Determination of In-vivo Glenohumeral Translation during Loaded and Unloaded Arm Elevation
Naoya NISHINAKA*1, 2), Takayuki MATSUHISA2), Yuji TAKAHASHI3), Hiroaki TSUTSUI4) and Takeyuki SAMBE1)
Abstract : An understanding of normal joint kinematics is essential to develop treatments that restore normal joint mechanics ; however, reports of kinematics during dynamic motion are rare. This study thus investigated glenohumeral (GH)
translation in vivo during loaded and unloaded shoulder abduction. Nine healthy shoulders were studied from our patient cohort (average age, 31 years). We cre- ated 3D models of the scapula and humerus using computed tomography (CT)
images and recorded fluoroscopic images during active abduction in neutral rotation in the plane of the scapula using a hand-held 3kg weight or no additional load.
3D motions were determined using model-based 3D-to-2D registration. Glenohu- meral translation was determined by finding the location on the humeral head with the smallest separation from the plane of the glenoid. The humerus moved an average of 2 mm during arm abduction, from inferior to the center of the glenoid.
There were no statistically significant differences between the unloaded and loaded conditions. Variability in humeral translation decreased with abduction using both 3-kg and 0-kg conditions, with significantly lower variability showing above a 70 GH abduction. We showed that humeral translation to the center of the glenoid maximizes joint congruency for optimal shoulder function and joint longevity. This data should lead to better strategies for shoulder injury prevention, enhanced reha- bilitation, and improved surgical treatments.
Key words : shoulder kinematics, fluoroscopy, model-image registration
Introduction
Various factors including the rotator cuff are important for stabilizing the glenohumeral joint over a wide range of motions and dynamic conditions. Indeed, inadequate control of glenohu- meral translation during dynamic activities is implicated in subacromial impingement syndrome, degenerative arthritis of the shoulder, and many other joint-damage mechanisms.
Single-plane fluoroscopic imaging has been used for the past 15 years to record and quantify the motions of knee replacements during dynamic activities. This technique was recently used Original
1)Showa University Research Institute for Sport and Exercise Sciences, 2-1-1 Fujigaoka, Aoba-ku, Yokohama 227-8518, Japan.
2)Department of Orthopaedic Surgery, Showa University Fujigaoka Hospital.
3)Department of Rehabilitation Medicine, Showa University Koto Toyosu Hospital.
4)Department of Orthopaedic Surgery, Showa University School of Medicine.
*To whom corresponding should be addressed.
to assess the shoulder joint with and without implanted devices1-3); however, it remains difficult to measure dynamic glenohumeral translation and reports are scarce of quantitative 3D measure- ment of shoulder motion during clinically relevant motions. This study was thus motivated by the assumption that treatment and rehabilitation of shoulder injuries could be improved with better knowledge of glenohumeral mechanics during dynamic activities in healthy and damaged joints.
This study investigated glenohumeral translation in vivo during loaded and unloaded shoulder abduction in the scapular plane. With the arm at the side and muscles relaxed, we assumed the humeral head would move with gravity to a relatively inferior position on the glenoid. With abduction against gravity, the rotator cuff, deltoid muscle, and other tissues will stabilize the glenohumeral joint and draw the humeral head to the center of the glenoid concavity. Thus, we hypothesized that the humeral head would be relatively inferior with respect to the glenoid with the arm at the side, moving to the center of the glenoid with arm elevation in a healthy shoulder. We also hypothesized that there would be no difference in glenohumeral translation for loaded and unloaded conditions in healthy shoulders. Because the joint is actively stabilized with increasing abduction, we also hypothesized that kinematic variability would decrease with arm abduction.
Materials and methods
Nine healthy shoulders in nine volunteer subjects (8 males, 1 female ; average 31.1 years, 27 to 38 years old) were studied. All shoulders were asymptomatic, had no history of injury, and lacked any clinical or radiographic signs of pathology. All subjects provided informed consent to participate in this study. CT scans of each shoulder were acquired at 0.5-mm intervals and 3D models of the scapula and proximal humerus were created in two stages. First, computed tomography (CT) images of the exterior cortical bone edges were segmented using commercial software (SliceOmatic, Tomovision, Montreal, CA, USA), and then these point clouds were con- verted into polygonal surface models (Geomagic Studio, Raindrop Geomagic, Research Triangle Park, NC, USA).
The subject was positioned in front of a fluoroscope and motions were recorded during active abduction in neutral rotation from arm at side to full abduction in the plane of the scapula.
The subjects performed two trials: one trial holding a 3 kg weight and one unloaded trial.
3D motions of the scapula and humerus were determined using model-based 3D-to-2D regis- tration (Fig. 1). A custom shape-matching program was used to obtain six-degrees-of-freedom shoulder kinematics. Estimated measurement errors for this process were 0.5 mm for scapular plane translations, and 0.5 degrees for shoulder abduction4, 5).
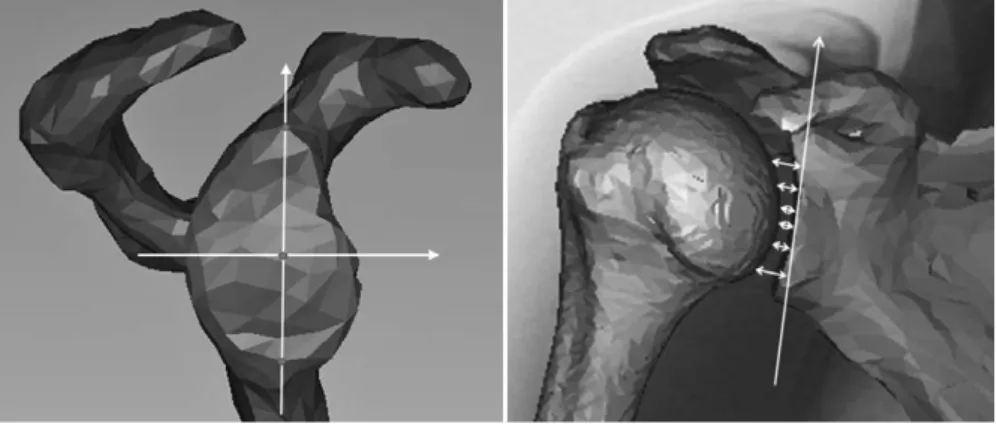
The glenoid plane was defined as the line parallel from the superior bony edge to the inferior glenoid edge and included the line defining the perpendicular short axis of the glenoid (Fig. 2). The glenoid center was defined as the midpoint of the long axis. Humeral translation was referenced to the glenoid center in the superior/inferior direction. Glenohumeral translation was determined in each data frame by finding the location on the humeral head with least separa-
tion from the plane of the glenoid (Fig. 3). Motion data were grouped into 10 intervals of glenohumeral (GH) abduction for loaded and unloaded conditions, and compared from 30 to 90 using t-tests with a Bonferroni correction with significance at P<0.05. The F-test was used to compare kinematic variability between the initial position and each position of incremental abduction.
Fig. 1. 3D-to-2D model-to-image regi- stration was used to determine 3D motion of the scapula and humerus during dynamic arm elevation with and without hand- held weights.
Fig. 2. The Glenoid plane was defined as para- llel to a line from the superior bony edge to the inferior glenoid edge and including the line defining the short axis (a perpendicular line intersecting the midpoint of the long axis) of the glenoid.
Fig. 3. (a.) The glenoid center was defined as the midpoint of the long axis. (b.)
Humeral translation was referenced to the glenoid center in the superior/
inferior direction. Glenohumeral translation was determined in each data frame by finding the location on the humeral head with the smallest separation from the plane of the glenoid.
Results
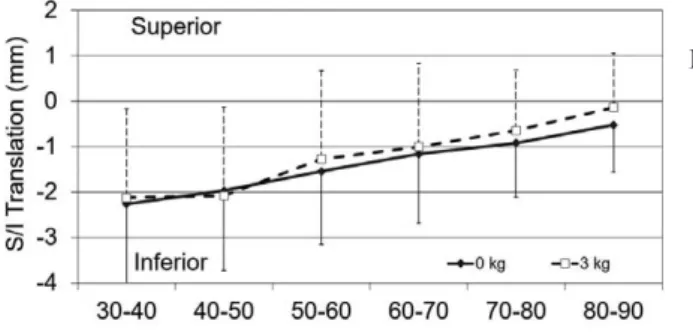
The humerus moved an average of 2 mm, from inferior to central on the glenoid, during arm abduction under both the unloaded and 3-kg loaded conditions (Fig. 4). The humeral head was centered within 1 mm from the glenoid center above 70 GH abduction. There were no statistically significant differences in translations between unloaded and 3-kg loaded conditions.
All shoulders exhibited the same pattern of motion and the main source of variability seemed to reflect the definition of the glenoid center, resulting in an offset of each shoulderʼs data from a consistent point on the glenoid. The standard deviation decreased gradually over the motions for both conditions, with significantly lower variability in glenohumeral translation above 70 GH abduction.
Discussion
Glenohumeral joint pathology results from a variety of mechanical and non-mechanical causes, and a better understanding of normal joint kinematics is essential for treatments to restore normal joint dynamics. Some authors suggest geometric mismatch between the humeral head and glenoid as one cause of pathology in high stress areas6). Thus, the objective of this study was to analyze the superior-inferior translations of the humeral head relative to the glenoid in vivo during 3-kg loaded and unloaded arm abduction. Limitations of our study include the need to use ionizing radiation to observe motion, the low number of participating subjects, and reduced measurement accuracy of single-plane fluoroscopy compared to biplane fluoroscopic or radiographic techniques.
A variety of methods have been used to describe humeral head translation and the impor- tance of passive stabilizers; however, these studies have provided few consistent findings. Poppen and Walker7, 8) observed on radiographs that the humeral head moved upward relative to the glenoid during unloaded abduction between 0 and 30 , with little additional translation thereafter for unloaded conditions. In contrast, Deutsch et al9) described a more centered position of the humeral head in healthy volunteers holding a weight equal to 2.5% of their body weight, and no significant change in position during abduction.
Other studies using x-ray imaging have also suggested that the glenohumeral joint behaves as
Fig. 4. The humerus translated from inferior to central locations on the glenoid during active arm abduction. The standard deviation
(STDV) decreased gradually during the motion, with significantly lower variability at above 70 and at the end of GH motion compared to the initial position with unloaded and 3-kg-loaded conditions. Glenohumeral translations were not different for unloaded and loaded conditions.
a perfectly congruent ball and socket joint10). Conversely, some cadaver studies showed gleno- humeral translation during abduction. Nobuhara et al11) evaluated movement of glenohumeral contact and suggested an inherent articular mismatch between the humeral head and glenoid. In addition to, Warner et al6) measured contact area and pressure on the glenoid over the range of abduction and concluded that the glenohumeral joint was relatively incongruent (small contact area and high peak pressures) for low arm angles and increasingly congruent (high contact areas and low peak pressures) for the arm abducted above 30 . These authors also suggested articular mismatch as the factor permitting humeral head translation at lower degrees of abduction, but subsequent measurements of glenoid contact area with 222N and 444N joint compressive loads revealed no significant differences in the contact patterns. Similarly, Greis et al12) also evaluated glenoid contact areas with the same loads and found no significant differences. Notably, these in vitro studies require assumptions about muscle forces, joint loads and coordination of motion, all of which are difficult to quantify in vivo, and such uncertainties make it more difficult to interpret and directly apply in vitro study findings to clinical treatment and interpretation.
Open magnetic resonance (MR) imaging recently showed three-dimensional glenohumeral motion in vivo with varied results. Graichen et al13) studied glenohumeral translations using MR with supine subjects holding a series of five static positions. They described inferior translation of the humerus from 30 to 150 , and found a more central humeral position when the arms were supporting a steady 1 kg load. Both of these findings are quite different from our fluoro- scopic data on upright subjects, suggesting that subject posture and/or dynamic motion may be important variables determining glenohumeral translation. Supporting this hypothesis, Beaulieu et al14) studied upright subjects in an open MR system and reported that the humeral head remained more-or-less centered on the glenoid over a full range of motion, deviating from the glenoid center by less than 3 mm.
Boyer et al1) used both biplane fluoroscopic imaging and MR-derived bone models to deter- mine glenohumeral kinematics during unloaded dynamic abduction in five subjects. They found the average humeral contact position was located approximately 5 mm from the glenoid center in the posterior-superior quadrant for abduction from 0 to 90 , and significant variability among the five shoulders tested. In a separate study, Matsuki et al15, 16) expressed translations based upon the relative positions of local bone coordinate system origins and the calculated glenohumeral center of rotation, which differed from our evaluation using contact points with the smallest dis- tance between the two bones. Thus, in the supero-inferior direction, translations calculated with the three different methods were roughly parallel showing statistically significant differences.
The glenohumeral kinematic data support the hypotheses that the humerus will move superior with abduction, from inferior to a location near the glenoid center, and that healthy shoulders will show no differences in glenohumeral translation for loaded and unloaded conditions. We also used scapulohumeral rhythm (SHR) to provide insight into neuromuscular control and fun- damental biomechanics of the shoulder using the same healthy subjects and technique17). SHR decreased (more scapular motion) with increasing abduction, in that scapulothoracic motion was significantly reduced through the range of 35 degrees to 45 degrees of glenohumeral motion
with a 3-kg load, whereas glenohumeral translation showed no differences for 0-kg and 3-kg conditions. These results indicated that muscular stabilization of the scapula with external load- ing increased in the healthy shoulders to provide a critical platform for upper extremity activity.
Numerous other studies have also shown the humeral head moving to the glenoid center during elevation in healthy shoulders7, 9, 13, 14, 18-21), in contrast, injured shoulders with diagnoses of cuff deficiency, instability, and trauma exhibit humeral translation away from the glenoid center7, 9, 18-22). Therefore, we assume that humeral translation to the center of the glenoid provides maximum joint congruency for optimal shoulder function and joint longevity.
Our data also support the prediction of decreased inter-subject variability in glenohumeral translation with increasing abduction. Greater centering and joint contact forces are developed with increased abduction, thus a stable joint provides efficient linkage for the rotator cuff with the deltoid muscle and scapular function in elevated postures. Active translation of the humeral head away from the glenoid center could therefore indicate insufficient passive and/or active sta- bilization and is likely causative of gradual joint degeneration due to local articular cartilage and labrum overload20, 22-27). Further studies are clearly required to fully understand the mechanisms providing glenohumeral stability during dynamic motion, and we believe 3D fluoroscopic analysis of shoulder kinematics can and will provide such information about shoulder function. This enhanced understanding will facilitate better strategy development to prevent shoulder injuries, enhance rehabilitation, and improve surgical treatments.
Acknowledgement
The authors gratefully acknowledge Katsuya Ishida for his assistance acquiring the fluoroscopic and CT images.
Conflict of interest statement disclosure
We have no financial affiliation or involvement with any commercial organization that has a direct financial interest in any matter included in this manuscript, except as disclosed in an attachment and cited in the manuscript. Any other conflict of interest is also disclosed in an attachment.
References
1) Boyer PJ, Papannagari R, Gill TJ, et al. In-vivo articular cartilage contact at the glenohumeral joint: preliminary report. J Orthop Sci. 2008;13:359-365.
2) Mahfouz M, Nicholson G, Komistek R, et al. In vivo determination of the dynamics of normal, rotator cuff- deficient, total, and reverse replacement shoulders. J Bone and Surg Am. 2005;87:107-113.
3) Nishinaka N, Tsutsui H, Mihara K, et al. Determination of in vivo glenohumeral translation using fluoroscopy and shape-matching techniques. J Shoulder and Elbow Surg. 2008;17:319-322.
4) Banks SA, Hodge WA. Accurate measurement of three-dimensional knee replacement kinematics using single- plane fluoroscopy. IEEE Trans Biomed Eng. 1996;43:638-649.
5) Moro-oka TA, Hamai S, Miura H, et al. Can magnetic resonance imaging-derived bone models be used for accu- rate motion measurement with single-plane three-dimensional shape registration? J Orthop Res. 2007;25:867-872.
6) Warner JJ, Bowen MK, Deng XH, et al. Articular contact patterns of the normal glenohumeral joint. J Shoulder Elbow Surg. 1998;7:381-388.
7) Poppen NK, Walker PS. Forces at the glenohumeral joint in abduction. Clin Orthop. 1978;(135):165-170.
8) Poppen NK, Walker PS. Normal and abnormal motion of the shoulder. J Bone Joint Surg Am. 1976;58:195-201.
9) Deutsch A, Altchek DW, Schwartz E, et al. Radiologic measurement of superior displacement of the humeral head in the impingement syndrome. J Shoulder Elbow Surg. 1996;5:186-193.
10) Howell SM, Galinat BJ. The glenoid-labral socket: A constrained articular surface. Clin Orthop Relat Res. 1989;
(243):122-125.
11) Nobuhara K, Inamochi H, Ikeda H, et al. Dynamic analysis of contact area in the shoulder joint. Seikei geka baiomekanikusu. 1983;4:91-93. (in Japanese).
12) Greis PE, Scuderi MG, Mohr A, et al. Glenohumeral articular contact areas and pressures following labral and osseous injury to the anteroinferior quadrant of the glenoid. J Shoulder Elbow Surg. 2002;11:442-451.
13) Graichen H, Stammberger T, Bonel H, et al. Glenohumeral translation during active and passive elevation of the shoulder - a 3D open-MRI study. J Biomech. 2000;33:609-613.
14) Beaulieu CF, Hodge DK, Bergman AG, et al. Glenohumeral relationships during physiologic shoulder motion and stress testing: initial experience with open MR imaging and active imaging–plane registration. Radiology.
1999;212:699-705.
15) Matsuki K, Matsuki KO, Yamaguchi S, et al. Dynamic in vivo glenohumeral kinematics during scapular plane abduction in healthy shoulders. J Orthop Sports Phys Ther. 2012;42:96-104.
16) Matsuki K, Kenmoku T, Ochiai N, et al. Differences in glenohumeral translations calculated with three methods:
Comparison of relative positions and contact point. J Biomech. 2016;49:1944-1947.
17) Kon Y, Nishinaka N, Gamada K, et al. The influence of handheld weight on the scapulohumeral rhythm. J Shoul- der Elbow Surg. 2008;17:943-946.
18) Chen SK, Simonian PT, Wickiewicz TL, et al. Radiographic evaluation of glenohumeral kinematics: a muscle fatigue model. J Shoulder Elbow Surg. 1999;8:49-52.
19) Oizumi N, Suenaga N, Minami A, et al. Analysis of the kinematics of the glenohumeral joint during active abduc- tion using open MRI. The Shoulder Joint. 2002;26:481-485. (in Japanese).
20) Pelet S, Jolles BM, Farron A. Bankart repair for recurrent anterior glenohumeral instability: results at twenty-nine yearsʼ follow-up. J Shoulder Elbow Surg. 2006;15:203-207.
21) Yamaguchi K, Sher JS, Andersen WK, et al. Glenohumeral motion in patients with rotator cuff tears: a compari- son of asymptomatic and symptomatic shoulders. J Shoulder Elbow Surg. 2000;9:6-11.
22) Morgan CD, Burkhart SS, Palmeri M, et al. Type Ⅱ SLAP lesions: three subtypes and their relationships to supe- rior instability and rotator cuff tears. Arthroscopy. 1998;14:553-565.
23) Andriacchi TP, Dryby CO. Interactions between kinematics and loading during walking for the normal and ACL deficient knee. J Biomech. 2005;38:293-298.
24) Beaupre GS, Stevens SS, Carter DR. Mechanobiology in the development, maintenance, and degeneration of articular cartilage. J Rehabil Res Dev. 2000;37:145-151.
25) Feeney MS, Oʼdowd J, Kay EW, et al. Glenohumeral articular cartilage changes in rotator cuff disease. J Shoulder Elbow Surg. 2003;12:20-23.
26) Hsu HC, Luo ZP, Stone JJ, et al. Correlation between rotator cuff tear and glenohumeral degeneration. Acta Orthop Scand. 2003;74:89-94.
27) Hovelius L, Augustini BG, Fredin H, et al. Primary anterior dislocation of the shoulder in young patients. A ten- year prospective study. J Bone Joint Surg Am. 1996;78:1677-1684.
[Received June 16, 2016 : Accepted August 15, 2016]