An optimal medical therapy for efficient cardiovascular protection
in subjects with coronary artery diseases in Japan: Comparisons
and analyses by quasi-randomized controlled trials with propensity
score matching and inverse probability treatment weighting
methods for a Japanese cohort
Tabito Kino, MD, PhD, Tomoaki Ishigami, MD, PhD, Hiroshi Doi, MD, PhD, Lin Chen, MD, PhD,
Rie Nakashima-Sasaki, MD, PhD, Michiko Sugiyama, PhD, Kentaro Arakawa, MD, PhD,
Shintaro Minegishi, MD, PhD, Kaito Abe, MD, PhD, Hiromichi Wakui, MD, PhD,
Kengo Azushima, MD, PhD and Kouichi Tamura, MD, PhD
Abstract:
Background: Optimal medical therapy (OMT) may play an important role in preventing secondary events in coronary artery diseases (CAD) and peripheral artery diseases (PAD). However, few practical pharmaceutical evidence-based regi-mens are available for patients with CAD and PAD to prevent secondary cardiovascular events due to practical reasons for performing clinical trials using the OMT regimen.Methods: To elucidate OMT for subjects with prior cardiovascular dis-eases in Japan, we performed a quasi-randomized clinical trial using statistically sophisticated propensity score matching and subsequent inverse probability treatment weighting methods to test which combination of medicines was most effective as OMT to prevent secondary cardiovascular events. Two hundred and sixty-one subjects who were admitted in our hospital were consecutively enrolled. We constructed the Cox models for the composite of death, myocardial infarction, stroke, ad-mission for heart failure, and target region revascularization. Results: On multivariable inverse probability of treatment-weighted Cox modeling, the best combination was antiplatelet agents, statins, and calcium channel blockers (CCBs) to pre-vent major adverse cardiac epre-vents (MACE) in patients with CAD in Japan, and significant effects were found in the new OMT group for both MACE and cardiovascular death. In contrast, we could not find any significantly effective combina-tions in patients with PAD. Conclusions: These findings suggested that the multiple medical regimen including antiplate-let agents, statins, and CCBs, which might be prescribed as new OMT, has significant effects for the prevention of secon-dary events in patients with CAD in Japan.
Key words:
Optimal medical therapy, Statins, Calcium channel blockers, Quasi-RCT, IPTW method
Introduction
Atherosclerosis is an inflammatory disease characterized by intense inflammatory activity; it is an increasingly sig-nificant threat to human health worldwide1)
. The most severe clinical event is the plaque rupture, which exposes the prothrombotic materials in the plaque to the blood and causes sudden thrombotic occlusion of the artery at the site
of disruption, resulting in myocardial infarction or ischemic stroke. Coronary plaque disruption evolves most frequently from mild to moderate stenosis2)
; thus, early detection and treatment of premature atherosclerosis are considered impor-tant.
According to the COURAGE trial3) and various clinical trials, optimal medical therapy (OMT) is significant for the cardiovascular protection in patients with stable coronary
Department of Medical Science and Cardiorenal Medicine, Yokohama City University Graduate School of Medicine Corresponding author: Tomoaki Ishigami, MD, PhD, [email protected]
Received: March 24, 2020, Accepted: June 16, 2020 CopyrightⒸ 2020 Japan Society for Vascular Failure
artery disease (CAD). Current guidelines that support the aggressive use of OMT before revascularization are framed so that the need for the additional treatment with percutane-ous coronary intervention (PCI) to control symptoms can be assessed4,5). In previous reports, antiplatelet agents, beta-blockers, statins, and angiotensin converting enzyme inhibi-tor I (ACE-I) or angiotensin recepinhibi-tor blockers (ARB) are prescribed as OMT for patients with CAD in western coun-tries3)
. In Japan, multiple trials have been conducted to eluci-date the effects of these drugs individually6-9). However, vari-ous investigators in Japan consider that Japanese OMT is different from the conventional OMT, and there are no stud-ies available to investigate the combination therapy for sec-ondary CAD prevention.
In addition, a few studies have reported the cardiovascular diseases prevention with medical therapy in patients with peripheral artery disease (PAD). Japanese guidelines indicate that cilostazol, beraprost sodium, and statins are efficient for claudication improvement10-12). In addition, statins have car-diovascular event reduction in high C-reactive protein (CRP) patients with PAD13). However, no randomized controlled trial (RCT) is currently available for MACE prevention and limb amputation by using combination drug therapy because the number of patients with PAD is fewer than that of the patients with CAD.
Therefore, currently we conducted a quasi-RCT using the inverse probability of treatment weighting (IPTW) tech-nique14) applied with propensity score (PS) matching to elu-cidate the best pharmaceutical combination of OMT in Japa-nese patients with CAD and PAD.
Methods
Study Participants
A retrospective cohort study using propensity score matching and subsequent IPTW method was conducted. Pa-tients admitted to our department to receive PCI due to CAD or endovascular treatment (EVT) due to PAD from November 1, 2012, to June 30, 2015 were randomly en-rolled and with informed consent and study approval. Pa-tients with acute myocardial infarction (AMI), unstable an-gina pectoris (UAP), stable AP, and arteriosclerosis obliter-ans (ASO) were included. Observation was performed from November 1, 2012 to December 31, 2015. Patients’ informa-tion was collected from their electronic medical record and telephone interview, and excluded when they cannot be fol-lowed up at the end of the observation period.
The study protocol was registered and approved by the Ethical Committee of the Yokohama City University Hospi-tal (UMIN000035665, R000040627).
Outcome
The primary outcome was major composite adverse car-diac event (MACE). MACE was defined as follows: non-fatal AMI, cardiovascular death, limb amputation,
hospitali-zation for UAP, heart failure (HF), and repeated revasculari-zation for target lesion. We examined the patient’s medical records when MACE occurred and calculated the day from the start of enrollment.
Statistical Analysis
First, the participants were divided into two groups ac-cording to presence of either CAD or PAD. Baseline charac-teristics were presented as means and standard errors for continuous variables and frequencies and percentages for categorical variables.
Then, cumulative event rate was compared using the Kaplan-Meier method. The primary drug efficacy was evalu-ated using the stratified log-rank test. Categorical variables were compared using the chi-square test or Wilcoxon rank-sum test, and continuous variables were compared using the Student’s t-test.
Conducting the RCT for our subjects is challenging and non-realistic because it conflicts with ethical concerns. Moreover, testing various combinations of OMTs requires much effort, and it is expensive and time-consuming. The PS matching is a statistically sophisticated method to de-velop a quasi-RCT. IPTW using propensity score allows for the marginal hazard ratio estimation with minimal bias and results in estimates with lower mean squared error when ap-proximating the effect of treatment15). In other words, the IPTW method does not decrease the number of patients for background adjustment; we can handle the weighed number directly, and it does not adjust the treatment group to the control group in the background compared with PS match-ing.
For the PS calculation, we used a logistic regression model in which the treatment status was regressed for the following three baseline characteristics: age, sex, and body mass index (BMI). Thereafter, we selected an effective com-bination and matched the baseline characteristics. Categori-cal variables were compared using the chi-square test or Wilcoxon rank-sum test, and continuous variables were compared using the Student’s t-test. Subsequently, multivari-able models were adjusted with the IPTW method combined with logistic regression modeling to control potential con-founders: age, sex, BMI, systolic blood pressure, triglyc-eride, high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), hemoglobin A1c (HbA1c), CRP, estimated glomerular filtration ratio (eGFR), uric acid (UA), d-dimer, and hemoglobin (Hb). We con-ducted a Cox hazards model analysis to consider an efficient survival time. Finally, we performed the log-rank test to identify the treatment effect as well as the patients’ survival time.
All statistical analyses were performed using the IBM SPSS Statistics 21.0 (IBM, Somers, NY, USA) and R 3.2.2 (R Foundation for Statistical Computing, Vienna, Austria). Statistical significance was defined as two-sided p<0.05.
Figure 1. Time course of the study participants
Results
Participants
A total of 261 patients were enrolled in this study, and 252 were analyzed. Among these patients, 181 were re-corded as having CAD, 95 as having PAD, and 24 with both CAD and PAD. The remaining nine patients were excluded because follow-up was impossible even via telephone inter-view.Figure 1 shows the flowchart of the enrolled patients.
Table 1 indicates the baseline characteristics of partici-pants. Mean age was 71.0 years, and male patients ac-counted for 76.6%. More than half of the patients had hy-pertension (HT), dyslipidemia (DL) and diabetes mellitus (DM). Approximately 30% of patients had chronic kidney disease (CKD), of which 66.2% were undergoing hemo-dialysis (HD). Almost all patients were receiving antiplatelet therapy (98.4%). ARBs and calcium channel blockers (CCBs) were mainly prescribed for HT treatment (51.2%). Beta-blockers were used for HT, AP, and heart rate control (45.6%). Statins were mainly used to treat DL (74.6%). The average serum creatinine was relatively high because pa-tients with HD were included (20.2%).
Our observation period was an average of 946.2 days in patients with CAD and 904.8 days in patients with PAD as for MACE, and an average of 1093.9 days and 1097.4 days for cardiovascular death in CAD and PAD including ampu-tation, respectively (Supplementary Figure 1).
Outcomes
MACE occurred in 38 and 23 patients in each group. Ta-ble 2 shows the detailed composition of these patients.
Supplementary Figures 1(a) and 2(c) show MACE-free survival curves in patients with CAD and PAD. Cumu-lative survival rates were 0.701±0.048 and 0.705±0.054, re-spectively. Supplementary figures 1 (b) and 2 (d) reveal car-diovascular death in patients with CAD and PAD including amputation. Cumulative survival rates were 0.909±0.035 and
0.882±0.069, respectively.
Supplementary Table 1 exhibits the effect of CAD prevention in terms of age, sex, and BMI matched using the IPTW method. Statins are only effective as a single-medicine therapy for MACEs (Odds ratio [OR], 0.280; 95% confidence interval [CI], 0.118-0.660, P=0.004), antiplatelet drugs (OR, 0.031; 95% CI, 0.002-0.550; P=0.018), and CCBs (OR, 0.095; 95% CI, 0.011-0.783; P=0.029) and are effective for cardiovascular death in patients with CAD. Fur-thermore, we found that the triple combination therapy (anti-platelet therapies, statins, and CCBs) is the best combination for MACE (OR, 0.333; 95% CI, 0.136-0.815; P=0.016) and cardiovascular death (OR, 0.031; 95% CI, 0.002-0.520; P= 0.001). On the other hand, we found that antiplatelet drugs, statins, and beta-blockers, which are the traditionally recog-nized OMT, are not significantly effective to prevent MACE (OR, 0.720; 95% CI, 0.347-1.493; P=0.377) and cardiovas-cular death (OR, 0.936; 95% CI, 0.243-3.608; P=0.924). These results did not change when multivariable models were adjusted with the IPTW method for MACE (OR, 0.259; 95% CI, 0.095-0.707; P=0.008) and cardiovascular death (OR, 0.040; 95% CI, 0.002-0.681; P=0.001) as shown in Table 3. However, in patients with PAD, there were no significantly effective combinations for MACE, as is shown inSupplementary Table 2.
We considered the efficiency including survival time, and we performed Cox hazards model analysis. The results were almost the same with logistic regression analysis as is shown in Supplementary Table 3. Antiplatelet drugs (Hazard ratio [HR], 0.597; 95% CI, 0.389-0.917; P=0.008) and statins (HR, 0.344; 95% CI, 0.176-0.674; P=0.014) were good for MACE prevention, and additional CCB com-bination was effective for MACE (HR, 0.365; 95% CI, 0.159-0.835; P=0.008) and cardiovascular death (HR, 0.000; 95% CI, 0.000-0.000; P=0.004). These results did not change when multivariable models were adjusted with the IPTW method for MACE (HR, 0.263; 95% CI, 0.097-0.710; P=0.007) and cardiovascular death (HR, 0.000; 95% CI,
Table 1. Baseline characteristics of this study. HDL-C, high-density lipoprotein
cholesterol; LDL-C, low-density lipoprotein cholesterol; UA, uric acid; eGFR, esti-mated glomerular fi ltration ratio; HbA1c, hemoglobin A1c; CRP, C-reactive protein; Hb, hemoglobin; PT-INR, international normalized ratio of prothrombin time; APTT, activated partial thromboplastin time, ARB, angiotensin II receptor blocker; ACEI, angiotensin converting enzyme inhibitor; CCB, calcium channel blocker; EPA, eicosapentaenoic acid; SAB, selective angiotensin blocker; PPI, proton pump inhibi-tor
CAD (n=181) PAD (n=95) All (n=252) Age (y.o.) 70.8±0.8 71.8±1.0 71.0±0.6 Male (%) 143 (79.0%) 71 (74.7%) 193 (76.6%) Body Mass Index (kg/m2) 24.8±1.5 22.4±0.4 24.1±1.1 Current Smoker 20 (11.1%) 14 (14.7%) 31 (12.3%) Systolic Blood Pressure (mmHg) 130.4±1.4 133.6±2.0 130.5±1.2 Diastolic Blood Pressure (mmHg) 71.0±1.0 69.1±1.4 70.2±0.9
Past History Hypertension (%) 132 (72.9%) 74 (77.9%) 185 (73.4%) Dyslipidemia (%) 108 (59.7%) 42 (44.2%) 137 (54.4%) Diabetic Mellitus (%) 82 (45.3%) 54 (56.8%) 119 (47.2%) Atrial Fibrillation (%) 22 (12.2%) 13 (13.7%) 32 (12.7%) Stroke (%) 33 (18.2%) 21 (22.1%) 44 (17.5%) Chronic Kidney Disease (%) 52 (28.7%) 34 (35.8%) 77 (30.6%) Hemodialysis (%) 30 (16.6%) 30 (31.6%) 51 (20.2%) NYHA (%) I: 123 (68.0%) - -II: 47 (26.0%) III: 11 (6.0%) Fontaine (%) - II: 53 (55.8%) -III: 16 (16.8%) IV: 26 (27.4%) Blood Test HDL-C (mg/dL) 51.0±1.1 54.6±2.0 52.4±1.1 LDL-C (mg/dL) 89.8±2.1 89.6±2.9 90.3±1.7 Triglyceride (mg/dL) 124.9±5.6 126.9±6.3 124.8±4.5 UA (mg/dL) 5.6±0.1 5.2±0.2 5.4±0.1 eGFR (mL/min/1.73 m2) 53.2±2.2 51.2±3.8 53.4±2.0 Glucose (mg/dL) 132.1±3.1 141.1±5.9 133.8±3.0 HbA1c (%) 6.3±0.1 6.3±0.1 6.3±0.1 CRP (mg/dL) 0.71±0.09 1.14±0.22 0.89±0.10 Hb (g/dL) 11.7±0.1 11.3±0.2 11.5±0.1 PT-INR 1.06±0.01 1.06±0.02 1.06±0.01 APTT (sec) 34.4±0.7 35.1±1.7 35.0±0.8 D-dimer (mg/dL) 2.3±0.4 2.4±0.4 2.4±0.3 Medication Antiplatelet agent (%) 179 (98.9%) 93 (97.9%) 248 (98.4%) Anticoagulant therapy (%) 15 (8.3%) 8 (8.4%) 23 (9.1%) ARB (%) 79 (43.6%) 49 (51.6%) 111 (44.0%) ACE-I (%) 40 (22.1%) 7 (7.4%) 45 (17.9%) CCB (%) 92 (50.8%) 53 (55.8%) 129 (51.2%) Alpha-blocker (%) 12 (4.8%) 4 (4.2%) 12 (4.8%) Beta-blocker (%) 99 (54.7%) 26 (27.4%) 115 (45.6%) Statin (%) 141 (77.9%) 62 (65.3%) 188 (74.6%) EPA (%) 16 (8.8%) 10 (10.5%) 22 (8.7%) Fibrate (%) 1 (0.6%) 1 (1.1%) 1 (0.4%) Ezetimibe (%) 15 (8.3%) 3 (3.2%) 16 (6.3%) Diuretic (%) 48 (26.5%) 17 (17.9%) 59 (23.4%) SAB (%) 3 (1.7%) 0 (0.0%) 3 (1.2%) Nitrate (%) 81 (44.8%) 17 (17.9%) 92 (36.5%) Oral antidiabetic therapy (%) 50 (27.6%) 29 (30.5%) 68 (27.0%) Insulin (%) 22 (12.1%) 13 (13.7%) 31 (12.3%) PPI (%) 121 (66.9%) 55 (57.9%) 164 (65.1%) H2 blocker (%) 23 (12.7%) 11 (11.6%) 30 (11.9%)
Table 2. Detailed distributions of MACE in all participants CAD (n=181) PAD (n=95) All (n=252) MACE (%) 38 (21.0%) 23 (24.2%) 61 (24.2%) Cardiovascular death (%) 9 (5.0%) 1 (1.1%) 10 (4.0%) Amputation (%) 0 (0.0%) 4 (4.2%) 4 (1.6%) Non-fatal AMI (%) 3 (1.7%) 0 (0.0%) 3 (1.2%) Non-fatal UAP (%) 5 (2.8%) 0 (0.0%) 5 (2.0%) Non-fatal CHF (%) 3 (1.7%) 0 (0.0%) 3 (1.2%) Non-fatal Stroke (%) 2 (1.1%) 1 (1.1%) 3 (1.2%) Revascularization (%) 16 (8.8%) 22 (23.1%) 38 (15.1%)
Table 3. Effectiveness of single, double, and triple therapies in patients with CAD. Performed matching with
multiple# factors using the IPTW method. * p<0.05 # Age, sex, BMI, systolic blood pressure, triglyceride, HDL-C,
LDL-C, HbA1c, CRP, eGFR, UA, d-dimer, and Hb
Medicines MACE Cardiovascular death OR CI (95%) p OR CI (95%) p Single Antiplatelet agent 0.175 0.011-2.870 0.222 0.031 0.002-0.550 0.018*
Anticoagulant therapy 2.584 0.739-9.030 0.137 5.152 0.801-33.14 0.084 ARB 1.578 0.766-3.250 0.216 0.156 0.019-1.277 0.083 ACE-I 1.047 0.444-2.467 0.917 0.876 0.172-4.464 0.874 CCB 0.992 0.472-2.086 0.992 0.095 0.011-0.783 0.029* Beta-blocker 0.995 0.484-2.044 0.988 1.609 0.389-6.654 0.511 Statin 0.280 0.118-0.660 0.004* 0.632 0.131-3.055 0.568 Double Antiplatelet agent+ARB 1.578 0.766-3.250 0.216 0.156 0.019-1.277 0.083 Antiplatelet agent+CCB 0.992 0.472-2.086 0.984 0.095 0.011-0.783 0.029* Antiplatelet agent+Statin 0.280 0.118-0.660 0.004* 0.632 0.131-3.055 0.568 CCB+Statin 0.333 0.136-0.815 0.016* 0.031 0.002-0.520 0.001* Triple Antiplatelet agent+CCB+Statin 0.333 0.136-0.815 0.016* 0.031 0.002-0.520 0.001* Antiplatelet agent+Beta-blocker+Statin 0.720 0.347-1.493 0.377 0.936 0.243-3.608 0.924
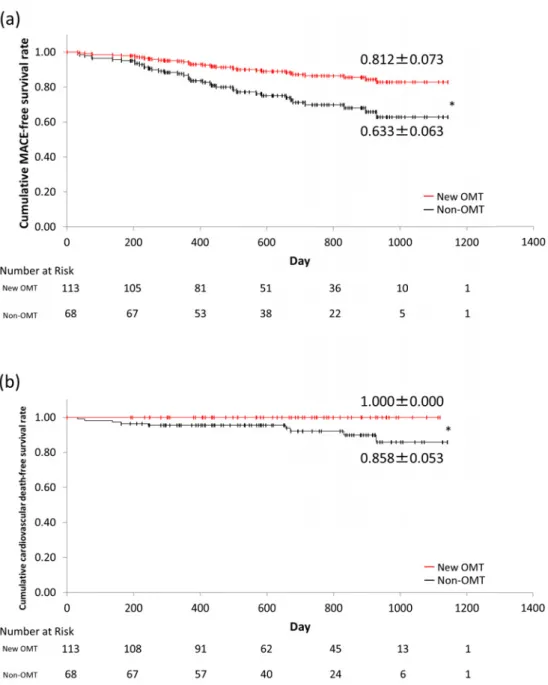
0.000-0.000; P=0.006) as shown in Table 4. Figure 2 shows the benefit of the new OMT (antiplatelet drugs, statins, and CCBs). There are significant effects for both MACE (0.812±0.073 vs. 0.633±0.063, P=0.017) and cardio-vascular death (1.000±0.000 vs. 0.858±0.053, P=0.020) in patients with CAD.
Discussions
The primary novel findings of the present study are that the combination of medicines, antiplatelet agents, statins, and CCBs, is significantly associated with better prognosis for MACE including cardiovascular death in Japanese pa-tients with stable CAD. These findings underlined the clini-cal importance of routine combinations in the management of patients with stable CAD.
Based on the COURAGE trial3) and associated trials16), we had to study the effect of OMT for secondary CAD preven-tion despite the improvement in the catheter intervenpreven-tion technology. Additionally, another study reported that there was no significant difference between the OMT and PCI+ OMT groups17); OMT in this study included antiplatelet drugs, statins, and beta-blockers18)
. Many studies were
con-ducted and had reported that single medication had a signifi-cant benefit in preventing secondary events. However, only a few studies used multi-drug regimen for prevention because it requires much time, significant cost, and might have con-flicting ethical concerns. Thus, we conducted the current analyses using PS matching with the IPTW method to avoid these difficulties and various confounding factors. We found that CCB plays an important role for the secondary preven-tion in Japanese patients with CAD. On the other hand, we could not currently find any beneficial effects of beta-blockers and ACE-I or ARB. This is similar to some previ-ous reports, in which investigators found no significant ef-fect of multi-drug regimen for secondary prevention without heart failure19,20).
In the present study, we could not find any benefits of beta-blockers for secondary prevention. Our analyses cannot prove the causes of this ineffectiveness, but we consider sev-eral reasons. Vascular spastic angina (VSA) is conceivable as one of the possibilities. It was reported that the VSA rate is higher in Japan than in other foreign countries21,22)
, and beta-blockers are not effective due to the risk of additional myocardial infarction according to the JBCMI study23). In addition, 69% of Japanese patients with AMI were positive
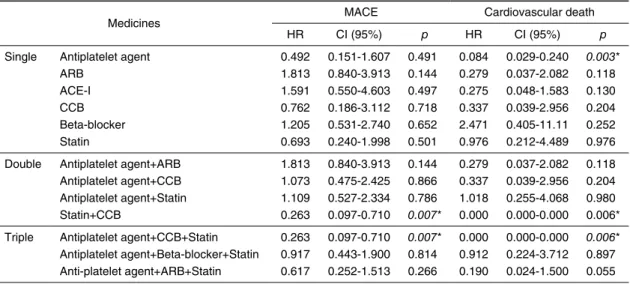
Table 4. Effectiveness of single, double, and triple therapies in patients with CAD. Performed matching with
multiple# factors using the IPTW method. * p<0.05. # Age, sex, BMI, systolic blood pressure, triglyceride, HDL-C,
LDL-C, HbA1c, CRP, eGFR, UA, d-dimer, and Hb
Medicines MACE Cardiovascular death HR CI (95%) p HR CI (95%) p
Single Antiplatelet agent 0.492 0.151-1.607 0.491 0.084 0.029-0.240 0.003* ARB 1.813 0.840-3.913 0.144 0.279 0.037-2.082 0.118 ACE-I 1.591 0.550-4.603 0.497 0.275 0.048-1.583 0.130 CCB 0.762 0.186-3.112 0.718 0.337 0.039-2.956 0.204 Beta-blocker 1.205 0.531-2.740 0.652 2.471 0.405-11.11 0.252 Statin 0.693 0.240-1.998 0.501 0.976 0.212-4.489 0.976 Double Antiplatelet agent+ARB 1.813 0.840-3.913 0.144 0.279 0.037-2.082 0.118 Antiplatelet agent+CCB 1.073 0.475-2.425 0.866 0.337 0.039-2.956 0.204 Antiplatelet agent+Statin 1.109 0.527-2.334 0.786 1.018 0.255-4.068 0.980 Statin+CCB 0.263 0.097-0.710 0.007* 0.000 0.000-0.000 0.006* Triple Antiplatelet agent+CCB+Statin 0.263 0.097-0.710 0.007* 0.000 0.000-0.000 0.006*
Antiplatelet agent+Beta-blocker+Statin 0.917 0.443-1.900 0.814 0.912 0.224-3.712 0.897 Anti-platelet agent+ARB+Statin 0.617 0.252-1.513 0.266 0.190 0.024-1.500 0.055
in coronary spasm-induced examination in the earlier stage24)
. No patients were diagnosed as VSA during enroll-ment and observation period. However, two patients with AMI (66.7%) were prescribed with beta-blockers. We cannot completely contradict that they had any contribution in in-ducing AMI. Further, as another possibility, the dose of beta-blockers is believed not to affect the efficiency. In the Multicenter Carvedilol Heart Failure Dose Assessment (MUCHA) trial and Japanese Chronic Heart Failure (J-CHF) study, carvedilol had dose-response effect in patients with chronic HF25,26). We examined the factors influencing this and checked the kinds and doses of drugs, and used a relative score that was calculated according to the amount of stan-dard medicine dosage per number of patients. We found that the dose of beta-blockers is significantly small for AP treat-ment (Suppletreat-mentary Table 4). In addition, evidences about beta-blockers in CAD were reported, especially in pa-tients with reduced left ventricular ejection fraction27)
or mild to severe HF26,28). Without those conditions, the effect of beta-blockers is limited in the acute phase29)
, and there are few studies in the chronic phase. Focusing on our cohort, 123 patients (68.0%) with CAD were New York Heart Asso-ciation (NYHA) Class I, and beta-blockers are not that strong to influence the long-term event-free survival. There-fore, we consider that beta-blockers have no significant ef-fect for the secondary prevention in patients with CAD.
CCBs, especially dihydropyridines, were not considered effective for secondary prevention in the mid-1990s30)
. It was believed that CCBs, especially short-acting CCBs, upon the induction of myocardial ischemia due to the sympathetic nerve activation, thereby resulting in tachycardia and hy-potension, might not be effective for secondary prevention. However, at present, long-acting CCBs show beneficial ef-fects for this purpose31), and diltiazem or verapamil are also considered beneficial32) in controlling the heart rate. In Ja-pan, CCBs are reported to be similar to beta-blockers for
their effects on secondary prevention33). In the current study, CCBs are also effective for MACE prevention in patients with CAD, but its mechanism in reducing events remains uncertain. As CCBs are approved for the treatment of angina due to blood vessel dilatation, a reduction in ischemic chest pain may prevent hospitalization and subsequent revasculari-zation procedures. Alternatively, blood pressure depression may have contributed to a relative risk reduction for MACE because CCB treatment significantly slowed atherosclerosis progression with intravascular ultrasound (IVUS) in patients with high systolic blood pressure34).
At present, we could not find any combination of medi-cine effective for MACE including amputation free survival in patients with PAD. As seen in the Framingham Heart Study, there were treatable risk factors, especially, HT, DL, DM, and smoking35). Controlling these risk factors was im-portant, although there are few studies to extend prognosis. Only statins has the effect of cardiovascular event reduction in specific patients with PAD13). Since PAD is a result of polyvascular disease, we set MACE as the primary outcome. However, we found no significant effects when the effect of OMT was examined in current populations. It was believed that there are two reasons to support our results. First, we chose patients with PAD who underwent EVT; therefore, it seemed that the severity of atherosclerosis was high and be-yond control using medication, which is sufficient to prevent subsequent cardiovascular events. Second, some patients were undergoing HD due to end-stage renal disease. As they started receiving HD, the blood vessels become impaired earlier because of enhanced arterial calcification due to CKD-MBD36)
, and controlling multiple complications with limited medications seemed to be difficult.
Our study has several limitations. First, the number of participants was relatively small. We used the IPTW method to avoid various factors confounding for our cohorts, and backgrounds of patients were statistically adjusted well.
Figure 2. Difference between the new OMT and non-OMT groups in (a) MACE and (b)
cardio-vascular death in patients with CAD. *p<0.05
Then, the statistical power for MACE was enough for CAD (beta=0.999), but not enough for PAD (beta=0.298). Second, as this study was essentially a retrospective cohort study, de-spite being statistically appropriate and sophisticated as the quasi-randomized cohort study design, we could not control the loading of the new medicine or dose despite the effects of intervention to be considered as intention-to-treat. How-ever, the subjects with stable CAD were those with one or more PCI during study periods and without PCI due to the lack of medical indication, detailed procedures including tar-get region characteristics, PCI devices and ischemic condi-tions might have an impact on cardiovascular outcome. This should be reviewed and analyzed in other fashion; however, our analyses effectively showed the significant prognostic values of multiple regimens for the subjects with stable CAD regardless of detailed target lesion characteristics.
Conclusions
In conclusion, we found traditional OMT unsuitable for secondary prevention in Japanese patients. We proposed that the current OMT (antiplatelet agents, statins, and CCBs) has significant effects for secondary prevention in patients with CAD through our current clinical test. We performed statisti-cally proven quasi-RCT using the PS matching and IPTW techniques, because testing multiple combinations in the ac-tual prospective clinical trials are unrealistically impossible to be planned in the actual clinical settings. Therefore, this statistically sophisticated technique should enable us to re-solve these kinds of clinical research questions without huge financial burdens and personnel costs. Clinical practice guidelines for stable CAD in Japan had been revised in 2019, and OMT for stable CAD is becoming one of the po-tent options that clinicians should consider for the subjects.
Our results might provide scientific evidences for effective cardiovascular protection of the subjects with CAD in Japan.
Abbreviations
ACE-I: angiotensin converting enzyme inhibitor, AMI: acute myocardial infarction, ARB: angiotensin receptor blocker, ASO: arteriosclerosis obliterans, BMI: body mass index, CAD: coronary artery disease, CCB: calcium channel blocker, CKD: chronic kidney disease, CKD-MBD: chronic kidney disease mineral and bone disorder, COURAGE: Clinical Outcomes Utilizing Revascularization and Aggres-sive Drug Evaluation, CRP: C-reactive protein, DL: dyslipi-demia, DM: diabetes mellitus, eGFR: estimated glomerular filtration ratio, EVT: endovascular treatment, Hb: hemoglo-bin, HbA1c: hemoglobin A1c, HD: hemodialysis, HDL-C: high-density lipoprotein cholesterol, LDL-C: low-density lipoprotein cholesterol, HF: heart failure, HR: hazard ratio, HT: hypertension, IPTW: inverse probability of treatment-weighted, IVUS: intravascular ultrasound, JBCMI: Japanese β-blockers and Calcium Antagonists Myocardial Infarction, J-CHF: Japanese Chronic Heart Failure, MACE: major com-posite adverse cardiac event, MUCHA: Multicenter Carve-dilol Heart Failure Dose Assessment, NYHA: New York Heart Association, OMT: optimal medical therapy, OR: odds ratio, PAD: peripheral artery disease, PCI: percutaneous coronary intervention, PS: propensity score, quasi-RCT: quasi-randomized control trial, UA: uric acid, UAP: unstable angina pectoris, VSA: vascular spastic angina
Declarations
Ethics approval and consent to participate
The study protocol was registered and approved by the Ethical Committee of the Yokohama City University Hospi-tal (UMIN000035665, R000040627), with notification for guaranteed withdrawal of participants on the website provid-ing means of “opt-out,” and because of the noninvasive ob-servational study design, additional informed consent was not obtained from the participants.
Consent for publication
In submitting our manuscript to the Vascular Failure, we confirm that it has not been published or presented else-where, in part or in entirety, and is not under consideration by another journal. The manuscript meets the authorship and ethical guidelines for publication in the Vascular Failure. We have read and understood your journal’s policies, and we believe that neither the manuscript nor the study violates any of these. All authors accept the ethical responsibility of publishing these data.
Availability of data and material None.
Research Funding
T.I. is supported by a Grant-in-Aid for Scientific Research from the Ministry of Education, Culture, Sports, Science, and Technology (MEXT) no. 17K09730, by Life Innovation Platform YOKOHAMA (LIP. Yokohama) from Economic Affairs Bureau City of Yokohama and Yokohama Foundation for Advancement of Medical Science. The funders had no role in study design, data collection and analysis, decision to publish, or manuscript preparation.
Competing Interests
The authors declare that they have no competing interests. Author Contributions
T.K. performed collection of dataset, statistical analyses, and table and figure preparations. T.I. supervised research scope, wrote a paper, and helped in the statistical analyses. H.D., L.C. R.NS., M.S., K.A., S.M., K.A., H.W., K.A., and K.T. helped in the dataset collection and acquisition of in-formed consent.
Acknowledgement
We appreciated all the parties involved in this study for the fulfillment of quasi-RCT by multiple regimens for the subjects with CAD and PAD in Japan.
Conflicts of Interest None
References
1. Hansson GK, Libby P. The immune response in atherosclerosis: a double-edged sword. Nature Reviews Immunology 2006; 6: 508-19.
2. Falk E, Shah PK, Fuster V. Coronary plaque disruption. Circula-tion 1995; 92: 657-71.
3. Boden WE, O’Rourke RA, Teo KK, Hartigan PM, Maron DJ, Kostuk WJ, et al. Optimal medical therapy with or without PCI for stable coronary disease. The New England Journal of Medicine 2007; 356: 1503-16.
4. Weintraub WS, Spertus JA, Kolm P, Maron DJ, Zhang Z, Jurk-ovitz C, et al. Effect of PCI on quality of life in patients with sta-ble coronary disease. The New England Journal of Medicine 2008; 359: 677-87.
5. Smith SC, Jr., Allen J, Blair SN, Bonow RO, Brass LM, Fonarow GC, et al. AHA/ACC guidelines for secondary prevention for pa-tients with coronary and other atherosclerotic vascular disease: 2006 update: endorsed by the National Heart, Lung, and Blood In-stitute. Circulation 2006; 113: 2363-72.
6. Yasue H, Ogawa H, Tanaka H, Miyazaki S, Hattori R, Saito M, et al. Effects of aspirin and trapidil on cardiovascular events after acute myocardial infarction. Japanese Antiplatelets Myocardial In-farction Study (JAMIS) Investigators. The American Journal of Cardiology 1999; 83: 1308-13.
7. Furuta H, Kimura A, Miyataka M, Taniguchi M, Katayama K, Yamamoto T, et al. Pravastatin reduces the incidence of cardiac events among patients with myocardial infarction. Japanese Heart Journal 2003; 44: 873-87.
8. Kohro T, Hayashi D, Okada Y, Yamazaki T, Nagai R, Investigators J. Effects of medication on cardiovascular events in the Japanese
coronary artery disease (JCAD) study. Circulation Journal 2007; 71: 1835-40.
9. Pfeffer MA, McMurray JJ, Velazquez EJ, Rouleau JL, Kober L, Maggioni AP, et al. Valsartan, captopril, or both in myocardial in-farction complicated by heart failure, left ventricular dysfunction, or both. The New England Journal of Medicine 2003; 349: 1893-906.
10. Dawson DL, Cutler BS, Meissner MH, Strandness DE, Jr. Cilosta-zol has beneficial effects in treatment of intermittent claudication: results from a multicenter, randomized, prospective, double-blind trial. Circulation 1998; 98: 678-86.
11. Lièvre M, Morand S, Besse B, Fiessinger JN, Boissel JP. Oral Beraprost sodium, a prostaglandin I(2) analogue, for intermittent claudication: a double-blind, randomized, multicenter controlled trial. Beraprost et Claudication Intermittente (BERCI) Research Group. Circulation 2000; 102: 426-31.
12. Randomized trial of the effects of cholesterol-lowering with sim-vastatin on peripheral vascular and other major vascular outcomes in 20,536 people with peripheral arterial disease and other high-risk conditions. Journal of Vascular Surgery 2007; 45: 645-654; discussion 53-54.
13. Schillinger M, Exner M, Mlekusch W, Amighi J, Sabeti S, Muell-ner M, et al. Statin therapy improves cardiovascular outcome of patients with peripheral artery disease. European Heart Journal 2004; 25: 742-8.
14. McCaffrey DF, Griffin BA, Almirall D, Slaughter ME, Ramchand R, Burgette LF. A tutorial on propensity score estimation for mul-tiple treatments using generalized boosted models. Statistics in Medicine 2013; 32: 3388-414.
15. Austin PC. The performance of different propensity score methods for estimating marginal hazard ratios. Statistics in Medicine 2013; 32: 2837-49.
16. Sedlis SP, Hartigan PM, Teo KK, Maron DJ, Spertus JA, Mancini GB, et al. Effect of PCI on Long-Term Survival in Patients with Stable Ischemic Heart Disease. The New England Journal of Medicine 2015; 373: 1937-46.
17. Henderson RA, Pocock SJ, Clayton TC, Knight R, Fox KAA, Jul-ian DG, et al. Seven-year outcome in the RITA-2 trial: coronary angioplasty versus medical therapy. Journal of the American Col-lege of Cardiology 2003; 42: 1161-70.
18. Borden WB, Redberg RF, Mushlin AI, Dai D, Kaltenbach LA, Spertus JA. Patterns and intensity of medical therapy in patients undergoing percutaneous coronary intervention. JAMA 2011; 305: 1882-9.
19. Bangalore S, Fakheri R, Wandel S, Toklu B, Wandel J, Messerli FH. Renin angiotensin system inhibitors for patients with stable coronary artery disease without heart failure: systematic review and meta-analysis of randomized trials. BMJ (Clinical research ed) 2017; 356: j4.
20. Schmidt M, Mansfield KE, Bhaskaran K, Nitsch D, Sørensen HT, Smeeth L, et al. Serum creatinine elevation after renin-angiotensin system blockade and long term cardiorenal risks: cohort study. BMJ (Clinical research ed) 2017; j791.
21. Wakabayashi K, Suzuki H, Honda Y, Wakatsuki D, Kawachi K, Ota K, et al. Provoked coronary spasm predicts adverse outcome in patients with acute myocardial infarction: a novel predictor of prognosis after acute myocardial infarction. Journal of the Ameri-can College of Cardiology 2008; 52: 518-22.
22. Pristipino C, Beltrame JF, Finocchiaro ML, Hattori R, Fujita M, Mongiardo R, et al. Major racial differences in coronary constric-tor response between japanese and caucasians with recent myocar-dial infarction. Circulation 2000; 101: 1102-8.
23. Japanese b-B, Calcium Antagonists Myocardial Infarction I.
Com-parison of the effects of beta blockers and calcium antagonists on cardiovascular events after acute myocardial infarction in Japanese subjects. The American Journal of Cardiology 2004; 93: 969-73. 24. Okumura K, Yasue H, Matsuyama K, Ogawa H, Morikami Y,
Obata K, et al. Effect of acetylcholine on the highly stenotic coro-nary artery: difference between the constrictor response of the infarct-related coronary artery and that of the noninfarct-related ar-tery. Journal of the American College of Cardiology 1992; 19: 752-8.
25. Hori M, Sasayama S, Kitabatake A, Toyo-oka T, Handa S, Yoko-yama M, et al. Low-dose carvedilol improves left ventricular func-tion and reduces cardiovascular hospitalizafunc-tion in Japanese patients with chronic heart failure: the Multicenter Carvedilol Heart Failure Dose Assessment (MUCHA) trial. American Heart Journal 2004; 147: 324-30.
26. Okamoto H, Hori M, Matsuzaki M, Tsutsui H, Yamazaki T, Nagai R, et al. Minimal dose for effective clinical outcome and predic-tive factors for responsiveness to carvedilol: Japanese chronic heart failure (J-CHF) study. International Journal of Cardiology 2013; 164: 238-44.
27. Dargie HJ. Effect of carvedilol on outcome after myocardial in-farction in patients with left-ventricular dysfunction: the CAPRI-CORN randomised trial. Lancet (London, England) 2001; 357: 1385-90.
28. Packer M, Coats AJ, Fowler MB, Katus HA, Krum H, Mohacsi P, et al. Effect of carvedilol on survival in severe chronic heart fail-ure. The New England journal of medicine 2001; 344: 1651-8. 29. Puymirat E, Riant E, Aissaoui N, Soria A, Ducrocq G, Coste P, et
al. beta blockers and mortality after myocardial infarction in pa-tients without heart failure: multicentre prospective cohort study. BMJ (Clinical research ed) 2016; 354: i4801.
30. Psaty BM, Heckbert SR, Koepsell TD, Siscovick DS, Raghu-nathan TE, Weiss NS, et al. The risk of myocardial infarction as-sociated with antihypertensive drug therapies. JAMA 1995; 274: 620-5.
31. Jamerson K, Weber MA, Bakris GL, Dahlof B, Pitt B, Shi V, et al. Benazepril plus amlodipine or hydrochlorothiazide for hyperten-sion in high-risk patients. The New England Journal of Medicine 2008; 359: 2417-28.
32. Bangalore S, Messerli FH, Cohen JD, Bacher PH, Sleight P, Man-cia G, et al. Verapamil-sustained release-based treatment strategy is equivalent to atenolol-based treatment strategy at reducing car-diovascular events in patients with prior myocardial infarction: an INternational VErapamil SR-Trandolapril (INVEST) substudy. American Heart Journal 2008; 156: 241-7.
33. Nakagomi A, Kodani E, Takano H, Uchida T, Sato N, Ibuki C, et al. Secondary Preventive Effects of a Calcium Antagonist for Ischemic Heart Attack. Circulation Journal 2011; 75: 1696-705. 34. Nissen SE, Tuzcu EM, Libby P, Thompson PD, Ghali M, Garza
D, et al. Effect of antihypertensive agents on cardiovascular events in patients with coronary disease and normal blood pressure: the CAMELOT study: a randomized controlled trial. JAMA 2004; 292: 2217-25.
35. Fowkes FGR, Rudan D, Rudan I, Aboyans V, Denenberg JO, McDermott MM, et al. Comparison of global estimates of preva-lence and risk factors for peripheral artery disease in 2000 and 2010: a systematic review and analysis. The Lancet 2013; 382: 1329-40.
36. Moe S, Drueke T, Cunningham J, Goodman W, Martin K, Olgaard K, et al. Definition, evaluation, and classification of renal osteo-dystrophy: a position statement from Kidney Disease: Improving Global Outcomes (KDIGO). Kidney International 2006; 69: 1945-53.