bone resorption:
– A predictable restorative outcome as a result of a pre-treatment evaluation
method using NobelClinician™ 26
References 28
Contents.
目 次
はじめに 即時負荷 参考文献 臨床ケース 治療計画 オッセオインテグレーションのパイオニアによる包括的治療ソリューション 無歯顎患者−社会的・機能的影響4
5
臨床ガイドライン−タイユナイト表面インプラントによる即時負荷17
28
軽度/
中等度骨吸収:
−ノーベルクリニシャンを用いた即時負荷による全顎的補綴修復 −上下顎多数歯欠損 中等度骨吸収: −オール・オン4・コンセプトによるインプラント埋入 中等度/
重度骨吸収: −ノーベルクリニシャンを用いた診査診断により予知性の高い補綴修復20
22
24
26
診査診断ガイドラインと検討事項: −口腔内検査 −骨吸収パターン 上顎: −既存骨の評価 −骨移植と遅延負荷 −トランジションライン −インプラント埋入本数の検討(4
本vs 6
本) 下顎: −無歯顎症例 ノーベルクリニシャンを用いた3Dプランニング ノーベルガイド・コンセプトによるガイディッド・サージェリー インプラントの荷重6
7
8
10
11
12
13
14
15
16
無歯顎患者のための補綴修復コンセプトRehabilitation concepts for edentulous patients // Introduction 4
Comprehensive range of
treatment solutions from the
pioneer of osseointegration.
In close cooperation with experienced clinicians and opinion leaders, Nobel Biocare has set the standard for integrated solutions for the treatment of edentulous patients and patients with a failing/terminal dentition. Clinicians can choose from a comprehensive range of implant-based fi xed and fi xed-removable restorations that can be custom designed to meet every patient’s specifi c needs. Compared to conventional removable dentures, these implant-based solutions provide superior benefi ts to the patients and help them improve their quality of life.
From the restorative perspective, there is broad fl exibility in the fi nal prosthetic design. CAD/CAM designed frameworks, bridges and bars in different materi-als meet the different patient conditions and needs, enabling clinicians to deliver precision-milled reconstructions with a passive and excellent fi t.
This guide on rehabilitation concepts for edentulous patients has been developed together with a group of experts to aid clinicians in their selection of the appropri-ate treatment for their patients based on the individual clinical parameters. All treatment concepts shown in this guide are supported by scientifi c evidence. For more information on Quality of Life studies, scientifi c evidence and other related publications, please refer to page 28.
Dr. Edmond Bedrossian USA Dr. Paulo Malo Portugal Dr. Steve Parel USA Dr. Enrico Agliardi Italy Dr. Lesley David Canada Dr. Charles Babbush USA Dr. Hannes Wachtel Germany Dr. Jack Hahn USA In tr o d u ct io n M ax ill a P la n n in g M an d ib le Im m ed ia te F u n ct io n C lin ic al c as es R ef er en ce s
オッセオインテグレーションのパイオニアによる
包括的治療ソリューション
ノーベルバイオケアは、経験豊富な臨床家とオピニオンリーダーの緊密な協力の もと、無歯顎症例または多数歯欠損症例の治療のために包括的ソリューションの スタンダードを確立しました。幅広い選択肢の中から、個々の患者様のニーズに 合わせてカスタマイズできるインプラント支持の固定式または可撤式補綴物を お選びいただけます。インプラント支持の補綴物は、従来の可撤式義歯と比較して さまざまな利点があり、患者様のQOL改善につながります。 補綴の観点から見た場合、最終補綴物のデザインには幅広い柔軟性があります。 種々の材料でCAD/CAMシステムにより設計されるフレームワーク、ブリッジおよび バーは個々の患者様の条件やニーズを満たし、また、精密な削り出しにより製作 されるため、パッシブフィットの獲得が可能です。 本書は、個々の臨床条件に基づいて、患者様に適した治療を選択できるように 専門家グループの協力のもとに作成されました。 本書で説明する治療コンセプトは、すべて科学的根拠によって裏付けられています。 参考文献については、28ページをご参照ください。
治療計画 上 顎 下 顎 即時 負 荷 臨床 ケ ー ス 参考文献 は じ め に 無歯顎患者のための補綴修復コンセプト // はじめにRehabilitation concepts for edentulous patients // Introduction 5 20% 25% 44% 42% 14% 15% 7% 6% 10% 5% 4% 8%
The edentulous patient – social
and functional implications.
The use of dental implants to improve patients’ quality of life has been docu-mented in a multitude of publications. The embarrassment caused by dentures moving during social interactions and the constant preoccupation with attempts to stabilize them leaves the majority of patients dissatisfi ed with this treatment option, as reported in the Quality of Life studies. The use of dental implants im-proves patients’ speech, esthetics, function and self-esteem. The overall improve-ment of patients’ social life, self-image, comfort as well as the internal loading of the alveolar bone halting its further resorption, make dental implants a predictable and reliable treatment option over conventional dentures.
A literature review from the National Library of Medicine has described edentu-lism as a global issue, with estimates for an increasing demand for complete denture prosthesis in the future. Patients with complete edentulism were found to be at higher risk of poor nutrition with higher incidence of coronary artery plaque formation. Chronic residual ridge resorption continues to be the primary intra-oral complication of edentulism. Without the use of dental implants there appears to be few opportunities to reduce bone loss.
Edentulism is a very common handicap and there is a tremendous need for differ-ent solutions to treat this group of patidiffer-ents. Complete eddiffer-entulism is the terminal outcome of multifactorial processes involving biological and patient-related fac-tors. It represents a tremendous global health care burden, and will do so for the foreseeable future. The demand for treatment extends to millions of edentulous people – more than 40 million in the Western world, and 250 million in Asia. Of the total population worldwide, around 6–10% are edentulous.*
Dental implants are well-documented to improve edentulous patients’ quality of life.
Patients with complete eden-tulism seem to be at risk for multiple systematic disorders if left untreated.
The enormous global demand for edentulous solutions will continue to increase.
Western world Asia
* Source: WHO and Nobel Biocare estimates.
Visit WHO http://www.whocollab.od.mah.se/countriesalphab.html for more details.
250 million people are edentulous in Asia: 67% live in China and India.
40 million people are edentulous in the Western world: 64% live in the USA and Brazil.
USA Brazil Other UK Germany Canada Italy China India Other Japan Indonesia R ef er en ce s C lin ic al ca se s Im m ed ia te F u n ct io n M an d ib le P la n n in g M ax illa In tro d u ct io n
無歯顎患者−社会的・機能的影響
歯科用インプラントによる治療が患者様のQOLを改善することを裏付けるデータ は、多数の文献で報告されています。研究によれば、義歯を使用している場合、 会話中の義歯のずれが気になるなど、多くの方がこの治療選択肢に不満を抱いて います。歯科用インプラントを使用すると、発音や審美性、機能性が改善され、 自尊心を取り戻すことができます。歯科用インプラントは患者様の社会生活や自己 イメージ、快適さといった問題を総合的に改善するのみならず、顎骨に適切な 負荷をかけることにより骨吸収の進行も抑制する可能性があるため、従来の義歯に 比べて予知性の高い、信頼できる治療選択肢であるといえます。National Library of Medicineに掲載された文献レビューによれば、無歯顎は
世界的な問題であり、今後、総義歯の需要は増大すると予測されています。完全 無歯顎のケースでは栄養不良のリスクが高く、冠動脈プラークの形成率が高いこと が分かっています。また、無歯顎症例の重大な口腔内合併症として、残存する顎堤の 慢性的な骨吸収が進行、持続します。現段階では、歯科用インプラントが骨吸収を 抑制する有効な手段であると思われます。 無歯顎は極めて一般的なハンディキャップであり、無歯顎治療のソリューションに 対するニーズは膨大です。完全無歯顎は、生物学的要因と患者独自の要因によって 起こる多因子性プロセスの終末的な結果です。無歯顎は世界中の医療費に莫大な 負担をかけており、今後もしばらくこの状態は続くと思われます。無歯顎治療の 需要は膨大であり、欧州・米州では無歯顎者は4千万人、アジアでは2億5千万人 以上にのぼります。世界総人口の実に6∼10%が無歯顎者と推定されています*。 歯科用インプラントが無歯顎患者 のQOL
を改善することを裏付ける データは数多く報告されています。 完全無歯顎の状態で治療せずに 放置すると、さまざまな系統的障害 を来す危険性があります。 無歯顎のソリューションに対する 世界的需要は膨大であり、今後も 増大し続けると推定されています。 欧州・米州 米国 ブラジル その他 英国 ドイツ カナダ イタリア 中国 インド その他 日本 インドネシア アジア 欧州・米州では4千万人が無歯顎者: 64%が米国およびブラジル居住者。 アジアでは 2億5千万人が無歯顎者: 67%が中国およびインド居住者。 * WHOおよびノーベルバイオケア社の推定。 治療計画 上 顎 下 顎 即時 負 荷 臨床 ケ ー ス 参考文献 は じ め に 無歯顎患者のための補綴修復コンセプト // はじめにRehabilitation concepts for edentulous patients // Planning 6
Pre-treatment guidelines and
considerations – oral examination
of the patient.
A thorough pre-treatment evaluation of edentulous patients or patients with failing/terminal dentition is necessary to establish a predictable treatment outcome. The aim of this guide is to assist clinicians in following suggestions in a systematic format and protocol, allowing for the formulation of a comprehensive treatment plan. To begin the evaluation of this group of patients, the following may be taken into consideration:
1 Medical history and chief complaint
Any conditions that might affect the result or infl uence can-didacy as a surgical patient are noted here. Consideration for referral for medical clearance as indicated.
2 Dental history
Ascertain the patient’s expectations, past dental history with dental failure, e.g. periodontal disease, admitted or known habits including clenching and bruxing.
3 Radiographic analysis
Initial radiographic evaluation may be done with the help of a panoramic radiograph (OPG). Upon the discretion of the practitioner, a full mouth periapical series (FMX/FMS), a medical CT scan or a CBCT (cone beam CT) analysis prior to the fi nal decision may be considered.
4 Intra- and extra-oral examination
Evaluate the condition of the remaining teeth documenting caries, occlusion, occlusal discrepancies and migration of teeth. For patients with remaining teeth, the oral examina-tion is always based on periodontal fi ndings and disease status of remaining teeth and soft tissue. This includes a full pocket depth charting with mobility, recession, furcation, bleeding, suppuration and apical lesions, all being noted. For both patients with partial and complete edentulism, the general and specifi c soft tissue conditions are also docu-mented. The soft tissue examination identifi es any palpated area observed in the oral cavity and oralpharynx, as well as evaluation of the temporomandibular joint (TMJ). The smile analysis is part of the external facial examination, which includes a neck examination for any palpable lymph nodes.
5 Treatment planning
To begin a systematic pre-treatment evaluation of the patient, the following information during the evaluation may also be helpful:
I) Presence or lack of hard and soft tissue: may aid the practitioner to determine the type of fi nal prosthesis to fabricate.
II) “Transition Line”: determination of a hidden or visible transition line can assist in determining potential esthetic considerations and needs.
III) “Zones/Groups of the Maxilla”: could be helpful for the practitioner in presenting a particular surgical and restor-ative treatment protocol. For more information regarding the overview of bone resorption patterns and treatment examples, please refer to pages 8–9 in this guide. IV) The use of 3D software such as NobelClinician is also
advisable to evaluate the potential sites for implant placement.
After implant treatment, an individual maintenance program (oral hygiene instructions etc.) for the patient is important to secure a favorable long-term treatment outcome.
The fi nal phase in treatment planning includes an in-depth presentation of all appropriate treatment options. Any dis-crepancies in the bone or anticipated esthetic or functional limitations to proposed treatment are documented here. Final acceptance to the plan is documented with patient confi rmation. In tr o d u ct io n M ax ill a P la n n in g M an d ib le Im m ed ia te F u n ct io n C lin ic al c as es R ef er en ce s
診査診断ガイドラインと検討事項
−口腔内検査
予知性の高い治療法の確立には、無歯顎患者または多数 歯欠損患者の十分な診査診断が不可欠です。本書の目的は、 系統的なフォーマットとプロトコルに従った診査診断の実行 を提案することにより、包括的な治療計画の策定を支援する ことです。1.
全身的既応歴および主訴 手術の可否または結果に影響を与える可能性のあるあらゆる 疾患はすべて記録します。健康診断が必要な場合は、別途 検討してください。2.
歯科的既応歴 患者の要望、歯周病等の疾患を含む歯科病歴のほか、クレン チングやブラキシズム等の習慣がないか確認します。3. X
線検査 パノラマX線写真(OPG)により初期X線評価を行います。 最終的な意思決定を行う前に、術者の裁量でデンタルX線 撮影(10枚法/18枚法)、医科用CTスキャンまたはCBCT (コーンビームCT)の実施を検討します。4.
口腔内および口腔外検査 残存歯の状態を評価し、カリエス、不正咬合および歯の位置 異常などを記録します。残存歯のある患者に関しては、口腔内 検査で必ず残存歯および軟組織の歯周所見および疾患の 状態を評価します。歯周ポケットの深さ、歯の動揺、歯肉退縮、 歯根分岐部、出血、排膿および根尖部病変等をチェックし、 すべて記録します。部分欠損患者または完全無歯顎患者の いずれについても、軟組織の総体的および具体的な状態を 記録します。軟組織の検査では、口腔および咽頭はもちろん、 顎関節(TMJ)もチェックします。口腔外顔貌検査ではスマイル 検査を行い、頸部リンパ節を触診します。5.
治療計画 系統的な診査診断を行うには、次の情報が有用であると 思われます。I)
硬組織および軟組織の有無:術者が最終補綴物のタイプ を決定する際に重要です。
II
)トランジションライン:トランジションラインが見えている か、または隠れているかを確認することにより審美的 ニーズと検討事項を判断することができます。
III
)上顎のゾーン
/
グループ分類:術者が具体的な外科および 補綴プロトコルを提示するのに役立つ可能性があります。 骨吸収パターンと治療例の概要については、本書の8
∼9
ページを参照してください。IV)
インプラント埋入部位の確認に際しては、ノーベルクリニ シャンのような3Dソフトウェアの使用も推奨されます。 インプラント治療後、良好な状態を維持するためには、個別 のメインテナンス・プログラム(口腔衛生の指導等)が重要 となります。 治療計画の最終段階では、すべての適切な治療選択肢を 詳細に提示します。骨の状態や提案する治療の審美的または 機能的限界についても、すべて記録します。患者の同意を 得て、治療計画に対する最終受諾を記録します。 は じ め に 上 顎 下 顎 即時 負 荷 臨床 ケ ー ス 参考文献 治療計画 無歯顎患者のための補綴修復コンセプト // 治療計画
Rehabilitation concepts for edentulous patients // Planning 7 P la n n in g M ax illa In tro d u ct io n
Rehabilitation concepts for edentulous patients // Planning 7
No resorption (tooth-only defect) Maxilla
Mandible
Mild composite defect Moderate composite defect Advanced composite defect It is very important to understand the degree of the existing volume of hard and
soft tissue loss, as this degree of atrophy directs the restorative protocol. This means that the remaining alveolar bone directs the surgical protocol, which in turn supports the restorative treatment plan.
Pre-treatment guidelines and
considerations – bone resorption
pattern.
Bone resorption
How much hard and soft tissue is missing? What is to be replaced? Is there a “Composite Defect”?*
* Bedrossian E et al. Fixed-prosthetic Implant Restoration of the Edentulous Maxilla: A Systematic Pretreatment Evaluation Method. J Oral Maxillofac Surg 2008;66:112-22
R ef er en ce s C lin ic al ca se s Im m ed ia te F u n ct io n M an d ib le P la n n in g M ax illa In tro d u ct io n
診査診断ガイドラインと検討事項
−骨吸収パターン
硬組織および軟組織の残存量の程度を把握することは、極めて重要です。この 吸収の程度により、補綴プロトコルが決定します。すなわち、残存する顎骨が外科 プロトコルを決定し、これにより補綴治療計画が左右されることを意味します。 硬組織および軟組織はどれほど吸収しているか? 何を置換すべきか?複合欠損はあるか?* 上 顎 吸収なし (歯の欠損のみ) 軽度複合欠損 中等度複合欠損 骨吸収 高度複合欠損 下 顎 は じ め に 上 顎 下 顎 即時 負 荷 臨床 ケ ー ス 参考文献 治療計画 無歯顎患者のための補綴修復コンセプト // 治療計画Rehabilitation concepts for edentulous patients // Planning 8 M ax ill a P la n n in g M an d ib le Im m ed ia te F u n ct io n C lin ic al c as es R ef er en ce s
上顎の症例では利用可能な既存骨の評価が
不可欠である
グループ1
ゾーンⅠ、ⅡおよびⅢに骨が存在 ゾーンⅠおよびⅡに骨が存在 ゾーンⅠにのみ骨が存在 グループ2
グループ3
骨吸収 は じ め に 下 顎 即時 負 荷 臨床 ケ ー ス 参考文献 上 顎 治療計画 無歯顎患者のための補綴修復コンセプト // 治療計画Rehabilitation concepts for edentulous patients // Planning 9 P la n n in g M ax illa In tro d u ct io n
Rehabilitation concepts for edentulous patients // Planning 9
Bone resorption
Treatment example Group 1
Treatment example Group 2
Treatment example Group 3 Surgical solution
Axial (straight) implants Restorative solution Screw-retained implant bridge
Surgical solution
Tilted implant concept All-on-4, bone graft or axial implants with cantilever
Restorative solution
Fixed or fi xed-removable solution
Surgical solution Tilted implant concept Brånemark System Zygoma or bone graft
Restorative solution Fixed or fi xed-removable prosthesis
The following publications have been used as support to pre-evaluate important factors as part of the decision making process for the edentulous treatment: – Bedrossian E et al. Fixed-prosthetic Implant Restoration of the Edentulous Maxilla: A Systematic Pretreatment Evaluation Method.
J Oral Maxillofac Surg 2008;66:112-22
– Maló P et al. The rehabilitation of completely edentulous maxillae with different degrees of resorption with four or more immediately loaded implants: a 5-year retrospective study and a new classifi cation. Eur J Oral Implantol 2011;4(3):227-43
R ef er en ce s C lin ic al ca se s Im m ed ia te F u n ct io n M an d ib le P la n n in g M ax illa In tro d u ct io n 治療例
グループ
1
治療例グループ
2
治療例グループ
3
外科ソリューション 垂直(ストレート)インプラント 補綴ソリューション スクリュー固定式インプラントブリッジ 外科ソリューション 傾斜インプラント(ブローネマルクシステム・ ザイゴマ)または骨移植 補綴ソリューション 固定式または可撤式の補綴物 外科ソリューション 傾斜インプラント(オール・オン4・コンセプト)、 骨移植または垂直インプラント+カンチレバー 補綴ソリューション 固定式または可撤式の補綴物 無歯顎治療のための意思決定プロセスにおいて事前評価を行うべき重要な因子の裏付けとして、以下の文献を参考にしています。 は じ め に 下 顎 即時 負 荷 臨床 ケ ー ス 参考文献 上 顎 治療計画 無歯顎患者のための補綴修復コンセプト // 治療計画Rehabilitation concepts for edentulous patients // Planning 10
Designing for Life
7–year follow-upCase courtesy of Dr. Paulo Malo, Portugal
For patients with pneumatized sinus, the grafting of the maxillary sinus fl oor is certainly an option. The Consensus Report* of 1996 regards maxillary sinus graft-ing to be a viable procedure with a success rate of 90% or greater. However, im-mediate loading of these cases is not recommended and the two-stage delayed loading protocol should be followed.
* Jensen OT, Shulman LB, Block MS, Iacono VJ. Report of the Sinus Consensus Conference of 1996. Int J Oral Maxillofac Implants.1998;13 Suppl:11-45
Grafting and delayed loading.
In tr o d u ct io n M ax ill a P la n n in g M an d ib le Im m ed ia te F u n ct io n C lin ic al c as es R ef er en ce s
骨移植と遅延負荷
上顎洞底の低い患者においては、上顎洞底挙上術が選択肢の1つであることは 間違いありません。1996年のConsensus Report*によれば、上顎洞底挙上術は
成功率90%以上の実行可能な術式です。しかし、このような症例では即時負荷は 推奨されず、2回法の遅延負荷プロトコルが適用されます。
7年後のフォローアップ写真 提供: は じ め に 下 顎 即時 負 荷 臨床 ケ ー ス 参考文献 上 顎 治療計画 無歯顎患者のための補綴修復コンセプト // 治療計画Rehabilitation concepts for edentulous patients // Planning 11
Transition line.
Evaluation of the esthetics of the fi nal prosthesis is made by recognizing the transition line between the prosthesis and the crestal soft tissues of the edentu-lous ridge. If the transition line is apical to the smile line, an esthetic outcome is predictable. However, if the smile line is apical to the transition line, further evalu-ation should be made, as the fi nal esthetic outcome may be compromised.
Transition line (in green) is apical to the smile line (in red) with an esthetic outcome.
Transition line (in green) is coronal to the smile line (in red) with an unesthetic outcome. R ef er en ce s C lin ic al ca se s Im m ed ia te F u n ct io n M an d ib le P la n n in g M ax illa In tro d u ct io n
トランジションライン
最終補綴物の審美性の評価は、軟組織と補綴物の位置関係によって決定します。 トランジションライン(下図の緑線)がスマイルライン(下図の赤線)に対して根尖側 にある場合は、審美的な修復治療のコントロールが可能となります。一方、トランジ ションラインがスマイルラインに対して歯冠側にある場合は、審美的な修復治療の コントロールが難しくなる可能性がありますので、さらに詳細な評価を行うべきです。 トランジションライン(緑色) がスマイルライン(赤色)に 対して根尖側にあり、審美性 がある。 トランジションライン(緑色) がスマイルライン(赤色)に 対して歯冠側にあり、審美性 に欠ける。 は じ め に 下 顎 即時 負 荷 臨床 ケ ー ス 参考文献 上 顎 治療計画 無歯顎患者のための補綴修復コンセプト // 治療計画Rehabilitation concepts for edentulous patients // Planning 12
Designing for Life
8–year follow-upCase courtesy of Dr. Enrico Agliardi, Italy
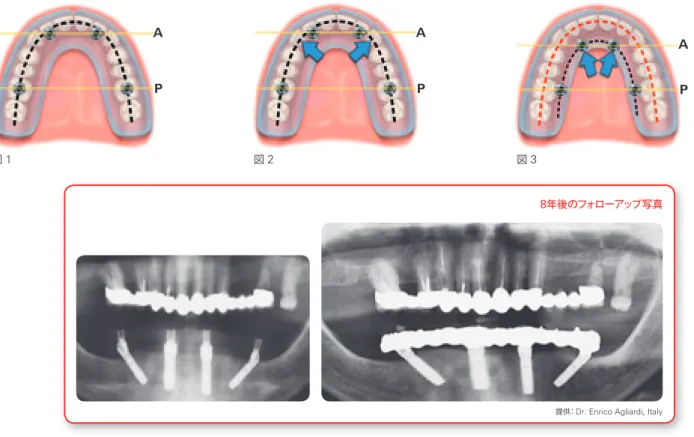
A P A P A P
Figure 1 Figure 2 Figure 3
In planning the position and the number of implants to place, it is important to consider the functional and biomechanical properties of the fi xed, implant-supported, fi nal prosthesis.
As reported (Silva et al. 2010, Bevilacqua et al. 2010),* the anterior-posterior spread (AP-spread) of the implants is important in limiting or eliminating the posterior cantilever. Tilting the posterior implants (All-on-4 or Zygoma concept) distalizes the implant platform (Krekmanov et al. 2000)** and a larger AP-spread is achieved, reducing the forces on the distal implants (fi gure 1).
However, during lateral function, increased stress values on the framework are observed, which may be addressed by the addition of two implants in the canine region (fi gure 2). In the resorbed maxilla
The resorption pattern of the maxilla (dictated by the black line in fi gure 3) may not allow for the placement of six implants. Therefore, four implants are placed. By distributing four implants as shown in fi gure 3, the biomechanical properties of the fi nal prosthesis are addressed by maintaining the AP-spread as well as lending support in lateral excursions.
Considerations for the placement
of 4 versus 6 implants.
* Silva GC, Mendonça JA, Lopes LR, Landre J Jr. Stress Patterns on Implants in Prostheses Supported by Four or Six Implants :A Three-Dimensional Finite Element Analysis. Int J Oral Maxillofac Implants 2010;25:239-46
* Bevilacqua M, Tealdo T, Menini M, Pera F, Mossolov A, Drago C, Pera P. The infl uence of cantilever length and implant inclination on stress distribution in maxillary implant supported fi xed dentures. J Prosthet Dent 2010;105:5-13
** Krekmanov L, Kahn M, Rangert B, Lindström H. Tilting of Posterior Mandibular and Maxillary Implants for Improved Prosthesis Support. Int J Oral Maxillofac Implants 2000; 15:405-14 In tr o d u ct io n M ax ill a P la n n in g M an d ib le Im m ed ia te F u n ct io n C lin ic al c as es R ef er en ce s
Rehabilitation concepts for edentulous patients // Planning 12
Designing for Life
8–year follow-upCase courtesy of Dr. Enrico Agliardi, Italy
A P A P A P
Figure 1 Figure 2 Figure 3
In planning the position and the number of implants to place, it is important to consider the functional and biomechanical properties of the fi xed, implant-supported, fi nal prosthesis.
As reported (Silva et al. 2010, Bevilacqua et al. 2010),* the anterior-posterior spread (AP-spread) of the implants is important in limiting or eliminating the posterior cantilever. Tilting the posterior implants (All-on-4 or Zygoma concept) distalizes the implant platform (Krekmanov et al. 2000)** and a larger AP-spread is achieved, reducing the forces on the distal implants (fi gure 1).
However, during lateral function, increased stress values on the framework are observed, which may be addressed by the addition of two implants in the canine region (fi gure 2). In the resorbed maxilla
The resorption pattern of the maxilla (dictated by the black line in fi gure 3) may not allow for the placement of six implants. Therefore, four implants are placed. By distributing four implants as shown in fi gure 3, the biomechanical properties of the fi nal prosthesis are addressed by maintaining the AP-spread as well as lending support in lateral excursions.
Considerations for the placement
of 4 versus 6 implants.
* Silva GC, Mendonça JA, Lopes LR, Landre J Jr. Stress Patterns on Implants in Prostheses Supported by Four or Six Implants :A Three-Dimensional Finite Element Analysis. Int J Oral Maxillofac Implants 2010;25:239-46
* Bevilacqua M, Tealdo T, Menini M, Pera F, Mossolov A, Drago C, Pera P. The infl uence of cantilever length and implant inclination on stress distribution in maxillary implant supported fi xed dentures. J Prosthet Dent 2010;105:5-13
** Krekmanov L, Kahn M, Rangert B, Lindström H. Tilting of Posterior Mandibular and Maxillary Implants for Improved Prosthesis Support. Int J Oral Maxillofac Implants 2000; 15:405-14 In tr o d u ct io n M ax ill a P la n n in g M an d ib le Im m ed ia te F u n ct io n C lin ic al c as es R ef er en ce s
インプラント埋入本数の検討(
4
本
vs 6
本)
インプラントの埋入本数および埋入位置の計画に際しては、 インプラント支持の最終補綴物の機能的および生体力学的 特性を検討することが重要です。Silvaら(2010)およびBevilacquaら(2010)
*が述べるよう
に、臼歯部のカンチレバーを制限ないし取り除くためには、 インプラントのアンテロポステリアスプレッド(APスプレッド)
が重要になります。臼歯部のインプラントを傾斜させる ことにより(オール・オン4またはザイゴマ・コンセプト)、 インプラントのプラットフォームをより遠心側に配置し (Krekmanovら、2000)
**、より大きなAPスプレッドを確保
することにより、遠心側インプラントにかかる応力を減じる ことができます(図1)。 一方で、側方機能時にフレームワークにかかる応力値は増大 しますが、これは犬歯部にインプラントを2本追加すること により対処することができます(図2)。 骨吸収のある上顎 上顎に大きな骨吸収があると(図3で黒線により描出)、6本の
インプラントを埋入できない可能性があり、このような場合は4本のインプラントを埋入します。
4本のインプラントを図3
のように分布させることにより、APスプレッドを確保し、側方
運動を支持することにより、最終補綴物の生体力学的特性 に対処します。 図 1 図 2 図 3 8年後のフォローアップ写真 提供: は じ め に 下 顎 即時 負 荷 臨床 ケ ー ス 参考文献 上 顎 治療計画 無歯顎患者のための補綴修復コンセプト // 治療計画Rehabilitation concepts for edentulous patients // Planning 13
Axial implants with a fi xed NobelProcera Implant Bridge
Axial and tilted implants with Multi-unit Abutments and a fi xed NobelProcera Implant Bridge
Two axial implants with Locator® Abutments and a removable prosthesis
Axial implants with a fi xed-removable NobelProcera Implant Bar Overdenture
Although it is possible to have a tooth-only defect in the edentulous mandible, most patients present some degree of bone resorption. The surgical treatment options for this group of patients include axially placed or tilted implants to support a fi xed NobelProcera Implant Bridge or a fi xed-removable NobelProcera Implant Bar Overdenture. The use of two axial implants to retain an overdenture in the mandible is a valid option that may also be considered.
Treatment of the
edentulous mandible.
Locator® is a trademark of Zest Anchors Inc. Treatment examples R ef er en ce s C lin ic al ca se s Im m ed ia te F u n ct io n M an d ib le P la n n in g M ax illa In tro d u ct io n
下顎無歯顎の治療
下顎無歯顎は歯牙欠損のみの可能性もありますが、症例の大半はある程度の 骨吸収を呈します。下顎無歯顎患者の外科的治療の選択肢としては、垂直または 傾斜埋入インプラントにより固定式のノーベルプロセラ インプラント ブリッジまた は可撤式のノーベルプロセラ インプラントバー オーバーデンチャーを使用する
方法が挙げられます。また、下顎に2本のインプラントを垂直埋入し、オーバー デンチャーを支持する方法も、有効な選択肢の1つとして検討することができます。 治療例 垂直方向に埋入したインプラント+固定式ノーベル プロセラインプラントブリッジ 垂直方向に埋入したインプラント+ノーベルプロセラ インプラントバーオーバーデンチャー(術者可撤式 または患者可撤式義歯) 垂直および傾斜埋入インプラント+マルチユニット・ アバットメント+固定式ノーベルプロセラインプラント ブリッジ 垂直方向に埋入したインプラント2本+ノーベル ロケーター・アバットメント+患者可撤式義歯 は じ め に 上 顎 即時 負 荷 臨床 ケ ー ス 参考文献 下 顎 治療計画 無歯顎患者のための補綴修復コンセプト // 治療計画Rehabilitation concepts for edentulous patients // Planning 14
One of the key tools needed for treatment planning is the patient’s radiograph. The use of the panoramic radiograph (OPG) as the scout fi lm is indicated for all patients. In cases where further study of the patient’s remaining alveolar bone is needed, a 3D study using the medical CT or CBCT (cone beam CT) scan may be obtained.
For clinicians who choose to relate the proposed implant positions to the patient’s available topography of the bone, the use of the 3D treatment planning software NobelClinician is available. By importing the patients DICOM fi les into the NobelClinician Software, the practitioner is able to “virtually” plan the implant posi-tions including diameter, length and angulation in a 3D environment.
NobelClinician Software
CBCT frontal view
3D treatment planning with
NobelClinician
™
.
In tr o d u ct io n M ax ill a P la n n in g M an d ib le Im m ed ia te F u n ct io n C lin ic al c as es R ef er en ce sノーベルクリニシャンを用いた
3D
プランニング
治療計画において重要なツールの1つが、患者のX線写真です。いずれの症例に おいても、単純X線写真としてのパノラマX線写真(OPG)は不可欠です。残存する 顎骨の詳細な評価が必要な場合は、医科用CTまたはCBCT(コーンビームCT) スキャンを用いて3D画像を撮影します。 骨の状態を確認しながらインプラント埋入位置を決定する場合は、3Dプランニング・
ソフトウェア「ノーベルクリニシャン」を利用することができます。患者のDICOM データをノーベルクリニシャン・ソフトウェアにインポートすることにより、3D環境で
径、長さおよび角度を含めたインプラント埋入位置のバーチャル・プランニングを 行うことができます。 CBCT正面像 ノーベルクリニシャン・ソフトウェア は じ め に 上 顎 下 顎 即時 負 荷 臨床 ケ ー ス 参考文献 治療計画 無歯顎患者のための補綴修復コンセプト // 治療計画Rehabilitation concepts for edentulous patients // Planning 15
Designing for Life
16–year follow-upCase courtesy of Dr. Hannes Wachtel, Germany
Guided surgery with NobelGuide®.
The diagnostic and treatment planning options for the clinician are enhanced by the use of the NobelClinician Software.
The software may be used in one or all of its functions: 1. Treatment plan only – NobelClinician Software
2. Designing the surgical template for guided surgery – NobelGuide treatment concept
After 3D treatment planning using the NobelClinician Software, the surgeon may choose to perform guided surgery with NobelGuide. A surgical template may be produced from the planning software, allowing the surgeon to perform a guided fl apless or mini-fl ap surgical procedure.
The expanded use of the NobelGuide concept allows for preoperative fabrication of a provisional all-acrylic bridge/prosthesis, which may be immediately connected after the implants have been placed using the surgical template.
The use of the NobelClinician Software as a 3D treatment planning tool allows for a comprehensive understanding of the bony anatomy as well as the existing vital structures. It also allows for the positioning of the proposed implants onto the patient’s 3D radiograph. The expanded use, the surgical template and the fabrica-tion of an all-acrylic bridge may be an opfabrica-tion to consider by the implant treatment team.
Prefabricated all-acrylic provisional bridge
Surgical template for the All-on-4/ NobelGuide concept
* Bedrossian E et al, Fixed-prosthetic Implant Restoration of the Edentulous Maxilla: A Systematic Pretreatment Evaluation Method. J Oral Maxillofac Surg 66:112-122,2008.
R ef er en ce s C lin ic al ca se s Im m ed ia te F u n ct io n M an d ib le P la n n in g M ax illa In tro d u ct io n
ノーベルガイド・コンセプトによる
ガイディッド・サージェリー
ノーベルクリニシャン・ソフトウェアを利用することにより、診査・診断・治療計画 の選択肢が広がります。 本ソフトウェアは、次の機能のいずれにも使用することができます。1.
治療計画のみ−ノーベルクリニシャン・ソフトウェア2.
ガイディッド・サージェリーに使用するサージカルテンプレートの設計−ノーベル ガイド・コンセプト ノーベルクリニシャン・ソフトウェアによる3Dプランニングが完了したら、ノーベル ガイド・コンセプトによるガイディッド・サージェリーを行うことができます。ノーベル クリニシャン・ソフトウェアからサージカルテンプレートを作製し、フラップレス またはフラップ手術を行うこともできます。 また、ノーベルガイド・コンセプトを利用して術前にプロビジョナル・レストレーション の製作が可能なため、サージカルテンプレートを利用してインプラントを埋入後、 ただちにプロビジョナルを装着することができます。 ノーベルクリニシャン・ソフトウェアを3Dプランニングツールとして利用すると、 骨の解剖学的特徴のみならず、重要な周囲組織を包括的に把握することができます。 また、提案するインプラントを患者の3D X線画像に配置することもできます。 サージカルテンプレートおよびプロビジョナル・レストレーションの術前製作も、 インプラント治療チームが検討すべき選択肢の1つです。 サージカルテンプレート (ノーベルガイドによるオール・オン4) 術前に製作されたプロビジョナル・ レストレーション 16年後のフォローアップ写真 提供: は じ め に 上 顎 下 顎 即時 負 荷 臨床 ケ ー ス 参考文献 治療計画 無歯顎患者のための補綴修復コンセプト // 治療計画Rehabilitation concepts for edentulous patients // Planning 16 Resonance Frequenc y Analysis RF A (Hz) 0 1 2 3 4 5 6 7 8 7000 6800 6600 6400 6200 6000
Higher stability with immediately loaded implants with TiUnite surface than with the same implants with machined surface in the posterior maxilla (Glauser et al. 2001).**
High stability in the critical healing phase
TiUnite machined surface
Time after implantation (months) After successful placement of the implants, immediate, early or delayed loading
may be considered. If the two-stage approach is the treatment of choice, the patients utilize their existing dentures during the osseointegration phase. If im-mediate loading of the newly placed implants is desired, consider the following protocol and rationale:
Immediate loading of implants is facilitated in part by the modifi cation of the implant surface generally referred to as “moderately rough surface”. This modifi -cation has led to higher predictability when adopting the immediate load concept. Reports of high cumulative survival rates (up to 100%) have been published using the TiUnite implant surface.
Studies have shown that the bone formation pattern on TiUnite differs from machined implants (Schüpbach et al. 2005, Zechner et al. 2003).* The difference emanates from the strong osseoconductive properties of TiUnite, which results in rapid bone growth along the implant surface and stable anchorage in surrounding bone. This is of particular importance when using the immediate load concept, and for implant treatment in soft bone and sub-optimal healing cases. Due to the formation of new bone directly on the implant surface, the mechanical stability can be maintained at a higher level throughout the healing phase compared with machined implants (Glauser et al. 2001).** Thus, TiUnite implants have allowed for higher predictability when using the immediate load concept, especially in regions with soft bone and sub-optimal healing.
The various criteria for the immediate loading of implants have been reported in the literature. Initial stability of implants is essential for a successful treatment. It is important to highlight that a minimum of 35 Ncm of insertion torque is required if immediate loading is being considered. The implant has to withstand a fi nal tightening torque of minimum 35 Ncm. This can be verifi ed by the use of the surgical manual torque wrench. If the implant does not rotate further, the initial stability of the implant is considered adequate for immediate loading.
Osteoblast on the TiUnite implant sur-face (courtesy of Dr Peter Schüpbach, Switzerland).
Loading of implants.
* Schüpbach P, Glauser R, Rocci A, Martignoni M, Sennerby L, Lundgren A, Gottlow J. The human bone-oxidized titanium implant interface: A light microscopic, scanning electron microscopic, back-scatter scanning electron microscopic, and energydispersive x-ray study of clinically retrieved dental implants. Clin Implant Dent Relat Res. 2005;7 Suppl 1:36-43
* Zechner W, Tangl S, Furst G, Tepper G, Thams U, Mailath G, Watzek G. Osseous healing characteristics of three different implant types. Clin Oral Implants Res 2003;14:150-7
** Glauser R, Portmann M, Ruhstaller P, Lundgren AK, Hammerle CH, Gottlow J. Stability measurements of immediately loaded machined and oxidized implants in the posterior maxilla. A com-parative clinical study using resonance frequency analysis. Applied Osseointegration Research 2001; 2:27-9
In tr o d u ct io n M ax ill a P la n n in g M an d ib le Im m ed ia te F u n ct io n C lin ic al c as es R ef er en ce s
インプラントの荷重
インプラント埋入後、即時、早期または遅延負荷のいずれのプロトコルを採用 するかについて検討します。2回法を選択した場合は、オッセオインテグレーション
が獲得されるまでの期間中、既存の義歯を使用します。即時負荷を採用する場合は、 以下のプロトコルと理論を検討してください。 インプラントの即時負荷は、インプラント表面を粗面加工処理することにより、 予知性が向上し、タイユナイト・インプラントを用いた試験研究では、高い累積 残存率(最大で100%)が報告されています。 タイユナイト表面の骨形成パターンは、機械加工表面のインプラントとは異なる ことが複数の研究で確認されています(Schüpbachら 2005、Zechnerら
2003)
*。
この差はタイユナイトの骨誘導性に由来しており、インプラント表面に速やかな 骨形成を促し、周囲の骨にしっかりと結合することができます。即時負荷コンセプト を用いる場合や、骨質が軟らかく、最適な治癒が得られない症例でのインプラント 治療においては、特に重要です。インプラント表面に直接新しい骨が形成される ため、機械加工表面のインプラントに比べ、治癒期間を通じて高いレベルで機械的 安定性を維持することができます(Glauserら 2001)**。このように、タイユナイト・
インプラントは、骨質が軟らかく、最適な治癒の獲得が困難な領域においても有効 であり、予知性の高い治療を行うことができます。 文献では、インプラントの即時負荷のためのさまざまな基準が報告されています。 治療を成功させるには、インプラントの初期固定が不可欠です。即時負荷を検討 する場合は、35Ncm以上の埋入トルクが必要であることに留意してください。
インプラントは、最低でも35Ncmの最終埋入トルクを達成する必要があります。 これは、外科用トルクレンチを使用して確認することができます。インプラントが 回転しなければ、インプラントの初期固定は即時負荷を行うには十分であると 判断できます。 タイユナイト・インプラント表面の骨芽 細胞(提供:Dr Peter Schüpbach、 スイス) 上顎臼歯部における即時負荷に よる術式では、タイユナイト表面の インプラントは機械加工表面の同一 デザインのインプラントと比較して、 より高い安定性が維持されます (Glauserら 2001)**。 重要な治癒期における高い安定性 共鳴振動周波数分析 インプラント埋入期間(ヶ月) は じ め に 上 顎 下 顎 即時 負 荷 臨床 ケ ー ス 参考文献 治療計画 無歯顎患者のための補綴修復コンセプト // 治療計画Rehabilitation concepts for edentulous patients // Immediate Function 17
Clinical guideline – Immediate
Function with TiUnite® implants.
Immediate Function means that patients leave the offi ce with a functional fi xed restoration in place directly after implant insertion.
Osseointegration is defi ned as a direct structural and functional connection between living bone and the surface of a load-carrying implant.* With the Immediate Function protocol, osseointegration has not yet taken place when abutment and provisional restoration are delivered to the patient. The majority of the scientifi c publications report on Nobel Biocare TiUnite implants that were performed with Immediate Function resulting in successful outcomes. The TiUnite implants maintain and increase the initial stability over time until the osseointegration takes place. Immediate Function with its potential loading is an alternative to later loading protocols for the experienced implant user. As with any implant surgical or restorative procedure, the treatment outcome is interdependent upon six variables: – Biocompatibility of materials
– Implant design – Implant surface – Surgical technique
– Prosthetic loading conditions – Individual patient local site conditions
Patient selection
– Compliant patient with good overall health and oral hy-giene.
– Good gingival/periodontal/periapical status of adjacent teeth.
– Favorable and stable occlusal relationship to avoid overload to newly placed implant during initial healing.
– No apical disorder/infl ammation at the area of the implant site.
– Suffi cient bone volume and density to allow placement of adequate numbers and diameters of implants to withstand potential loads.
– Suffi cient bone density to maintain stability throughout osseointegration phase.
– No pronounced bruxism.
– Indicated for all regions as long as selection criteria are met. For patients not meeting these criterias, an unloaded proto-col to achieve secondary stability is still appropriate. As with any procedure, it is the responsibility of the health-care provider to determine the benefi ts and risks of Immedi-ate Function compared with delayed loading for a given patient and implant site.
Clinical relevance
– Immediate Function means that patients leave the offi ce with a functional fi xed restoration.
– Immediate loading is an alternative to later loading protocols for the experienced implant user. – Careful patient selection is indicated.
* Brånemark P-I, Zarb G, Albrektsson T. Tissue-integrated prostheses: Osseointegration in clinical dentistry. Chicago: Quintessence Publishing Co., Inc. 1985.
R ef er en ce s C lin ic al ca se s Im m ed ia te F u n ct io n M an d ib le P la n n in g M ax illa In tro d u ct io n
Rehabilitation concepts for edentulous patients // Immediate Function 17
Clinical guideline – Immediate
Function with TiUnite® implants.
Immediate Function means that patients leave the offi ce with a functional fi xed restoration in place directly after implant insertion.
Osseointegration is defi ned as a direct structural and functional connection between living bone and the surface of a load-carrying implant.* With the Immediate Function protocol, osseointegration has not yet taken place when abutment and provisional restoration are delivered to the patient. The majority of the scientifi c publications report on Nobel Biocare TiUnite implants that were performed with Immediate Function resulting in successful outcomes. The TiUnite implants maintain and increase the initial stability over time until the osseointegration takes place. Immediate Function with its potential loading is an alternative to later loading protocols for the experienced implant user. As with any implant surgical or restorative procedure, the treatment outcome is interdependent upon six variables: – Biocompatibility of materials
– Implant design – Implant surface – Surgical technique
– Prosthetic loading conditions – Individual patient local site conditions
Patient selection
– Compliant patient with good overall health and oral hy-giene.
– Good gingival/periodontal/periapical status of adjacent teeth.
– Favorable and stable occlusal relationship to avoid overload to newly placed implant during initial healing.
– No apical disorder/infl ammation at the area of the implant site.
– Suffi cient bone volume and density to allow placement of adequate numbers and diameters of implants to withstand potential loads.
– Suffi cient bone density to maintain stability throughout osseointegration phase.
– No pronounced bruxism.
– Indicated for all regions as long as selection criteria are met. For patients not meeting these criterias, an unloaded proto-col to achieve secondary stability is still appropriate. As with any procedure, it is the responsibility of the health-care provider to determine the benefi ts and risks of Immedi-ate Function compared with delayed loading for a given patient and implant site.
Clinical relevance
– Immediate Function means that patients leave the offi ce with a functional fi xed restoration.
– Immediate loading is an alternative to later loading protocols for the experienced implant user. – Careful patient selection is indicated.
* Brånemark P-I, Zarb G, Albrektsson T. Tissue-integrated prostheses: Osseointegration in clinical dentistry. Chicago: Quintessence Publishing Co., Inc. 1985.
R ef er en ce s C lin ic al ca se s Im m ed ia te F u n ct io n M an d ib le P la n n in g M ax illa In tro d u ct io n
臨床ガイドライン
−タイユナイト表面インプラントによる即時負荷
即時負荷プロトコルとは、一度の診療でインプラントの埋入 手術を終え、プロビジョナルを装着して帰宅することを意味 します。 オッセオインテグレーションは、負荷を伴うインプラントの 表面と生体骨との構造的かつ機能的な直接結合を意味します。*
即時負荷プロトコルでは、アバットメントおよびプロビジョナル・ レストレーションの装着時点において、オッセオインテグ レーションは生じていません。タイユナイト表面インプラント を使用した即時負荷の術式は臨床的に実証されており、 成功症例については数多くの科学文献があります。タイユナイト 表面インプラントは、オッセオインテグレーションが始まる までの期間、初期固定の維持と向上に寄与します。インプラント 治療経験の豊富な歯科医師であれば、遅延負荷プロトコル の代替法として検討できます。 通常のインプラント外科や補綴修復治療と同様、以下の6つ の項目が治療結果に影響します。 −材料の生体適合性 −インプラントのデザイン −インプラントの表面性状 −外科的テクニック −補綴物への負荷の状態 −埋入部位の状態 適用条件 − 良好な全身の健康状態および口腔衛生状態。 − 良好な隣接歯の歯肉/歯周/歯根尖周囲の状態。 − 初期治癒期において新たに埋入したインプラントへの 過荷重を回避できる良好かつ安定した咬合関係。 − インプラント埋入部位における歯根部の病変/炎症が みられない。 − 予想される咬合負荷に対し十分な本数と径のインプラント を埋入するための十分な骨量および骨密度がある。 − オッセオインテグレーション期間において固定性を維持 するための十分な骨密度がある。 −ブラキシズムがない。 上記の適用条件を満たせばほとんどの部位に適用可能です。 その他の症例については、2回法遅延負荷を適用し、二次
固定獲得後に負荷のタイミングを設定します。 一般的な治療と同様、遅延負荷と比較した即時負荷のメリット とリスクについては、個々の患者およびインプラントの埋入 部位ごとに歯科医師の責任で判断します。 臨床上のポイント −即時負荷とは、一度の診療でインプラントの埋入手術 を終え、プロビジョナルを装着して帰宅することを意味 します。 −インプラント治療経験の豊富な歯科医師であれば、 遅延負荷プロトコルの代替治療法として即時負荷を 検討できます。 −適用条件を慎重に考慮する必要があります。 は じ め に 治療計画 上 顎 下 顎 臨床 ケ ー ス 参考文献 即時 負 荷 無歯顎患者のための補綴修復コンセプト // 即時負荷Rehabilitation concepts for edentulous patients // Immediate Function 18
Surgical guidelines
– Adapt implant site preparation technique to bone quality/ quantity or use a tapered implant body for high initial implant stability.
– Individual implants should be able to withstand a fi nal tightening torque of minimum 35 Ncm torque without further rotation to confi rm stability at time of implant placement.
– If resonance frequency measurement is performed at time of placement – ISQ values > 60 is recommended.
– Regardless of anatomic site or bone quality, implants typi-cally show a drop in the initial stability over the fi rst several weeks before osseointegration takes place. While the maintenance of initial stability is higher with TiUnite than a machined implant surface, this phenomenon can still be expected to occur. Consequently, it is not just the Immedi-ate Function itself but also other prosthetic manipulation of the implant during the healing phase that needs to be considered, e.g. unscrewing of provisional restoration and impression copings.
Restorative guidelines
– A restorative strategy should be developed to ensure minimal handling and tightening of prosthetic components and transference of forces to the implants during the fi rst weeks after placement.
– Special care is recommended when it comes to evaluating load distribution and the elimination of cantilevers and lateral forces. If possible, the occlusal contact should be reduced during the fi rst two to three months after implant placement.
– To obtain optimal esthetics, when practical, the placement of the fi nal abutment at time of implant placement can minimize further disruption of the soft tissue interface. – A well designed provisional restoration to be used during
the maturation of the soft tissue improves the esthetic end results.
– Cantilevers of all types should be avoided in Immediate Function protocol. In tr o d u ct io n M ax ill a P la n n in g M an d ib le Im m ed ia te F u n ct io n C lin ic al c as es R ef er en ce s 負荷プロトコルの定義 即時負荷 0時間 即時負荷 早期負荷 遅延負荷 48時間 (2日間) 1週間 6週間 12週間 (3ヶ月) 24週間 (6ヶ月) 早期負荷 遅延負荷 (1回法/2回法) 外科ガイドライン −インプラントの高い初期固定を得るためには、骨質
/
骨量 に合わせたインプラント埋入部位の形成を行う、または テーパード・インプラントを使用します。 −インプラント埋入時、最終埋入トルク35Ncm
以上で締め 付けてもそれ以上回転せず固定された状態である必要 があります。 −インプラント埋入時に共鳴周波数測定を実施する場合、ISQ
値が60
超であることが推奨されます。 −解剖学的部位や骨質に関わらず、インプラントは通常、 埋入後の数週間、オッセオインテグレーションが始まる 前に、初期固定の低下が見られます。ただ、タイユナイト 表面は機械加工表面以上に初期固定の維持をサポート します。したがって、この治癒期においては、即時負荷の 適用に限らずプロビジョナル・レストレーションや印象用 コーピングの取り外しなど、インプラント補綴修復の手順 においても注意が必要となります。 補綴修復ガイドライン −インプラント埋入後数週間において、補綴物への関与・ 着脱やインプラント体への負荷について、最小限に留める 必要があります。 −負荷配分の評価、またカンチレバーや側方力の排除の 検討は注意深く行ってください。 −可能であれば、インプラント埋入後2
∼3
ヶ月間は咬合接触 を軽減することが推奨されます。 −軟組織の接触面の吸収を最小限に抑えて審美性を得る ために、状況に応じて、インプラント埋入と同時に最終 アバットメントを装着することも検討できます。 −最終的な審美性を得るためには、軟組織の治癒期間に使用 するプロビジョナル・レストレーションを適切にデザイン する必要があります。 −即時負荷プロトコルでは、カンチレバーは禁忌です。 タイユナイト表面 インプラントによる 即時負荷 は じ め に 治療計画 上 顎 下 顎 臨床 ケ ー ス 参考文献 即時 負 荷 無歯顎患者のための補綴修復コンセプト // 即時負荷Rehabilitation concepts for edentulous patients // Immediate Function 19
Post-surgery and maintenance program The follow-up and maintenance is the same as for all implant-based treatments with special attention to the following:
– Antibiotics on the day of surgery and some days post-surgery may be indicated.
– Restrict diet to soft food fi rst weeks after implant placement.
– A soft toothbrush used with a chlorhexident gel twice a day for the fi rst few weeks.
– Follow-up visit at individual intervals with examination of the soft tissue, the construction, and the occlusal condi-tion as for all implant cases.
Clinical relevance
– Follow recommended guidelines for successful outcomes.
– Implant should be able to withstand a tightening torque of minimum 35 Ncm.
– It is recommended to wait for soft tissue maturation prior to proceeding with fi nal restoration.
R ef er en ce s C lin ic al ca se s Im m ed ia te F u n ct io n M an d ib le P la n n in g M ax illa In tro d u ct io n 術後フォローアップおよびメインテナンス 術後フォローアップおよびメインテンスは、他の外科的治療における場合と同じです。 次のことに注意してください。 −手術当日および術後数日間の抗生物質を処方します。 −インプラント埋入後数週間は、食事を軟らかい食べ物に制限します。 − インプラント埋入後数週間は1日に2回、クロルヘキシジンゲルを付けた軟らかい 歯ブラシを使用します。 − 症例に適した間隔でフォローアップ診療を実施し、軟組織、アバットメントの接合、 および咬合状態を評価します。 臨床におけるポイント −推奨されるガイドラインに従い治療を行ってください。 −インプラント埋入時に
35Ncm
以上の締め付けトルク を得る必要があります。 −最終補綴物は軟組織の治癒後に装着することを推奨 します。 は じ め に 治療計画 上 顎 下 顎 臨床 ケ ー ス 参考文献 即時 負 荷 無歯顎患者のための補綴修復コンセプト // 即時負荷Rehabilitation concepts for edentulous patients // Clinical cases 20 In tr o d u ct io n M ax ill a P la n n in g M an d ib le Im m ed ia te F u n ct io n C lin ic al c as es R ef er en ce s
Mild/moderate bone resorption.
Initial analysis shows the complete maxillary denture with the partial mandibular denture in occlusion. The decreased retention and insta-bility of the maxillary denture lead to its replacement.
Pre-op panoramic radiograph (OPG) shows the mild to moder-ate horizontal and vertical bone resorption patterns in maxilla resulting in the instability of the maxillary denture. The bilateral sinus pneumatization is also ob-served.
The intra-oral analysis shows the healthy condition of the soft tis-sues. The bone height and width were seen to be adequate for the planned treatment and optimal surgical and restorative outcome. Immediate loading for full-arch rehabilitation using NobelClinician
Patient: 65-year-old male, edentulous in the upper jaw. The dentures were made six years ago. Chief complaint: Patient was self-conscious of having a removable upper denture. He complained about the decreased retention and was often worried about the falling out of the denture. The patient’s re-quirement was to replace the removable upper denture with a fi xed restoration. Overall health: Healthy and non-smoker. Oral examination: Soft tissues within normal limits. Mild to moderate horizontal and vertical bone resorption patterns, with bilateral posterior sinus pneumatization.
Decision: The predecessor of the NobelClinician Software was used for treatment planning, followed by the use of a surgical template for a precise implant placement and a minimally invasive and fl apless surgical procedure. Five Brånemark System Mk III Groovy implants and one Nobel-Speedy Shorty implant were placed posteriorly on the left side. As fi nal restoration, a NobelProcera Implant Bridge Titanium with acrylic teeth was used. The fi nal restoration was prepared one day prior to surgery and inserted into the patient’s mouth at the time of implant placement. Time for total treatment: 3 months