Past, Present, and Future of Non-vascular IVR
Tetsuya Yoshioka, M.D.,1) Hiroshi Anai, M.D.,2) and Hiroshi Sakaguchi, M.D.2)
Summary
The 1980s appeared to be the dawn of a new era of non-vascular interventional radiology (IVR) in Japan. The procedures conducted during this time included cyst ablation, abscess drainage, urinary and biliary drainage, external-internal drainage, endoprosthesis, bougie or balloon dilatation for luminal stenosis, litho-tomy, biopsy, and percutaneous gastrostomy. The aim of these strategies was primarily radical cure in benign diseases or palliative treatment in malignant diseases to improve the quality of life (QOL) of patients. These procedures or treatment approaches are still popular today, but the non-vascular IVR of that
NICHIDOKU-IHO
Vol. 50 No. 1 84–97 (2005) 1) Department of Radiology, Nara Prefectural Nara Hospital 2) Department of Radiology, Nara Medical University
放射線診療の過去・現在・未来
放射線診療
3-2.IVRの過去・現在・未来−非血管系
(Non-vascular IVR)
奈良県立奈良病院 放射線科1) 奈良県立医科大学 放射線科2)
吉岡 哲也
1),穴井 洋
2),阪口 浩
2)era covered only narrow areas as compared with vascular IVR, and the target diseases were limited.
In the 1990s, however, the advent of metallic stents brought dynamic change to the field of non-vascular IVR, not only in Japan, but also throughout the world. New areas were introduced, and many new treatment approaches were developed, including percutaneous ethanol injection therapy (PEIT), a treatment developed in Japan for hepatic tumors, as well as procedures for the reproductive organs such as prostatic urethral balloon dilatation and fallopian tube recanalization. The era could be represented not only by the advent of new devices such as metallic stents implant-able in the body but also by progress in mechanization, such as the rotablator used in gallbladder lithotomy, usher-ing in an era of progress in which immense strides were made.
In the 2000s, the techniques advanced into the orthopedic field, an area largely uncultivated until then. The rep-resentative treatment procedures included percutaneous injection of acrylic bone cement, as well as percutane-ous laser disk decompression. In addition, as a replacement for PEIT, percutanepercutane-ous microwave coagulation therapy and radiofrequency ablation appeared as topical heat therapies, in addition to the opposite technique of cryotherapy, or topical freezing. Also attracting attention are anastomoses formed by magnetic compression, with surgical anas-tomosis completed with IVR for the first time in the world. The era after 2000 can be considered an era of evolu-tion. As described above, progress in non-vascular IVR has been remarkable since the 1990s. Through the efforts of many experts, including those in Japan, many new devices, procedures, and treatment approaches were developed and established, and their indications continue to be extended. The low invasiveness of IVR was emphasized in the 1990s. In the future, narrower devices will be developed, and, although current common procedures generally in-volve puncture, future treatment will advance so as not to require puncture, as with the focused ultrasound therapy used in tumor ablation.
Further, the trend toward uniform, standardized procedures that offer more precise results and are not dependent on the operator’s skill have led to the development of medical robots, some of which are already in practical use in the surgical field and are expected to be introduced into the field of IVR as well. In recent years, radiation exposure to patients and medical personnel has drawn attention, especially with use of CT-guided IVR. To reduce radiation
はじめに
本邦のinterventional radiology(IVR)の歴史を、日本 人の活躍を中心に振り返りながら将来を展望する。 1.1980年代 本邦で最初に発刊されたIVRの聖書あるいは教科書と いっても過言でない書物は1 9 8 7 年の「I n t e r v e n t i o n a l Radiology−放射線診断技術の治療的応用」(平松京一、 打田日出夫編集)1)であろう。これには、当時確立され ていた手技、まだ確立されていないが注目されていた手 技や治療法が紹介されている(表 1)。 このなかでnon-vascular IVRに関しては、N胞では主 に腎N胞アブレーションが、膿瘍では広い範囲の膿瘍ド レナージが、尿路系では経皮的腎瘻造設術と、その応用 として内瘻化、尿管狭窄拡張術、結石除去が、胆道系で は経皮経肝胆道造影とドレナージ、内外瘻術、内瘻術、 さらにこれらの応用として胆道腔内照射や腔内温熱療 法、胆道拡張術、胆道内結石除去術、胆道生検法が紹介 されている。その他、この本では取り上げられていない が、経皮的胃瘻造設術や良性食道狭窄に対するブジーや バルーンによる拡張術などが行われていた。良性疾患に 対しては根治術を目指し、悪性疾患に対しては患者の quality of life(QOL)の向上を目的とした姑息的治療が 中心であった。これらの手技、治療法は現在も広く行わ れているものの、当時のnon-vascular IVRは、vascular IVRに比べるとまだまだその範囲は狭く、対象疾患も限 定され、その多くの手技が欧米で完成された時点で本邦 に導入されていた。いわば1980年代は本邦のnon-vas-cular IVRにおいては“黎明期”であったといえよう。 2.1990年代 しかし、1990年代に入るとmetallic stentが登場し、 non-vascular IVRの領域は本邦だけでなく、世界全体を 一変させた。本邦で開発された肝腫瘍に対する経皮的エ タ ノ ー ル 局 注 療 法( p e r c u t a n e o u s e t h a n o l i n j e c t i o n therapy:PEIT)、前立腺部尿道バルーン拡張術や卵管 開通術に代表されるような生殖器に対する治療など新し い分野が開拓され、次々と治療法が誕生してくる。一 方、metallic stentのような体内に埋め込む新しいdevice だけでなく、胆N結石除去術に用いるrotablatorなどの ような機械化も進んできた時代であり、大いなる発展を 遂げる“発展期”へと移行する(表 2)。 3.2000年代 さらに、近年においてはそれまで生検のみで未開に近 かった整形外科領域にも足を踏み入れている。その代表 的なものが骨病変に対するセメント注入療法やレーザー による椎間板ヘルニア減圧術といった治療法である。ま た、経皮的マイクロ波凝固療法(percutaneous micro-wave coagulation therapy:PMCT)ならびに経皮的ラジ オ波焼灼術(radiofrequency ablation:RFA)のような局 所を温熱する治療法と、それと正反対の発想から生まれ た局所を凍結させる凍結治療が出現する一方、世界で初 めて外科的吻合術をIVRで完成させた磁石圧迫吻合術 (山内法)も話題となっている(表 2)。2000年以降は、今 後も進化していくと考えられることから“進化期”とでも 名づけよう。しかし、non-vascular IVRにこのような進 歩と発展をもたらしたものとして、より安全でかつリア ルタイムに穿刺術の施行を可能にした「画像の進歩」が、 その一翼を担っていることはいうまでもないであろう。 このように現在のnon-vascular IVR領域は多くの手技、治療法が種々の疾患に広く行われている。ここでは 話題のdeviceや手技、治療法についてその一部を概説し ながら将来を展望する。
Metallic stent
細いintroducerで挿入できる大口径のmetallic stentの 登場は一大センセーションを巻き起こし、時代を一変さ せた。1986年に初めて気管狭窄に対するステント留置2) が報告されたのを機に、胆道3)、食道4、5)、大腸6–8)の狭 窄性病変に応用されていった。このmetallic stentは欧米 で開発されたものの、同時期に本邦に導入され、胆 道9–11)、食道4)領域では欧米に遅れることなく臨床応用 が開始された。本邦においてはmetallic stentが市販され るまではoriginalあるいはmodified Gianturco stentを手 製していたが、その作製法は早期に日本Metallic Stents & Grafts研究会が設立されたことも手伝って一気に全国 に広まった。まずは、胆道系が世界をリードするぐらい までに成長した12、13)。特に従来のplastic stentでは制御 困 難 で あ っ た 肝 門 部 、 肝 内 胆 管 閉 塞 に 対 す る m u l t i -stenting12、13)(図 1)は現在でも明らかに世界をリードしている。また、tumor ingrowthというuncovered stent の問題点を解消するために開発された胆道系covered stentにおいても世界に先駆けて臨床応用がなされ14、15)、 本邦のみの市販ではあったが、世界で初めて日本オリ ジナルのNT stent16)が商品化されるに至った。少し遅れ て食道ステントも臨床応用に入った(図 2)。この領域 1.Interventional Radiologyとは 2.経カテーテル動・静脈塞栓術と動注療法 A. 塞栓物質と動注薬剤 B. 基本手技 C. 頭頸部領域 D. 乳癌 E. 肺 F. 動脈管開存症 G. 肝細胞癌 H. 消化管出血 I. 胃・食道静脈瘤 J. 脾 K. 非特異性炎症性腸疾患 L. 腎 M.骨盤 N. 精索静脈瘤 3.経カテーテル血管拡張術(PTA)と血栓溶解 A. 基本手技 B. 冠状動脈 C. 腎血管 D. 骨盤,四肢,下大静脈 4.血管内異物除去・下大静脈フィルタ 5.エコーガイドによる治療 A.N胞 B.膿瘍 C.尿路 D.胆道 新しく開発された治療法 ステント留置術 食道ステント留置術 大腸ステント留置術 胆道ステント留置術 気管ステント留置術 涙管ステント留置術 経皮的腫瘍根治術 経皮的エタノール局注療法
(percutaneous ethanol injection therapy:PEIT) 熱湯局注療法
経皮的マイクロ波凝固療法
(percutaneous microwave coagulation therapy:PMCT) 経皮的ラジオ波焼灼術
(radiofrequency ablation:RFA) 経皮経食道胃管挿入術
(percutaneous transesophageal gastro-tubing:PTEG) 経皮経胃的膵仮性N胞穿刺術 前立腺部尿道バルーン拡張術 卵管開通術 胆N 結石除去術:rotablator 結石溶解術 胆Nアブレーション 経皮的神経ブロック 最近話題のnon-vascular IVR 凍結治療 骨病変に対するセメント注入療法 椎間板ヘルニア減圧術 収束超音波治療 磁石圧迫吻合術(山内法) 本邦で開発された新しいdevice ステント Spiral Z stent
胆道系covered stent(NT stent) 術前標識糸付きフックワイヤー 生検針固定器具
表 1 「Interventional Radiology―放射線診断技術の治療的応 用」の目次から1)
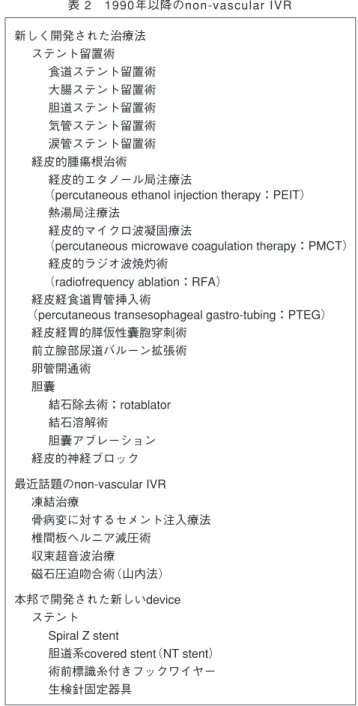
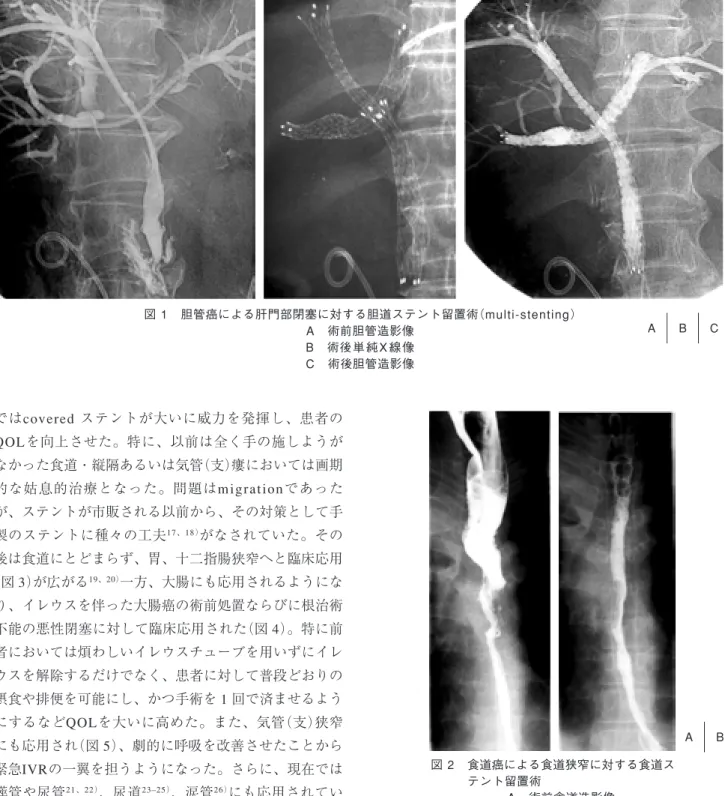
図 1 胆管癌による肝門部閉塞に対する胆道ステント留置術(multi-stenting) A 術前胆管造影像 B 術後 単 純 X 線 像 C 術後胆管造影像 A B C 図 2 食道癌による食道狭窄に対する食道ス テント留置術 A 術前食道造影像 B 術後食道造影像 A B ではcovered ステントが大いに威力を発揮し、患者の QOLを向上させた。特に、以前は全く手の施しようが なかった食道・縦隔あるいは気管(支)瘻においては画期 的な姑息的治療となった。問題はm i g r a t i o n であった が、ステントが市販される以前から、その対策として手 製のステントに種々の工夫17、18)がなされていた。その 後は食道にとどまらず、胃、十二指腸狭窄へと臨床応用 (図 3)が広がる19、20)一方、大腸にも応用されるようにな り、イレウスを伴った大腸癌の術前処置ならびに根治術 不能の悪性閉塞に対して臨床応用された(図 4)。特に前 者においては煩わしいイレウスチューブを用いずにイレ ウスを解除するだけでなく、患者に対して普段どおりの 摂食や排便を可能にし、かつ手術を 1 回で済ませるよう にするなどQOLを大いに高めた。また、気管(支)狭窄 にも応用され(図 5)、劇的に呼吸を改善させたことから 緊急IVRの一翼を担うようになった。さらに、現在では 膵管や尿管21、22)、尿道23–25)、涙管26)にも応用されてい る。そのなかで日本オリジナルのspiral Z stent27)が開発 され、胆道、食道、気管に用いられた。
今後の展開
現在、non-vacular領域に認可されているステントは 胆道、食道、気管のみで、大腸など他領域では認可され ていない。また、次々と新しいステントが市販される最 も発展した胆道系でさえその多くが血管系として開発さ れたdeviceの転用であり、近年は新しいタイプのステン トは開発されていない。ステントが開発されてから未解 決の問題としては、除去不能、良性狭窄や小児への適応ステントの未開発などがある。一部の研究者が除去可 能28–30)あるいは逆流防止の工夫31、32)をしているが商品化 には至っていない。一方、良性狭窄については、胆道系33) や食道34)、大腸35)、気管28)などに応用されてきたもの の、早期の閉塞や多くの合併症が発現することから、す べての治療が不成功に終わったときに適応となる最終選 択治療の位置付けにある。成人と異なり日々成長する小 図 3 胆N癌による十二指腸狭窄に対するステント留 置術 A 術前消化管造影像:十二指腸狭窄があり,大腸 への瘻孔もみられる. B 術後単純X線像 C 術後消化管造影像 A B C D 図 4 大腸癌によるS字状結腸狭窄に対するステント留置術 A 術前注腸造影像 B 術後注腸造影像 A B 児においては適応するステントの開発は遅々として進ん でいない。そこで将来的に期待がかけられているのが、 回収しなくても一定期間経過すれば溶解・吸収される生 体吸収性ステント(bioabsorbable stent)である。生体吸 収性ステントは加水分解によって溶解・吸収される性質 をもち、既に医療器具として縫合糸や骨釘など使われる ポリ乳酸、ポリグリコール酸、カプロラクトンなどが材
質として使われている。食道36)、気管37–39)、尿道40)など で基礎実験され、良好な結果が得られており、本邦でも 独自に開発されたステントが基礎実験されている41、42)。 当初は良性狭窄に有用であると考案されたが、悪性胆道 狭窄に留置したmetallic stentが胆管炎や結石形成の原因 になることから、それらが生じる前に溶解・吸収されれ ばこのような合併症の発現を避けることができるので、 悪性病変にも応用可能であろう。 一方、現在のステント治療はその多くが悪性疾患を対 象にしていることから、抗癌剤投与や放射線治療などに よる抗腫瘍療法との併用療法が盛んに行われているが、 いまだ確立されていないのが現状である。現在、ステン トに薬剤を封入した薬剤溶出性ステント(drug eluting stent)が、vascular領域を中心に臨床応用されており、 non-vascular領域への応用も始まった43、44)。これらの新 しい発想のステントには今後大いに期待がかけられてい る。
経 皮 的 直 達 治 療( p e r c u t a n e o u s t u m o r
ablation:PTA)
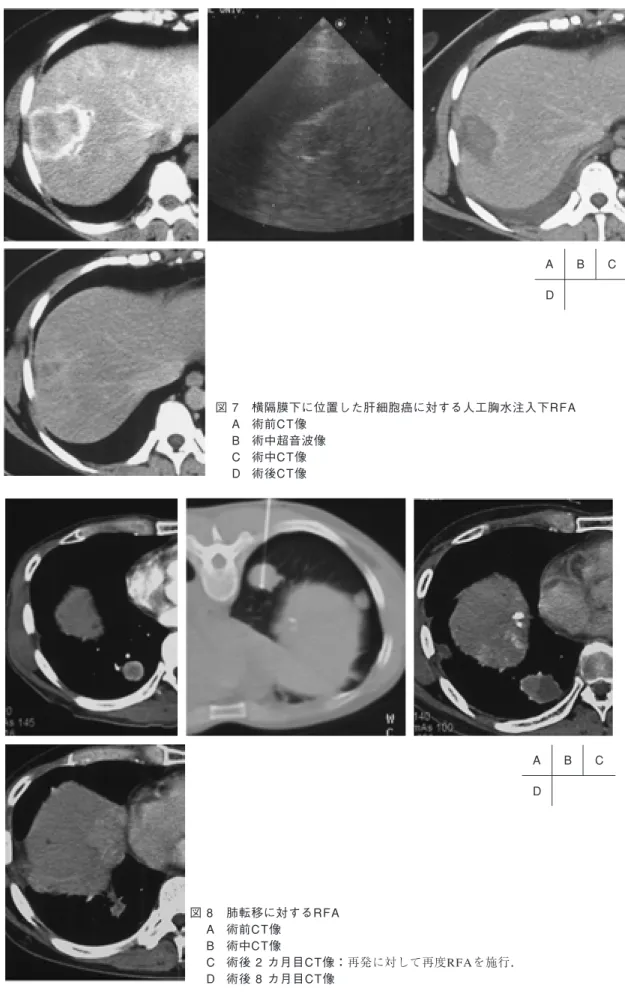
経皮的に直接腫瘍を穿刺し、腫瘍壊死に陥らせる手技 や治療法が、肝細胞癌や転移性肝癌を対象に始まり、治 療法の変革とともに肝以外の領域にもその応用を広げて 図 5 肺癌による気管狭窄に対するステント留置術 A 術前CT像 B 術後単純X線像 C 術後CT像 A B C いった。その発端となったのが、1980年代前半にエタ ノールの蛋白凝固ならびに脱水作用による腫瘍の壊死効 果を利用したPEITが本邦で考案され45)、世界中に広ま ったことである。しかし、エタノール自体の毒性から 1 回使用量が限定され、かつ血管内や胆管内への溢流によ る合併症も問題となった。これを解消するために沸騰し た生理的食塩水による熱凝固壊死効果を利用した熱湯局 注療法46)が新たに考案されたり、エタノールの代わりに 酢酸が用いられたりした47)。しかし、いずれの方法も液 体を用いるため、硬化型肝癌や転移性肝癌のように内部 に間質が多く含まれるような腫瘍などではその拡散が一 様でなく、治療効果が不十分になることが多かった。こ のため、液体を注入する方法ではなく、腫瘍部分を温め ることで腫瘍を壊死に陥らせようとする局所温熱療法と いう新しい治療法が生まれた。その代表的なものが PMCTとRFAである。PMCTはマイクロ波が水分子など 生体内の極性物質を振動させるため、極性物質同士が互 いに衝突しあって発する摩擦熱(誘電過熱)を利用したも のであり、RFAはラジオ波が体組織内の通過時に発生 するジュール熱を利用したものである。いずれも蛋白質 の凝固変性を引き起こすことで壊死に陥らせる。 肝腫瘍に関してはPEITは径 3cm以下で 3 個以内が対 象であったが、PMCT48、49)やRFA50、51)(図 6)では、径 3cm以下は同様であるが、個数や部位には制限がない。さらに、血流を遮断したり52、53)、生理的食塩水を注入 し先端を冷却する方法54)を併用したりすると凝固範囲を 広げることができるため、もう少し大きな腫瘍も対象と なっている。また、横隔膜下に存在し超音波で描出困難 な肝腫瘍へのアプローチの工夫として、人工気胸を作成 し胸腔内に生理的食塩水を注入する方法55)(図 7)も考案 された。これらの治療法は肝以外にも臨床応用されてい る。PEITでは甲状腺56)や副甲状腺57)、副腎腫瘍58)、リ ンパ節転移59)に、RFAでは肺癌60、61)(図 8)、腎癌62、63)、 副腎腫瘍64)、骨腫瘍65、66)、転移性骨腫瘍67)(図 9)などに 行われ、膵臓への応用も検討されている。
今後の展開
肝細胞癌に関しては、現時点では少なくともPEITは RFAやPMCTと比べるとやや劣っているようである68、69) が、今後は肝以外の領域も含めてこれら各治療法の淘汰 がなされ、それぞれの適応も確立されるであろう。その なかで最近、病変部を凍結させる新たな治療法(凍結治 療)が注目されている。凍結治療とは、超高圧の気体を 大 気 な ど の 低 圧 環 境 に さ ら す と 超 低 温 に な る J o u l e -Thomson効果を利用して、急激な温度低下と融解を繰 り返して局所の壊死を得る方法である。アルゴンガスで 凍結させ、ヘリウムガスで解凍する方法が一般的で、 −140˚Cから20˚Cまでの温度差を利用している。組織破壊 の機序は、① 細胞内の凍結によって生じる核偏位や細 胞膜の破壊、② 細胞外液の凍結によって生じる細胞内 外の浸透圧の変化、③ 播種性血管内凝固(disseminated intravascular coagulation:DIC)による0.5mm以下の微 細血管の塞栓である70)と考えられている。凍結治療の特 徴は、① 凍結による麻酔効果で術中の疼痛がない、② 疼痛の治療が可能である、③ 組織変性がないため副産 物を生成しない、④ ガス産生がないため塞栓の危険が ない、⑤ 凍結免疫がない、⑥ 画像モニタで治療範囲を 正確にモニターできる、⑦ 穿刺プローべは凍結により 強固に固着される、⑧ アイスボールは術中緩徐に形成 され、治療範囲が任意にデザインできることであり、 肝71–73)、腎74、75)、前立腺76、77)、子宮78、79)、肺80)などに臨 床応用されている。特に進んでいる肝腫瘍においては、 PMCTやRFAと比べて、治療範囲が画像でよく観察で き、3cm以上の肝癌に対しても治療可能で、流量の多い 血管に接している腫瘍でもその血管を入り江状に避けて アイスボールを形成するので根治的治療が期待できる点 で優れている。さらにこれらの治療のほかにレーザーや 収束超音波による治療法も登場してきた。レーザーによ る治療は子宮筋腫81)や、肝腫瘍82)、甲状腺腫瘍83)に応用 さ れ 、 収 束 超 音 波 は 子宮筋腫8 4 )のほか、脳8 5 )、前立 腺8 6 )、腎87)、肝、膀胱88)、乳腺腫瘍89)に臨床応用されつ 図 6 肝細胞癌に対するRFA A 術前CT像 B 術中CT像 C 術後CT像 A B C図 7 横隔膜下に位置した肝細胞癌に対する人工胸水注入下RFA A 術前CT像 B 術中超音波像 C 術中CT像 D 術後CT像 図 8 肺転移に対するRFA A 術前CT像 B 術中CT像 C 術後 2 カ月目CT像:再発に対して再度RFAを施行. D 術後 8 カ月目CT像 A B C D C A B C D C
つある。凍結治療やレーザー治療、収束超音波を用いた 治療はまだ始まったばかりであり、今後多くの症例を積 み重ねながら、その領域を広げていくであろう。それに 伴って適応や他の治療法との併用、使い分けなども明ら かとなろう。
消化管のIVR
1.経皮経食道胃管挿入術(percutaneous transeso-phageal gastro-tubing:PTEG) 従来用いられてきた経鼻胃管栄養法では、食道入口部 をチューブが通るため、嚥下時に違和感や疼痛を生じ、 チューブに痰が絡んで痰の喀出を困難にしたり、時には 重篤な肺炎を併発することもある。このため経皮的胃瘻 造設術が考案されたが、胃切除後症例などでは施行困難 なことから、次にこれに代わるものとしてPTEG90、91)が 考案された。PTEGは胃の手術の有無にかかわらず施行 可能なことから経皮的胃瘻造設術を凌駕しており、胃管 が必要なすべての患者に適応がある。本法の真の目的は 在宅医療への応用であり、中心静脈栄養に代わるものと して期待されている。 2.磁石圧迫吻合術(山内法) 2 つの磁石を用い、その磁力によって吻合したい臓器 を挟み込み、瘻孔を形成する方法92、93)で、胆管・十二 指腸、胃・小腸、小腸・大腸、大腸・大腸などの吻合形 成に応用されている。従来、開腹下にしか行えなかった 吻合形成をIVR手技で行えるようにしたことは画期的で あり、全身状態が不良な患者のQOL向上に大いに役立 つものと思われる。吻合部は縫合よりも滑らかに形成さ れるが、経過中再狭窄も生じる。本法の大きな問題点は 吻合形成に要する時間が少なくとも約10∼14日必要で あり、経口あるいは経肛門的に磁石を挿入しなければな らないので、磁石の大きさが限定されることである。今後の展開
現在のnon-vascular IVRは時代とともに結果が早く求 められる傾向にあるが、自然の流れに任せたところがあ る磁石圧迫吻合術(山内法)は、この流れに逆行してい る。したがって、この治療法が生き残れるか否かは、こ の逆行をも容認できるものと評価されるのか、またde-viceがどれぐらい早く市販されるかにかかっていると思 われる。画期的なIVRであるが、現時点でのnon-vascu-図 9 43歳・男性.肺癌からの腸骨転移に対するRFAA 右腸骨に溶骨性変化をきたした転移性腫瘤を認める.疼痛はvisual analogue scale score(VAS score)で術前8.0を示し歩行も困難であった.
B CT下にcool-tip針を穿刺し,RFAを施行した.
C 造影CTで腫瘤は濃染されず壊死に陥ったと考えられた.疼痛は術後 1 週間でVAS scoreが2.0ま で低下し,自立歩行が可能となった.
A B C D E C とで、椎体に加重がかかる悪性腫瘍の椎体転移94)や骨粗 鬆症95)などの圧迫骨折が原因である疼痛の軽減、椎体の 安定性が得られる経皮的椎体形成術(図10)が最も頻繁 に行われている。血管腫99)や骨髄腫、aneurysmal bone ことから、将来的には禁忌でなくなるだろう。局所治療 である本法が全身疾患である骨粗鬆症を適応とするには 異論もあり、今後の動向に注目したい。一方、本法は症 状緩和を中心とした治療法であり、原疾患である悪性病 図10 7 0 歳・男性.直腸癌から の椎体骨転移に対する経皮 的椎体形成術 A∼C CTで第 2,第 3 腰椎に溶骨 性 変 化 を 認 め , M R I で も C T に一致した部位に信号 変化を認め,椎体骨転移と 診断した.術前疼痛はVAS s c o r e で 8 . 0 と 高 度 で あ っ た. D,E C T 下に経皮的椎体形成術 を施行した.第 2 腰椎の病 変 に 対 し て 骨 セ メ ン ト を 1.5mL,第 3 腰椎病変に対 して2.0mLを注入した.術 後 2 日目にはVAS scoreは 2 . 0 まで低下し,鎮痛剤の 使用も不要となり,歩行可 能となった.
変に対しては放射線治療をはじめとして前述のpercuta-neous tumor ablation therapyなど、何らかの抗癌療法 が必要である。それにより効果の持続性や再発率の低 下、再発時期の遅延が図られる。そのなかで、佐野ら102) は磁力にて42˚C前後に発熱する骨セメントを開発して おり、放射線化学療法との併用で相乗効果が期待できる かもしれない。しかし、骨セメントによるショックは少 なからず発生しており、今後は骨セメントの安全性の向 上と確立が期待される。
経皮的レーザー椎間板ヘルニア減圧術
1987年にChoyら103)によって初めて報告された治療法 で、椎間板の髄核の水分をレーザーで蒸散させて椎間板 内圧を減圧し、神経根への圧排を軽減させて症状の改善 を得るもので、その改善率は極めて高率である。髄核の 蒸散と炭化を正確にモニタリングできるCT104)やMRガ イド105)下に行われる。適応は、① 急性・慢性を問わな い、② ヘルニアが後縦靱帯を越えない、③ ヘルニアが 原因で神経根症状を呈している、④ 保存的治療に抵抗 性、あるいはヘルニアを合併する脊椎管狭窄で、ヘルニ ア圧による神経根圧迫やそれに伴う循環障害による神経 根の浮腫に起因する症状発現が主たるものである。合併 症としては熱性、感染性椎間板炎や神経損傷が報告され ている。将来展望
このように1990年代以降におけるnon-vascular IVR の進歩は著しい。日本人の活躍もあって多くの新しい deviceや手技・治療法が開発され、確立されていった。 そして現在もますますその適応を拡大しつつある。IVR の特徴である低侵襲性は1990年代に入って強調される ようになり、今後はさらにdeviceの細径化が進むであろ うし、現在、多くの手技が穿刺をベースにしているが、 収束超音波のように穿刺しなくても治療ができる方向へ と進むことが予測される。また、術者の巧拙を問わず、 より正確に手技を行うための均質化、標準化が求められ るなかで、その対策のひとつとして、既に外科領域で応 用が始まっている医療ロボットが、このIVR106)の世界 にも導入されてくるであろう。このように、IVR手技・ 治療法が広がりをみせる一方で、術者や患者被曝が注目 されるようになっている。特にCT透視下のIVRが行わ れるようになり、それはより顕著となった。この術者や 患者被曝の低減に医療ロボットはその一助となるであろ うし、超音波と同様、全く被曝しないMRガイド下の IVRの発展にも拍車がかかるであろう。患者のQOLに ついてはP E I Tの登場を機に、悪性病変に対するn o n -vascular IVRの目的が一変した。従来は、その多くが姑 息的治療であったが、根治を目指した治療へ転じ、確固 たる地位を築いた。今後は現在注目を浴びつつある遺伝 子免疫療法1 0 7)や再生医療においても、n o n - v a s c u l a r IVRはその一翼を担うであろう。 国の医療費の貧窮や包括医療の影響もあろうが、今後 は患者のQOLをさらに向上させるために、入院期間の 短縮、外来ベースでの治療も進むに違いない。non-vas-cular IVRは今後も次々と新しい手技・治療法が開発さ れ、ますます発展していくであろう。 【参考文献】 1) 平松京一,打田日出夫編:Interventional radiology−放射 線診断技術の治療的応用.1987,金原出版,東京 2) Wallace MJ, Charnsangavej C, Ogawa K, et al:Tracheo-bronchial tree: expandable metallic stents used in experi-mental and clinical applications. Work in progress. Radi-ology 158: 309–312, 1986
3) Coons HG: Self-expanding stainless steel biliary stents. Radiology 170(3 Pt 2): 979–983, 1989
4) 前田宗宏,玉田俊明,幕谷士郎,ほか:消化管のステン ト.画像診断 3:309–314,1993
5) Song HY, Choi KC, Cho BH, et al: Esophagogastric neoplasms: Palliation with a modified gianturco stent. Radiology 180: 349–354, 1991
6) Raijman I, Siemens M, Marcon N: Use of an expandable Ultraflex stent in the treatment of malignant rectal stric-ture. Endoscopy 27: 273–276, 1995
7) Mainar A, Tejero E, Maynar M, et al: Colorectal obstruction: treatment with metallic stents. Radiology 198: 761–764, 1996 8) Saida Y, Sumiyama Y, Nagao J, et al: Stent endoprosthesis for obstructing colorectal cancers. Dis Colon Rectum 39: 552–555, 1996
9) Yoshioka T, Sakaguchi H, Yoshimura H, et al: Expandable metallic biliary endoprostheses: preliminary clinical evalu-ation. Radiology 177: 253–257, 1990
10) 森田荘二郎:胆道系悪性腫瘍におけるexpandable metallic stentsの有用性に関する臨床的検討.日本医放会誌 52: 623–640,1992
metal Z stentの有用性.Gastroenterol Endosc 36:1255– 1260,1994
16) 吉岡哲也,阪口 浩,松尾尚樹,ほか:胆道系における covered stentの基礎的研究.IVR会誌 12(suppl):112, 1997
17) Tanaka T, Maeda M, Uchida H, et al: Clinical results of t h e i n t e r n a l l y c o v e r e d s p i r a l Z s t e n t f o r m a l i g n a n t esophagogastric obstruction and the reduction of stent migration. J Vasc Interv Radiol 11: 771–776, 2000 18) 富田 優,廣田省三,松本真一,ほか:連結部を持たない
両面被覆covered stentの検討.IVR会誌 10:381–384,1995 19) Truong S, Bohndorf V, Geller H, et al: Self-expanding metal stents for palliation of malignant gastric outlet obstruction. Endoscopy 24: 433–435, 1992
20) Kozarek RA, Ball TJ, Patterson DJ: Metallic self-expand-ing stent application in the upper gastrointestinal tract: ca-veats and concerns. Gastrointest Endosc 38: 1–6, 1992 21) Lugmayr H, Pauer W: Self-expanding metal stents for
pal-liative treatment of malignant ureteral obstruction. AJR Am J Roentgenol 159: 1091–1094, 1992
22) Cantasdemir M, Kantarci F, Numan F, et al: Renal trans-plant ureteral stenosis: treatment by self-expanding metallic stent. Cardiovasc Intervent Radiol 26: 85–87, 2003 23) Gujral RB, Roy S, Baijal SS, et al: Treatment of recurrent
posterior and bulbar urethral strictures with expandable metallic stents. J Vasc Interv Radiol 6: 427–432, 1995 24) Song HY, Park H, Suh TS, et al: Recurrent traumatic
ure-thral strictures near the external sphincter: treatment with a covered, retrievable, expandable nitinol stent—initial re-sults. Radiology 226: 433–440, 2003
25) 永江浩史,伊藤寿樹,丸山哲史,ほか:前立腺肥大症およ び前立腺癌による排尿障害に対する尿道メタルステントの 治療効果.IVR会誌 19(suppl):5,2003
26) Ko GY, Song HY, Seo TS, et al: Obstruction of the lacri-mal system: treatment with a covered, retrievable, expand-able nitinol stent versus a lacrimal polyurethane stent. Radiology 227: 270–276, 2003
27) Maeda M, Timmermans HA, Uchida BT, et al: In vitro
metallic stentの開発.IVR会誌 19(suppl):31,2004 31) Do YS, Choo SW, Suh SW, et al: Malignant esophagogastric
junction obstruction: palliative treatment with an antireflux valve stent. J Vasc Interv Radiol 12: 647–651, 2001 32) Laasch HU, Marriott A, Wilbraham L, et al: Effectiveness
of open versus antireflux stents for palliation of distal esoph-ageal carcinoma and prevention of symptomatic gastroe-sophageal reflux. Radiology 225: 359–365, 2002 33) Laasch HU, Martin DF: Management of benign biliary
stric-tures. Cardiovasc Intervent Radiol 25: 457–466, 2002 34) Sandha GS, Marcon NE: Expandable metal stents for
be-nign esophageal obstruction. Gastrointest Endosc Clin N Am 9: 437–446, 1999
35) Paul L, Pinto I, Gomez H, et al: Metallic stents in the treat-ment of benign diseases of the colon: preliminary experi-ence in 10 cases. Radiology 223: 715–722, 2002 36) Fry SW, Fleischer DE: Management of a refractory benign
esophageal stricture with a new biodegradable stent. Gastrointest Endosc 45: 179–182, 1997
37) Korpela A, Aarnio P, Sariola H, et al: Comparison of tis-s u e r e a c t i o n tis-s i n t h e t r a c h e a l m u c o tis-s a tis-s u r r o u n d i n g a bioabsorbable and silicone airway stents. Ann Thorac Surg
66: 1772–1776, 1998
38) Korpela A, Aarnio P, Sariola H, et al: Bioabsorbable self-reinforced poly-L-lactide, metallic, and silicone stents in the management of experimental tracheal stenosis. Chest
115: 490–495, 1999
39) Robey TC, Valimaa T, Murphy HS, et al: Use of internal bioabsorbable PLGA“finger-type”stents in a rabbit tracheal reconstruction model. Arch Otolaryngol Head Neck Surg
126: 985–991, 2000
40) Petas A, Talja M, Tammela T, et al: A randomized study to compare biodegradable self-reinforced polyglycolic acid spiral stents to suprapubic and indwelling catheters after vi-sual laser ablation of the prostate. J Urol 157: 173–176, 1997 41) 田中豊彦,古川 顕,新田哲久,ほか:消化管用生体吸収
性ステントの開発.IVR会誌 17:237–239,2002 42) 山本清誠,吉岡哲也,古市欣也,ほか:胆道系における生
体吸収性ステントの基礎的研究.胆道 17:299,2003 43) Kalinowski M, Alfke H, Kleb B, et al: Paclitaxel inhibits
proliferation of cell lines responsible for metal stent obstruction: possible topical application in malignant bile duct obstructions. Invest Radiol 37: 399–404, 2002 44) 女澤慎一,本間久登:抗癌剤のdelivery systemとしての胆 管stenting.消化器内視鏡 15:1235–1239,2003 45) 杉浦信之,高良健二,大藤正雄,ほか:超音波映像下経皮 的腫瘍内エタノール注入による小肝細胞癌の治療.肝臓 24:920,1983 46) 本田伸行,打田日出夫:肝細胞癌に対する熱湯局注療法 (PHoT).IVR会誌 10:279–282,1995
47) Ohnishi K, Yoshioka H, Ito S, et al: Prospective random-ized controlled trial comparing percutaneous acetic acid injection and percutaneous ethanol injection for small hepa-tocellular carcinoma. Hepatology 27: 67–72, 1998 48) 内山正三,北川真一,仲野俊成,ほか:肝細胞癌に対する
エコーガイド下マイクロ波凝固療法(第 1 報).日本超音波 医学会講演論文集 56:123–124,1990
49) 松川哲也,山下康行,高橋睦正,ほか:PMCTの本邦での 展開.Radiology Frontier 3:121–126,2000
50) Rossi S, Fornari F, Buscarini L, et al: Percutaneous ultra-sound-guided radiofrequency electrocautery for the treat-ment of small hepatocellular carcinoma. J Intervent Radiol
8: 97–103, 1992
51) 椎名秀一朗,寺谷卓馬,小尾俊太郎,ほか:Cool-tip型電 極を用いた経皮的ラジオ波焼灼療法による肝細胞癌の治 療.肝臓 41:24–30,2000
52) Chinn SB, Lee FT Jr, Kennedy GD, et al: Effect of vascu-lar occlusion on radiofrequency ablation of the liver: re-sults in a porcine model. AJR Am J Roentgenol 176: 789– 795, 2001
53) Ishida T, Murakami T, Shibata T, et al: Percutaneous mi-crowave tumor coagulation for hepatocellular carcinomas with interruption of segmental hepatic blood flow. J Vasc Interv Radiol 13(2 Pt 1): 185–191, 2002
54) Livraghi T, Goldberg SN, Monti F, et al: Saline-enhanced radio-frequency tissue ablation in the treatment of liver metastases. Radiology 202: 205–210, 1997
55) S h i b a t a T , I i m u r o Y , I k a i I , e t a l : P e r c u t a n e o u s radiofrequency ablation therapy after intrathoracic saline solution infusion for liver tumor in the hepatic dome. J Vasc Interv Radiol 13: 313–315, 2002
56) Tarantino L, Giorgio A, Mariniello N, et al: Percutaneous ethanol injection of large autonomous hyperfunctioning thyroid nodules. Radiology 214: 143–148, 2000
57) 秦 康博,森下 哲,川村正喜,ほか:二次性副甲状腺機 能亢進症に対する経皮的エタノール注入療法(PEIT) .Ra-diology Frontier 3:133–138,2000
58) Shibata T, Maetani Y, Ametani F, et al: Percutaneous ethanol
injection for treatment of adrenal metastasis from hepato-cellular carcinoma. AJR Am J Roentgenol 174, 333–335, 2000
59) Lewis BD, Hay ID, Charboneau JW, et al: Percutaneous ethanol injection for treatment of cervical lymph node metastases in patients with papillary thyroid carcinoma. AJR Am J Roentgenol 178: 699–704, 2002 60) 安井光太郎,金沢 右,向井 敬,ほか:肺腫瘍に対する RF ablationの適応:これまでの経験より.IVR会誌 19 (suppl):11,2004 61) 松岡利幸,豊島正実,山本 晃,ほか:LeVeen針を用い た小肺癌のRFA:CTによる局所制御成績の評価.IVR会誌 19(suppl):11,2004
62) Gervais DA, McGovern FJ, Wood BJ, et al: Radio-frequency ablation of renal cell carcinoma: early clinical experience Radiology 217: 665–672, 2000
63) 高木治行,山門亨一郎,中塚豊真,ほか:経皮的腎ラジオ 波焼灼術の初期治療効果.IVR会誌 19(suppl):13,2004 64) 山門亨一郎,高木治行,明星匡郎,ほか:副腎腫瘍に対す るRFA:初期治療経験.IVR会誌 19(suppl):12,2004 65) Woertler K, Vestring T, Boettner F, et al: Osteoid osteoma:
CT-guided percutaneous radiofrequency ablation and follow-up in 47 patients. J Vasc Interv Radiol 12: 717–722, 2001 66) Erickson JK, Rosenthal DI, Zaleske DJ, et al: Primary treat-ment of chondroblastoma with percutaneous radio-frequency heat ablation: report of three cases. Radiology 221: 463– 468, 2001
67) 小島博之,谷川 昇,狩谷秀治,ほか:有痛性転移性骨腫 瘍に対する経皮的ラジオ波焼灼術の初期成績.IVR会誌 19 (suppl):14,2004
68) Shibata T, Iimuro Y, Yamamoto Y, et al: Small hepatocel-lular carcinoma: comparison of radio-frequency ablation and percutaneous microwave coagulation therapy. Radiol-ogy 223: 331–337, 2002
69) Lencioni RA, Allgaier HP, Cioni D, et al: Small hepato-cellular carcinoma in cirrhosis: randomized comparison of radio-frequency thermal ablation versus percutaneous etha-nol injection. Radiology 228: 235–240, 2003
70) G a g e A A , B a u s t J : M e c h a n i s m s o f t i s s u e i n j u r y i n cryosurgery. Cryobiology 37: 171–186, 1998 71) 若林 剛,田邊 稔,上田正和,ほか:エコーガイドによ る肝癌凍結融解壊死治療.IVR会誌 19:113–116,2004 72) 清水 匡,澤田明宏,児玉芳尚,ほか:MRIガイドによる 肝癌凍結治療.IVR会誌 19:122–126,2004
73) Ruers TJ, Joosten J, Jager GJ, et al: Long-term results of treating hepatic colorectal metastases with cryosurgery. Br J Surg 88: 844–849, 2001
74) 澤田明宏,清水 匡,児玉芳尚,ほか:腎癌に対するMRI ガイド下経皮的凍結治療.IVR会誌 19:133–138,2004 75) S h i n g l e t o n W B , S e w e l l P E J r : P e r c u t a n e o u s r e n a l
79) Sewell PE, Arriola RM, Robinette L, et al: Real-time I-MR-imaging—guided cryoablation of uterine fibroids. J Vasc Interv Radiol 12: 891–893, 2001
80) 中塚誠之,川村雅文,杉浦弘明,ほか:CT透視による肺 悪性腫瘍に対する凍結治療.IVR会誌 19:117–121,2004 81) Law P, Gedroyc WM, Regan L: Magnetic-resonance-guided percutaneous laser ablation of uterine fibroids. Lancet 354: 2049–2050, 1999
82) Pacella CM, Bizzarri G, Cecconi P, et al: Hepatocellular carcinoma: long-term results of combined treatment with l a s e r t h e r m a l a b l a t i o n a n d t r a n s c a t h e t e r a r t e r i a l chemoembolization. Radiology 219: 669–678, 2001 83) Dossing H, Bennedbaek FN, Karstrup S, et al: Benign
soli-tary solid cold thyroid nodules: US-guided interstitial la-ser photocoagulation—initial experience. Radiology 225: 53–57, 2002
84) Tempany CM, Stewart EA, McDannold N, et al: MR imag-ing-guided focused ultrasound surgery of uterine leiomyomas: a feasibility study. Radiology 226: 897–905, 2003 85) Heimburger RF: Ultrasound augmentation of central
ner-vous system tumor therapy. Indiana Med 78: 469–476, 1985 86) Foster RS, Bihrle R, Sanghvi NT, et al: High-intensity focused ultrasound in the treatment of prostatic disease. Eur Urol 23(suppl 1): 29–33, 1993
87) Vallancien G, Chartier-Kastler E, Bataille N, et al: Focused extracorporeal pyrotherapy. Eur Urol 23(suppl 1): 48–52, 1993 88) Visioli AG, Rivens IH, ter Haar GR, et al: Preliminary results of a phase I dose escalation clinical trial using fo-cused ultrasound in the treatment of localised tumours. Eur J Ultrasound 9: 11–18, 1999
89) Hynynen K, Pomeroy O, Smith DN, et al: MR imaging-guided focused ultrasound surgery of fibroadenomas in the breast: a feasibility study. Radiology 219: 176–185, 2001 90) Allen S Chen: Method and means for esophageal feeding. United States Patent. Washington, D.C. 1983, 4384584 91) 大石英人,笠井 恵,村田 順,ほか:経皮経頚部食道的 胃瘻造設術.その適応と有用性に関して.日外会誌 98: 471,1997 96) 上野真一郎,本郷哲央,浅井邦浩,ほか:骨盤骨への転移 に対する経皮的骨セメント局注療法の有用性.IVR会誌 17:33–38,2002
97) Cotten A, Deprez X, Migaud H, et al: Malignant acetabu-lar osteolyses: percutaneous injection of acrylic bone ce-ment. Radiology 197: 307–310, 1995
98) Weill A, Kobaiter H, Chiras J: Acetabulum malignancies: technique and impact on pain of percutaneous injection of acrylic surgical cement. Eur Radiol 8: 123–129, 1998 99) Galibert P, Deramond H, Rosat P, et al: Preliminary note
on the treatment of vertebral angioma by percutaneous acrylic vertebroplasty. Neurochirurgie 33: 166–168, 1987 1 0 0 ) G a i l l o u d P , M a r t i n J B , O l i v i A , e t a l : T r a n s o r a l vertebroplasty for a fractured C2 aneurysmal bone cyst. J Vasc Interv Radiol 13: 340–341, 2002
101) Appel NB, Gilula LA: Percutaneous vertebroplasty in p a t i e n t s w i t h s p i n a l c a n a l c o m p r o m i s e . A J R A m J Roentgenol 182: 947–951, 2004
102) 佐野哲也,竹上謙次,若林弘樹,ほか:セメント型発熱 材料を用いた実験的骨腫瘍に対する局所温熱療法の効 果.Orthop Ceramic Implants 17:49–52,1998 103) Choy DS, Ascher PW, Ranu HS, et al: Percutaneous
la-ser disc decompression. A new therapeutic modality. Spine
17: 949–956, 1992 104) 土肥美智子,原田潤太,福田国彦,ほか:CTガイド下経 皮的レーザー椎間板ヘルニア減圧術.IVR会誌 17:12– 16,2002 105) 橋本卓雄,寺尾 亨,石橋敏寛,ほか:MRガイド下経皮 的腰椎椎間板ヘルニア蒸散法.日磁医誌 18:98–107, 1998
106) Solomon SB, Patriciu A, Bohlman ME, et al: Robotically driven interventions: a method of using CT fluoroscopy without radiation exposure to the physician. Radiology
225: 277–282, 2002
107) Suh RD, Goldin JG, Wallace AB, et al: Metastatic renal cell carcinoma: CT-guided immunotherapy as a techni-cally feasible and safe approach to delivery of gene therapy for treatment. Radiology 231: 359–364, 2004