Acta Med. Nagasaki 37:183-186
Omentopexy
Masao Tomita, Hiroyoshi Ayabe, Katsunobu Kawahara, and Yutaka Tagawa The First Department of Surgery, Nagasaki University School of Medicine
The operative procedure of bronchial anastomosis is of great use to prevent major complication in relation to anastomosis insufficiency as well as to reduce the inci- dence of anastomosis insufficiency.
In particular, omentopexy is indispensable for tracheo- bronchial anastomosis in combination with esophagectomy, which means a loss of supporting tissue and a reduction of collateral blood flow through the wall of the trachea.
Furthermore, the application of omentopexy is limited in case of a history of abdominal surgery and the diseases of the spleen and/or the omentum.
Introduction
The omentum is well adaptable for tissue defect of various sizes and shapes and poses sufficient blood supply.
The use of the omentum offers some advantage that it has rich tissue volume and is able to preserve the long pedicle by gastroepiploid artery. Moreover, neovascularity
is facilitated, lymphedema is eliminated, providing rich fibroblast. As a consequence, wound healing is satisfied.
In addition, it is of great value to prevent spreading of infection and to wrap the infectious tissue by contracting the infected deadspace.
Mobilization of The Omentum
The omentum is nourished by supply of the blood from bilateral gastroepiploic arteries and their branches form the vascular arcade. The size of the omentum measured 14 to 36 cm long, 23 to 46 cm wide and it was possible to draw up to the level of the breast gland (Fig. 1) and to draw down to the site of the inguinal ligamentum. Furthermore, the addition of the procedure of mobilization by making free of the attachment of the stomach makes it possible to draw up to the neck in 88%, to the Axilla in 70%, to the upper arm in 25% and the middle of the thigh in 10%.
respectively.
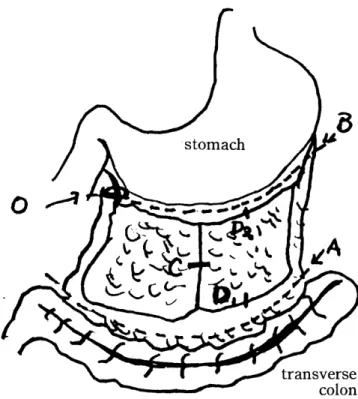
Fig. 1. Mobilization of the omentum
A) a line between the omentum and the transverse colon
B) a line between the omentum and the stomach, preserving the gastroepiploic artery
C) mobilized by division of the middleo mental artery D) dividing between D, and D2 to make it elongation
Indication of Omentopexy
Omentopexy is usually applied for prevention of major complication when expecting the impairment of wound healing, for promotion of severely impaired wound healing when occurring complication and for supplement of tissue defect.
Validity of Omentopexy for tracheobronchial anastomosis
When occurring impairment of wound healing of tracheo-
bronchial anastomosis, respiratory function was severely
affected by spreading infection to the pleural cavity and the
1 84
:=f r {
*=<'s::̲ *.*:
Upper:
Lower:
;=
M. Tomita et al: Omentopexy
Fig. 2. Microangiogram
The bronchial arterial flow was interrupted at bronchial anastomosis on day 3 after bronchial anastomosis The bronchial flow was appearently seen aross the bronchial anastomosis on day 14
mediastinum. In consequence, it takes a rapid fatal course.
It is indispensable that bronchial arteries are interrupted at anastomosis so that nutritional blood flow should be remarkable reduced. As a result, wound healing at anasto‑
mosis is impaired.
After anastomosis of tracheobronchial tree, the time of regeneration of the bronchial artery was investigated by the grades of developing recannalization on microangiography.
According to our study as shown in Fig. I , recannal‑
ization of the bronchial artery was initiated at day 5 to 7 and completed at day 10 to 14. When wrapping of the omentum was applied, the start of regeneration was seen at day 3 to 4 and the completion was observed at day 5 to 7 as shown in Fig. 3.
Grade
Ill
II
l