1
顎口腔領域疾患への先端的画像診断法の評価
Assessment of advanced imaging modalities for the maxillomandibular lesions
日本大学大学院松戸歯学研究科 放射線学
村松 輝晃
(指導: 金田 隆 教授)
2 1. Abstract
2. 要旨 3. 諸 言
4. 資料及び方法
4- 1. LEBLA-PXR を用いた、画像診断への新たなエックス線源としての評価
4- 2. MRI を用いた、歯周炎による下顎骨骨髄浮腫の検討
5. 結果
5- 1. LEBLA-PXR を用いた、画像診断 5- 2. 歯周炎による下顎骨骨髄浮腫 6. 考察
6- 1. 新しい単色エックス線の LEBLA-PXR の画像診断への可能性について 6- 2. 歯周炎と下顎骨骨髄浮腫の関係
6- 3. 歯周炎の画像診断法として MRI の有用性 7. まとめ
8. 参考文献 9. 図および表
3 Abstract
Currently, Parametric radiation-based X-ray (PXR), one of the pioneering modalities using
an accelerator, is being studied as a new kind of X-ray source in the Laboratory for Electron Beam
Research and Application (LEBRA). PXR is generated using a relatively small linear accelerator
(LINAC; 125 MeV) and a silicon crystal, with unique features that differ from conventional X-ray.
However, only a few experiments have been reported on the practical applications of PXR. On the
other hand, the clinical utility of the no radiation imaging modality will become increasingly
important for maxillomandibular lesion. Periodontitis is a highly prevalent chronic inflammatory
disease caused by oral infection of anaerobic gram-negative bacteria. A clinical diagnosis of
periodontitis is made by measuring alveolar bone loss on periodontal and radiological examination.
Mandibular bone mainly consists of cancellous bone and bone marrow. However, radiological
examination reveals only cortical bone resorption, and does not provide complete information
concerning the bony conditions, such as histopathological changes in the bone marrow. Evaluation
of bone marrow is critical for the diagnosis, treatment and prognosis of patients with various
diseases. However, there is little attention between periodontitis and bone marrow edema in the
mandible.
The purposes of this study were 1) to evaluate the potential of LEBRA-PXR as a new X-ray
source for diagnostic imaging, 2) to use MRI to investigate bone marrow edema caused by
4
periodontitis in the mandible and to assessment of advanced imaging modalities for the
maxillomandibular lesion.
1) Dog mandibular tissue with malignant melanoma was examined. Simple X-ray images
were taken with LEBRA-PXR at several wavelengths. An energy-subtracted image was generated
with the image with the longest wavelength PXR and the image with the shortest wavelength PXR.
As a control, an image was taken with conventional X-ray. The subject tissue was cut, hematoxylin
and eosin stained, and viewed with a microscope after X-ray examinations. Simple X-ray images
were taken with LEBRA-PXR, and the energy subtracted and conventional X-ray images were
compared with the histopathological findings.
2) 104 patients underwent MRI examination to evaluate brain and maxillofacial diseases as
outpatients at the Department of Radiology at our institution. The mandibular image was divided
into six regions. We classified signal intensity of mandibular bone marrows into five categories. A
total of 412 sites with periodontitis were evaluated on MRI. When bone marrow signal intensity was
higher than fat (low) signal intensity on short tau inversion recovery (STIR) MR imaging, it is
considered with presence of bone marrow edema.
1) Using the images of LEBRA-PXR, displays malignant tumors as differently contrasted from
those of conventional X-ray images. 2) Bone marrow abnormalities were observed in a high
percentage of MR images of mandible with periodontitis, suggesting that bone marrow edema is
5
caused by periodontitis in the mandible. The present study, these new imaging modalities suggested
that new possibilities as advanced imaging modalities for the assessment of maxillomandibular
lesions.
Key Words:
Advanced imaging modalities, Magnetic resonance imaging (MRI), Malignant tumor, Parametric
radiation-based X-ray (PXR), Periodontitis
6 要 旨
近年、臨床のエックス線とは異なる新しいタイプの電磁放射現象を用いた、エックス線
の一つとして単色エックス線のパラメトリックエックス線(Parametric radiation-based X-ray
(PXR))が注目され、新たな画像診断用エックス線源の研究が進められている。日本大学量
子科学研究所(Laboratory for Electron Beam Research and Application (LEBRA))では、独自の
技術により、世界で唯一長時間の安定したパラメトリックエックス線(LEBRA-PXR)を発
生させることに成功した。しかしながら、PXR に関する医療応用の研究は世界でも非常に
乏しい。また、顎口腔領域の疾患に対してエックス線を利用しない画像診断法および診断
装置の臨床的有用性は益々高まっている。歯周炎は歯肉の炎症と歯槽骨の吸収を主徴候と
する疾患であり、日常臨床にて主に歯周病検査とエックス線検査で歯周炎の検出がなされ
ている。しかしながら、顎骨内部には骨髄が存在するが、顎骨骨髄が歯周炎によりどのよ
うに反応するかはいまだ報告されていない。全身の筋骨格系では、骨髄の画像化にMRIが
有用とされ、そのうち悪性腫瘍や全身疾患等の重大疾患に随伴する骨髄浮腫はMRIの信号
異常として観察される。しかしながら、歯周炎と顎骨骨髄浮腫との関係についての検討は
いまだみられない。そこで本研究では1) 新たなエックス線源として LEBLA-PXRの画像
診断への可能性を評価し、2)エックス線を用いない歯周炎の診断装置として、被曝のない
MRI 検査を用い、歯周炎による下顎骨骨髄浮腫について検討し、顎口腔領域疾患への先端
的画像診断法の評価を行うことを目的とした。
7
PXRの研究は悪性黒色腫に罹患した犬下顎骨を対象とし評価した。LEBRA-PXRの線
源を用いて単純エックス線検査を施行し、そこで得られたエネルギーサブトラクション画
像、従来法エックス線画像および組織病理学的所見を比較検討した。エネルギーサブトラ
クション画像は、LEBRA-PXRを用いて異なる条件の波長で撮影し、これらの最長波長およ
び最短波長のPXR画像から生成した。撮影後、対象組織にHematoxylin-Eosin重染色を施行
し、顕微鏡下で観察を行った。MRIを用いた歯周炎の下顎骨骨髄浮腫の検討は、2006 年8 月
から2012 年8 月までに、本学付属病院で脳ドックのためにMRI検査を施行した104 例の
下顎骨を左右の前歯部、小臼歯部および大臼歯部に分け、歯周炎と臨床診断された412 部
位を対象とした。また、対象を① 歯槽骨吸収および4 mm以上のプロービングポケット深
さ(Probing pocket depth (PPD))がみられた、② 歯槽骨吸収およびプロービング時の出血
(Bleeding on probing (BOP))がみられた、③ 歯槽骨吸収、4 mm以上のPPDおよびBOP
がみられた、④ 歯槽骨吸収のみがみられた部位の4 パターンに分け、それぞれのブロック
でMRI Short tau inversion recovery 法画像での骨髄信号強度を評価した。信号強度は、脳脊
髄液の高信号、筋肉の中信号、脂肪の低信号を基準とし、さらに中~高信号、低~中信号
を加えた計5 段階評価を行い、低信号を正常骨髄、低信号より高い信号強度を呈した場合
を骨髄浮腫として評価した。
本検討により、単波長の LEBRA-PXR は従来のエックス線源よりも悪性腫瘍検出や進展
範囲の画像診断に有用と示唆された。また、MRI にて歯周炎患者の下顎骨骨髄に骨髄浮腫
8
が高率にみられ、エックス線を用いない新しい歯周炎の診断法としてMRIの有用性が示唆
された。これら新しい画像検査装置は顎口腔領域疾患への先端的画像診断法の新たな可能
性を示した。
キーワード:
先端的画像診断法、磁気共鳴画像検査法(MRI)、悪性腫瘍、パラメトリックエックス線、
歯周炎
9 諸 言
1895 年に Wilhelm Conrad Röntgen によって発見されたエックス線が医学に応用されて
100 年以上経過した。その間、顎口腔領域を含む全身の臓器や器官の疾病の診断や治療に
エックス線は不可欠なものとなり、現代の臨床医学はエックス線なしにはありえないもの
となっている1, 2)。一方、コンピューターの進化と共にエックス線を利用しない磁場を用い
たMRI装置も様々な撮像方法が研究、報告されており、その画像診断法は進化を続けてい
る3-5)。
新しいタイプの電磁放射現象を用いた、臨床のエックス線とは異なるエックス線の一つ
として単色エックス線のパラメトリックエックス線(Parametric radiation-based X-ray (以下
PXR とする))が注目され、新たな画像診断用エックス線源の研究も進められている 6-9)。
Hamburgの European XFEL、Stanford のLELS、Tsukuba のKEK-PF、Harima のSpring 8等
の巨大な加速器を用いた、PXR に関する研究は以前から行われているが、PXR の発生は国
家規模の大施設が必要であるとされていた。一方、日本大学量子科学研究所(Laboratory for
Electron Beam Research and Application (以下LEBRAとする))では、独自の技術により、世
界で唯一長時間の安定したパラメトリックエックス線(LEBRA-PXR) を発生させること
に成功した10)。LEBRA-PXR は比較的小さな線形加速器 (LINAC; 125MeV) と従来のエ
ックス線とは異なり、シリコーン結晶を使用して発生が可能である。PXR は相対性理論が
適応され、光速に近い速さの荷電粒子が、結晶のような周期構造を持つ物質への入射時に
10
生じる電磁放射現象の一種でもある11)。こうして発生したLEBRA-PXR は、従来の臨床で
用いられているエックス線とは異なり、① 単色性、② 連続エネルギー可変性、③ 指向性
および④ 高コヒーレントという4つのユニークな特徴を持つが12, 13)、医療応用の研究は世
界でも非常に乏しい。
また、顎口腔領域の日常臨床において、頻用される歯周炎のエックス線検査は、主に口
内法エックス線検査やパノラマエックス線検査を用いて検出されるが、近年では、CT や歯
科用 CT が用いられることも増えてきている 14-16)。一方、顎骨内部には骨髄が存在してい
るが、それら組織が歯周炎でどのように反応するか、いまだ報告されていない。特に、全
身の筋骨格系の骨髄の画像診断は磁気共鳴画像検査法 (Magnetic resonance imaging (以下
MRIとする))が有用とされ、そのうち、骨髄浮腫は悪性腫瘍や全身疾患に随伴する様々な
状態で異常所見として観察される17-23)。しかしながら、MRI を用いた歯周炎と顎骨骨髄浮
腫との関係についての検討はいまだみられない。
そこで本研究は1) 新たなエックス線源としてLEBRA-PXR の画像診断への可能性を評
価し、2) エックス線を用いない歯周炎の診断装置として、被曝のないMRI検査を用い、
歯周炎による下顎骨骨髄浮腫について検討し、顎口腔領域疾患への先端的画像診断法の評
価を行うことを目的とした。
11 資料及び方法
本研究は、日本大学松戸歯学部倫理委員会 (EC12-009)によって承認を受けている。
1. LEBRA-PXR を用いた、画像診断への新たなエックス線源としての評価
LEBRA-PXR (Figs. 1, 2) を用いて単純エックス線検査にて撮影、単純エックス線検査お
よび得られたエネルギーサブトラクション画像所見を用いて、従来法エックス線画像所見
および病理組織所見の比較を行った。対象資料は悪性黒色腫に罹患した犬下顎骨を用いた。
LEBRA-PXRによる単純エックス線画像は、検出器にYCR21(ヨシダ)を用い、各波長(12
keV、15 keV、18 keV、21 keV、24 keV、27 keV、30 keV)で撮影し、各々従来のエックス
線検査と比較し評価した。また、画像処理を施したエネルギーサブトラクション画像は最
長波長と最短波長のPXR画像から生成した。また、比較対象は、検出器にFCR(フジメデ
ィカル)を使用し、従来のエックス線(40 kV、125 mA、40 msec≒21 keV)による単純エッ
クス線検査を施行した。撮影後、対象組織をHematoxylin-Eosin重染色(以下H.E.とする)
し、顕微鏡下で癌の進展範囲の観察も行った。
2. MRI を用いた歯周炎による下顎骨骨髄浮腫の検討
2006 年8 月から2012 年8 月までに、本学付属病院で脳ドックのためにMRI検査を施
行した104 名(男性52 名、女性52 名、年齢21-78 歳、平均年齢56.3 歳)の下顎骨を、
左右の前歯部、小臼歯部および大臼歯部に分け、歯周炎と臨床診断された 412 部位を対象
とした。なお、放射線治療の既往患者、全身疾患により下顎骨に影響がある患者、下顎骨
12
に腫瘍や嚢胞のある患者、金属アーチファクトにより下顎骨の読影が困難なものは対象か
ら除外した。
歯周炎の評価
評価項目は、歯槽骨吸収の有無、プロービングポケット深さ (Probing pocket depth (以下
PPDとする))、プロービング時の出血 (Bleeding on probing (以下BOPとする))の有無とした。
歯槽骨吸収の評価は、デジタルパノラマエックス線装置(Veraviewepocs; J. Morita, Kyoto,
Japan)を用いた。撮像条件は管電流1‐10 mA、60-80 kVとした。パノラマエックス線写真
上で骨吸収を認めたものを歯周炎と診断し、PPD は、歯周ポケットプローブ(ヒューフレ
ディ― CP11)を用いて測定し、3 mm以下または4 mm以上の2つに分けて評価した。BOP
はプロービング時の出血が有りまたは無しの2つに分けて評価した。
画像評価
MRI は 1.5 テスラー超伝導型(Intera Achieva 1.5T Nova; Philips Medical Systems, Best,
Netherlands)を使用し、頭部専用コイルを用いて撮像を行った。画像評価は過去の文献より
骨髄浮腫の評価が最適となる以下の撮像条件で得られた MRI Short tau inversion recovery
(以下STIRとする) 画像を用いた24)。繰り返し時間 (TR):2500 ms、エコー時間 (TE):
60 ms、反転時間 (TI):180 ms、スライス厚:6 mm、マトリックス:320×256、撮像範囲:
230×195.5、加算回数:1 回である。画像は下顎骨最大断面の体軸横断像を用いて、骨髄が
観察できるスライスの下顎骨を左右の前歯部、小臼歯部および大臼歯部の6 部位に分け(Fig.
13
3)、それぞれの部位の骨髄信号強度を評価した。信号強度は、過去の報告 24)より、脳脊髄
液を高信号、筋肉を中信号、脂肪を低信号として評価の基準とし、さらに中~高信号、低
~中信号を加えた 5 段階で評価を行い、低信号を正常骨髄、低信号より高い信号強度を呈
した場合を骨髄浮腫として評価した。MRI の画像評価は、2 人の歯科放射線専門医によっ
て個別に評価し、評価が分かれた場合は話し合いにより1つの評価とした。
統計解析
統計解析にはSPSS(SPSS Japan, Tokyo, Japan)を用い、下顎骨骨髄浮腫と歯周炎による
それぞれの臨床症状との関連に関してχ2検定を用いて検討した。検定においてはP値<0.01
を有意差判定の基準とした。
14 結 果
1. LEBRA-PXRを用いた画像診断
従来のエックス線画像と比較して、LEBRA-PXR 画像は波長を変化させることにより、
悪性黒色腫の進展範囲がより明確に判定された。特にエネルギーサブトラクション画像に
より、従来のエックス線検査とは異なる軟組織や骨の形態および骨構造に関する情報を得
ることができた。組織学的所見と比較すると、悪性腫瘍の LEBRA-PXR 画像は従来のエッ
クス線画像では不可能であった悪性腫瘍の軟組織の進展範囲も病理組織像に近似した進展
範囲像を呈した。(Fig. 4)
2. 歯周炎による下顎骨骨髄浮腫
結果をTable 1 に示す。歯周炎がみられた412 部位のうち365 部位 (88.6 %)に下顎骨
骨髄浮腫が認められた(Fig. 5)。歯槽骨吸収のみがみられた 107 部位において、84 部位
(78.5 %)で下顎骨骨髄浮腫が認められ、歯周炎で有意に骨髄浮腫がみられた(P < 0.01)。
歯槽骨吸収および BOP がみられた63 部位において、54 部位(85.7 %)で下顎骨骨髄浮腫
が認められ、有意に骨髄浮腫がみられた(P < 0.01)。特に歯槽骨吸収および4 mm以上の
PPD がみられた97 部位において、92 部位(94.8 %)で下顎骨骨髄浮腫が認められ、有意
に骨髄浮腫がみられた(P < 0.01)。 歯槽骨吸収、BOP および4 mm以上の PPD がみら
れた 145 部位において、135 部位(93.1 %)で下顎骨骨髄浮腫が認められ、有意に骨髄浮
腫がみられた(P < 0.01)。MR 画像により、歯周炎は下顎骨骨髄浮腫を高頻度に引き起こ
15 していた。
16 考 察
1. 新しい単色エックス線のLEBRA-PXR の画像診断への可能性について
LEBRA-PXR 画像は、波長を変えることにより従来のエックス線画像に比べて、悪性腫
瘍の軟組織と骨吸収像の組織学的な違いを描出することが可能であった。PXR は結晶内部
の電子運動によって生成され、放出された光子は結晶によって回析される。そして、その
放射強度は結晶構造に依存する。生成された PXR 放射角と電子ビームの入射角の関係は
Bragg’s 法の条件と類似する。エックス線エネルギーは電子の入射角によって定義されるた
め、PXR の波長は電子ビームの入射角を選択することで任意に決定することができる。
LEBRA-PXR はLINAC によってシリコーン結晶と加速電子の相互作用から生成され、その
放射線はパルス構造、マクロパルス構造、マイクロパルス構造を有している。LINAC によ
って生成されたPXR の短い露光時間は、人体への被曝による影響も減少させる可能性があ
る。この点が医療応用に向けた大きな利点であり、特に LEBRA-PXR 発生装置は特徴的な
二重結晶構造を持ち、PXR の放射方向を常に一定にすることが可能で、LEBRA-PXR に関
する実験設定も容易にしている 25-27)。また、その加速器の全長は 2 メートル程度であり、
数キロメートルという巨大な加速器研究所と比較すると非常にコンパクトで、病院に設置
することも可能なため、臨床応用の可能性も秘めている。
エックス線の波長はエックス線吸収構成要素の吸収係数に関するものであり、対象物に
異なる構成要素が含まれる場合、波長を変化させることで様々なコントラストを示した画
17
像を作り出すことが可能である。LEBRA-PXR はターゲットとなるシリコーン結晶を傾斜
させることにより、0.248 nm (5.0 keV) から0.034 nm (36.0 keV) までと広くエックス線の波
長を変化させることができる。そうして放出された放射線はほぼ完全な単色エックス線で
ある。異なる波長のエックス線を照射する方法で、単色エックス線の利点に関する生物医
学的研究が過去にも行われており、その有用性が示唆されている 28)。また、定量的な骨分
析において、単色エックス線は局所的な骨ミネラル含有量(BMC)や骨ミネラル密度(BMD)
の測定だけでなく、骨体のミネラル含有量検査にも有用であるとの報告もある29, 30)。
LEBRA-PXR がエックス線源として他の施設と比較し優れた点は、1) 小さなLINAC、小
さくて短いエックス線発生装置により、単色光の波長の揃ったエックス線を生成すること
ができること、2) 波長の変換が容易であること、3) エックス線照射方向が一定であるこ
と等が挙げられる。
現在、正確なエックス線検査や画像研究の応用のため、科学的根拠に基づいた、コンパ
クトで、位相が揃った、波長可変性の新たなエックス線源が望まれている。本検討から画
像診断のための新たなエックス線源として LEBRA-PXR の医療応用への可能性が示唆され
た。
2. 歯周炎と下顎骨骨髄浮腫の関係
本検討から、歯周炎患者の下顎骨骨髄では412 部位の内365 部位(88.6 %)と高率に下
顎骨骨髄浮腫が観察された。歯周炎は歯周病原細菌の感染によって起こる慢性炎症として
18
広く知られており、歯槽骨吸収の程度を口内法やパノラマエックス線検査で測定すること
が、臨床の 1 つの方法となっている 14-16)。一方、下顎骨は主に皮質骨、海綿骨および骨髄
によって構成されているが、従来のエックス線検査では結果として起きた皮質骨を主とす
る顎骨の吸収を観察することはできるが、内部骨髄の病理組織学的変化の把握は困難であ
る。一方で、全身の筋骨格系において骨髄の評価は、その診断、治療および予後の予測に
非常に重要で、様々な病態が骨髄にいくつかのパターンで病理組織学的変化を引き起こす
とされている18-23)。これら変化は、
reconversion、 marrow infiltration
またはreplacement、
myeloid depletion、 bone marrow edema
およびbone marrow ischemia
の5 群に分類することができ、そのうち骨髄浮腫は感染によって引き起こされると言われている 17)。歯周
炎は細菌感染症であることが広く知られ、本検討において、下顎骨骨髄に生じた骨髄浮腫
は歯周炎に由来するものと考えられた。
3. 歯周炎の画像診断法へのMRI の有用性
本検討は、歯周炎患者下顎骨骨髄の病理組織学的な変化を観察するためにMRI装置を利
用した。MRI は日常臨床において、様々な疾患の画像検査法として広く用いられ3-5)、撮像
方法により様々な特徴を持つ画像を作り出せる特徴をもつ。今回用いた脂肪抑制法の 1 つ
であるSTIR 法は骨髄炎の検出、炎症の進展範囲、腫瘍や炎症性疾患の術後再発等の検査に
有用であることが報告されており 17, 24)、とくに全身の骨髄の質的診断には欠かせないもの
である 31)。また、本検討で注目した骨髄浮腫に関しても、脂肪抑制法を用いることで観察
19
可能であるとの報告がある13-18)。本検討において評価した下顎骨骨髄は、20 歳を超えると
ほとんどの骨髄が赤色骨髄から黄色骨髄つまり脂肪髄に変化するとの報告がある 32, 33)。本
検討において、365 部位(88.6 %)の下顎骨骨髄が STIR 法にて浮腫の信号強度である低
~中信号以上の信号強度を呈し、47 部位(11.4 %)の骨髄は低信号を呈した。下顎骨骨髄
が正常であればすべてが黄色骨髄(脂肪髄)であるため、STIR 法にて低信号で描出される。
よって47 部位のみは正常な骨髄信号であったと評価できる。
骨髄の画像評価は、癌の転移や白血病などの血液疾患および筋骨格系の骨疾患などの診
断や治療効果判定に用いられる 13-18, 34)。骨髄浮腫は外傷や感染により引き起こされ、その
病態は慢性的な炎症を持った状態であると言われている 17)。顎口腔領域における慢性炎症
性疾患の歯周炎と全身との関係についても、心疾患や糖尿病などの全身疾患との関わりが
過去にも多く報告されている 35-42)。そのため、歯周炎罹患患者の下顎骨骨髄の病理組織学
的変化を理解することはとても重要である。今回の検討では、歯周炎患者の下顎骨骨髄に
骨髄浮腫が高率にみられた。このことからも、歯周炎の診断は従来のエックス線検査だけ
でなく、骨髄の状態を評価することも全身に関連する影響として重要な情報となり、その
診断法はMRI が有用であることが示唆された。
20 まとめ
本検討により、単波長の LEBRA-PXR は従来のエックス線源よりも悪性腫瘍の画像診断
に有用と示唆された。また、MRI にて歯周炎患者の下顎骨骨髄に骨髄浮腫が高率にみられ、
エックス線を用いない新しい歯周炎の診断法としてMRI の有用性が示唆された。これら新
しい画像検査装置は顎口腔領域疾患への先端的画像診断法の新たな可能性を示した。
21 参考文献
1. Lou L, Lagravere MO, Compton S, et al. Accuracy of measurements and reliability of landmark
identification with computed tomography (CT) techniques in the maxillofacial area: a
systematic review, Oral Surg Oral Med Oral Pathol Oral Radiol Endod, 104: 402-411, 2007.
2. De Vos W, Casselman J, Swennen GR. Cone-beam computerized tomography (CBCT) imaging
of the oral and maxillofacial region: a systematic review of the literature, Int J Oral Maxillofac
Surg, 38: 609-625, 2009.
3. Minami M, Kaneda T, Ozawa K, et al. Cystic lesions of the maxillomandibular region: MR
imaging distinction of odontogenic keratocysts and ameloblastomas from other cysts, American
Journal of Roentgenology, 166: 943-949, 1996.
4. Minami M, Kaneda T, Yamamoto H, et al. Ameloblastoma in the maxillomandibular region:
MR imaging, Radiology, 184: 389-393, 1992.
5. Yanagi Y, Asaumi J, Unetsubo T, et al. Usefulness of MRI and dynamic contrast-enhanced MRI
for differential diagnosis of simple bone cysts from true cysts in the jaw, Oral Surg Oral Med
Oral Pathol Oral Radiol Endod, 110: 364-369, 2010.
6. Feder R, Spiller E, Topalian J, et al. High-resolution soft x-ray microscopy, Science, 197:
259-260, 1977.
7. Kirz J, Sayre D. Soft x-ray microscopy of biological specimens; in Synchrotron Radiation
22
Research (Winick H, et al. ed): 277-322, Plenum Press, NewYork, 1980.
8. Suckewer S, Skinner CH. Soft x-ray lasers and their applications, Science, 247: 1553-1557,
1990.
9. Young L, Kanter EP, Krässig B, et al. Femtosecond electronic response of atoms to ultra-intense
X-rays, Nature, 466: 56-61, 2010.
10. Hayakawa Y. Parametric X-ray radiation and possibility of monochromatic X-ray source using
a linac, KURRI-KR, 43: 43-49, 2000.
11. Baryshevsky VG, Feranchuk ID. Parametric X-rays from ultrarelativistic electrons in a crystal:
theory and possibilities of practical utilization, J Physique, 44: 913-922, 1983.
12. Sones B, Danon Y, Block R. Production and application of a novel energy-tunable X-ray source
at the RPI LINAC, Nucl Instrum Methods Phys Res B, 261: 98-101, 2007.
13. Wilkins SW, Gureyev TE, Gao D, et al. Phase-contrast imaging using polychromatic hard
X-rays, Nature, 384: 335-338, 1996.
14. Socransky SS, Haffajee AD. The bacterial etiology of destructive periodontal disease: current
concepts, J Periodontol, 63: 322-331, 1992.
15. Liljenberg B, Lindhe J, Berglundh T, et al. Some microbiological, histopathological and
immunohistochemical characteristics of progressive periodontal disease, J Clin Periodontol, 21:
720-727, 1994.
23
16. Takei HH, Carranza FA. Clinical Diagnosis; in Carranza’s Clinical Periodontology, 11th Edition
(Newman MG, et al. ed): 341-358, Elsevier Saunders, St. Louis, 2012.
17. Vogler JB III, Murphy WA. Bone marrow imaging, Radiology, 168: 679-693, 1988.
18. Zanetti M, Bruder E, Romero J, et al. Bone marrow edema pattern in osteoarthritic knees:
correlation between MR imaging and histologic findings, Radiology, 215: 835-840, 2000.
19. Hayes CW, Conway WF, Daniel WW. MR imaging of bone marrow edema pattern: transient
osteoporosis, transient bone marrow edema syndrome, or osteonecrosis, Radiographics, 13:
1001-1011, 1993.
20. Vande Berg BE, Malghem JJ, Labaisse MA, et al. MR imaging of avascular necrosis and
transient marrow edema of the femoral head, Radiographics, 13: 501-520, 1993.
21. Reinus WR, Fischer KC, Ritter JH. Painful transient tibial edema, Radiology, 192: 195-199,
1994.
22. Lieberman JM, Gardner CL, Motta AO, et al. Prevalence of bone marrow signal abnormalities
observed in the temporomandibular joint using magnetic resonance imaging, J Oral Maxillofac
Surg, 54: 434-439, 1996.
23. Kijowski R, Stanton P, Fine J, et al. Subchondral bone marrow edema in patients with
degeneration of the articular cartilage of the knee joint, Radiology, 238: 943-949, 2006.
24. Lee K, Kaneda T, Mori S, et al. Magnetic resonance imaging of normal and osteomyelitis in the
24
mandible: Assessment of short inversion time inversion recovery sequence, Oral Surg Oral Med
Oral Pathol Radiol Endod, 96: 499-507, 2003.
25. Momose A, Takeda T, Itai Y, et al. Phase-contrast X-ray computed tomography for observing
biological soft tissues, Nature Medicine, 2: 473-475, 1996.
26. Shapiro D, Thibault P, Beetz T, et al. Biological imaging by soft X-ray diffraction microscopy,
Proc Natl Acad Sci, 102: 15343-15346, 2005.
27. Hayakawa Y, Sato I, Hayakawa K, et al. Simulations to the project of a PXR based X-ray
source composed of an electron linac and a double-crystal system, Nucl Instru Meth Phys Res B,
27: 32-40, 2004.
28. Clark GL. Medical, biological and industrial applications of monochromatic radiography and
microradiography, Radiology, 49: 483-495, 1947.
29. Nakada H, Sakae T, Suwa T, et al. Comparison between parametric X-ray and dental X-ray for
observing new bone formation in implant surroundings, Nihon Univ J Oral Sci, 31: 110-115,
2005.
30. Nakada H, Sakae T, Suwa T, et al. Observation of Newly Formed Bone Around Dental Implant
Using Parametric X-ray, Key Engineering Materials, 309-311: 31-34, 2006.
31. Kaneda T, Minami M, Ozawa K, et al. Magnetic resonance imaging of osteomyelitis in the
mandible: comparative study with other radiologic modalities, Oral Surg Oral Med Oral Pathol
25 Radiol Endod, 79: 634-640, 1995.
32. Kaneda T, Minami M, Ozawa K, et al. Magnetic resonance appearance of bone marrow in the
mandible at different ages, Oral Surg Oral Med Oral Pathol Radiol Endod, 82: 229-233, 1996.
33. Hashimoto M. The distribution of active marrow in the bones of normal adult, Kyushu J Med
Sci, 11: 103-111, 1960.
34. Chen BB, Hsu CY, Yu CW, et al. Dynamic contrast-enhanced MR imaging measurement of
vertebral bone marrow perfusion may be indicator of outcome of acute myeloid leukemia
patients in remission, Radiology, 258: 821-831, 2011.
35. Humphrey LL, Fu R, Buckley DI, et al. Periodontal disease and coronary heart disease
incidence: a systematic review and meta-analysis, J Gen Intern Med, 23: 2079-2086, 2008.
36. Scannapieco FA, Bush RB, Paju S. Associations between periodontal disease and risk for
atherosclerosis, cardiovascular disease, and stroke: a systematic review, Ann Periodontol, 8:
38-53, 2003.
37. Bryan RN, Manolio TA, Schertz LD, et al. A method for using MR to evaluate the effects of
cardiovascular disease on the brain: the cardiovascular health study, Am J Neuroradiol,
15:1625-1633, 1994.
38. Janket SJ, Baird AE, Chuang SK, et al. Meta-analysis of periodontal disease and risk of
coronary heart disease and stroke, Oral Surg Oral Med Oral Pathol Oral Radiol Endod, 95:
26 559-569, 2003.
39. Iacopino AM. Periodontitis and diabetes interrelationships: role of inflammation, Ann
Periodontol, 6: 125-137, 2001.
40. Scannapieco FA, Bush RB, Paju S. Periodontal disease as a risk factor for adverse pregnancy
outcomes: a systematic review, Ann Periodontol, 8: 70-78, 2003.
41. Scannapieco FA, Papandonatos GD, Dunford RG. Associations between oral conditions and
respiratory disease in a national sample survey population, Ann Periodontol, 3: 251-256, 1998.
42. von Wowern N, Klausen B, Kollerup G. Osteoporosis: a risk factor in periodontal disease, J
Periodontol, 65: 1134-1138, 1994.
27
Fig. 1 LEBRA-PXR Generator
The total length of the LEBRA-PXR generator is only 2 m in comparison with that of needed at the giant accelerator laboratories, being several hundred meters to several kilometers in size.
28
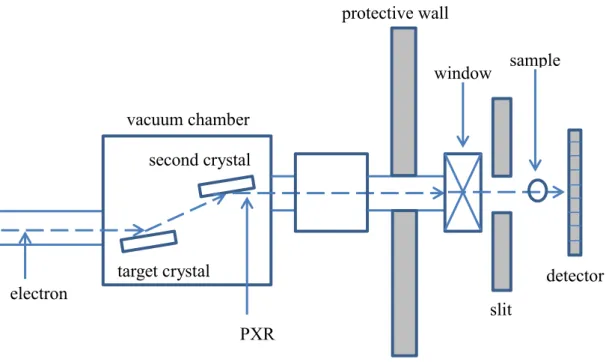
Fig. 2 Principle and generation of parametric X-rays
Parametric X-ray radiation is generated by the motion of electrons inside a crystal; the emitted photons are diffracted by the crystal, and the radiation intensity is critically dependent on the parameters of the crystal structure. The generated PXR radiation angle and the incident electron beam angle are the same, consistent with Braggʼs law. Because the wavelength, or X-ray energy, of the generated PXR is defined by the incident angle of the electrons, the PXR wavelength is arbitrarily determined by selecting the incident electron beam angle. The tunability of the X-ray wavelength has previously been possible only at giant accelerator laboratories.
sample
electron
window protective wall
vacuum chamber second crystal
target crystal detector
slit
PXR
29
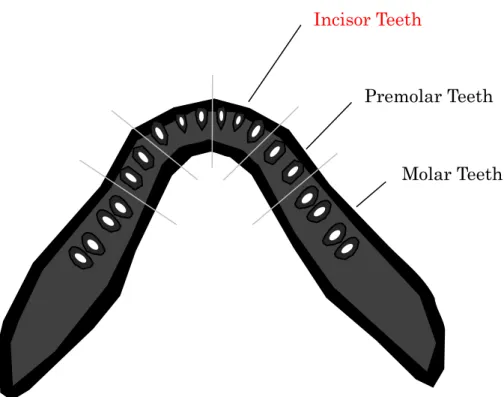
Fig. 3 Six mandibular regions evaluated in each participant on MRI.
Incisor Teeth
Premolar Teeth
Molar Teeth
30
Fig. 4 Conventional X-ray, LEBRA-PXR images, and histological findings of a dog melanoma specimen
Energy subtraction imaging with LEBRA-PXR offers more soft tissue and osteolytic bony image information related to morphology and structure. Comparing histological findings, the malignant tumor images with LEBRA-PXR are clearer than those of the conventional X-ray images.
Dual-Energy PXR image (H.E. ×10)
12 keV
Color mapped Dual-Energy PXR image
30 keV 27 keV
24 keV 21 keV
18 keV 15 keV
Simple X-ray image with conventional X-ray
source (42kV)
31
Fig. 5 Radiographic and MR images of 42-year-old woman with periodontitis.
Slight alveolar bone resorption (black arrows) and severe bone resorption (white arrows) are seen on panoramic radiograph of the mandible. However, the image provides no information about inner bone structures such as the bone marrow (A). Axial STIR image shows high signal intensity areas (arrow heads) in the mandible. This finding indicates histological changes in the bone marrow, such as bone marrow edema caused by periodontitis (B).
32
Table 1
Bone marrow edema prevalence, according to clinical signs of periodontitis (cases)
Bone marrow edema total P values
presence absence
Only alveolar bone loss 84(78.5%) 23(21.5%) 107 <0.01 Alveolar bone loss and BOP 54(85.7%) 9(14.3%) 63 <0.01 Alveolar bone loss and PPD 4 92(94.8%) 5(5.2%) 97 <0.01 Alveolar bone loss, PPD 4 and BOP 135(93.1%) 10(6.9%) 145 <0.01
total 365(88.6%) 47(11.4%) 412 <0.01
*BOP = bleeding on probing, PPD 4 = probing pocket depth is more than 4 mm. The percentage in parenthesis.