Disclaimer: The manuscript and its contents are confidential, intended for journal review purposes
only, and not to be further disclosed.
Vascular Injury Is a Major Cause of Lung Injury after Balloon Pulmonary Angioplasty
1
in Patients with Chronic Thromboembolic Pulmonary Hypertension
2
3
First author’s surname: Ejiri
4
Short title: Vascular injury causes lung injury after BPA
5
6
Authors: Kentaro Ejiri, MD1, 2; Aiko Ogawa, MD, PhD3; Shinya Fujii, MD1; Hiroshi Ito, MD,
7
PhD2; Hiromi Matsubara, MD, PhD1, 3
8
1Department of Cardiology and 3Department of Clinical Science, National Hospital
9
Organization Okayama Medical Center, Okayama, Japan
10
2Department of Cardiovascular Medicine, Okayama University, Okayama, Japan
11
12
Address for correspondence:
13
Hiromi Matsubara, MD, PhD, Department of Cardiology and Department of Clinical Science,
14
National Hospital Organization Okayama Medical Center, 1711-1 Tamasu, Kita-ku, Okayama
15
701-1192, Japan
16
Tel: +81-86-294-9911, Fax: +81-86-294-9255, E-mail: [email protected]
17
Total word count: 5,993 words
18 19
Disclaimer: The manuscript and its contents are confidential, intended for journal review purposes
only, and not to be further disclosed.
1
Abstract
1
Background: Balloon pulmonary angioplasty (BPA) has become an alternative treatment for
2
inoperable patients with chronic thromboembolic pulmonary hypertension (CTEPH). Lung
3
injury (LI) is a major complication of BPA and may attenuate the benefits of BPA. Therefore,
4
we conducted a retrospective study to evaluate the association between patient and procedural
5
characteristics and LI in patients with CTEPH.
6
Methods and Results: We reviewed 76 patients with CTEPH who underwent BPA and
7
multi-detector computed tomography (MDCT) scanning pre- and post- BPA procedures. We
8
performed BPA on 1247 vessels during 297 BPA procedures and reviewed 594 MDCT scans.
9
By comparing pre- and post-BPA MDCT images, we diagnosed LI as follows: newly
10
appeared ground-glass opacity, consolidation, and pleural effusion. LI was detected using
11
MDCT scans during 138 procedures (47%), and mechanical ventilation was required during
12
40 procedures (13%). Angiographic findings of extravasation with or without simultaneous
13
clinical symptoms (BPA-related vascular injury) occurred during 50 procedures (17%). In
14
mixed-effect logistic regression models, BPA-related vascular injury was an independent
15
predictor of LI after BPA, odds ratio (OR) 20.1 (6.43-63.1). High mean pulmonary artery
16
pressure before BPA procedure and BPA-related vascular injury were independent predictors
17
of mechanical ventilation after BPA, OR 1.13 (1.03-1.24) and 10.8 (3.77-30.9), respectively.
18
Conclusions: Vascular injury during BPA could be a triggering factor of LI after BPA, and its
19
severity could be exacerbated by a high pulmonary artery pressure.
20
Disclaimer: The manuscript and its contents are confidential, intended for journal review purposes
only, and not to be further disclosed.
2
Abbreviations and Acronyms
1
BPA = balloon pulmonary angioplasty
2
CTEPH = chronic thromboembolic pulmonary hypertension
3
PEA = pulmonary endarterectomy
4
PAP = pulmonary artery pressure
5
CT = computed tomography
6
MDCT = multi-detector computed tomography
7
WHO = World Health Organization
8
LI = lung injury
9
BRVI = balloon pulmonary angioplasty-related vascular injury
10
OR = odds ratio
11
CI = confidence interval
12
SD = standard deviation
13
Disclaimer: The manuscript and its contents are confidential, intended for journal review purposes
only, and not to be further disclosed.
3
Introduction
1
Chronic thromboembolic pulmonary hypertension (CTEPH) is caused by stenoses or
2
obstructions of the pulmonary arteries due to organized thrombi.1-3 The prognosis of patients
3
with CTEPH is poor, because pulmonary hypertension-specific drugs are not sufficient to
4
improve hemodynamics and disease outcomes.3, 4 Pulmonary endarterectomy (PEA) is the
5
definitive surgical therapy for CTEPH;2, 5 however, not all patients can undergo PEA due to
6
surgical inaccessibility of the lesions, old age, and high comorbidities.6
7
Balloon pulmonary angioplasty (BPA) is an alternative treatment for inoperable
8
CTEPH, which uses a balloon catheter to dilate the pulmonary stenosis. In 2001, the results
9
of BPA in 18 cases of inoperable CTEPH were reported;7 however, the procedure was not
10
widely adopted because of the high incidence of lung injury (LI) as a complication. We
11
started to refine the BPA procedure to overcome the low efficacy and high complication rate
12
of BPA; BPA is now accepted for inoperable patients with CTEPH.8-10
13
However, the refined BPA procedure has not fully overcome the onset of clinically
14
serious complications. It is important to know the risk factors of LI to improve the safety of
15
the BPA procedure. Previous studies reported that hemodynamic parameters, such as high
16
pulmonary artery pressure (PAP) and low cardiac output, might be related to complications
17
and adverse outcomes,9, 11 but the other risk factors remain unknown due to a limited study
18
population. In addition, the varying definitions of LI among studies are another problem in
19
Disclaimer: The manuscript and its contents are confidential, intended for journal review purposes
only, and not to be further disclosed.
4
identifying the risk factors. Therefore, this study sought to determine the incidence and cause
1
of LI using high-resolution multi-detector CT (MDCT) scanning performed before and after
2
BPA. Furthermore, we aimed to identify the factors that trigger and/or exacerbate LI after
3
BPA.
4
5
Methods
6
The data, analytic methods, and study materials will not be made available to other
7
researchers for purposes of reproducing the results or replicating the procedure.
8
Patient selection
9
This is a single-center, retrospective observational study. The study population consisted of
10
consecutive patients with CTEPH undergoing BPA procedures at the National Hospital
11
Organization Okayama Medical Center between November 2012 and December 2013. A
12
diagnosis of CTEPH was based on detailed medical history, physical examination, chest
13
radiography, MDCT scan, transthoracic echocardiography, lung ventilation-perfusion
14
scintigraphy, and right heart catheterization. All patients underwent pulmonary angiography,
15
and had at least one of the following features: ring-like stenosis lesion, web lesion, subtotal
16
lesion, total occlusion lesion or tortuous lesion.12 All patients were diagnosed as inoperable
17
by experienced surgeons because of the location and surgical accessibility of the thrombi,
18
age, and comorbidities and, they were treated with warfarin and more than one pulmonary
19
Disclaimer: The manuscript and its contents are confidential, intended for journal review purposes
only, and not to be further disclosed.
5
hypertension-targeted drug.
1
The inclusion criteria of this study was that the CTEPH patients received the initial
2
BPA procedure during the study period. All patients were checked for other causes of
3
pulmonary hypertension, including congenital heart disease and lung disease. None of the
4
patients had any other diseases that caused hypoxemia or pulmonary hypertension. Patients
5
who were treated with mechanical ventilation before BPA and who did not undergo MDCT
6
scanning during the periprocedural period (before or within 24 hours after BPA) were
7
excluded. This study was conducted according to the principles expressed in the Declaration
8
of Helsinki and was approved by the Institutional Review Board, and written informed
9
consent was obtained from each patient before the procedure.
10
BPA procedures and perioperative management
11
BPA procedures and perioperative management were based on a previous report;8 however,
12
there were some modifications in this study. Preoperative application of epoprostenol was not
13
effective in the previous study;8 therefore, we did not administer it generally. However, in
14
two patients who were already receiving continuous infusion of epoprostenol, we did not
15
interrupt it before BPA. We used a 0.014-inch wire (Agosal XS; Asahi Intecc CO., LTD.,
16
Tokyo, Japan or Chevalier 14 floppy; FMD CO., LTD., Saitama, Japan) to cross the targeted
17
lesion. We determined the appropriate balloon size according to the proximal vessel diameter
18
measured using pulmonary angiography. The maximal balloon size depended on the vessel
19
Disclaimer: The manuscript and its contents are confidential, intended for journal review purposes
only, and not to be further disclosed.
6
diameter and lesion types. Respiratory care after BPA was performed according to the
1
patient’s condition. We performed the MDCT scans in the periprocedural period —the pre-
2
BPA and post-BPA MDCT scans were taken upon hospital admission for the BPA procedure
3
and within 24 hours after the procedure.
4
Study design and definition of lung injury
5
For the assessment of LI after the BPA procedure, we reviewed MDCT scans before and after
6
the BPA procedure. LI was defined as new abnormalities found in the post-BPA MDCT scans
7
as follows: ground-glass opacity, consolidation, and pleural effusion (Figure 1A-C). The
8
diagnosis was independently made by radiologists who were blinded to the BPA procedure
9
and results.
10
We used a retrospective cohort study design. To identify predictive factors, we
11
compared patients with and without LI (per patient analysis). To identify triggering factors,
12
we compared BPA procedures with and without PI (per procedure analysis).
13
Furthermore, BPA procedures with LI were classified into two groups: treatment with
14
mechanical ventilation, non-invasive or invasive positive pressure ventilation (ventilator
15
group) or standard oxygen therapy (standard care group) after BPA. We used a ventilator after
16
BPA when oxygen saturation was less than 95%, despite the high concentration of oxygen
17
supplemented by standard care. To identify the exacerbating factors of LI, we compared
18
clinical variables between the ventilator and standard care group.
19
Disclaimer: The manuscript and its contents are confidential, intended for journal review purposes
only, and not to be further disclosed.
7
Data collection and BPA-related vascular injury
1
The investigators reviewed the data including charts, laboratory results, and catheter reports
2
(the number of treated lesions, fluoroscopy time, amount of contrast medium, hemodynamic
3
data, and lesion types). We used the right heart catheterization data obtained one week before
4
the BPA procedure. In terms of the BPA procedural data, three cardiologists unaware of the
5
incidence of LI evaluated the hemodynamic data and carefully reviewed the angiography of
6
BPA.
7
We defined BPA-related vascular injury (BRVI) as angiographic findings of
8
extravasation of the contrast medium with or without simultaneously observed clinical
9
symptoms (cough, bloody sputum, and significant hypoxia). We classified BRVI into three
10
types, based on the angiographic findings: the focal type, focal extravasation of the contrast
11
medium from a distal vessel due to wire injury (Figure 1D); the stain and pooling type,
12
staining and pooling of the contrast medium around dilated vessel due to balloon over-
13
dilatation (Figure 1E); and the diffuse blooming type, diffuse blooming of the contrast
14
medium in the alveoli due to pressure overload caused by the injection (Figure 1F). The
15
BRVI movie files are included in the Data Supplement.
16
Statistical analysis
17
Continuous variables are presented as means ± standard deviation (SD) or as medians with
18
interquartile ranges; categorical variables are presented as numbers and ratios (%). In per-
19
Disclaimer: The manuscript and its contents are confidential, intended for journal review purposes
only, and not to be further disclosed.
8
patient analyses, the difference between patients with or without LI was examined using
1
Student’s t-test or the Mann-Whitney U test for continuous variables and Fisher’s exact test
2
for categorical variables. In per-procedure analyses, we used mixed-effect models or mixed-
3
effect logistic models with compound symmetry correlation matrix to account for the within-
4
participant correlation. In the analyses, non-normally distributed responses were log (x+1)
5
transformed.
6
The predictive and exacerbating factors of LI after BPA were investigated using
7
logistic regression models adjusted for pretreatment patient characteristics (Table S1 in the
8
Data Supplement), and mixed-effect logistic models that included a random intercept to
9
account for the within-participant correlation, adjusted for pretreatment procedural
10
characteristics (Table S2 and S3 in the Data Supplement; except for variables directly related
11
to the requirement of the use of a ventilator: number of treated vessels and segments,
12
fluoroscopy time, and amount of contrast medium). They were indicated by odds ratios (ORs)
13
and 95% confidence intervals (CIs). For mixed-effect logistic models, the degrees of freedom
14
were estimated with the Kenward-Roger approach. Furthermore, we divided the BPA
15
procedures with LI and compared each incidence of mechanical ventilator use after BPA by
16
Fisher’s exact test for independence. All analyses were performed using IBM SPSS Statistics
17
19 (IBM, Armonk, NY, USA) and SAS software, version 9.4 (SAS Institute, Cary, NC,
18
USA). P values of less than 0.05 were considered statistically significant.
19
Disclaimer: The manuscript and its contents are confidential, intended for journal review purposes
only, and not to be further disclosed.
9 1
Results
2
Baseline Characteristics
3
During the study period, we performed 428 BPA procedures in 116 patients with CTEPH
4
(Figure 2). There were 37 patients with a history of BPA treatment who were excluded from
5
this study. Two patients with mechanical ventilation before the initial BPA, and one patient
6
who did not undergo the post-BPA MDCT scan were also excluded. Thus, this study
7
consisted of 76 patients, 15 males (20%) and 61 females (80%), with inoperable CTEPH.
8
Their mean age was 62.7 ± 12.6 years, and their mean body mass index was 22.5 ± 3.7.
9
Patients with CTEPH undergoing BPA procedures between November 2012 and March 2013
10
(n = 65) were included in another study published elsewhere.13
11
Pretreatment patient characteristics are shown in Table 1 (per-patient analysis). Sixty
12
patients (79%) were in the World Health Organization (WHO) functional class III or IV with
13
a high mean PAP (42.5 ± 12.0 mmHg). One patient in WHO functional class I underwent
14
BPA because he wanted to be a professional football player. The median duration between
15
diagnosis and first BPA procedure was 9.1 (1.5-38.1) months.
16
Procedural Characteristics
17
There were 76 patients, on whom a total of 297 BPA procedures were performed. Their
18
procedural characteristics are shown in Table 1 (per-procedure analysis). The number of
19
Disclaimer: The manuscript and its contents are confidential, intended for journal review purposes
only, and not to be further disclosed.
10
vessels dilated per procedure was 4.0 (3.0–6.0). The fluoroscopy time was 46.0 ± 17.4
1
min/procedure, and the amount of contrast medium was 105.0 ± 35.4 mL/procedure. We
2
examined the lesion types based on angiographic classification. If multiple lesion types were
3
treated in a single BPA procedure, we counted each treated lesion type in the procedure as
4
one. We divided the sum of the number of treated lesions by 297 (total number of all the
5
procedure) and presented in Table 1. All BRVIs (100%) were noticed by pulmonary
6
angiography. The most common type of lesions treated was the web lesion type, and BPA was
7
performed for all types of lesions, except for tortuous lesion type. BRVIs occurred during 50
8
procedures (17%) and more than half of the BRVIs were focal type injuries due to wire injury
9
(details are shown in Table S4 in the Data Supplement). LI detected by MDCT scans after
10
BPA occurred in 58 patients (76%) and in 138 BPA procedures (47%). The post-BPA MDCT
11
scans were performed within 24 hours after the procedure (median: 17.1 [4.6-21] hours).
12
None of the patients experienced delayed-onset LI, developed after post-BPA MDCT scans.
13
Forty BPA procedures (13%) required mechanical ventilation (non- invasive) after the
14
procedure. Invasive positive pressure ventilation after BPA was required in four procedures
15
(1.3%), and two of those procedures also required extracorporeal membrane oxygenation
16
support after BPA (0.7%).
17
Triggering factors of LI after BPA
18
Table 2 illustrates the comparison of baseline clinical and hemodynamic variables between
19
Disclaimer: The manuscript and its contents are confidential, intended for journal review purposes
only, and not to be further disclosed.
11
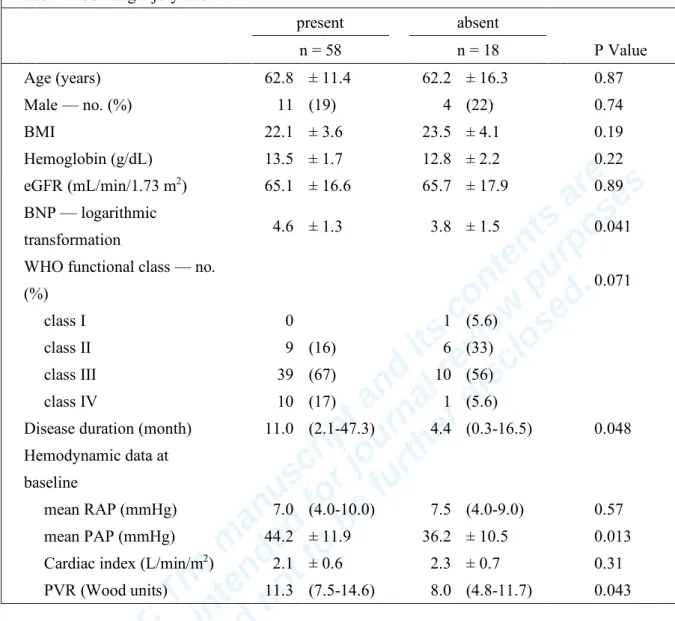
patients with and without LI after BPA. Pretreatment BNP, disease duration, mean PAP, and
1
pulmonary vascular resistance (PVR) were significantly different between the two groups.
2
The univariate correlation of the incidence of LI were pretreatment BNP, WHO functional
3
class, mean PAP, and PVR (Table S1 in the Data Supplement). In a multiple logistic
4
regression model adjusted for pretreatment patient characteristics, WHO functional class was
5
an independent predictor of the incidence of LI after BPA (OR, 4.46; 95% CI, 1.03-19.28; P =
6
0.046) (Figure 3A).
7
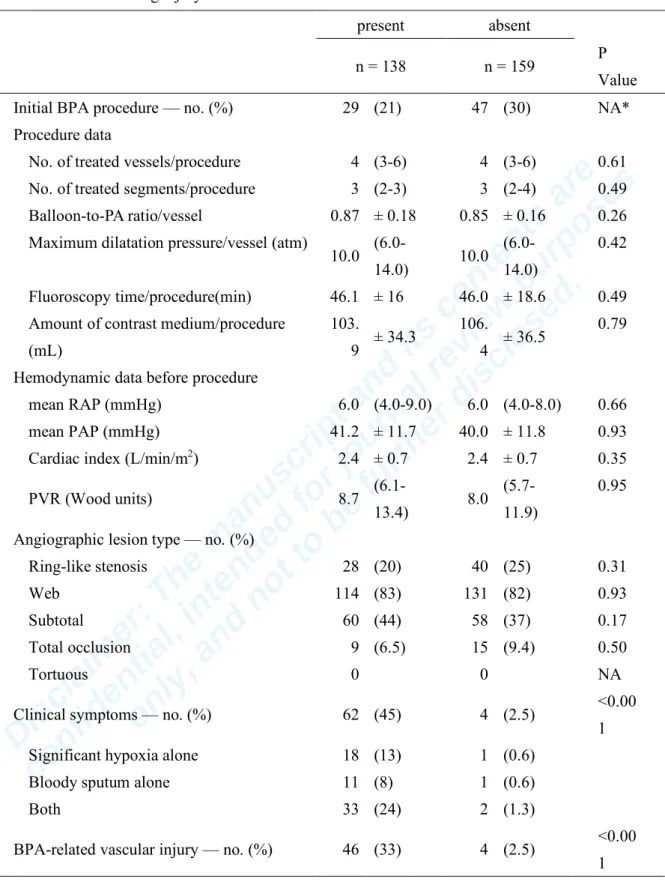
Table 3 illustrates the comparison of lesion characteristics and procedural variables
8
between procedures associated with and without LI among 297 BPA procedures. These were
9
well-balanced between the two groups, except for the incidence of BRVI, which was
10
significantly higher in those with LI than in those without LI (33% and 2.5%; P <0.001)
11
(Figure S1 in the Data Supplement). Post-BPA MDCT was performed within 24 hours in both
12
groups (16.2 [4.6-22.0] hours and 17.4 [4.4-20.6] hours), respectively. Univariate analysis
13
revealed that BRVI is the only variable related to LI (Table S2 in the Data Supplement). In a
14
multiple logistic regression model adjusted for procedural characteristics, an independently
15
strong predictor of the incidence of LI was BRVI (OR, 20.1; 95% CI, 6.43-63.1; P <0.001)
16
(Figure 3B).
17
Exacerbating factors of LI after BPA
18
Mechanical ventilation was required significantly more often after BPA associated with LI
19
Disclaimer: The manuscript and its contents are confidential, intended for journal review purposes
only, and not to be further disclosed.
12
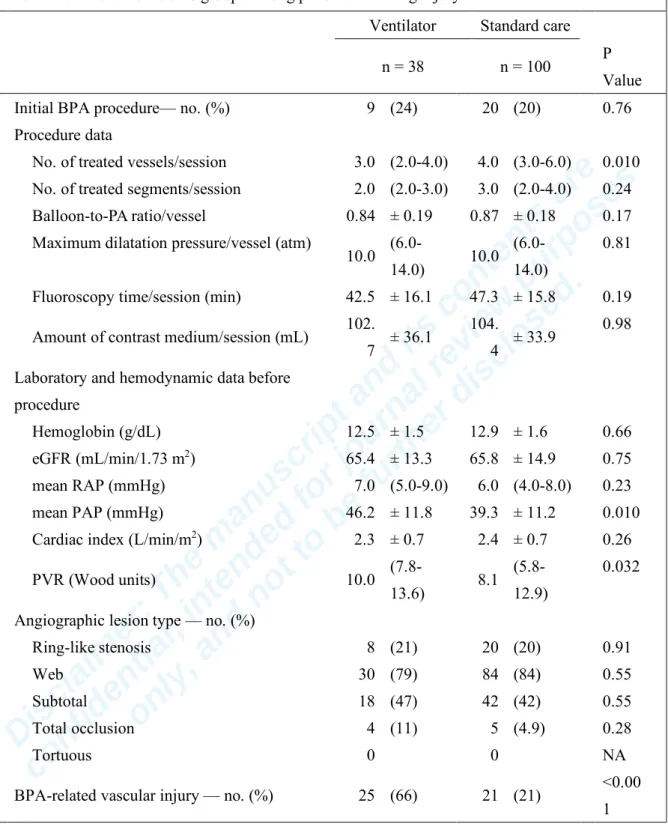
than after BPA without LI (38/138 [28%] vs. 2/159 [1.3%]; P <0.001). Among the 138 BPA
1
procedures associated with LI, we compared the clinical, hemodynamic, and procedural
2
variables between the ventilator (n= 38) and standard care groups (n= 100) (Table 4). The
3
number of treated vessels in the ventilator group was significantly less than in the standard
4
care group (3.0 vs. 4.0; P = 0.010). The mean PAP and PVR in the ventilator group were
5
significantly higher than in the standard care group (46.2 vs. 39.3 mmHg; P = 0.010, and 10.0
6
vs. 8.1 Wood units; P = 0.032, respectively). Furthermore, the incidence of BRVI in the
7
ventilator group was significantly higher than in the standard care group (66% vs. 21%; P
8
<0.001). In the univariate analysis, the risk factors for the requirement of mechanical
9
ventilation after BPA had a high mean PAP and BRVI (Table S3 in the Data Supplement). In a
10
multiple logistic regression model adjusted for procedural characteristics, the independent
11
predictors for ventilator had a high mean PAP (OR, 1.13; 95% CI, 1.03-1.24; P = 0.012), and
12
BRVI (OR, 10.8; 95% CI, 3.77-30.9; P <0.001) (Figure 3C). The median of mean PAP before
13
the BPA procedures was 40 mmHg; when mean PAP was ≥40 mmHg, the requirement for
14
mechanical ventilator was significantly higher than when <40 mmHg (18% vs. 8%; P =
15
0.039) (Figure S2 in the Data Supplement).
16
17
Discussion
18
In the present study, we evaluated the triggering factors of LI after BPA and the exacerbating
19
factors of LI after it occurred. For this purpose, we strictly defined LI as the new appearance
20
Disclaimer: The manuscript and its contents are confidential, intended for journal review purposes
only, and not to be further disclosed.
13
of ground-glass opacity, consolidation, and/or pleural effusion in MDCT images within 24
1
hours after BPA. We found that poorer WHO functional class as a patient factor and BRVI as
2
a procedural factor are independent predictors of LI after BPA, and that BRVI and a high
3
mean PAP before BPA were independent predictive factors for mechanical ventilator
4
requirement once LI occurred. To our knowledge, this is the first study to clarify the main
5
cause of LI after BPA.
6
The incidence of “reperfusion” pulmonary edema was reported to be 61% in the
7
original BPA study by Feinstein et al.,7 30-60% in some refined BPA studies,8, 9, 11 and 46.5%
8
in this study, though its definition has varied among studies. Reperfusion pulmonary edema is
9
a leading complication after PEA, and its incidence are reported to be 16-22%.14, 15 LI after
10
BPA has been considered to be the same as so-called “reperfusion” pulmonary edema in PEA.
11
Since PEA and BPA are quite different procedures, we hypothesized that “reperfusion” lung
12
injury after BPA might be different from reperfusion pulmonary edema after PEA.
13
By carefully reviewing MDCT images, we found that the so-called “reperfusion”
14
pulmonary edema was a focal infiltration only at the site of BPA-targeted lesions. The post-
15
BPA MDCT scans were performed within 24 hours after the procedure, and no patient
16
experienced delayed-onset LI developed more than 24 hours after BPA. The number of
17
treated lesions and the angiographic type of treated lesion, which could influence the extent
18
and degree of reperfusion, showed no correlation with the occurrence of LI. The treated
19
Disclaimer: The manuscript and its contents are confidential, intended for journal review purposes
only, and not to be further disclosed.
14
number of the subtotal and total occlusion lesions in procedures with BRVI tended to be
1
greater than in procedures without BRVI (50% vs. 38%, and 10% vs. 7.6%, respectively, in
2
Table S4 in the Supplementary file). Thus, the lesion characteristics could be related to the
3
incidence of BRVI and LI after BPA; however, there was no statistical significance, because
4
of the small number of the high-risk lesion types. Multivariate analysis indicated that BRVI is
5
the independent factor associated with LI. These results suggested that almost all LIs after
6
BPA were caused by vascular injury due to a procedural complication during BPA. Our group
7
reported the histological changes in pulmonary arteries during BPA, which may explain a part
8
of the mechanism of vascular injury.16 In this case, BPA caused the organized thrombi to be
9
forced to one side and the dissection of the pulmonary artery caused a false lumen, which
10
increased the risk of vascular injury. There is always a risk of vascular injury due to
11
procedural complications (e.g. wire injury and over-dilation by the balloon) during BPA.
12
Figure 4 illustrates the incidence and relationships of complications associated with BPA. LI
13
after BPA collectively means all pulmonary abnormalities occurred after BPA detected by
14
MDCT. Based on the results of the present study, vascular injury due to procedural
15
complication is the main cause of LI after BPA. A slight injury could not be visible as an
16
angiographic finding of extravasation, and only a severe vascular injury could be visible and
17
recognized as BRVI (approximately one-third of LI). In other words, the occurrence of
18
vascular injury could not be rejected only on the basis of the absence of the angiographic
19
Disclaimer: The manuscript and its contents are confidential, intended for journal review purposes
only, and not to be further disclosed.
15
finding of extravasation. Finally, severe vascular injuries can appear as bloody sputum, and
1
some of them require ventilator support.
2
Furthermore, this study showed that a high mean PAP before BPA is an independent
3
risk factor of severe LI requiring mechanical ventilation after BPA. Although some studies
4
also reported that hemodynamic parameters affected the occurrence of LI,7, 9, 11 they did not
5
reveal the mechanism of LI occurrence in detail. As per the results of this study, in the case of
6
vascular injury during BPA, direct exposure of high pressure to the injured pulmonary
7
arteries could induce and exacerbate LI.
8
Previous studies, including ours, have reported some approaches to reduce the
9
occurrence of LI, such as the preoperative application of epoprostenol and
10
methylprednisolone, and the prophylactic use of non-invasive positive pressure ventilation.8,
11
17, 18 However, these approaches failed to reduce the incidence of LI, because they did not
12
prevent the pulmonary vascular injury associated with BPA. We have demonstrated that there
13
is a learning curve effect in the BPA procedure to reduce the occurrence of LI.8 Recently, we
14
carried out the BPA procedure very carefully to reduce procedural complications, so that the
15
incidence of LI after BPA in this study was lower than that in previous studies12 (47% and
16
67%, respectively), although we intensively examined MDCT scans and counted the number
17
of LI in the present study. However, complete prevention of vascular injury seems impossible
18
in the real world. To prevent the worsening of LI after BPA, we propose the following two
19
Disclaimer: The manuscript and its contents are confidential, intended for journal review purposes
only, and not to be further disclosed.
16
important points: (1) prevent pressure overload to the distal pulmonary artery, and (2) to
1
establish treatment for pulmonary hemorrhage caused by procedural complication during
2
BPA. To prevent pressure overload, avoidance of the over-dilatation of the pulmonary artery
3
during BPA is necessary. Furthermore, the establishment of a treatment for severe pulmonary
4
hemorrhage during BPA, without reducing BPA treatment efficacy, is indispensable.
5
In conclusion, we demonstrate that vascular injury due to procedural complications
6
during BPA is the main cause of LI, which we identified by analyzing MDCT scans, and we
7
revealed that a high mean PAP before BPA was related to a worsening of LI. It is important to
8
note that most cases of LI that were detected on MDCT scans were subclinical; thus, the
9
routine use of MDCT scanning for the care after BPA seems unnecessary.
10
Limitations
11
This study has several limitations. First, this study was a retrospective observational study in
12
a single high-volume center. Predictors of LI after BPA in this study should be confirmed in a
13
prospective, multi-center study. Second, selection bias and residual confounding bias were
14
inevitable in this type of observational study.
15
16
Acknowledgement
17
We are indebted to Ms. Akiko Ohina and Ms. Mihoko Yoshimori for their assistance.
18
Disclaimer: The manuscript and its contents are confidential, intended for journal review purposes
only, and not to be further disclosed.
17
Our findings were presented in part at the European Society of Cardiology congress 2015,
1
London, United Kingdom on August 31, 2015, and at the 80th annual scientific meeting of the
2
Japanese Circulation Society, Sendai, Japan on March 20, 2016.
3
4
Sources of Funding
5
None
6
7
Disclosures
8
Dr Ejiri, Dr Fujii and Dr Ito received no financial support. Dr Ogawa received lecture fees from
9
Bayer Yakuhin, Ltd; Pfizer Japan, Inc; Nippon Shinyaku, Co, Ltd. Dr Matsubara received
10
lecture fees from AOP orphan Pharmaceuticals AG; Bayer Yakuhin, Ltd; Pfizer Japan, Inc;
11
Nippon Shinyaku, Co, Ltd; Actelion Pharmaceuticals Japan, Ltd; GlaxoSmithKline K.K.; and
12
Kaneka Medix Corporation.
13
Disclaimer: The manuscript and its contents are confidential, intended for journal review purposes
only, and not to be further disclosed.
18
References
1
1. Piazza G, Goldhaber SZ. Chronic thromboembolic pulmonary hypertension. N Engl J
2
Med. 2011;364:351-360. doi: 10.1056/NEJMra0910203.
3
2. Kim NH, Delcroix M, Jenkins DP, Channick R, Dartevelle P, Jansa P, Lang I, Madani
4
MM, Ogino H, Pengo V, Mayer E. Chronic thromboembolic pulmonary hypertension. J Am
5
Coll Cardiol. 2013;62:D92-99. doi: 10.1016/j.jacc.2013.10.024.
6
3. Lang IM, Madani M. Update on chronic thromboembolic pulmonary hypertension.
7
Circulation. 2014;130:508-518. doi: 10.1161/circulationaha.114.009309.
8
4. Cabrol S, Souza R, Jais X, Fadel E, Ali RH, Humbert M, Dartevelle P, Simonneau G,
9
Sitbon O. Intravenous epoprostenol in inoperable chronic thromboembolic pulmonary
10
hypertension. J Heart Lung Transplant. 2007;26:357-362. doi: 10.1016/j.healun.2006.12.014.
11
5. Madani MM, Auger WR, Pretorius V, Sakakibara N, Kerr KM, Kim NH, Fedullo PF,
12
Jamieson SW. Pulmonary endarterectomy: recent changes in a single institution's experience
13
of more than 2,700 patients. Ann Thorac Surg. 2012;94:97-103; discussion 103. doi:
14
10.1016/j.athoracsur.2012.04.004.
15
6. Pepke-Zaba J, Delcroix M, Lang I, Mayer E, Jansa P, Ambroz D, Treacy C, D'Armini
16
AM, Morsolini M, Snijder R, Bresser P, Torbicki A, Kristensen B, Lewczuk J, Simkova I,
17
Barbera JA, de Perrot M, Hoeper MM, Gaine S, Speich R, Gomez-Sanchez MA, Kovacs G,
18
Hamid AM, Jais X, Simonneau G. Chronic thromboembolic pulmonary hypertension
19
Disclaimer: The manuscript and its contents are confidential, intended for journal review purposes
only, and not to be further disclosed.
19
(CTEPH): results from an international prospective registry. Circulation. 2011;124:1973-1981.
1
doi: 10.1161/circulationaha.110.015008.
2
7. Feinstein JA, Goldhaber SZ, Lock JE, Ferndandes SM, Landzberg MJ. Balloon
3
pulmonary angioplasty for treatment of chronic thromboembolic pulmonary hypertension.
4
Circulation. 2001;103:10-13. doi: 10.1161/01.CIR.103.1.10.
5
8. Mizoguchi H, Ogawa A, Munemasa M, Mikouchi H, Ito H, Matsubara H. Refined
6
balloon pulmonary angioplasty for inoperable patients with chronic thromboembolic
7
pulmonary hypertension. Circ Cardiovasc Interv. 2012;5:748-755. doi:
8
10.1161/CIRCINTERVENTIONS.112.971077.
9
9. Kataoka M, Inami T, Hayashida K, Shimura N, Ishiguro H, Abe T, Tamura Y, Ando
10
M, Fukuda K, Yoshino H, Satoh T. Percutaneous transluminal pulmonary angioplasty for the
11
treatment of chronic thromboembolic pulmonary hypertension. Circ Cardiovasc Interv.
12
2012;5:756-762. doi: 10.1161/circinterventions.112.971390.
13
10. Lang I, Meyer BC, Ogo T, Matsubara H, Kurzyna M, Ghofrani HA, Mayer E, Brenot
14
P. Balloon pulmonary angioplasty in chronic thromboembolic pulmonary hypertension. Eur
15
Respir Rev. 2017;26:160119. doi: 10.1183/16000617.0119-2016.
16
11. Inami T, Kataoka M, Shimura N, Ishiguro H, Yanagisawa R, Taguchi H, Fukuda K,
17
Yoshino H, Satoh T. Pulmonary edema predictive scoring index (PEPSI), a new index to predict
18
risk of reperfusion pulmonary edema and improvement of hemodynamics in percutaneous
19
Disclaimer: The manuscript and its contents are confidential, intended for journal review purposes
only, and not to be further disclosed.
20
transluminal pulmonary angioplasty. JACC Cardiovasc Interv. 2013;6:725-736. doi:
1
10.1016/j.jcin.2013.03.009.
2
12. Kawakami T, Ogawa A, Miyaji K, Mizoguchi H, Shimokawahara H, Naito T, Oka T,
3
Yunoki K, Munemasa M, Matsubara H. Novel Angiographic Classification of Each Vascular
4
Lesion in Chronic Thromboembolic Pulmonary Hypertension Based on Selective Angiogram
5
and Results of Balloon Pulmonary Angioplasty. Circ Cardiovasc Interv. 2016;9:e003318. doi:
6
10.1161/circinterventions.115.003318.
7
13. Ogawa A, Satoh T, Fukuda T, Sugimura K, Fukumoto Y, Emoto N, Yamada N, Yao A,
8
Ando M, Ogino H, Tanabe N, Tsujino I, Hanaoka M, Minatoya K, Ito H, Matsubara H. Balloon
9
Pulmonary Angioplasty for Chronic Thromboembolic Pulmonary Hypertension: Results of a
10
Multicenter Registry. Circ Cardiovasc Qual Outcomes. 2017;10. doi:
11
10.1161/circoutcomes.117.004029.
12
14. Thistlethwaite PA, Kaneko K, Madani MM, Jamieson SW. Technique and outcomes
13
of pulmonary endarterectomy surgery. Ann Thorac Cardiovasc Surg. 2008;14:274-282.
14
15. Adams A, Fedullo PF. Postoperative management of the patient undergoing
15
pulmonary endarterectomy. Semin Thorac Cardiovasc Surg. 2006;18:250-256. doi:
16
10.1053/j.semtcvs.2006.09.002.
17
16. Kitani M, Ogawa A, Sarashina T, Yamadori I, Matsubara H. Histological changes of
18
pulmonary arteries treated by balloon pulmonary angioplasty in a patient with chronic
19
Disclaimer: The manuscript and its contents are confidential, intended for journal review purposes
only, and not to be further disclosed.
21
thromboembolic pulmonary hypertension. Circ Cardiovasc Interv. 2014;7:857-859. doi:
1
10.1161/circinterventions.114.001533.
2
17. Rana S, Jenad H, Gay PC, Buck CF, Hubmayr RD, Gajic O. Failure of non-invasive
3
ventilation in patients with acute lung injury: observational cohort study. Crit Care.
4
2006;10:R79. doi: 10.1186/cc4923.
5
18. Bresser P, Fedullo PF, Auger WR, Channick RN, Robbins IM, Kerr KM, Jamieson
6
SW, Rubin LJ. Continuous intravenous epoprostenol for chronic thromboembolic pulmonary
7
hypertension. Eur Respir J. 2004;23:595-600. doi: 10.1183/09031936.04.00020004.
8
9 10
Disclaimer: The manuscript and its contents are confidential, intended for journal review purposes
only, and not to be further disclosed.
22
Figure legends
1
Figure 1: Representative computed tomography (CT) scans and angiographic findings of lung
2
injury (LI) after balloon pulmonary angioplasty (BPA) showing BPA-related vascular injury.
3
-A: LI is defined by ground-glass opacity that is seen on CT images after BPA (white arrows).
4
-B: LI is defined by consolidation that is seen on CT images after BPA (white triangles).
5
-C: LI is defined by pleural effusion that is seen on CT images after BPA (black triangles).
6
-D: Vascular injury induced by inserting the wire too deeply.
7
After wiring, pulmonary angiography shows focal extravasation of the contrast medium from
8
the wire tip inserted in the distal vessel (white arrow).
9
-E: Vascular injury induced by over-dilatation. After balloon dilatation, pulmonary
10
angiography shows the staining and pooling of the contrast medium around the dilated vessel
11
(white arrows).
12
-F: Vascular injury induced by the pressure overlord caused during the injection of the contrast
13
medium. Simultaneously with the injection, pulmonary angiography shows a diffuse blooming
14
contrast of the distal site in the target area (white arrows).
15
16
Figure 2: Recruitment and follow-up flow diagram per patient and procedure analysis.
17
Balloon pulmonary angioplasty (BPA) procedures were divided into two groups: lung injury
18
(LI) after BPA or without. Chronic thromboembolic pulmonary hypertension (CTEPH) patients
19
Disclaimer: The manuscript and its contents are confidential, intended for journal review purposes
only, and not to be further disclosed.
23
who underwent BPA were divided into two groups: LI after BPA or without. LI after BPA cases
1
were divided into two groups: treatment using mechanical ventilation (ventilator group) or
2
using standard oxygen therapy (standard care group).
3
4
Figure 3: Adjusted odds ratio (OR) for lung injury (LI) after balloon pulmonary angioplasty
5
(BPA) and the use of mechanical ventilator.
6
-A: Adjusted OR for LI after BPA per patient analysis.
7
Adjustment for age, log transformed brain natriuretic peptide (log BNP), World Health
8
Organization (WHO) functional class III/IV or not, and disease duration (Supplementary file
9
Table S2).
10
-B: Adjusted OR for LI after BPA per procedure analysis.
11
Adjustment for the initial BPA procedure or not, number of treated vessels, mean right atrium
12
pressure >5 mmHg or not, mean PAP, cardiac index, PVR, angiographic lesion type per
13
procedure, and BPA-related vascular injury or not were made (Supplementary file Table S3).
14
-C: Adjusted OR for the use of mechanical ventilator after BPA in procedures with LI.
15
Adjustment for mean PAP, cardiac index, PVR, and BPA-related vascular injury or not were
16
made (Supplementary file Table S4).
17
18
Figure 4: The incidence of complications associated with balloon pulmonary angioplasty
19
Disclaimer: The manuscript and its contents are confidential, intended for journal review purposes
only, and not to be further disclosed.
24
(BPA) and a schematic diagram of the etiology of lung injury after BPA.
1
-A: Bar graph summarizes the incidence of complications associated with BPA: lung injury
2
after BPA (white bar, 46% of all BPA procedures); BPA-related vascular injuries (BRVI) (red
3
bar, 17%); clinical symptoms (yellow bar, 22%); and requirement for mechanical ventilator
4
after BPA (green bar, 13%).
5
-B: Multi-detector computed tomography (MDCT) scanning could detect the slightest LI after
6
BPA (white circle), mostly caused by vascular injury from procedural complications during
7
BPA (gray circle). Vascular injuries with some exacerbating factors become BRVIs, which are
8
detected using angiography (red circle). Severe vascular injuries can appear as clinical
9
symptoms, such as hypoxia, bloody sputum or both (yellow circle), and some of the vascular
10
injuries with clinical symptoms require mechanical ventilator (green circle). Percentages of
11
types for BRVI, mechanical ventilator, and clinical symptom are shown in the lower panels.
12 13
Disclaimer: The manuscript and its contents are confidential, intended for journal review purposes
only, and not to be further disclosed.
25
Tables
1
Table 1. Patients and procedural characteristics Patient characteristics (n = 76)
Age 62.7 ± 12.6
Male — no. (%) 15 (20)
BMI 22.5 ± 3.7
Hemoglobin (g/dL) 13.2 ± 1.8
eGFR (mL/min/1.73 m2) 64.6 ± 17.1
BNP — logarithmic transformation 4.4 ± 1.3
WHO functional class — no. (%)
class I 1 (1.3)
class II 15 (20)
class III 49 (64)
class IV 11 (14)
Disease duration (month) 9.1 (1.5-38.1)
Hemodynamic data at baseline
mean RAP (mmHg) 7.0 (4.0-10.0)
mean PAP (mmHg) 42.5 ± 12.0
Cardiac index (L/min/m2) 2.2 ± 0.6
PVR (Wood units) 10.3 (5.3-14.3)
Lung injury after BPA — no. (%) 58 (76)
Procedural characteristics (n = 297)
Treated vessels — no. 1247
Procedure data
No. of treated vessels/procedure 4.0 (3.0-6.0)
No. of treated segments/procedure 3.0 (2.0-4.0)
Treated vessel size/vessel (mm) 3.6 (3.1-4.5)
Balloon size/vessel (mm) 3.0 (2.5-4.0)
Balloon-to-PA ratio/vessel 0.86 ± 0.17
Maximum dilatation pressure/vessel (atm) 10.0 (6.0-14.0)
No. of balloons/procedure 2.0 (2.0-3.0)
IVUS use — no. (%) 296 (99)
Fluoroscopy time/procedure (min) 46.0 ± 17.4
Amount of contrast medium/procedure (mL) 105.0 ± 35.4
Hemodynamic data before procedure
mean RAP (mmHg) 6.0 (4.0-8.0)
mean PAP (mmHg) 40.5 ± 11.7
Cardiac index (L/min/m2) 2.4 ± 0.7
Disclaimer: The manuscript and its contents are confidential, intended for journal review purposes
only, and not to be further disclosed.
26
PVR (Wood units) 8.5 (5.9-12.4)
Angiographic lesion type — no. (%)
Ring-like stenosis 68 (23)
Web 245 (83)
Subtotal 118 (40)
Total occlusion 24 (8.1)
Tortuous 0
Complications
Clinical symptoms — no. (%) 66 (22)
Significant hypoxia alone 19 (6)*
Bloody sputum alone 12 (4)*
Both 35 (12)*
BPA-related vascular injury — no. (%) 50 (17)
Lung injury after BPA — no. (%) 138 (46)
Ground-glass opacity 119 (86)†
Consolidation 73 (53)†
Pleural effusion 15 (11)†
Data are presented as mean ± standard deviation, no. (%) or median (interquartile range).
Disease duration is the time between diagnosis and the first BPA.
* The incidence of clinical symptoms attributed to procedures during BPA.
† The incidence of new abnormalities in post-BPA MDCT scans in BPA procedures with lung injury after BPA.
BMI, body mass index; eGFR, estimated glomerular filtration rate; BNP, brain natriuretic peptide; PA, pulmonary artery; IVUS, Intravascular ultrasound; RAP, right arterial pressure;
PAP, pulmonary artery pressure; PVR, pulmonary vascular resistance; BPA, balloon pulmonary angioplasty; MDCT, multi-detector computed tomography; WHO, World Health Organization.
1 2
Disclaimer: The manuscript and its contents are confidential, intended for journal review purposes
only, and not to be further disclosed.
27
Table 2. Comparison of baseline clinical and hemodynamic variables between patients with and without lung injury after BPA
present absent
n = 58 n = 18 P Value
Age (years) 62.8 ± 11.4 62.2 ± 16.3 0.87
Male — no. (%) 11 (19) 4 (22) 0.74
BMI 22.1 ± 3.6 23.5 ± 4.1 0.19
Hemoglobin (g/dL) 13.5 ± 1.7 12.8 ± 2.2 0.22 eGFR (mL/min/1.73 m2) 65.1 ± 16.6 65.7 ± 17.9 0.89 BNP — logarithmic
transformation 4.6 ± 1.3 3.8 ± 1.5 0.041
WHO functional class — no.
(%) 0.071
class I 0 1 (5.6)
class II 9 (16) 6 (33)
class III 39 (67) 10 (56)
class IV 10 (17) 1 (5.6)
Disease duration (month) 11.0 (2.1-47.3) 4.4 (0.3-16.5) 0.048 Hemodynamic data at
baseline
mean RAP (mmHg) 7.0 (4.0-10.0) 7.5 (4.0-9.0) 0.57 mean PAP (mmHg) 44.2 ± 11.9 36.2 ± 10.5 0.013 Cardiac index (L/min/m2) 2.1 ± 0.6 2.3 ± 0.7 0.31
PVR (Wood units) 11.3 (7.5-14.6) 8.0 (4.8-11.7) 0.043
Data are presented as mean ± standard deviation, no. (%) or median (interquartile range).
Disease duration is the time between diagnosis and the first balloon pulmonary angioplasty.
BNP, brain natriuretic peptide; RAP, right arterial pressure; PAP, pulmonary artery pressure;
PVR, pulmonary vascular resistance; WHO, World Health Organization.
1 2
Disclaimer: The manuscript and its contents are confidential, intended for journal review purposes
only, and not to be further disclosed.
28
Table 3. Comparison of lesion characteristics and procedural variables between procedures with and without lung injury
present absent
n = 138 n = 159 P
Value Initial BPA procedure — no. (%) 29 (21) 47 (30) NA*
Procedure data
No. of treated vessels/procedure 4 (3-6) 4 (3-6) 0.61 No. of treated segments/procedure 3 (2-3) 3 (2-4) 0.49 Balloon-to-PA ratio/vessel 0.87 ± 0.18 0.85 ± 0.16 0.26 Maximum dilatation pressure/vessel (atm)
10.0 (6.0-
14.0) 10.0 (6.0- 14.0)
0.42 Fluoroscopy time/procedure(min) 46.1 ± 16 46.0 ± 18.6 0.49 Amount of contrast medium/procedure
(mL)
103.
9 ± 34.3 106.
4 ± 36.5 0.79
Hemodynamic data before procedure
mean RAP (mmHg) 6.0 (4.0-9.0) 6.0 (4.0-8.0) 0.66
mean PAP (mmHg) 41.2 ± 11.7 40.0 ± 11.8 0.93
Cardiac index (L/min/m2) 2.4 ± 0.7 2.4 ± 0.7 0.35
PVR (Wood units) 8.7 (6.1-
13.4) 8.0 (5.7- 11.9)
0.95
Angiographic lesion type — no. (%)
Ring-like stenosis 28 (20) 40 (25) 0.31
Web 114 (83) 131 (82) 0.93
Subtotal 60 (44) 58 (37) 0.17
Total occlusion 9 (6.5) 15 (9.4) 0.50
Tortuous 0 0 NA
Clinical symptoms — no. (%) 62 (45) 4 (2.5) <0.00
1
Significant hypoxia alone 18 (13) 1 (0.6)
Bloody sputum alone 11 (8) 1 (0.6)
Both 33 (24) 2 (1.3)
BPA-related vascular injury — no. (%) 46 (33) 4 (2.5) <0.00 1
Data are presented as mean ± standard deviation, no. (%), or median (interquartile range).
Disclaimer: The manuscript and its contents are confidential, intended for journal review purposes
only, and not to be further disclosed.
29
*P-value was not calculated because the fitting process of the model did not converge.
BPA, balloon pulmonary angioplasty; PA, pulmonary artery; RAP, right arterial pressure;
PAP, pulmonary artery pressure; PVR, pulmonary vascular resistance.
1 2
Disclaimer: The manuscript and its contents are confidential, intended for journal review purposes
only, and not to be further disclosed.
30
Table 4. Comparison of clinical, hemodynamic, and procedural variables between the ventilator and standard care groups among patients with lung injury
Ventilator Standard care
n = 38 n = 100 P
Value Initial BPA procedure— no. (%) 9 (24) 20 (20) 0.76
Procedure data
No. of treated vessels/session 3.0 (2.0-4.0) 4.0 (3.0-6.0) 0.010 No. of treated segments/session 2.0 (2.0-3.0) 3.0 (2.0-4.0) 0.24 Balloon-to-PA ratio/vessel 0.84 ± 0.19 0.87 ± 0.18 0.17 Maximum dilatation pressure/vessel (atm)
10.0 (6.0-
14.0) 10.0 (6.0- 14.0)
0.81 Fluoroscopy time/session (min) 42.5 ± 16.1 47.3 ± 15.8 0.19 Amount of contrast medium/session (mL) 102.
7 ± 36.1 104.
4 ± 33.9 0.98 Laboratory and hemodynamic data before
procedure
Hemoglobin (g/dL) 12.5 ± 1.5 12.9 ± 1.6 0.66
eGFR (mL/min/1.73 m2) 65.4 ± 13.3 65.8 ± 14.9 0.75 mean RAP (mmHg) 7.0 (5.0-9.0) 6.0 (4.0-8.0) 0.23
mean PAP (mmHg) 46.2 ± 11.8 39.3 ± 11.2 0.010
Cardiac index (L/min/m2) 2.3 ± 0.7 2.4 ± 0.7 0.26
PVR (Wood units) 10.0 (7.8-
13.6) 8.1 (5.8- 12.9)
0.032
Angiographic lesion type — no. (%)
Ring-like stenosis 8 (21) 20 (20) 0.91
Web 30 (79) 84 (84) 0.55
Subtotal 18 (47) 42 (42) 0.55
Total occlusion 4 (11) 5 (4.9) 0.28
Tortuous 0 0 NA
BPA-related vascular injury — no. (%) 25 (66) 21 (21) <0.00 1
Data are presented as mean ± standard deviation, no. (%) or median (interquartile range).
eGFR, estimated glomerular filtration rate; PA, pulmonary artery; RAP, right arterial pressure; PAP, pulmonary artery pressure; PVR, pulmonary vascular resistance; BPA, balloon pulmonary angioplasty.
1
Disclaimer: The manuscript and its contents are confidential, intended for journal review purposes
only, and not to be further disclosed.
31
Figures
1
Figure 1
2
3 4
Disclaimer: The manuscript and its contents are confidential, intended for journal review purposes
only, and not to be further disclosed.
32
Figure 2
1
2
Disclaimer: The manuscript and its contents are confidential, intended for journal review purposes
only, and not to be further disclosed.
33
Figure 3
1
2
Disclaimer: The manuscript and its contents are confidential, intended for journal review purposes
only, and not to be further disclosed.
34
Figure 4
1
2