NII-Electronic Library Service
mp7eszaee
eg
23Uas
8il 497--506R'
(1996
F)
Report
Therapeutic
Exercise
for
Children
with
Spastic
Spinal
Paraplegia"
Masamichi
FURUSAWA'",
Nobuhiro
HIURA,
Masahiro
TAKESHITA,
Yuki
NOMOTO,
andKanako
IZUMI
Abstract
'
The purpose of thisresearch
is
toascertain the characteristics thatdifferentiate
spastic spinal paraplegia(SSP)
from
spasticdiplegia
of cerebral palsy(CP
・SD),
an.dthe pointsthatshould be taken
into
considerationin
the treatment of SSP byphysi-cal therapists, We report on ways of physicaltherapistscan prevent,by therapeutic
exercise, abnormal development of SSP children. Eleven SSP children are analyzed
through clinical charts, and with video-films, photographs, and Bobath's postural
tone
test
incomparison with CP(SD)
children who had had lumbago and footpain,No
child withSSP
wasborn
at abirth
weight ofless
than 2,500g,unlike the typicalscenario
for
CP
(SD)
children(p<O,Ol),
Allchildren acquired the ability towalk at2.6±
1.4
years on average(ranging
from
1
year to5
years1
month).Eight
achievedindependent without
braces,
one with shortleg
braces,
two with Lofstrand crut6heSand short leg
braces.
SSP children were clearly superior todiplegic
children interms
of normal extensor patternsof thelower extremities and selective movementsof individual
joints.
Lumbago was presentin
5(45.4%)
at 7.8±1.3years and footpain was presentin4
(36.3%)
at 8.5±2.6years of our 11 cases. Posturaltone of thelower trunk tended to be low inSSP. Inorder to obtain walking and prevent
lum-bago,
physicaltherapists
should make effortsto
promote sustained coactivation ofthe
lower
trunk musculature early inthecourse of treatment,Key
wordsChildren
with spastic spinal paraplegia,Spastic
diplegia,
Therapeutic
exerclse
Introduction
Spastic
spinal paraplegia(SSP)
is
paralysisdue todegenerationinthe spinal cord mainly
'
,JivaffM,trpm,msWzzfiAdiffbltwix 'S Bebath Memorial HospiLal
(1-6-5Higashinakahama,
Joto-ku,Osaka536, Japan)
(ReceivedJune21,19941AcceptedAugust31, 1996}
with
bilateral
involvement
to thecor-ticospinal tractsi).
It
has
recentlybeen
reported thatspastic spinal paraplegia
in
pe-diatric
patientsis
not necessarilylimited
to the spinal cord but possibly includesdegenerativechanges inhigher centers of the
NII-Electronic Library Service
498
wa7diza\
diseasesisimportant
because
of thedifferent
clinical picture that ultimately emerges.
Most children with SSP who received
thera-peuticexercise at eur
hospital
wereoriginal-lydiagnosed elsewhere as having spastic
di-plegia of cerebral palsy
(CP・SD).
Physical
therapists should
differentiate
SSP
from
other conditions and proceed with treatment after having obtained a 'thorough knowledge of thc characteristics of abnormal
develop-ment inSSP. Inthisstudy, we ascertain the characteristics thatdifferentiate
SSP
from
CP
(SD),
and the pointsthatshould be takeninto
consideration in the treatment of SSP by physical therapists,
Subjects
andMethods
The
subjects were eleven children withSSP,
who received therapeutic exercise atBobath Mernorial Hospital between August
1982
andJuly
1993
(Fig.
1). Priortoreceiv-ing treatment at our hospital,cight children
(72,7%)
had originally been diagnosed ashaving
had
CP
(SD>,
one(9.0%)
as havingSSP, and thecondition
had
been
evaluated as unknownin
two(18.2%).
Thus, the rnajorityof these children
had
been
treatedby
physi-cal therapistsunder thediagnosis of CP
(SD),
They were seven boys and four girls.None
had
Segawa
disease(hereditary
progressivedystonia)6}or
juvenile
Parkinsonism7),
both
ofwhich can produce symptorns similar to
those of
SSP.
Neurogenic
bladder8)
was notobserved inany of these ehildren. The mean age at
initial
examination was 6.8±2.3years(ranging
'from 2 to13
years).Five
childrenwere treatcdon beth an inpatientand an
out-patient basis,and 6 werc treated by
thera-peuticexercise only on an outpaticnt basis.
Diagnosis
prior to treatment at ourhospi-ee
23igag
8e
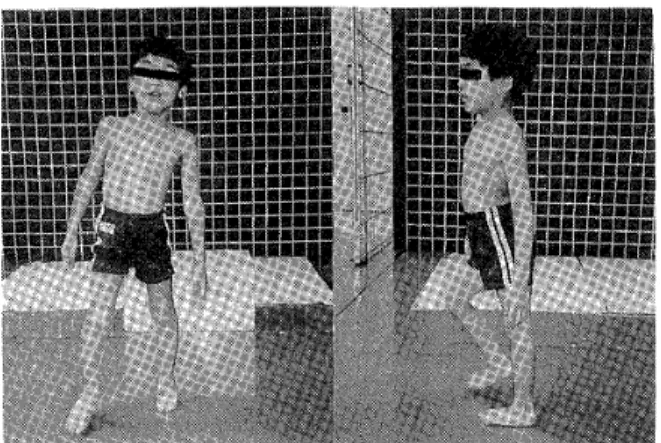
Fig.1. Pattern of walking inchildren with spastic
spinaE paraplegia. Lordosisisremarkable
and compensatory sideflexion of trunk is observed when he shifts hisweight toone
leg.
tal,
birth
history,family history,locomotordevelopment, presence or absence and the
oc-casion of
lumbago
and foot pain, and anyprevious surgical opcrations were ascertaincd
from
medical charts.Standing
posture and walking patterns were assessed fromvideo-films
(VTR)
and photographs inorder to findout abnormal patterns caused by spasticity
in
legsand compensatory movements espe-cially in trunks, Posturaltone was assessedwith the postural tone test advocated
by
Bobath9). Points that should be taken into
consideration
in
treating
pediatric patientswith SSP by our approachiO} were in-vestigated by comparing our data on SSP children with the report of CP
(SD}
childrenby
Suzukiii),
many clinicalfeatures
of which resemble those ofSSP.
We checked on thedifferentiationof both groups in the birth
weights and the gestationalages. Lumbago and foot pain of SSP were compared with
those of
CP
<SD)
in scanning the clinicalrecords. They were also tested to have speech disturbanceor not,
NII-Electronic Library Service
TherapeuticExerciseforChildrenwith SpasticSpinal Paraplegia 499
Results
Eight children had blood relatives who
either had
definitive
SSP
or were suspegtedof having
SSP.
SSP
was a known entity intwo pairs of twins
(four
children), twofathers,a mother, and an eider sister.
One
uncle was suspected of
having
SSP.
Among
the eight children who had
blood
relatives withSSP,
sixhad
been
diagno$ed
ashaving
CP
(SD)
and one as havingSSP,
and thecon-dition had been evaluated as unknown in
one.
Of
the three children whohad
noknown
blood
relatives withSSP,
two were referred to our hospitalunder the diagnosis ofCP
(SD)
and one remained undiagnosed.Cephalic presentation was common to the
birthof all the children, The values of
jaun-dicewere within normal range. Four of the
childrcn weighed 2,500-3,OOOg at birth,and
the other seven 3,OOO-3,500g, so none of
them had abnormally low birthweight.
As-phyxia was present
in
3
children(27.2%),
who were maintained in incubators fer lessthan 7 days after birth,and their subsequent conditions was favorable.
Gestation
had
been
36
weeksfor
two children, 38 weeks for one, 39 weeksfor
four,and 40 weeks forfour.
The threechildren with asphyxiahad
been
born
at gestations of 39 weeks and 40 weeks. Three children had speech disturb-ance. A pairof 8 year old twin boys and a6,5
year old girl haddysarthria.
Locomotordevelopment
is
shownin
Fig,
2,
Thechil-dren could roll over at 7,l±2.4 months on
the average
(ranging
from 4 to 12 months).Sitting was achieved at 7.7±2.6 months
(ranging
from 5 to 13 months), although theage was uncertain in one child.
Crawling
was achieved at11.8
±4.8
months(ranging
WALKINGWITHOUTBRACES
WALKING WITH SHORT L.EG BRACES WALKINGWITHLOFSTRAND CRUTCHESANDSHORTLEa BRACESWALKINGWITHWALKER CRUTSINGLOCOMOTIONASSESSMENT F --o " :--o H --o 1 H , M , '111'''/11''1T''b' IN:TtAL ASSESSMENTF]NALASSESSMENT
Fig.2. Change of locomotion.
from 6 to 16 months), but with the ages un-certain
in
two children.The
children could cruise along the furniture at18.8
±11.1
month
(ranging
from
9
months to2.6
years),All
children acquired the ability to walk,As
shown in Flg. 2, nine ambulatedinde-pendently, but two needed Lofstrand
crutches. They
became
able towalk at 2,6±1.4
years(ranging
from
1 year to 5 years 1month).
Six
of the children underwent surgicalproceduresi2)i3). The Baker operation to
lengthen the gastrocnemius was performed
bilaterally
infivechildren, and the surface of adductorlongus
was released bilaterallytoalleviate flexionand adduction contracture of
the hip
joints
in one child.Medial
ham-strings were clongated
bilaterally
in
onechild to increase the ability to extend the
knees. The flexor hallucis longus was
released bilaterallyinone child fortreatment
of hammer toes.
Pain was noted
in
seven(63.6%)
of the children withSSP.
Five(45.4%)
hadlumba-ge at 7.8±
1.3
years(ranging
from 6years toNII-Electronic Library Service
500
Table
ve\wtzaeig
ee23igees・g-l Comparisonof birthweight betweenSSP and CP
{SD)
Birthweight
(g)
1,ooe-1,soe 1,500-2,OOO 2,OOON2,500 2,500--・3,OOO 3,OOO<
SSP
(N-11)
CP
(SD)
(N-9)'o3 o2 o2 4o 72
'Suzuki 19goll).
8.5±2.6 years
(ranging
from
5 years to12
years), In scanning our clinical records of
thirteen children with cerebral palsy, we
found
that eightdiplegic
children and onediplegic
adulthad
suffered Iumbago at 12.9±5,6years
(ranging
from 5 years 2 months to22 years),and fivediplegicchildren had had
foot pain at 9.4±3,1 years
(ranging
from 5years 9 rnonths to
l3
years).All
of three children with CP(SD)
could walk independ-ently without crutches,
When
spasticity of thelower
extremities was reduced by thetherapisVshandling,chil-dren with SSP were betterable than children
with
CP
(SD)
to maintain the lowerex-tremitiesextended against gravity,which is
necessary for standing and walking. The chi!dren with
SSP
alsodernonstrated
greaterability for selective movement at the hips,
knees,and ankles, especially inmovement
in-volving fiexion and extension of the knee and
dorsifiexion
of the ankle.In
contrast, the children withSSP
had
diMculty with coactivation in thc lower trunk, particularlywith sustaining contraction of the abdominal
muscles
during
extension of the trunk against gravity.Our
clinical observations, gait analysis using VTR and photographs, and posturaltone testing have confirmed that postural
tone of the lower trunk inchildren with SSP
islower than that inchildren with CP
(SD),
and that SSP isassociated with a
tendency
(P<O.Ol)
for
markedlumbar
lordosis.
Discussion
1.
Knowledge
ofSSP
in
terms of physical therapySome recent studies using
diagnostic
im-aging, such as computed tomography and magnetic resonance imaging, as well as
cere-brospinal
fluid
testing, haveShown
that thedegeneration
QfSSP
isnot necessarily limit-ed tothe spinal cordbut
can also includethebrain2-5).
Two brothers,10 and 8 years old,did indeed exhibit slight
intellectual
handi-caps. However, they were independent in
ac-tivitiesof dailylivingand theycould socially
interactwith other persons.
Eight
(72.5%)
of the11
children withSSP
had
been
treated by therapeutic exerciseunder thediagnosisof CP
(SD)
priortobeing
brought to our hospital,in day-care centers
for
disabled
preschool children. Birthweightwas investigated
in
comparison with thereport by Suzukiii}
(Table
1). Arnong the nine children observed and fellowedby
Suzuki
in
a neenatalintensive
care unit andfinallydiagnosed as having CP
(SD),
seven(77,7%)
were born at birth weights below2,OOO
g, and the remaining two(22,3%)
weighed 3,OOOg or more. AIIof the childrenwith SSP, howeyer, weighed 2,500g or more
at birth,so none werc low birth weight
in-fants. This differencein distribution
be-tween
theCP
(SD)
andSSP
children wasNII-Electronic Library Service
TherapeuticExerciseforChildrenwith SpasticSpinalParaplegia
Table 2 Comparisen ofgestationalages betweenSSP and CP
CSD)
501
Gestationalage
(weeks)
2728293031323334353637383940
SSP
(N-
11)CP
(SD)
(N
==9)*o1o1o1o1o1ooo1ooeo2ooo1o4!42"Suzuki 19goil),
nificant
(p<O,Ol)
according to theMann-Whltney
U
test.The
CP
CSD)
children andSSP
children were compared according to gestational age(Table
2). NineSSP
children(8i.8%)
wereborn
at gestationalages of38
weeks or more,According to the report by Suzuki,
however,
only three children
(33.3%)
with CP(SD)
wereborn
at38
we6ks or rnore,This
differ-encebetween
thediagnostic
grouPs was sig-nificant<p<O.05)
according to the U test.Bobath
andBlecki4)
have
alsodescribed
many children with CP(SD)
as having beenpremature babies. Hagberg et al.i5) reported
that 88
(45.5%)
of 207 children withCP
(SD)
were born at fullterm,
From
the viewpoint of motordevelopment,
rolling over and sitting were achieved verylateonly in the twin boys with SSP, The
period of achievement of
these
behaviors
wasnormal or only slightly
delayed
in
the other children. Six(60%)
of the 10 children achieved cruisingby
one year of age, exceptpossibly
for
one child whosedata
wereun-known. The other four acquired cruising at
1
year3
months to3
years2
months.These
findings suggest the occult presentation of
SSP insome children.
In
Japan,
differentiatingSSP from CP(SD)
isdifiicultbecause of the small number of
day-care centers for preschool handicapped
children that
have
full-time
specialistdoctors.
It
is
thereforeimportant,
in
differentiating
(p< O.05)
SSP
fromCP
(SD),
for
physical therapiststoinvestigate gestational age at birth, birth
weight,
birth
history,
presence or absence qfSSP
in
blood
relatives, course of motordevel-opment, and presence or absence Qf
dysarthria.
Pediatric
patients' responses to stimulationduring
therapeutic exercise should also be observed carefully.・ SSP is characterizedby
deficiency
of sustainedcon-traction of the abdominal muscles during
antigravitational extension of
the
trunk
andby
more selective movementin
thelower
ex-tremitiesthan typicallyfound in spastic
di-plegia SSP should
be
suspected after acom-prehensive assessment of all of the
informa-tion described above, and physicians should
be
requested to make adifferential
diagnosis,
attempting torule outCP
(SD}.
Besides the differentiationof SSP from CP
(SD),
itisalsoimportant
in
planningtreat-ment to
differentiate
these disordersfrom
human T-lymphotropic virus-type associated
myelopathy
(HAM),
as reportedby
Shimazaki
et al,i6)When
a physical therapistsuspectsthatthe condition of a child may not
be
cere-bral
palsy with spasticdiplegia,
the therapist should clearly describethe various responses obtained through therapeutic exercise and speculate Qn the reasons forthose responses.2. Essentialpoints on therapeuticexercise
The
distribution
of spasticityin
the lowerextremities of children with SSP and
their
NII-Electronic Library Service
so2 wreetw2kee
abnormal walking patternsresembled the
ab-normal developmenti7) inCP
(SD).
Eight ofthe 11 SSP children had been treated by
therapeutic exercise under a diagnosis of CP
<SD)
before
being
brought
toourhospital,
Bealsi8}reported that 52.6% of children
with
CP
(SD)
achieved independentambula-tion and 20.4%
became
able to walk withcrutches. Kajiurai9)similarly reported that
50% of children with CP
(SD)
became able towalk
independently
while another 25%became ambulatory with crutchcs. From
these reports, the rate of acquiring theability
to walk inchildren with CP
(SD)
can becon-sidered
to
be
about 75%. In contrast, all ofthe children with SSP acquired the ability to
walk, although 2
(18.1%)
were limited to crutch arnbulation. None of the patientswith
SSP
showed severe spasticity20), enoughto prevent movement, although moderate
spasticity was present
in
thelower
ex-tremitiesof all
SSP
children.According
toBealsi8)and Okawa et al.i3>, some children
with
CP
require iliopsoasrelease because themuscle
is
shorteneddue
to severe spasticity.None of the presentchildren with SSP
under-went
this
operation.It
is particularlydiMcult,
in
treatingSSP,
to obtain sustainedcoactivation of
the
abdominal and glutealmuscles, necessary for extending the pelvis and trunk against gravity during standing and walking. The diMculty in sustaining contraction of the abdominal muscles
in
an attempt to extend the trunkin
therapeutic exercise was confirmed by comments oftherapistsin our group. Physical therapists
should promote continuous contraction of
the child's lower trunk, particularlythe
ab-dominal muscles, when attempting to elicit
antigravitational extension of the trunk
ee
23gee
8e
during the walking portionof treatment.
The appearance of lumbar and footpain in seven
(63.6%)
of theSSP
children, rangingin
age from fiveyears to twelve years of age, canbe
considered unusually frequent. These children could walkfast
or even run, Ac-cording to the Welch test,SSP children suffered lumbago significantly earlier thanthe nine diplegicchildren
(p<O,05),
but footpain showed no such significant difference
between
the two groups.The
results of the analysis suggest thatpain,especiallylumba-go, tends toappear inpediatric patientswith
SSP
earlier than inthose withCP
(SD),
Lumbar lordosiswas particularly
remarka-bleinnine clients
(Fig.
1).Posturaltonetest-ing revealed slight to moderate spasticity in
flexorsand adductors of the hip
joints.
Thespasticity of these muscles was particularly marked in the outer range of hip
joints.
Spasticity
ofthe
hip
flexors
and adductorsinterferes
with antigravitational posteriortiltof the pclvisand extension of the lower
ex-tremities. Since righting activities from the
pelvisand lower trunk appear lateas a
re-sponse,
however,
unilateralloading
of body weight onto a lower extremity andthe
pro-pulsion necessaryfor
walking are promotedby hyperextension and lateralflexionof the
lumbar spine by excessively using the back
muscles, Allfivepatientswho complained of
lumbago showed lumbar lordosisinstanding
as well as
during
walking. The lumbago might havedeveloped
as a result ofrepeti-tion of compensatory movements.
Treatment of lumbago
is
incorporated
intosystematic therapeuticexercise.
Contraction
of the abdominal muscles issustained during extension of the trunk and lumbar lordosisismo-NII-Electronic Library Service
Therapeutic Exercise forChildren with Spastic SpinalParaplegia
Fig.3. Promotion of sustained coactivation in
trunk musculatures.
bility
improves
in
painful lumbar extensors.Whcn occasien demands, soft tissue
mobiliza-tion istransiently performcd in the lurnbar
region2i) to reduce pain prior to continuing
therapeutic exercise.
As
a result,lumbago
may disappear after thisapproach. To
im-prove gait and prevent
lumbago
in
SSP,
physical therapists should reduce the spasticity of flexorsand adductors of the hipjoints,
promote sustained contraction of theabdominal muscles
during
coactivation of thelewer trunk, starting in infancy,particularly
during
extension of the trunk,and must con-sciously pursuc preventjon of lumbarlordo-sis.
With regard tofootpain, evaluation of
pos-turaltone revealed spasticity with a slight to
moderate degree of resistance9) inthe tibialis
anterior, the tibialis posterior and
gastrocnemius muscles, Postural tone testing revealed moderate spasticity in the
plantarflexors.Intrinsicmusclcs of the foot,
however, exhibited low tone. The
arrange-ment of the longitudinalarch of the
foot
wasdisrupted
and pes pianovalgas was observed.503
These findingswere considered to be
respon-sible forpain resulting
from
loading
ofbody
weight onto the
feet,
particularly the soles.Before wcight loading onto the lower
ex-tremities,the
hypersensitivity
offeet
wasdesensitized
and thedifferenceindistributionof postural tone of the lower cxtrernities and
feet
was cqualized while selective movementsof the lower extremities were performed in
supine or sitting during treatment
(right
andleftparts of Fig.4)22}.Loading
in
thestand-ing
position was then gradually increased(right
and leftparts of Fig.5),
The footpaindisappeared
with stepwise progression of thisFig.4.Desensitization of hypersensitivity insoles and tricepssuraes toweight on hee]s.
Fig.5.Treatrnent in walking. In order to
de-crease lordosisand toprevent compensato-ry sidefiexion of his trunk, contraction of abdominal muscles issustained jn
stand-ing and walking.
NII-Electronic Library Service
5o4
fft';'tasZkr'"
program.
A pair of
8
year-old twin boys and one 6.5year-old girlunderwent speech therapy
be-cause all three had
dithculty
with speechdue
to
dysarthria,
They
were suggested supraspinal involvement, but theirintellectu-al abilitieswere normal. Takahashi et at.3>5) reported autosomal recessively inheritedSSP
with dysarthria. Physical therapistsshould
help
theSSP
childto
sustain a syrnmetrical neutral position of thehead
and neckduring
walking, inconjunction with speech therapy.
The
pelvisin
such a childis
insuMciently
mobile because of spasticity in the muscles surrounding the hip
joint.
During walking,the center of gravity moves
in
a compensato-ry manner, withlateral
fiexion
and anteriorflexionof the trunk,head and neck, and with
horizontal
instability
of thejaw
(Fig.
1).
As
a result, fine independent skillful movementsof the lower
jaw,
tongue, and lips,necessaryfor
articulation,do
not develop adequately,exacerbating the
diMculty
with speech devel-opment. Physical therapistscarry outtreat-ment
by
reducing the spasticity of thehip
flexorsand adductors and eliciting sustained
coactlvation of the abdominal muscles and
glutealmuscles with the aim of helping the
child rnaintain the head and neck in neutral
position without compensatory movements
during
walking.With
these ways physicaltherapistsmust thus cooperate with speech
therapists in planning and administering
treatment.
Conclusion
Eleven pediatric patients with SSP were studied. The points to which physical
therapists should pay attention in
ministering therapeutic exercise for
acquisi-eg
23tseg
8-ijtion of the ability to walk were also
described. Physicaltherapists can contribute
to the preventien of abnormal
development,
Iumbago, and foot pain in SSP by applying
therapeutic exercise
based
on an adequateknowledge of the characteristjcs and
differ-ences in the individual clinical features of
SSP and CP
(SD).
References
D Hirayama Ki Shinkeishokegaku
<Neurological
Semielogy). Bunkodo, Tokyo, 1984,pp375
{In
Japanese>.
2)Mukai E,et al.: Clinicalstuciy of familial
tic paraplegia. Rinsho Shinkeigaku (Clinical
Neurology)27
(1}:
1399-14・09,1987(In
nese).3)Takahashi A, Mukai E: Familial spastic
plegia. ShinkeiKenkyu no Shinpo
(Advances
inNeurologicaiSciences)31{6}:
954-956, 1987(In
Japanese).4)JoshitaY: Familial spastic paraplegia: Report
of fourteencases and comparison with cases in the Iiterature. Shinkei Naika
(Neurological
Medicine) 28
(2):
190-197, 1988(In
Japanese). 5)Takahashi A,Mukai E: Familial spasticplegia. Spineand SpinalParaplegia2
C2):
134,1989
(In
Japanese).6)Segawa M: HerediLary progressive dystonia
with marked diurnal fluctuation.Shinkei
Kenkyu no Shinpo
(Advances
in NeurologicalSciences)25
"):
73・-81,1981(In
Japanese) 7)Yokochi M: Clinicalcharacteristics ofjuvenile
Parkinsonism and possible participation ofhypothalamic mechanism to Parkinsonism.
Shinkei Kenkyu no Shinpo
(Advances
in rological Sciences)25{D:
82-94,1981(In
nese),8>Yamashita H, Kurnasawa JiNeurogenic
derdue toHAM. Journalof the
Japan
Medical Society of Paraplegia 3{1}:
124-125. 1990(In
Japanese). ・
9)Suzuki T: Diagnosis on Motor Development:
Bobath Approach. Ini Suzuki K, Akiyama T (eds)Noseimahi Kenkyu
<Research
of Cerebral Palsy). Vol. ll, Kyodo I$ho Shuppansha, Tokyo, 1979,pp 147-158(In
Japanese).10)Bobath K: A NeurophysioiogicalBasisforthe
Treatment of Cerebral Palsy. Clinics in Developmental Medicine,No. 75, WMiam
NII-Electronic Library Service
Therapeutic Exercise
HeinernannMedicalBooks Ltd.London,1980,,
pp 77-87.
11)Suzuki T: Treatment forCerebralPalsied
fantsat NICU. In: Tezuka K
(ed)
Noseimahi
(Cerebral
Palsy). No. 10, Kyodo IshoShuppansha,Tokyo, 1990,pp 1-21
(In
nese),
12)KiiK,Okawa A: Physical therapy, surgery and
orthopedics incerebral palsyiCo-operation
tween NDT
Lherapists
and orthopedic surgeonsin treatment of cerebral paisied children.
Rigakuryoho
janaru
{The
Japanese
J
ofcal Therapy) 23
{7):
471-476, 1989(In
nese}.
13)Okawa A,et al.: Physical therapeutic and gicalrnanagement inspastic diplegia.Clinical
Orthopaedicsand Related Research 253: 44,1990.
14)BleckEE: SpasticDiplegia:Orthopaedic
agement in Cerebral Palsy, In:Bleck EE (ed) ClinicsinDevelopmental Medicine. No. 99, William Heinemann Medical Books Ltd. London, 1987,p 282.
15)Hagberg B,Hagberg G:Prenataland Perinatal
Risk Factorsin a Survey of 681 Swedish
Cases.IntStanley F,A]berman E
(eds)
Clinicsin DevelopmentalMedicine. VoL 87,William Heinemann MedicalBooks Ltd.,London,1984, pp 116-134.
forChildren with SpasticSpinalParaplegia 505
16) ShimaZaki K, et al.: A ehild of HTLV-I
associated myeiopathy found by serological
screening testforchildren with spastic
plegia. Journalof the JapanPediatricSociety 95
(5):
1213-1217,1991(InJapanese).
17>Bobath B,Bobath K: Motor Development in
the Differenttypes of Cerebral Palsy. William
Heinemann Medical Books, London, 1978, pp
21-42.
18) Beals RK: Spasticparaplegia and diplegia.
Journalof Bone and JointSurgery 48--A
(5):
827--846,1966.
19> Kajiura I;Metor Development on Cerebral
sied Children, In:Tsuyama N (ed)Noseimahi Kenkyu (Researchof CerebralPalsy),Vol, I,
Kyodo IshoShuppansha,Tokyo, 1977,pp
150
{In
Japanese).20) Kii K: Bobath Approach. In: Hosoda K,
Yanagisawa K
{eds)
Rigakuryoho Handbook <PhysicalTherapy Handbook). Kyodo Isho Shuppansha,Tokyo, 1992,pp 352-408(In
anese),
21)Tsujii Y/ Manual therapy: Myofascial friction and stretch technique. Rigaku ryohogaku
<Journal
of theJapanesePhysicalTherapysociation) 16
(3):
177-182, 1989(In
Japanese).22)Lynch M, GrisogonoV: Strokesand Head
juries.
John
Murray,London, 1991,pp125.
NII-Electronic Library Service 506 理学療法学 第 23巻第 8 号 〈要 旨〉 小 児 脊 髄 性 痙 性 対 麻 痺へ の運 動 療 法 古 澤 正 道,月浦 伸 祐,竹 下 正 弘,野 本 由 紀,泉 佳 奈 子 ボバ ース記 念病院 本研究の目的は小 児の 脊 髄 性 痙性対 麻 痺 (
![Fig. 4.Desensitization of hypersensitivity in soles and triceps suraes to weight on hee]s.](https://thumb-ap.123doks.com/thumbv2/123deta/9870119.984833/7.892.174.378.135.440/fig-desensitization-hypersensitivity-soles-triceps-suraes-weight-hee.webp)
