論文受理 2014年 4 月 23 日 Code Nos. 521 522
A Review of the Position Adopted by Patients When
Acquiring Images of the Base of the Hamate Hook
Shunsuke Takamatsu,1* Seiichirou Miyakawa,1 Hisaya Sato,2 Wataru Suzuki,3 Takeshi Nishizawa,4 Masami Nakamura,3 Hirotaka Umeda,3 Shogo Sai,3 Kyoichi Kato,2 Yasuo Nakazawa,2 and Jun Ikeda5
1
Department of Radiology, Showa University Hospital
2
Showa University Graduate School of Medical Health Care
3
Department of Radiology, Showa University Koto Toyosu Hospital
4
Department of Radiology, Showa University Fujigaoka Hospital
5
Department of Orthopaedic Surgery, Showa University School of Medicine
Received May 10, 2013; Revision accepted April 23, 2014 Code Nos. 521, 522
Summary
The hamate bone, one of the carpal (wrist) bones, has a large uncinate process protruding from the palm side. In sports such as golf and tennis, the hamate bone can break if is subjected to a high external force, such as from the handle of a racquet or club. At our hospital we take X-ray images of the hamate bone from two directions: an axial image through the carpal tunnel and an image at the base of the hamate hook (conven-tional method). While the conven(conven-tional method makes it easy to create images of the base of the hamate hook, the patient may suffer pain during image-taking because the hamate bone is pulled to cause radial flexion. We therefore investigated a method of imaging that would create three-dimensional computed tomography (3DCT) images of the base of the hamate hook in which the patient would only have to only rotate the wrist externally and elevate the forearm without any radial flexion. Our results suggest that it is possible to obtain images of the base of the hamate hook as clear as those acquired using the conventional method with the patient in a comfortable and painless position taking images at an external rotation angle of 50.3˚ and a fore-arm elevation angle of 20.3˚.
Key word: hamate hook
*Proceeding author 緖 言 有鉤骨は,掌側部から突き出した大型の鈎状突起に ちなんで名づけられた,手根骨を構成する骨の一つ1∼ 3) である.その役割は,手根管の尺側壁を形成している ため,有鉤骨鉤近傍を走行する尺骨神経・尺骨動脈を保 護し,短小指屈筋・小指対立筋の起始部として存在して いる4, 5). 有鉤骨という名前の由来にもなっている大きな鉤状 突起は,有鉤骨遠位尺掌側面から手掌に向かう約 1 cm の突起であり,ゴルフ,テニス,野球,バドミントンな どのスポーツにおいて,握っているグリップから直接有 鉤骨鉤に大きな外力がかかることで骨折することがあ る4, 6, 7). 有鉤骨骨折は体部骨折と鉤部骨折に分類される6). 体部骨折は,Milch の分類8)によると , 有鉤骨鉤の内 側で骨の尺側部を貫く骨折と,有鉤骨の上内側より下 外側に向かって常に斜めに走る骨折に大別される.体 部骨折の発生機序は,第 4,5 中手骨末梢から加わっ た長 軸 方 向の 外 力が 有 鉤 骨 遠 位関 節 面を介 達し, carpometacarpal関節脱臼骨折の形でみられることが多 1 昭和大学病院放射線室 2 昭和大学大学院保健医療学研究科 3 昭和大学江東豊洲病院放射線室 4 昭和大学藤が丘病院放射線室 5 昭和大学整形外科医学教室
い.それに対し,鉤骨折は手掌側に突出した鉤に外力 がかかることで発生する7∼ 9).Stark らは,有鉤骨鉤骨 折を認めた 62 例の内,75%にあたる 47 例が鉤基部も しくは鉤部近位 1/3 部分での骨折であると報告してい る10).そのため,有鉤骨鉤骨折の X 線診断において, 好発部位である近位 1/3 から基部までの描出が重要と なる. 現在,当院で実施している有鉤骨撮影は,手根管軸 位11)と有鉤骨鉤基部撮影12)(以下,従来法)の二方向で ある.従来法は手関節側面の状態から,有鉤骨が描出 できるように手関節を橈屈し,中心 X 線を垂直に入射 して撮影を行っている(Fig. 1).従来法では有鉤骨鉤基 部の描出に優れる一方で,橈屈位を取ることで,有鉤 骨がけん引されるため,患者に疼痛を強いる場合があ る.そこで,今回われわれは,橈屈位をとらない状態で 有鉤骨鉤基部の描出が可能か検討したので報告する. 1.方 法 1-1 使用機器 X 線 computed tomography(CT)装 置 は GE 横 河 メ デ ィ カ ル 社 製 Hi speed Nx/i お よ び SIEMENS 社 製 Sensation64を使用した.診断用 X 線装置は,東芝メ ディカルシステムズ社製 KXO 50F,X 線画像処理装置 は,アミン社製 ZIO STATION を使用した.X 線受光 系として,Carestream 社製 CR850 と富士フイルムメ ディカル社製 SPEEDIA CS を使用した. 1-2 撮影肢位の検討 手関節を橈尺屈させず,村上の報告13)や,古川の報 告4)に準じて,外旋と前腕挙上のみで有鉤骨鉤基部を描 出できる撮影肢位を,three-dimensional(3D)CT画像を 用いて検討した. 使用したデータは,当院倫理委員会の承認を得た, 手関節 CT 検査を撮影した患者 27 症例である.症例の 内訳は,男性 15 症例,17∼85 歳で平均年齢は 55 歳, 女性 12 症例,20∼89 歳で平均年齢は 63 歳であった. なお,手根骨全域に変形や転位のみられる関節リウマ チや骨折の患者は除外した.CT 検査時の撮影肢位は, 腹臥位の状態で検側上肢の肘を伸展させ検側手掌面を 下に向け,前腕軸と中指が寝台軸と平行になる肢位と した.撮影条件は 120 kV,effective mA second(mAs) 150,slice 厚 0.75 mm,ヘリカルピッチ 0.8 である.再 構成関数は B30 medium smooth を使用した. 今回,新しい撮影肢位を検討するため,3DCT 画像 を用い,有鉤骨鉤基部が最も明瞭に描出される外旋角 度 A と,前腕挙上角度 B を求めた.外旋角度 A の計 測方法は,3DCT 画像を橈尺骨が重なった側面の状態 にし,そこから 1 度ずつ 90 度まで外旋し,有鉤骨鉤基 部が最も明瞭に描出される角度とした.前腕挙上角度 Bは,橈尺骨が重なった側面の状態にし,1 度ずつ 90 度まで前腕挙上を行い,有鉤骨鉤基部が豆状骨と中手 骨から最も分離されている角度とした. 外旋角度 A と前腕挙上角度 B を組み合わせた撮影 肢位を新しい有鉤骨鉤基部撮影とした(Fig. 2). 1-3 臨床における従来法と新法の比較 当院の倫理委員会において,「有鉤骨鉤基部撮影の 臨床データ取得への御協力のお願い」と題する説明文書 をもとに,①研究の目的,②提供していただく画像デー タ,③画像データの採取方法,④画像データの使用方 法,⑤画像データ管理と保管,⑥画像データ提供に伴 う利益・不利益,⑦自由意思による同意と同意撤回の自 由,⑧研究への参加を断っても診療上の不利益は受け ないこと,⑨プライバシーの保護,⑩個人の解析結果 は原則的に開示しないこと,⑪研究に関わる費用,⑫研 究結果の公開,⑬知的財産権,⑭質問の自由,以上の
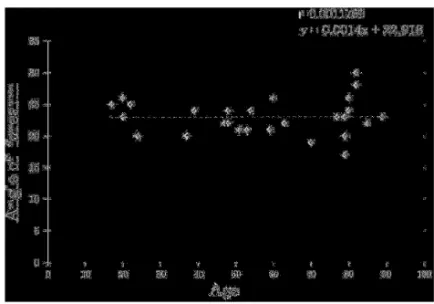
内容について承認を得た.そこで,上記の内容につい て同意が得られた患者 5 名を対象に,従来法と新しい 有鉤骨鉤基部撮影(新法)を行った.次に,撮影した有 鉤骨鉤基部画像の有鉤骨の描出能について視覚評価を 行った.視覚評価の観察者は,研究に対して賛同が得 られた経 験 年数 2 年,10 年,11 年,12 年,33 年の診 療放射線技師 5 名,整形外科医師 1 名である.なお, 観察者には,事前に視覚評価の結果の公表について承 諾を得た.視覚評価の項目は 1. 有鉤骨鉤は基部まで明 瞭に描出されているか,2. 有鉤骨と第 5 中手骨との重 なりはないか,3. 有鉤骨と豆状骨との重なりはないか, の 3 点とした.また,撮影を行った患者 5 名に対し,従 来法と新法の比較を行うために,アンケート調査を行っ た.調査項目は,1. 撮影時に痛みがあったか,2. 撮影 肢位の保持は容易であったか,3. 診療放射線技師から の撮影肢位の説明はわかり易かったか,の 3 点とした. 評価方法はいずれも,リッカート尺度法を用い,5 段階 評価とした. 2.結 果 2-1 3DCT画像を用いた撮影肢位について 3DCT より,有鉤骨鉤基部が最も明瞭に描出される外 旋角度 A は平均 50.3 度,標準偏差は 2.56 であった. 前腕挙上角度 B の平均値 23.0 度,標準偏差は 2.83 で あった.また,外旋角度 A および前腕挙上角度 B は, 年齢によって変化することはなかった(Fig. 3,4). 外旋角度 A を 50 度とし,前腕挙上角度 B を 23 度と した. a b
Fig. 2 External rotation angle “A” and forearm elevation angle “B”. (a) External rotation angle “A”
(b) Forearm elevation angle “B”
新法の概観を Fig. 5 に示す.
2-2 臨床における従来法と新法の比較
Fig. 6 に従来法と新法の X 線画像を,リッカート尺度 法によって得られた視覚評価の結果を Fig. 7∼9 に示
Fig. 5 Overview of the new technique.
(a) New technique showing a 50 degrees external rotation angle
(b) New technique showing a 23 degrees forearm elevation angle
a b
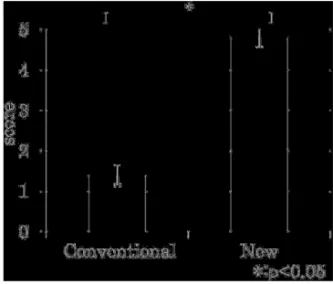
Fig. 6 Radiographic images. (a) Conventional technique (b) New technique す.新法は,従来法と比べ,有鉤骨鉤基部の描出能が 高い結果となり,有意差水準 5%で有意差が得られた (Fig. 7).また豆状骨との重なりに関して,従来法よりも 解消された結果が得られ,有意差水準 5%で有意差が 得られた(Fig. 8).しかし,中手骨との重なりに関して Fig. 7 Is the hamate hook including its base
clearly visualized?
Fig. 8 Are the hamate and the fi fth metacar-pal visualized without overlapping?
は新法よりも従来法が有鉤骨と重なりが解消される結 果となったが有意差はみられなかった(Fig. 9).また, アンケート調査では,回答者全員が,新法において痛 みが少なかったと回答した(Fig. 10).撮影肢位の保持 に関しても従来法と比較し,保持しやすいという結果が 得られた(Fig. 11).更に診療放射線技師による撮影肢 位の説明がわかり易いという結果が得られた(Fig. 12). すべてのアンケート項目において,有意差水準 5%で有 意差が得られた. 3.考 察 今回われわれが考案した新法は,骨折の好発部位で ある有鉤骨鉤基部の描出能に関して,従来法よりも描出 能が高いことを示す結果が得られた.その理由として, 撮影肢位の違いが大きく影響していると考えた.Fig. 13 に従来法と新法の volume rendering 像を示す.従来法 では,手掌の外旋をしないため,有鉤骨鉤基部が中手 骨近位部に重なって投影される.それに対し新法は, 手掌を 50 度外旋する肢位をとることで有鉤骨体部を中 手骨近位部から外して投影できるため有鉤骨鉤基部を 明瞭に描出することができたと考えられる. ところが,今回われわれが考案した新法の懸案事項 として,50 度外旋することによって有鉤骨が正確な側 面像として投影されていない可能性が考えられる.そこ で,3DCT 画像を用いて従来法と新法の撮影肢位を再 現し,有鉤骨の側面性について検証した.Fig. 14 は有 鉤骨鉤を遠位から見た図である.両者を比較すると従 来法(Fig. 14a)は有鉤骨鉤が垂直に投影されるが,新法 (Fig. 14b)は 50 度外旋して投影されることがわかった. 以上のことから従来法は有鉤骨鉤を正投影する一方 で,中手骨近位部が障害陰影となり,有鉤骨鉤基部の 描出が困難になる特徴がある.われわれの考案した新 法は,有鉤骨鉤が斜位像として投影されるが,有鉤骨 鉤を中手骨近位部から外して投影することが可能とな るため,有鉤骨鉤基部骨折や有鉤骨鉤部骨折に対して 有用な撮影法であると考えられる.
Fig. 9 Are the hamate and the pisiform bones visualized without overlapping?
Fig. 10 Did the patient experience pain during imaging?
Fig. 11 Was it easy to maintain the position during imaging?
Fig. 12 Was it easy to understand the clinical radiologist’s instructions on imaging position?
Fig. 13 Difference in projection image between the conventional technique and the new technique.
(a) A projection image obtained using the conventional technique (b) A projection image obtained using the new technique
a b
a b
Fig. 14 (a) Projective method using the conventional technique (b) Projective method using the new technique
今回検討を行った新法と従来法について,当院にお いて手の外科専門外来を行っている医師 3 名に意見を 求めたところ,画像は異なるが,特別大きな違和感は なく,診断 材 料として,十分 参 考になるとの見解で あった. 患者に対するアンケート調査から,新法は,撮影時 の痛みが少なく肢位保持が容易であり,診療放射線技 師からの撮影肢位の説明もわかり易いという結果が得ら れた.その理由として,新法は手の回外と拳上のみを 行う単純な撮影肢位が有効であったと考えられる.そ れに対し,従来法は,手関節を橈屈し母指を掌側外転 させる複雑な肢位をとる.通常,手関節を橈屈した場 合,母指は指背側を向くのが生理的な状態である.し かし,従来法の肢位は生理的に相反する複雑な運動で あるため,肢位の説明を受けてもわかりにくいと感じ, その肢位保持も困難であったと考える.その一方で, 新法は従来法よりも第 5 中手骨が有鉤骨に重なり易い 特徴があった.その理由として,新法においては橈屈を 行わないために有鉤骨を描出させる角度の許容範囲が 減少し,重なり易くなったと考えられる.有鉤骨と第 5 中手骨および豆状骨との重なりについて,3DCT を用 い,角度の許容について検証を行ったところ,23 度か ら±3 度の範囲であった.このことから,撮影保持の際 に生じる患者のわずかな動きによる設定角度の変化が 原因で重なりが生じる可能性がある. 4.結 語 今回われわれは,従来法で行っていた橈屈をとらず に有鉤骨鉤基部を描出する新法を検討した.新法は, 手関節側面の状態から外旋 50 度,前腕挙上 23 度で撮
参考文献 1)上羽康夫.深部解剖学.深部解剖学手その機能と解剖改 訂 5 版.金芳堂,京都,2010: 105. 2) F.H.マティーニ,M.J.ティモンズ,M.P.マッキンリ.カラー 人体解剖学.西村書店,東京,2004: 149. 3)鳥巣岳彦,国分正一,中村利孝,他編.標準整形外科学 第 9 版.医学書院,東京,1989: 1519-1526. 4)古川秀樹.有鉤骨鉤の役割に関する一考察.日本手の外科 学会雑誌 1991; 8(3): 573-576. 5)嶋田智明,平田総一郎.筋骨格系のキネシオロジー.医歯 薬出版,東京,2010: 187-202. 6)三木堯明.有鉤骨骨折.整形外科Reference 骨折と外傷 分類・診断基準・評価基準・定義改訂 2 版.金芳堂,京都, 2005: 1012-1013.
7)堀内行雄.CASE METHOD APPROACH. 整形外科専門医 を目指す CASE METHOD APPROACH 2.手の外科.日
本医事新報社,東京,2001: 72-77.
8) Milch H. Fracture of the hamate. J Bone Joint Surg1934; 16: 459-462.
9)茨木邦夫,斎藤英彦,吉津孝衛.各論I 外傷.手の外科診 療ハンドブック.南江堂,東京,2004: 145.
10) Stark HH, Chao EK, Zemal NP, et al. Fracture of the hook of the hamate, J Bone Joint Surg Am, 1989; 71(8): 1202 -1207. 11)鍵田政 雄.上肢 撮 影法.図説 単純X線 撮 影法.金 原出 版,東京,2002: 78. 12)松井宣夫.整形外科救急外傷の処置.整形外科救急外傷ハ ンドブック.メジカルビュー,東京,2002: 115. 13)村上恒二.有鉤骨鉤骨折における鉤部側面撮影法につい て.日本手の外科学会雑誌 1995; 12(1): 120-124. 問合先 〒 142-8666 品川区旗の台 1-5-8 昭和大学病院放射線室 髙松俊介