第93回日本感染症学会総会・学術講演会座長推薦演題
Tm mapping 法が迅速診断に有用であった脳膿瘍の小児例
1)埼玉県立小児医療センター感染免疫・アレルギー科,2)富山大学臨床分子病態検査学講座,
3)埼玉県立小児医療センター脳神経外科
上島 洋二
1)2)栗原 淳
3)古市美穂子
1)佐藤 智
1)仁井見英樹
2)川野 豊
1)大石 勉
1)菅沼 栄介
1)(令和元年9月6日受付)
(令和2年1月29日受理)
Key words : brain abscess, melting temperature mapping method,Streptococcus intermedius
序 文
2018
年に「多項目遺伝子関連検査の実施指針」が 示され,臨床応用が進められてきている.早期に原因 菌が特定されれば,抗菌薬の適正使用につながること が期待される.
melting temperature mapping method(以下,Tm mapping 法)は,16S rRNA 遺伝子(16
S rDNA)を用いた新たな迅速原因菌同定法であり,培養液を用いずに検体採取から最短
3時間で原因菌を 同定することができる
1).今回,我々は
Tm mapping法により,脳膿瘍の排膿液から
Streptococcus interme- diusを迅速同定し,経験的治療を支持することができ た脳膿瘍の男児例を報告する.
症 例
患者は
11歳の男児で,乳児期に他院で両大血管右 室起始症,肺動脈狭窄症,総肺静脈還流異常症に対し
て
Fontan手術(右左短絡作成)を施行され,その後
も他院で術後管理を行われていた.無脾症を指摘され ていたが予防的抗菌薬の内服は行われていなかった.
予防接種歴は,Hib ワクチンは未接種で,7 価肺炎球 菌結合型ワクチンを
1回,3 種混合ワクチン,日本脳 炎ワクチンを各々
3回,
MRワクチン,水痘ワクチン,
ポリオ生ワクチンを各々
2回,BCG を接種済であっ た.X−18 日に頭痛のため近医を受診し鎮痛薬を処方 されたが改善せず,X−4 日に頭痛が増悪したため
X日に前医を再診した.頭部
CTで脳腫瘍を疑われ当院 へ紹介受診した.
入 院 時 体 温
36.3℃,血 圧86/42mmHg,心 拍 数80回/分,呼吸数
20回/分,意識清明.神経学的に異常 所見は認められなかった.血液検査では,
WBC 11,900/μL(Band 2%,Seg 64%),CRP 0.82mg/dL
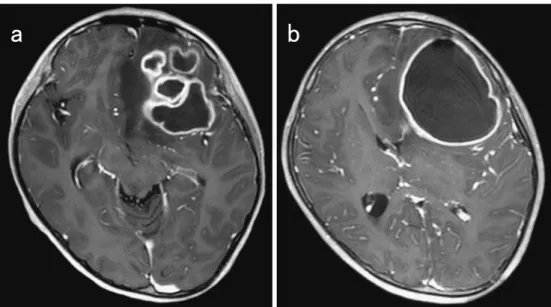
と炎症 反応の上昇を認めた.頭部造影
MRIで左前頭葉に,周 囲に造影効果のある被膜様構造を有する多房性腫瘤
(57mm×54mm)を認めた(Fig. 1a).画像所見より 脳膿瘍と考え,入院
4日目に術前抗菌薬としてセファ ゾリンを投与後に脳膿瘍排膿ドレナージ術を行った.
排膿液の性状は黄緑色膿性,異臭を伴い,グラム染色 では連鎖状のグラム陽性球菌が認められた.入院時に 採取されていた血液培養は
2セットとも陰性であっ た.手術直後からセフォタキシム(CTX)
300mg/kg/day
とメトロニダゾール(MNZ)40mg/kg/day を開 始した.排膿液を用いて当院で
melting temperature mapping法(以下,Tm mapping 法)を行い,排膿 液採取後,4 時間半後に
S. intermediusを同定した.心 臓超音波検査では疣贅や血栓などは認められなかった が,耳鼻科医,歯科医の診察により,副鼻腔炎,齲歯 を指摘された.術後
4日目に排膿液の培養検査からコ ロ ニ ー が 得 ら れ た た め 当 院 で
MALDI Biotyper(Bruker Japan)による質量分析法で,同じ
S. interme- diusが
Score Value 2.26(Score Value 2.0以上は菌種 レベルの一致,Score Value 1.7 以上
2.0未満は属レベ ルの一致,Score Value 1.7 未満 は分類不能)で同定 された.また,生化学的性状を調べる
API 20 Strep(bioMérieux)で も
S. intermediusと 同 定 さ れ た.排 膿後に頭痛は軽快し
WBC,CRPは低下したが,徐々 に頭痛が増悪し,入院
15日目の
MRIで膿瘍が拡大し ており(Fig. 1b),脳膿瘍摘出術を行った.頭痛は消
症 例別刷請求先:(〒330―8777)埼玉県さいたま市中央区新都心 1―2
埼玉県立小児医療センター感染免疫・アレル
ギー科 上島 洋二
Fig. 1 Enhanced MRI showing (a) multiple abscesses in the left frontal lobe of the brain upon admission and (b) a ring-enhancing developed lesion that caused a midline shift of the left frontal lobe to the right side of the brain 24 days after admission.
㼍 㼎
失し,CTX と
MNZを継続した.薬疹を疑う皮疹の 出現があり,抗菌薬は計
40日間で入院
43日目に終了 した.入院
49日目にアモキシシリン内服後に抜歯を 行い,同日退院した.術後
1年経過するが合併症や後 遺症はなく再燃を認めていない.
考 察
小児脳膿瘍は,4 人/100 万人程度と稀な疾患であ る
2).そのリスク因子として,未修復のチアノーゼ性 先天性心疾患,化膿性血栓性静脈炎や感染性心内膜炎 などの血行性因子が
30%,また,中耳炎や副鼻腔炎,齲歯,VP シャント感染などの脳の隣接部から直接波 及することが
40% 程度,原因不明が30% と考えられている
3).また,感染性心内膜炎の中枢神経合併症と して脳膿瘍を起こすことが知られている.本症例では,
先天性心疾患に対して
Fontan手術が行われ,右左短 絡が形成されていた.また,来院時に膿性鼻漏があり,
耳鼻咽喉科医の診察で急性副鼻腔炎を,歯科医により 齲歯を指摘されていたが,MRI では副鼻腔炎は右上 顎洞であり,上顎洞や齲歯に隣接した部位に骨髄炎な どはなかった.脳の隣接部から直接波及した可能性は 低いと考えられたため,血液培養は陰性であったもの の血行性に波及した可能性が考えられた.それぞれの リスク因子に対しては,心臓超音波検査で疣贅がない ことを確認し,歯科で口腔環境の保清と抜歯などの適 切な介入を行った.
S. intermedius
は
viridans streptococciの一種で,16
S rDNAの 系 統 解 析 で は
Streptococcus anginosus,Streptococcus constellatus,S. intermedius
の
3種類を含 む
anginosus groupに分類される
4).なかでも
S. inter-medius
は中枢神経感染症や肝膿瘍の起因菌となるこ
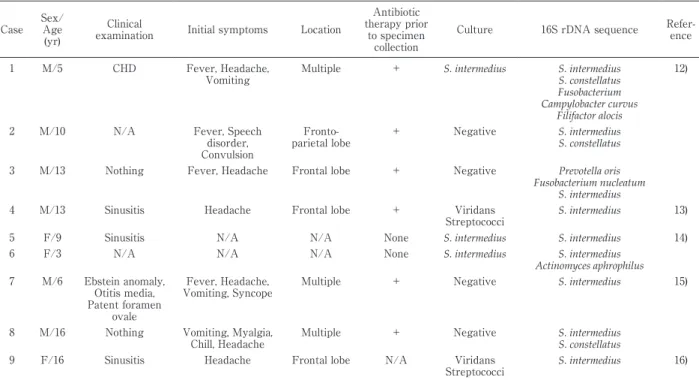
とが多い.PubMed で渉猟しえた範囲で,16S rDNA 系統解析で
S. intermediusが同定され原因菌として報 告された
16歳以下の小児脳膿瘍の過去の
9症例を
Tableに示す.9症例中
5症例では
S. intermedius以外 にも細菌が検出されており,単独感染よりもむしろ複 数菌の混合感染と考えられる症例のほうが多かった.
9症例中,6 症例では培養検査で
S. intermediusを検出 できなかった.一般細菌培養は先行抗菌薬の影響を受 けて偽陰性になることがある.このような場合でも
16S rDNA
であれば同定できる可能性がある.原因菌が
同定できないと,経験的治療で選択した広域抗菌薬を 治療終了まで継続せざるを得なくなり,抗菌薬適正使 用の観点からも好ましくない.先行して抗菌薬を投与 された脳膿瘍の症例では,培養検査よりも
16S rDNAを用いた検査は原因菌の同定に有用と思われる.
Tm mapping
法は
16S rDNAに対する
bacterial universal PCRを用いた細菌の迅速同定検査である
1). 先ず,全血やそのほかの臨床検体から
bacterial DNAを抽出する.次に
bacterial DNAの
contaminationが 皆無である
eukaryote-made Taq DNA polymeraseと
1つの
bacterial universal primer(全ての細菌をPCR検出するプライマー)を用いて
1st PCRを行い,そ の後に
7つの
bacterial universal primerを使用して
2nd nested PCRを行う.そして,得られた
7つの
PCR ampliconの
Tm値を測定し
2次元にマッピングし,
データベースに登録されている菌種と照合して細菌を
迅速同定する.同定結果の正確性は
Difference Value値を用いて評価する.Tm mapping 法の敗血症起炎
Table Case reports of brain abscesses with S. intermedius detected with the 16S rDNA sequence
Case Sex/
Age (yr)
Clinical
examination Initial symptoms Location
Antibiotic therapy prior
to specimen collection
Culture 16S rDNA sequence Refer- ence
1 M/5 CHD Fever, Headache,
Vomiting
Multiple + S. intermedius S. intermedius S. constellatus Fusobacterium Campylobacter curvus
Filifactor alocis
12)
2 M/10 N/A Fever, Speech
disorder, Convulsion
Fronto- parietal lobe
+ Negative S. intermedius
S. constellatus
3 M/13 Nothing Fever, Headache Frontal lobe + Negative Prevotella oris
Fusobacterium nucleatum S. intermedius
4 M/13 Sinusitis Headache Frontal lobe + Viridans
Streptococci
S. intermedius 13)
5 F/9 Sinusitis N/A N/A None S. intermedius S. intermedius 14)
6 F/3 N/A N/A N/A None S. intermedius S. intermedius
Actinomyces aphrophilus 7 M/6 Ebstein anomaly,
Otitis media, Patent foramen
ovale
Fever, Headache, Vomiting, Syncope
Multiple + Negative S. intermedius 15)
8 M/16 Nothing Vomiting, Myalgia, Chill, Headache
Multiple + Negative S. intermedius
S. constellatus
9 F/16 Sinusitis Headache Frontal lobe N/A Viridans
Streptococci S. intermedius 16) CHD: congenital heart disease, F: female, GPC: Gram positive cocci, GSD: glycogen storage disease, M: male, N/A: not applicable, +: detected
菌同定システム(データベース型起炎菌同定ソフト ウェア)には
2019年
7月現在,162 菌種が登録され て お り,そ れ ぞ れ の 菌 種 に は 更 に
2〜3の
mutant strainsが含まれる.埼玉県立 小 児 医 療 セ ン タ ー で
2011年から
2015年に採取された血液培養で陽性と なった
605ボトルでは,データベースは
99%(588ボ トル)をカバーしていた.一方,菌種では,陽性となっ た菌種は
46菌種で,そのうち
91%(42菌種)をカバー していた.データベースの拡充により,まれな菌種の 同定が可能となるか検証が必要である.Tm mapping 法では,PCR 法により核酸を増幅するため臨床検体
内の
dominantな菌が増幅される.また,複数菌が量
的に同程度含まれる場合,7 つの
Tm値が重なり合っ て起炎菌の同定が困難となるため,Tm mapping 法 は主に無菌検体に対する単一菌の同定に適している.
喀痰や肛門周囲膿瘍などの複数菌の関与が多い感染症 の起炎菌の同定時には複数菌の菌量の割合によって
dominant
な菌のみ同定するか,同定が不可能となる.
また,bacterial universal primer を用いた
PCR検出 であるため,細菌のみを同定する.Tm mapping 法 は培養を要せず臨床検体から直接同定が可能であるた め,特に迅速検査を必要とするケースでの用途が期待 される.汎用化のためには検査工程で
contaminationが起こらないように簡易化と機械化が今後の課題であ る.本症例では,術中に得られた排膿液
50μLから
Bac- terial DNA Extraction Kit(三井化学,日本)を用いて添付説明書に従って
bacterial DNAを抽出した.そ
の後,上記の通り
1st PCRを行い,16S rDNA の増 幅を確認した(Fig. 2a).2nd PCR の結果,7 つの
Tm値が得られ(Fig. 2b),データベースと照合し
S. inter-medius
と一致し脳膿瘍の
dominantな原因菌を早期に
検出した(Fig. 2c).検出された原因菌の種類から,口 腔内ないしは上気道が感染の侵入門戸と考えられた.
脳膿瘍において齲歯や副鼻腔炎などの上気道が感染 の侵入門戸と考えられた場合には,viridans strepto-
cocci,Haemophilusspp.,Fusobacteriumspp.,Bacteroi-des spp.などが一般的な原因菌として頻度が高いため,
内科的治療として,抗菌薬は第三世代セフェムとメト ロニダゾールが推奨される
5).小児において初期治療 として外科的治療と内科的治療を比較した前向き臨床 研 究 は な い が,Arlotti ら
6)は シ ス テ マ テ ィ ッ ク レ ビューを行い,入院時に重度の神経学的障害がない
(GCS>12),2.5cm 未満の小膿瘍,多発性脳膿瘍,外 科手術の禁忌がある場合,には内科的治療を先行し,
1〜2
週間以内に臨床的および画像評価による改善が 見られない場合,手術を再検討すべきとしている.ま た,治療期間として,内科的治療のみでは
6〜8週間,
外科的治療を行った患者では
4〜6週間の治療が推奨
される.抗菌薬の移行性に関しては,CTX と
MNZの脳膿瘍への移行性は良いことが報告されている
7)8).
本症例では,神経学的所見に異常は認めず,入院時の
MRIで左前頭葉に被膜様構造を有する多房性腫瘤を
認めた.菌量の減少と原因菌の同定目的に排膿ドレ
ナージを行い,術後から脳膿瘍への移行性の良い
CTXFig. 2 (a) Amplification of the 16S rDNA using the bacterial universal primer. (b) Melting curves of the seven amplicons. (c) The seven melting temperatures (Tm) of the amplicons were mapped and its plot matches with the plot of S. intermedius in the database.
と
MNZの点滴静注を継続したが,排膿ドレナージ後,
3
週間後に膿瘍径が
5cmまで拡大し,改善に乏しい ため開頭による膿瘍摘出術を行った.開頭時に得られ た排膿液は白色膿であった.開頭に至った理由として,
膿瘍が多房性であったことから初回の排膿ドレナージ で十分に排膿されなかった可能性が考えられた.外科 的治療と約
6週間の抗菌薬治療により後遺症なく改善 した.
Tm mapping
法は,16S rDNA から得られた
7つ の
ampliconの
Tm値をもとに菌を同定するため,厳 密には
16S rDNA系統解析と手法は異なる.
Tm map- ping法によって迅速診断や治療につながった小児の 症例は過去に
3例報告されている
9)〜11).いずれの症例 においても
Tm mapping法で得られた結果と臨床情 報を参考にして抗菌薬の
de-esalation,または経験的治療の支持が行われた.本症例では,排膿ドレナージ 直後から経験的治療として
CTXと
MNZで治療を開 始し,術直後の排膿液から
Tm mapping法で
S. inter-medius
を短時間で同定し,経験的治療としての
CTXと
MNZの継続を支持した.後日,排膿液の培養検査
BacT/ALERT 3D Microbial Detection System(BioMerieux, France)でコロニーが発育し
MALDI- TOF MSでも
S. intermedius/milleriが同定され,その 後に得られた感受性の結果も全般的に良好であった.
副鼻腔炎や齲歯を認め,上述のとおり,過去の報告で
は他の口腔内常在菌との複数菌による混合感染が否定 できないと判断し,抗菌薬の
de-escalationは行わず
CTXと
MNZ併用をその後も継続した.
様々な検査ツールが開発されているが,それによっ て得られる結果と臨床情報を鑑み,適切に治療方針を 選択することが求められる.本症例では,
Tm mapping法により
dominantである原因菌を短時間で同定した
が,同定された菌種から口腔内の常在菌による複数菌 の混合感染が想定されたため抗菌薬の
de-escalationには至らなかった.確実な初期治療を選択することが できたが,一方で,複数菌混合感染の診断ないしは否 定をどう行い,抗菌薬の適正使用につなげることがで きるかさらに症例を蓄積し詳細な検討が必要である.
利益相反自己申告:著者仁井見英樹は三井化学(株)
から奨学寄附金を受けている.
本研究は国立研究開発法人日本医療研究開発機構
(AMED)の支援によって行われた.
文 献
1)Niimi H, Ueno T, Hayashi S, Abe A, Tsurue T, Mori M,et al.:Melting Temperature Mapping Method : A Novel Method for Rapid Identifica- tion of Unknown Pathogenic Microorganisms within Three Hours of Sample Collection. Sci Rep. 2015;5:12543.
2)Frazier JL, Ahn ES, Jallo GI:Management of brain abscess in children. Neurosurg Focus.
2008;24(6):E8.
3)Christopher JH:Focal Suppurative Infections of the Nervous System. In:SS Long, CG Prober, M Fischer, eds. Principles and Practice of Pediatric Infectious Diseases(5th ed). Elsevir, 2018;p. 329―39.
4)Facklam R:What happened to the strepto- cocci : overview of taxonomic and nomenclature changes. Clin Microbiol Rev. 2002;15:613―30.
5)Xavier SL, Javier NG:Parameningeal Infec- tions. In:Cherry JD, Harrison GJ, Kaplan SL, Steinbach WJ, Hotez PJ, eds. Feigin and Cherryʼs Textbook of Pediatric Infectious Dis- eases. Elsevir, 2019;p. 336―45.
6)Arlotti M, Grossi P, Pea F, Tomei G, Vullo V, De Rosa FG,et al.:Consensus document on contro- versial issues for the treatment of infections of the central nervous system : bacterial brain ab- scesses. Int J Infect Dis. 2010;14:79―92.
7)Sjölin J, Eriksson N, Arneborn P, Cars O:Pene- tration of cefotaxime and desacetylcefotaxime into brain abscesses in humans. Antimicrob Agents Chemother. 1991;35:2606―10.
8)Warner JF, Perkins RL, Cordero L:Metronida- zole therapy of anaerobic bacteremia, meningi- tis, and brain abscess. Arch Intern Med. 1979;
139:167―9.
9)小竹悠子,閑野将行,芳賀光洋,今西利之,佐 伯久子,閑野知佳,他:嫌気性菌Fusobacterium
nucleatumによる新生児敗血症の1例.小児臨
2018;71:1116―20.
10)Sato S, Aoyama T, Uejima Y, Furuichi M, Suganuma E, Takano T,et al.:Pyogenic liver abscess due to hypervirulent Klebsiella pneumo-
niae in a 14-year-old boy. J Infect Chemother.
2019;25:137―40.
11)上島洋二,樋渡えりか,櫻谷浩志,南部隆亮,佐 藤 智,菅沼栄介,他:迅速診断と早期からの 治療介入により救命できた侵襲性髄膜炎菌感染 症.日小児会誌 2019;123:53―9.
12)Hu HL, Guo LY, Wu HL, Feng WY, Chen TM, Liu G:Evaluation of next-generation sequenc- ing for the pathogenic diagnosis of children brain abscesses. J Infect. 2019;78:323―37.
13)Issa E, Salloum T, Panossian B, Ayoub D, Ab- boud E, Tokajian S:Genome Mining and Com- parative Analysis of Streptococcus intermedius Causing Brain Abscess in a Child. Pathogens.
2019;8:E22.
14)Kommedal Ø, Wilhelmsen MT, Skrede S, Meisal R, Jakovljev A, Gaustad P:Massive parallel se- quencing provides new perspectives on bacte- rial brain abscesses. J Clin Microbiol. 2014;
52:1990―7.
15)Petti CA, Simmon KE, Bender J, Blaschke A, Webster KA, Conneely MF,et al.:Culture- Negative intracerebral abscesses in children and adolescents from Streptococcus anginosus group infection : a case series. Clin Infect Dis.
2008;46:1578―80.
16)Tran MP, Caldwell-McMillan M, Khalife W, Young VB:Streptococcus intermediuscausing in- fective endocarditis and abscesses : a report of three cases and review of the literature. BMC Infect Dis. 2008;8:154.
A Case of a Brain Abscess withStreptococcus intermediusRapidly Diagnosed with the Melting Temperature Mapping Method
Yoji UEJIMA1)2), Jun KURIHARA3), Mihoko FURUICHI1), Satoshi SATO1), Hideki NIIMI2), Yutaka KAWANO1), Tsutomu OH-ISHI1)& Eisuke SUGANUMA1)
1)Division of Infectious Diseases and Immunology and Allergy, Saitama Childrenʼs Medical Center, 2)Department of Clinical Laboratory and Molecular Pathology, Graduate School of Medical and Pharmaceutical Science, University of
Toyama,3)Department of Neurosurgery, Saitama Childrenʼs Medical Center
An 11-year-old boy, who had undergone repair of a total anomalous pulmonary venous connection (TAPVC) and double outlet right ventricle (DORV) during infancy, presented with a headache. Sinusitis and dental caries were also observed. Computed tomography (CT) scan revealed a mass on the left frontal lobe of his brain. He was diagnosed as having a brain abscess (BA) based on the magnetic resonance imaging (MRI) findings. The BA was drained, and the patient was treated with 300mg/kg cefotaxime and 40mg/kg metronidazole per day intravenously as empirical therapy. The melting temperature mapping method re- vealedStreptococcus intermediusin the intracranial pus 4.5 h after drainage. The echocardiogram showed no infective endocarditis. Matrix-assisted laser desorption/ionization-time of flight mass spectrometry (MALDI- TOF MS) detected the same organism from the pus 3 days after drainage. The organism was pansuscep- tible, and treatment was continued because the presence of anaerobic, Gram-negative bacilli was suspected in the sinus cavity and dental plaque. The brain abscess, however, grew to 5cm 3 weeks after the drainage even under continued antibiotic therapy. A craniotomy was performed, and the entire abscess, including the abscess wall, was excised. Antibiotics were continued for 6 weeks, and the patient recovered completely.
Rapid detection empirical therapy by administering appropriate antibiotics and total excision of the abscess successfully treated the patient. Thus, the use of rapid diagnostic tests and the melting temperature map- ping method had significant impacts on effective antimicrobial stewardship.