日集中医誌.2009;16:439~445.
東京医科歯科大学大学院循環制御内科学(〒113-8510 東京都文京区湯島1-5-45) 受付日2008年12月10日
採択日2008年12月31日 要約:心不全は,心臓のポンプ機能の低下とそれに基づく水分の体内貯留が本態である。最
近の臨床的観察から,心収縮機能低下を伴わない拡張機能障害によっても心不全が惹起され ることが明らかにされてきた。この病態は心不全症例の約40%を占め,予後は収縮不全症例 と変わらない。背景因子としては高血圧,糖尿病,肥満が重要である。また,高齢者や女性 に多く発症する。現在,救急搬送される心不全患者の多くが「拡張不全による心不全」になり つつある。従来,afterload mismatchとされてきた症例の多くが拡張不全であることが明らか となったためである。誘因として過剰な水分摂取が多い。急性期治療は収縮不全と大きく変 わるところはないが,利尿薬への反応はより速やかである。拡張機能の臨床的評価は,心エコー 法や組織ドプラーにより行われる。急性期治療の後に血圧の適正化,心房細動患者ではリズ ムあるいは心拍数のコントロール,適切な利尿薬の使用,虚血合併例では虚血の解除が行わ れる。急性期を脱した後の薬物治療に関しては,十分なエビデンスがあるとは言えない。
Key words: ①heart failure, ②ejection fraction, ③hypertension, ④diabetes mellitus,
⑤fibrosis
総 説
拡張不全による心不全
磯部 光章
Ⅰ.拡張不全による心不全とは
心不全は「心臓のポンプ機能の障害により体組織の 代謝に見合う十分な血液を供給できない病態」と定義 される。従来は心ポンプ機能のうち,駆出機能に焦点 が当てられ,収縮機能の低下が心不全の主体であると 漠然と考えられてきた。しかし,Senniらは心不全症 例の約40%では左室駆出率が保持されていること,さ らにその患者の生命予後は必ずしもよくないことを報 告した1)。その多くは拡張不全に起因した心ポンプ機 能障害と考えられている。
この病態は,“heart failure with preserved ejection fraction”,“diastolic heart failure”,“heart failure due to diastolic dysfunction”など,いくつかの名称で呼ば れる。“Preserved ejection fraction”とする場合も,
駆出率の定義は40%以上とすることもあり,決して収 縮機能が正常とは言えない症例も含まれる。従って
「駆出率の保たれた心不全」が必ずしも「拡張不全によ る心不全」を意味するものではない。さらに駆出率そ のものが心収縮機能のゴールドスタンダードではな く,その測定値も検出法によって異なることがあり,
定義としては曖昧である。また収縮機能の低下をきた す心臓は,多くの場合,拡張機能も障害されており,
その点では収縮機能障害による心不全と対立する概念 ではない。本邦では,この病態が「拡張期心不全」と呼 ばれることも多いが,病態の本質を必ずしも反映した 表記ではないとの考え方から,ここでは「拡張不全に よる心不全」とした。
左室駆出率が正常である心不全の病態は多岐にわた る。甲状腺機能亢進症,貧血,脚気衝心などの高心拍 出性心不全,心臓弁膜症,慢性肺疾患,肺動脈性肺高 血圧,収縮性心膜炎などが含まれるが,通常狭い意味 で「拡張不全による心不全」として議論されるのは,こ れらを除外して高血圧心や虚血性心疾患,肥大心に 伴って起きる拡張不全である。
Ⅱ.疫 学
「拡張不全による心不全」の発症頻度は不明である。
Owanらによれば,心不全のうち正常駆出率の割合は 増加の一途であり,低駆出率での発症数を凌駕する勢 いである(Fig. 1)2)。Tsutsuiらの統計では,本邦にお ける慢性心不全の入院患者の約4割,外来通院慢性心
不全患者の約7割が左室駆出率50%以上であったとし ている3)。我々の検討では,急性心不全の入院患者で も28%が左室駆出率50%以上であった4)。心不全発 症前の拡張機能障害患者はさらに多数にのぼることが 推測される。
「拡張不全による心不全」患者は,収縮不全による心 不全患者と比して高齢者に多いという特徴がある1)。
生理的に心臓の拡張機能が年齢とともに低下すること と関係していると思われる。性別では女性に多く,収 縮不全による心不全が男性に多いことと対照的であ る5)。また背景因子として高血圧,糖尿病,肥満の割 合が比較的高い(Table 1)6)。
「拡張不全による心不全」の生命予後についての調 査結果も報告されている7)。駆出率の保たれた心不全
Reduced EF r=−0.33,P=0.23 Preserved EF
r=0.81,P<0.001
r=0.92,P<0.001 250
70
60
50
40
30
20 0
1986 1990 1994 1998 2002
No. of admissions
Patients with preserved EF(%)
1986 1990 1994 1998 2002
200
150
100
50
0
(a) (b)
Fig. 1 Increased incidence of heart failure with preserved ejection fraction (from Owan TE, et al. NEJM 2006)2)
(a) Percentage of patients with heart failure who had preserved ejection fraction.
(b) Number of admission for heart failure with preserved ejection fraction.
EF, ejection fraction.
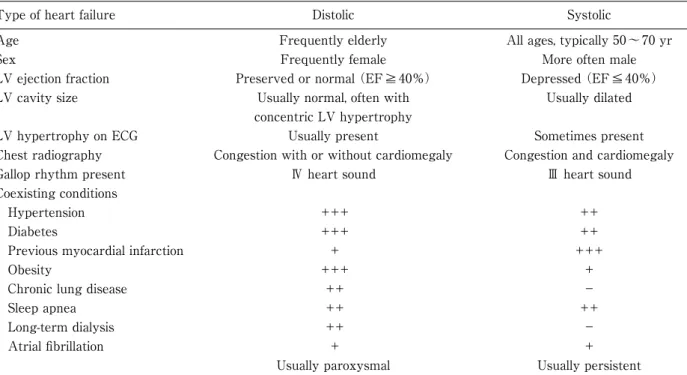
Table 1 Clinical characteristics of diastolic and systolic heart failure (from Jesseup M, et al. NEJM 2003)6)
Type of heart failure Distolic Systolic
Age Frequently elderly All ages, typically 50〜70 yr
Sex Frequently female More often male
LV ejection fraction Preserved or normal (EF≧40%) Depressed (EF≦40%)
LV cavity size Usually normal, often with Usually dilated
concentric LV hypertrophy
LV hypertrophy on ECG Usually present Sometimes present
Chest radiography Congestion with or without cardiomegaly Congestion and cardiomegaly
Gallop rhythm present Ⅳ heart sound Ⅲ heart sound
Coexisting conditions
Hypertension +++ ++
Diabetes +++ ++
Previous myocardial infarction + +++
Obesity +++ +
Chronic lung disease ++ -
Sleep apnea ++ ++
Long-term dialysis ++ -
Atrial fibrillation + +
Usually paroxysmal Usually persistent ECG, electrocardiogram; EF, ejection fraction; LV, left ventricular.
患者と低下した患者の生命予後については全く差がな いことが,Owanらによって報告されている2)。本邦 における我々のデータでは,収縮不全患者に比べて拡 張不全患者の予後は若干良好であった8)。心不全によ る再入院率も,6ヶ月〜1年の観察期間中,収縮不全,
拡張不全両患者で大きな差は認められない3),9)。収縮 不全患者では心不全死,不整脈死する頻度が高いのに 対して,拡張不全患者では心不全以外の心疾患や非心 血管疾患で死亡する率が比較的高い10)。
Ⅲ.病 態
拡張機能障害の基盤にあるのが,高血圧と糖尿病で ある。高血圧心では,左室肥大と心線維化を介して拡 張機能が低下する。糖尿病では,レニン–アンジオテ ンシン系賦活による心筋線維化や高血糖がもたらす心 筋細胞のCa過負荷を介して拡張機能障害が進行す
る11),12)。また基盤には,加齢に伴って進展する拡張
機能低下もある。病理学的な検討では,「拡張不全に よる心不全」では心臓のコラーゲン量の増加にかかわ らず心筋細胞径が増大していることが報告されてい る13),14)。
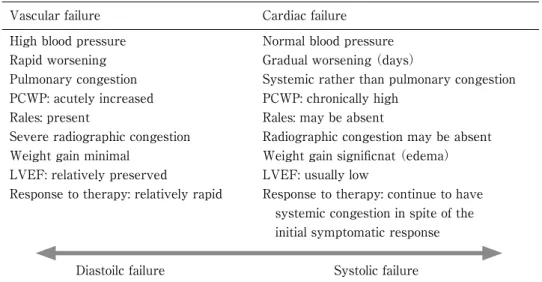
臨床的には,収縮不全による心不全と同様,急性 心不全,慢性心不全,慢性心不全の急性増悪の形態 をとる。Gheorghiadeらは,急性心不全をvascular failureとcardiac failureの2つの病型に大別している
(Table 2)15),16)。拡張不全による急性心不全は,血圧 上昇を伴い,急激に発症することが多く,肺うっ血が 強く,全身的なうっ血が少ないなど,vascular failure
の病像をとることが多い。心エコーでは,左室肥大が あり,心拡大は比較的少ない。利尿薬や血管拡張薬に よる治療に速やかに反応するのも,このタイプの心不 全の特徴である。左室のコンプライアンスが低下して いるため,比較的わずかな循環血漿量の増加に対応で きず,左室拡張末期圧が上昇し,容易に肺うっ血をき たすものと考えられる。従って,「拡張不全による心 不全」の増悪因子として,高血圧,頻拍,貧血,塩分過 負荷,心房細動などが特に重要である(Table 3)。
Table 2 Two types of acute decompensated heart failure (from Gheorghiade M, et al.)15),16)
Vascular failure Cardiac failure
High blood pressure Normal blood pressure Rapid worsening Gradual worsening (days)
Pulmonary congestion Systemic rather than pulmonary congestion PCWP: acutely increased PCWP: chronically high
Rales: present Rales: may be absent
Severe radiographic congestion Radiographic congestion may be absent Weight gain minimal Weight gain significnat (edema)
LVEF: relatively preserved LVEF: usually low
Response to therapy: relatively rapid Response to therapy: continue to have systemic congestion in spite of the initial symptomatic response
Diastoilc failure Systolic failure LVEF, left ventricular ejection fraction; PCWP, pulmonary capillary wedge pressure.
Table 3 Clinical characteristics of heart failure due to diastolic dysfunction
Characteristics of heart failure
– Acute decompensated heart failure ・Intolerability to water inbalance (narrow window)
・Unstable blood pressure ・Acute pulmonary congestion – Chronic heart failure (NYHA I〜IV)
Precipitative factors – Hypertension
– Atrial fibrillation, tachycardia – Sleep apnea
– Diabetes mellitus – High salt diet – Renal dysfunction – Obesity
– Myocardial ischemia – Anemia
– Iatrogenic (overhydration)
NYHA, New York Heart Association functional class.
Ⅳ.診 断
Vasanらが提唱している拡張不全の診断基準は,
①心不全症状・徴候の存在(胸部X線像,利尿薬への 反応など),②左室収縮機能が正常であることの客観 的な証拠(駆出率50%以上など),③左室拡張機能不
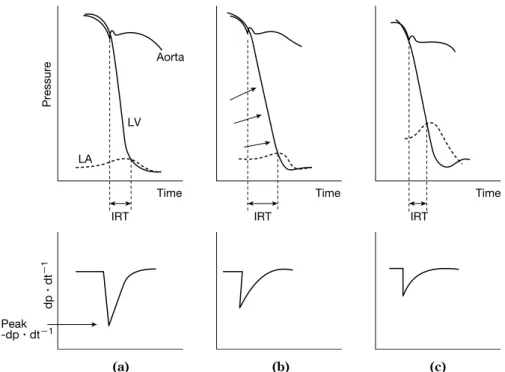
全の客観的な証拠,である(Table 4)17)。臨床的には 最後の項目の評価は容易でない。最も信頼がおける指 標は,左室圧,左房圧の同時記録による左室内圧の時 定数や変化率である(Fig. 2)。通常は心エコー・ドプ ラー検査を用いた拡張機能の評価が行われる18)〜20)。 拡張特性の変化に応じて僧帽弁口を通過する左室流入 血流速度が変化する。さらに組織ドプラー法を用いて,
Table 4 Diagnosis of diastolic dysfunction (from Vasan RS, et al. Circulation 2000)17) Possible DHF Probable DHF Definite DHF
Definitive evidence of CHF + + +
(Chest X-ray, response to diuretics)
Objective evidence of normal - + +
LV systolic function (EF≧50%)
Objective evidence of LV - - +
diastolic dysfunction
Reasons to upgrade diagnosis from possible DHF to probable DHF:
① Markedly elevated blood pressure during the episode of heart failure (SBP>160 mmHg or DBP>100 mmHg)
②Echocardiographic concentric LV hypertrophy without wall-motion abnormalities ③A tachyarrhythmia with a shortened diastolic filling period
④Precipitation of event by the infusion of a small amount of intravenous fluid
⑤ Clinical improvement in response to therapy directed at the cause of diastolic dysfunction (such as lowering blood pressure, reducing heart rate, or restoring the atrial booster mechanism)
CHF, congestive heart failure; DBP, diastolic blood pressure; DHF, diastolic heart failure; EF, ejection fraction; LV, left ventricular; SBP, systolic blood pressure.
Fig. 2 Time-dependent change of LV and LA pressure (top), and changing rate of LV pressure (bottom)
in diastolic dysfunction
(a) Normal intracardiac pressure curves and rate of LV pressure change.
(b) Decreased LV relaxation. The arrows show decline of LV pressure drop rate.
(c) Severe diastolic dysfunction. Marked increase in left atrial pressure.
IRT, isovolumic relaxation time; LA, left atrium; LV, left ventricle.
(a) (b) (c)
Pressure
LA LV
Aorta
IRT IRT IRT
dp・dt−1
Peak-dp・dt−1
Time Time Time
Mitral annular longitudinal tissue velocity
E/ADT(msec) IRT(msec) Em(cm・sec−1)
<1.0 250< 100<
<8 1.0〜2.0
150〜250 60〜100
8≦
<2.0
<150
<60
<8 1.0〜2.0
150〜250 60〜100
<8 Mitral
inflow velocity ECG
Em
IRT DT IRT DT IRT DT IRT DT
Em Em Em
Am Am Am Am
A
A
A
A E
Normal Abnormal
Relaxation Pseudo-
normalization Restriction
E
E E
Fig. 3 Progression of diastolic dysfunction and left ventricular inflow velocity (from Brum P, et al. JACC 1992)18) A, mitral inflow velocity in atrial contraction phase; Am, mitral annular longitudinal tissue velocity in atrial contraction phase; DT, deceleration time; E, mitral inflow velocity in early filling phase; ECG, electrocardio- gram; Em, mitral annular longitudinal tissue velocity in early filling phase; IRT, isovolumic relaxation time.
僧帽弁輪部の移動速度(Em,e’)や左室流入血流速度 のE波との比(E/e’)が,より信頼のおける指標として 日常的に用いられている(Fig. 3)18)。
血液マーカーとして血漿脳性ナトリウム利尿ペプチ ド値(brain natriuretic peptide, BNP)が上昇すること は,収縮不全による心不全と同様である21)。BNPの カットオフ値を62 pg・ml-1と,収縮不全による心不 全よりやや低値にとった方が,正診率が上がるとされ ている22)。
Ⅴ.治療と予防
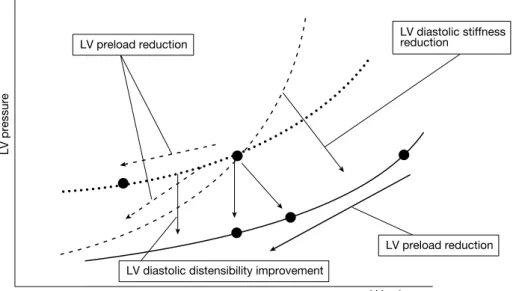
Fig. 4に示す圧容積関係からも推測できるように,
拡張不全による急性心不全における肺うっ血の改善に 必要なのは,左室前負荷の軽減であり,拡張不全によ る急性心不全の発症予防には左室拡張特性の改善が必 要である。
拡張不全による急性心不全発症時の対処は,基本的 に収縮不全による心不全と変わるところはない23),24)。 血行動態の把握と救急対応を進め,速やかに高血圧,
頻脈,体液過剰などの増悪因子の除去を試みる。「拡 張不全による心不全」では,前述のようにvascular failureタイプの急性心不全の病型をとることが多いた め,高血圧のコントロール,利尿薬やカルペリチドな どの血管拡張薬によるうっ血の軽減により,急速に症
状が軽減することが多い15)。拡張不全では左室充満 の心房収縮への依存度が特に高いことから,心房細動,
特に頻脈性心房細動では心拍数のコントロールが重要 である。可能な限り洞調律化することにより,再増悪 の予防を行う。
しかし,慢性期の治療方針は確立されていない。大 規模臨床試験に基づくエビデンスが少ないためであ る。アンジオテンシン変換酵素阻害薬25),アンジオテ ンシン受容体拮抗薬26),β遮断薬27)やスタチン28)の 有効性が期待されるところであるが,Candesartan in Heart Failure - Assessment of Mortality and Morbidity(CHARM)など多くの大規模臨床試験は,
「左室駆出率が40%以上である心不全」を対象として おり,必ずしも「拡張不全による心不全」を対象として いるわけではない。左室駆出率40〜50%は明らかに 収縮機能が低下していると考えられ,“preserved ejection fraction”とする根拠はない。
現状では,血圧コントロール,水分・塩分制限,心 房細動治療,貧血の改善,糖尿病のコントロールなど 増悪要因の治療・改善を行った上で,一般的な心不全 治療の経験をもとにした薬物治療が行われている。高 血圧,糖尿病,肥満が基盤となって起きることから,
生活習慣の改善は特に重要である。Meyerらは,長期 にわたりカロリー制限食を摂取することで,加齢に伴 う拡張機能障害が改善することを報告している29)。
Fig. 4 Relationship between LV pressure and volume in diastolic heart failure LV, left ventricular.
Ⅵ.今後の課題
「拡張不全による心不全」が心不全症例の約40%を 占めることが明らかにされたのは,比較的最近のこと である。臨床的特徴は徐々に明らかにされてきたが,
成因や治療についてはなお不明なことが多い。病態や 病因も多様であると考えられる。罹病率や死亡率も正 確なところは不明である。個々の患者の病態に即した 治療法の検討が待たれるところである。BNPの普及 は診断を容易にしてきたが,拡張機能そのものの評価 はなお困難であり,臨床的には,より簡便で正確な診 断法が確立されねばならない。
高齢化が進行する中で,「拡張不全による心不全」患 者は増加の一途をたどっている。一旦心不全を発症し た後の患者の生活の質は著しく制限され,多くは入退 院を繰り返して短時日のうちに不良な転帰をとる。今 後重要なことは,治療法の確立もさることながら,拡 張機能障害の予防である。加齢そのものにより年余に わたって進展する左室リモデリングは不可避である が,左室肥大や心筋梗塞の原因となる高血圧,動脈硬 化,メタボリック症候群を予防的に治療することが,
より切実な課題となっている。
文 献
1) Senni M, Tribouilloy CM, Rodeheffer RJ, et al. Congestive heart failure in the community: a study of all incident
cases in Olmsted County, Minnesota, in 1991. Circulation.
1998;98:2282-9.
2) Owan TE, Hodge DO, Herges RM, et al. Trends in preva- lence and outcome of heart failure with preserved ejection fraction. N Engl J Med. 2006;355:251-9.
3) Tsutsui H, Tsuchihashi M, Takeshita A. Mortality and readmission of hospitalized patients with congestive heart failure and preserved versus depressed systolic function. Am J Cardiol. 2001;88:530-3.
4) Konishi M, Maejima Y, Inagaki H, et al. Clinical charac- teristics of acute decompensated heart failure with rapid onset of symptoms. J Card Fail. 2009;15:300-4.
5) Owan TE, Redfield MM. Epidemiology of diastolic heart failure. Prog Cardiovasc Dis. 2005;47:320-32.
6) Jessup M, Brozena S. Heart failure. N Engl J Med.
2003;348:2007-18.
7) Redfield MM, Jacobsen SJ, Burnett JC Jr, et al. Burden of systolic and diastolic ventricular dysfunction in the community. JAMA. 2003;8:194-202.
8) Goda A, Yamashita T, Suzuki S, et al. Heart failure with preserved versus reduced left ventricular systolic function: A prospective cohort of Shinken Database 2004-5. in submission.
9) Dauterman KW, Massie BM, Gheorghiade M. Heart failure associated with preserved systolic function: a common and costly clinical entity. Am Heart J. 1998;135:
S310-9.
10) Curtis JP, Sokol SI, Wang Y, et al. The association of left ventricular ejection fraction, mortality, and cause of death in stable outpatients with heart failure. J Am Coll Cardiol.
2003;42:736-42.
11) Boyer JK, Thanigaraj S, Schechtman KB, et al.
Prevalence of ventricular diastolic dysfunction in asymp- tomatic, normotensive patients with diabetes mellitus.
Am J Cardiol. 2004;93:870-5.
12) Kirpichnikov H, Mcfarlane SI, Sowers JR, et al. Heart failure in diabetic patients: utility of blockade. J Card Fail.
2003;9:333-44.
13) Martos R, Baugh J, Ledwidge M, et al. Diastolic heart
LV pressure
LV preload reduction LV diastolic stiffness
reduction
LV diastolic distensibility improvement
LV preload reduction
LV volume
failure. Evidence of increased myocardial collagen turnover linked to diastolic dysfunction. Circulation.
2007;115:888-95.
14) van Heerbeek L, Borbely A, Niessen HWM, et al.
Myocardial structure and function differ in systolic and diastolic heart failure. Circulation. 2006;113:1966-73.
15) G h e o r g h i a d e M , L u c a L D , F o n a r o w G C , e t a l . Pathophysiologic targets in the early phase of acute heart failure syndromes. Am J Cardiol. 2005;96[Suppl]:11G-17G.
16) Gheorghiade M, Zannad F, Sopko G, et al. Acute heart failure syndrome: current state and framework for future research. Circulation. 2005;112:3958-68.
17) Vasan RS, Levy D. Defining diastolic heart failure: a call for standardized diagnostic criteria. Circulation. 2000;101:
2118-21.
18) Brun P, Tribouilloy C, Duval AM, et al. Left ventricular flow propagation during early filling is related to wall relaxation: a color M-mode Doppler analysis. J Am Coll Cardiol. 1992;20:420-32.
19) Oh JK, Hatle L, Tajik AJ, et al. Diastolic heart failure can be diagnosed by comprehensive two-dimentional and Doppler echocardiography. J Am Coll Cardiol. 2006;47:
500-6.
20) Kasner M, Westermann D, Steendijk P, et al. Utility of Doppler echocardiography and tissue Doppler imaging in the estimation of diastolic function in heart failure with normal ejection. A comprehensive Doppler-conductance catheterization study. Circulation. 2007;116:637-47.
21) Nakao S, Goda A, Yuba M, et al. Characterization of left ventricular filling abnormalities and its relation to elevated plasma brain natriuretic peptide level in acute
to chronic diastolic heart failure. Circ J. 2007;71:1412-7.
22) Maisel AS, Krishnaswamy P, Nowak RM, et al. Rapid measurement of B-Type natriuretic peptide in the emergency diagnosis of heart failure. N Engl J Med. 2002;
347:161-7.
23) 合同研究班(松㟢益徳班長).慢性心不全治療ガイドライン
(2005年 改 訂 版 ). 日 本 循 環 器 学 会 ホ ー ム ペ ー ジ.
Available from: http://www.j-circ.or.jp/guideline/pdf/
JCS2005_matsuzaki_h.pdf
24) 合同研究班(丸山幸夫班長).急性心不全治療ガイドライン
(2006年 改 訂 版 ). 日 本 循 環 器 学 会 ホ ー ム ペ ー ジ.
Available from: http://www.j-circ.or.jp/guideline/pdf/
JCS2006_maruyama_h.pdf
25) Cleland JGF, Tendera M, Adamus J, et al. The perindopril in elderly people with chronic heart failure (PEP-CHF) study. Eur Heart J. 2006;27:2338-45.
26) Yusuf S, Pfeffer MA, Swedberg K, et al. Effects of candesartan in patients with chronic heart failure and preserved left-ventricular ejection fraction: the CHARM- Preserved Trial. Lancet. 2003;262:777-81.
27) Flather MD, Shibata MC, Coats AJS. Randomized trial to determine the effect of nebivolol on mortality and cardio- vascular hospital admission in elderly patients with heart failure (SENIORS). Eur Heart J. 2005;26:215-25.
28) Fukuta H, Sane DC, Brucks S, et al. Statin therapy may be associated with lower mortality in patients with diastolic heart failure: a preliminary report. Circulation.
2005;112:357-63.
29) Meyer TE, Kovacs SJ, Ehsani AA, et al. Long-term caloric restriction ameliorates the decline in diastolic function in humans. J Am Coll Cardiol. 2006;47:398-402.
Abstract
Diastolic heart failure Mitsuaki Isobe
Department of Cardiovascular Medicine, Tokyo Medical and Dental University 1-5-45 Yushima, Bunkyo-ku, Tokyo 113-8510, Japan
In nearly 40% of heart failure patients, left ventricular ejection fraction is not impaired. Majority of them develop heart failure due to impaired left ventricular diastolic function. This disease has some clinical characteristics including elderly people, female dominancy, and quick response to diuretic therapy. Hypertension, diabetes, and obesity are more closely associated with diastolic heart failure. Recent investigation shows that prognosis of this kind of heart failure is as worse as heart failure with systolic dysfunction. Since treatment for this condition has not been established, conventional treatments for systolic heart failure are applied. The incidence of diastolic heart failure is increasing according to the increment of elderly population. Further investigation is needed to elucidate the pathophysiology and clinical management of diastolic heart failure.
Key words: ①heart failure, ②ejection fraction, ③hypertension, ④diabetes mellitus, ⑤fibrosis
J Jpn Soc Intensive Care Med. 2009;16:439〜445.