熊本大学薬学部附属育薬フロンティアセンター・
臨床薬理分野 平田純生
クイズ
です。
透析患者さんの
クレアチニン値
は低い方が予後が良い?
透析患者さんの
血清尿酸値
は低い方が予後が良い?
透析患者さんの
血清リン値
は低い方が予後が良い?
透析患者さんはリン吸着薬の服用量が少ない方が予後が
良い?
透析患者さんのBMI 40の超肥満患者よりも26の肥満患者
の方が予後が良い?
透析患者さんの
血清LDL値
は低い方が予後が良い?
透析患者は太っているほど長生きする
Kalantar-Zadeh, et al: Am J Clin Nutr 81: 534-554, 2005
一般人
透析患者
BMI(kg/m
2
)
3
2.5
2
1.5
1
0.5
相
対
的
死
亡
リ
ス
ク
0
>18
20
22
24
26
28
30
32
34
36
38
>40
Calle EE, et al NEJM, 1999
14年の調査
Leavey SF, et al: NDT, 2001
4年の調査
170cmなら115kg以上
1度肥満
1.60
1.28
1.05
1.00
0.00
0.50
1.00
1.50
2.00
<21.1
21.1~24.1 24.1~28.1
>28.1
+
+
透析患者は痩せているよりメタボ気味の方が長生きできる
相
対
的
死
亡
リ
ス
ク
Baseline BMI, kg/m
2
REF
Pifer TB, et al: Kidney Int 62: 2238-2245, 2002
+
+
+: P<0.001
慢性透析療法の現状
死
亡
リ
ス
ク
BMIの範囲
<16
0
0.5
1.0
1.5
2.0
日本透析医学会,図説 わが国の慢性透析療法の現況 2009年12月31日現在:69より作成
16~
18~
20~
22~
24~
26~
28≦
太っている
痩せている
マークなし :
* :
*** :
n.s.
p < 0.05
p < 0.0001
1.835***
1.414***
1.163***
対 照
0.907*
0.784***
0.881
0.894
圧
力
逆濾過
(back filtration)
透
析
液
流
入
正濾過
溶
質
除
去
水
分
除
去
高性能ダイアライザー内の圧力の変化
血液入口側
血液出口側
透析液入口側
透析液出口側
限外濾過に伴う水分・溶質の除去
逆濾過に伴う透析液の流入
(
エ
ン
ド
ト
キ
シ
ン
)
アミノ酸・水溶性ビタミン・カルニチン
CKD-MBD
慢性腎臓病に伴う
骨ミネラル代謝異常
透析前血清リン濃度のリスク(全死亡)
全
死
亡
の
リ
ス
ク
透析前血清リン濃度(mg/dl)
0
0.0
0.5
1.0
1.5
2.0
日本透析医学会,図説 わが国の慢性透析療法の現況 , 2004年12月31日現在 図表45より作成
3
4
5
6
7
8
9~
マークなし :
* :
n.s.
p < 0.05
2.20*
1.27*
1.00
対 照
0.92*
0.99
1.05
1.22*
1.57*
平均年齢は67.9歳
高齢化に伴う「やせ」
の問題が深刻に
透析患者数は32.5万人
高リン血症患者の生命予後
相
対
死
亡
リ
ス
ク
<3
3~4
4~5
5~6
6~7
7~8
8~9
>9 (mg/dL)
血清リン濃度
相対死亡リスク±95%信頼区間
(Reference)
2.2
2.0
1.8
1.6
1.4
1.2
1.0
0.8
0
透析患者における血清リン濃度と死亡リスク(海外データ)
【対 象】 北米のデータベースに登録された透析患者40,538例
【方 法】 血清リン濃度と死亡リスクの関連を解析、相対死亡リスクは年齢、性別、人種、糖尿病、アルブミンなどで補正
生存年数
(リスクのある患者数)
生
存
率
kestenbaum B, et al: JASN 16: 520-528, 2005
低リン値群
中間リン値群
高リン値群
eCCrに応じた血清リン値
CKD患者では血清リン値が高いほど生命予後が不良
生存率が低い
蛋白制限してリンを下げると
死亡リスクは上昇する
死亡率比
0.8
0.9
1.0
1.1
蛋白摂取量 ↑
血清リン濃度 ↑(基準)
蛋白摂取量 ↑
血清リン濃度 ↓
蛋白摂取量 ↓
血清リン濃度 ↑
蛋白摂取量 ↓
血清リン濃度 ↓
最小補正
Case-mix補正
Cox回帰モデル
死亡しやすい
長生きしやすい
蛋白摂取量が多くリンが
低い人は死亡リスクが低い
蛋白摂取が低くリンが高い人
の死亡リスクがかなり高い
蛋白摂取が少なくリンが
低い人は死亡リスク上昇
フレイル(Frailty)は介入により再び健常な状態に戻る
という可逆性が含まれる(老年医学会のステートメント)
Aging
(加齢)
疾患・ストレス
健康寿命
生物学的寿命
出典:長寿医療研究センター病院レター 第49号 虚弱(フレイル)の評価を診療の中に
http://www.ncgg.go.jp/hospital/pdf/news/Hospitalletter49.pdf
予備能力
要支援・要介護状態
要支援・要介護の
危険が高い状態
No Frailty
(健康)
Frailty
(虚弱)
Disability
(身体機能障害)
フレイル
サルコペニア
看取り
フレイルサイクル
Fried L.P et al: J Gerontology 56: M146-157, 2001を改変
慢性的な
低栄養
サルコペニア
筋力
低下
身体機能
低下
活動量
低下
エネルギー
消費量低下
食事量
低下
加齢に伴う
食欲不振
加齢に伴う
筋肉量低下
疾患
歯の
喪失
リン・カルシウム・PTHの目標値
リン
3.5~6.0mg/dL
補正カルシウム 8.4~10.0mg/dL
インタクトPTH
(whole PTH)
60~240pg/mL
35~150pg/mL
CKD-MBDの治療方針
第1にリンを上げない。
第2にCaを上げない。
最期にPTHを上げない
Lynch KE, et al: Clin J Am Soc Nephrol 6: 620-629, 2011
透析患者におけるリン制限と予後の関係
リン摂取処方量(mg/日)
周辺構造モデル
周辺構造モデル+摂取量
周辺構造モデル:年齢、性別、人種、透析方法、ブラッドアクセス、eKt/V、DM、CHF、動脈疾患、
血清アルブミン・Cr・Ca・P・PTH・VD、DW、三頭筋の厚さ、中腕周囲径、PCR、食欲、栄養サプリ
使用などで補正
リ
ン
制
限
な
し
制限なし
予
後
不
良
の
割
合
リン吸着薬
の量が少ない
リンの制限をせず
リン吸着薬を多く
飲んだ患者群
リ
ン
制
限
な
し
透析中のNepro摂取により血清アルブミン値
は早期に改善
2.0
2.5
3.0
3.5
4.0
4.5
0
1
2
3
4
5
6
S
e
rum
a
lbum
in,
g/
dL
(月)
P < 0.0001
2.0
3.0
4.0
5.0
6.0
7.0
Baseline
3ヶ月後
6カ月後
透析中のNepro
Ⓡ
摂取により栄養状態改善
SGA
score
N=85
N=49
N=39
*
*
P < 0.05 vs baseline.
エンシュアリキッド 1
缶
リーナレンMP
1
パック
リーナレンLP
1
パック
Nepro
1缶
液量
250mL
125mL
125mL
237 mL
カロリー
250kcal
200kcal
200kcal
427kcal
たん白質
8.8g
7.0g
2.0g
19.1g
リン
130mg
70mg
40mg
170mg
カリウム
370mg
60mg
60mg
250mg
カルシウム
130mg
60mg
60mg
250mg
ナトリウム
200mg
120mg
60mg
250mg
ビタミンC
38mg
10mg
10mg
25mg
亜鉛
3.75mg
1.5mg
1.5mg
6.4mg
Nepro
®
の組成
リン管理不良症例
から学んだこと
0
2
4
6
8
10
97
98
99
00
01
02
03
補正
Ca
P
2.0g夕
2.0g昼夕
3.0g
昼夕
1.5g昼夕
2.0g
1.5g昼夕
CaCO3
ガスター
20mg/日
20mgをHD後週3回
0
200
400
pg/mL
i
P
T
H
血
清
・
P
濃
度
Ca
mg/dL
血清リン値のコントロール不良の症例
僧房弁
置換術
内シャント
再手術
下肢切断
ワーファリン常用
オキサロール
小泉 晶子, 平田純生, 他: 日病薬誌 44: 1365-1368, 2008
リン吸着薬をいつ飲めばよいか理解できていない。
リンが高いとなぜよくないか理解できていない。
リン吸着薬の飲み忘れが最も多い。
外食時にリン吸着薬を持参しない人が最も多い。
理解度調査による血清リン値
7mg/dL以上群の特徴
リン吸着薬に関する指導不足・理解不足が高リン
血症を招いている可能性があるのでは?
患者指導用パンフレット
●血清リン値が高いと骨だけでなく、心臓や血管系に
悪影響を及ぼすこと。
●リン吸着薬は食事をしない時に飲んでも効果がな
いだけでなく、薬によっては異所性石灰化や鉄過剰
が起こることがある。食直前、食事中または食直後の
いずれかに飲まなければ効果がないこと。
●リン吸着薬はいつも携帯して、外食時やリンの多く
含まれる間食時にもきちんと服用すること。
リン吸着剤の正しいのみ方
リンの多く含まれる間食時にも
のんだ方がいいです。でも主治医
にはちゃんと報告してください。
1枚120mg
2枚204mg
100gで390mg
カルタン
Ⓡ
は空腹時に
飲んじゃダメです!
プロセスチーズ
50gで500mg
4.0
5.0
6.0
7.0
8.0
9.0
10.0
n=24
n=68
6.0~6.9mg/dL 7.0mg/dL≦
前
後
前
後
P<0.0001
P<0.05
血清リン濃度
(mg/dL
)
服薬指導前後の血清リン値の変化
30
40
50
60
70
80
90
n=24
n=68
6.0~6.9mg/dL
7.0mg/dL≦
前
後
前
後
P<0.0005
P<0.01
100
P<0.0001
前
後
n=120
5.0~5.9mg/dL
Calc
ium
-pho
spho
rus
produ
ct
(mg
2
/d
L
2
)
服薬指導前後のCa・P積の変化
リン吸着薬の安全性
について考えてみよう
炭酸Ca投与量と石灰化スコア
(echoによる)
石灰化スコア
g/日
n=120
Guerin AP, et al: Nephrol Dial Transplant 15: 1014-1021,2000を改変
0
0.5
1.0
1.5
2.0
0
1
2
3
4
Ca
投
与
量
炭
酸
2.5
3.0
石灰化スコア : 0
0
20
40
60
80
0.25
0.50
0.75
1
石灰化スコア : 1
石灰化スコア : 2
石灰化スコア : 3
石灰化スコア : 4
生
存
率
(月)
0
Blacher J, et al : Hypertension. 38:938,2001より引用
27%
50%
69%
83%
97%
冠動脈石灰化スコア別生存率
リン吸着薬の効力比と服用時間
1.0gの効力 = 2gの効力
=3gの効力
カルタン
フォスブロック
レナジェル
ピートル
リオナ
キックリン
1
1
1.5 1.5
3
ホスレノール
3
食直前
食直前
食直前
食直後
食直後
食直後
あまり使われていない250mg錠
各種リン吸着薬
カルタン
Ⓡ
安価・消化器系副作用少ない
保存期に使いやすい
石灰化の助長
胃内pHの影響
レナジェル
Ⓡ
フォスブロック
Ⓡ
石灰化抑制
脂質代謝改善
便秘
アシドーシス
・腹部膨満
ホスレノール
Ⓡ
作用が強力
石灰化抑制?
嘔気・嘔吐
臓器蓄積・憩室炎?
利点
欠点
リン吸着薬
キックリン
Ⓡ
腹部膨満なし
アシドーシスなし
石灰化抑制?
軽度便秘
カプセルが大きい
リオナ
Ⓡ
石灰化抑制?
鉄補給の必要なし?
鉄過剰?
ピートル
Ⓡ
作用が強力
下痢
石灰化抑制?
33
カルタン錠
500mg
レナジェル錠
250mg
レナジェル錠
750mg
これが腹部膨満の原因?
~セベラマーの膨潤性~
リン吸着剤の正しいのみ方
リンの多く含まれる間食時にも
のんだ方がいいです。でも主治医
にはちゃんと報告してください。
1枚120mg
2枚204mg
100gで390mg
カルタン
Ⓡ
は空腹時に飲んではいけない
薬です!(低Ca血症時のCa補給を除く)
プロセスチーズ
50gで500mg
ホスレノール
®
は重金属だから怖い?
重金属とは鉄以上の比重を持つ金属の総称であり、水銀、
ヒ素、鉛、カドミウムなど人体に蓄積し、重度の障害を起こ
すイメージが強いが、TPNで投与しなければならない必須
元素の亜鉛、銅、マンガンも重金属。
脳内に移行するというデータはおそらく間違い
であり、肝臓
内濃度は高いが胆汁排泄されるための通り道に過ぎず
肝障害もおこさない。ただし
骨内濃度は年々上昇
し、6年間
以降の安全性は証明されていない。
0~40mg/kgのLaCl
3
を6か月間経口
投与したラットのLaの脳内分布
SRXRF: Synchrotron Radiation
X-ray Fluorescence
Feng L, et al: Toxicology Letters 165 (2006) 112–120
8日間のMorris water maze test の
平均逃避潜時(たどり着く時間)
Haratake J, et al: Am J Surg Pathol 39: 767-771, 2015
胃前庭部粘膜のLa沈着による多発性の不規則な浸食
活動性消化性潰瘍,潰瘍性大腸炎,クローン病,
腸管狭窄のある患者[本剤の主な副作用は消化
器症状のため,これらの疾患に影響を及ぼすお
それがある.](慎重投与)
腸管憩室のある患者[腸管穿孔を起こした例が
報告されている.](慎重投与)
ホスレノール
®
の体内動態
Behets GJ et al.: J Am Soc Nephrol. 2004; 15: 2219
尿中排泄率
0.6~1.8%
排泄されたLaの97%が
糞便中排泄(ラット)
胆汁排泄
消化管吸収
<0.0012%
炭酸La
経口投与
吸収率:0.0013%
(Alは0.01~0.1%)
ほとんど吸収されない
血漿蛋白結合:99.7%以上、
毒性を示す遊離型濃度は
測定できないくらい低い
Hutchison AJ, et al:Nephron Clin Pract 110:c15-c23, 2008
Hutchinton AJ: Kidney Int 75: 355-357, 2009
脳には移行しない
Semin Dial
19:195-199, 2006
経口投与では、いかなる動物
実験でも肝内濃度は蓄積しない
1年間投与のHD患者34人の骨濃度
1.8µg/g 、4-5年間投与のHD患者13
人の骨濃度は5µg/g湿重量と
骨への蓄積が懸念される
Fe
2+
+H
2
O
2
→Fe
3+
+HO
-
+
HO・
(Fenton反応
)
ヒドロキシルラジカルは、存在するのは100万分の1秒間と寿命が
短いが、酸化力は強く、酵素蛋白質や細胞骨格蛋白質、脂質、糖質、
核酸(DNA、RNA)、などと反応する。
鉄原子は細胞毒
であり、肝細胞内でも、またマクロファージ
内でも、毒性が発現しないように鉄結合性蛋白である
フェリチンと結合した形態で貯えられている。
透析患者では静脈回路があるため静注鉄剤投与が一般的
だが、ガイドラインに推奨されている週1回13回投与法は
毎透析後13回連続投与に比し酸化ストレスが軽減される。
リオナ・ピートルは鉄剤だから怖い?
~怖いのは静注鉄~
静注鉄よりはるかに安全でフェリチンが300ng/mL以上に
なれば中止・減量すればよい。
健常者
静注鉄非投与透析患者
静注鉄投与透析患者
Nonmercaptalbumin
(disulfide form:酸化型)
nonmercaptalbumin
(oxidized form:酸化型)
静注鉄投与により酸化アルブミンが有意に上昇
Anraku M, et al: Kidney Int (2004) 66, 841–848
毎透析後にフェジン40mgを4週間投与
タール便と鉄剤やリオナ
Ⓡ
、ピートル
Ⓡ
投与による黒色便は違う
タール便
胃・食道などの上部消化管で大量出血を起こすと胃液と
混ざり、胆汁に含まれるビリルビンの影響で黒くなって
タール便と呼ばれるものになって排泄される。タール便
は
コールタール状の便で、海苔の佃煮のようなドロッと
した形状で鉄のにおいがあり生臭く、便器に付くとなか
なか流れない
のが特徴。消化管から出血した便がなる。
血便は胃酸の影響のない十二指腸以下の出血による。
黒色便
鉄剤やリオナ
Ⓡ
投与や海苔、イカスミによる黒色
便は通常便が単に便の色が黒色に着色したもの。
透析患者の
この数値は?
2014年末の統計調査
男性181人(1.0%)
女性129人(1.2%)
透析患者の腸閉塞による年間死亡者
透析患者の死亡原因病名リストには「腸閉
塞」しかないが、透析患者の致死性腸病変は
腸閉塞だけでなく、虚血性腸炎、腸管穿孔、
腸管壊死など様々。これらの病変に続発する
腹膜炎や敗血症は感染症に分類されるかも?
少なくとも
独立変数
オッズ比
95%信頼区間
P
値
透析方法(HD, CAPD)
2.10
0.80~5.49
0.1311
性別(女性、男性)
1.83
1.01~3.32
0.0460
年齢(歳)
1.07
1.04~1.10
<0.0001
透析歴(月)
1.00
1.00~1.00
0.3637
原疾患(DM, nonDM)
2.25
1.12~4.54
0.0235
CaCO
3
服用者
1.51
0.47~4.84
0.4899
カリメート服用者
2.44
0.98~6.10
0.0555
便秘に影響する因子
(多重ロジスティック回帰分析)
R
2
= 0.143
西原 舞, 平田純生, 他:透析会誌37: 1887-1892, 2004.
年齢
年齢と便秘の割合
~49
N=34
50~59
N=44
60~69
N=91
70~79
N=58
80~
N=8
0
20
40
60
80
100
%
18%
46%
54%
67%
88%
P
= 0.0098
P
= 0.0003
P
< 0.0001
P
< 0.0001
西原 舞, 平田純生, 他:透析会誌37: 1887-1892, 2004
2010年国民生活基礎調査より作成.
1.0
4.0
1.4
4.1
3.0
5.9
8.1
9.8
12.5
11.9
症 例1
年齢:63歳、女性、透析歴:2年5ヶ月
投薬歴
カリメート
®
20g 分4×28日/月
CaCO
3
2g 分2×30日/月
リン酸ジヒドロコデイン
1g 分3×12日/月
下剤の投与なし
原病歴
平成8年11月1日透析終了1時間後より腹痛が発現
し、痛みは次第に増強。嘔吐も発現する。緊急入院し
腹部X線上free air(遊離ガス)を認め、開腹手術とな
る。下行結腸に穿孔を認め穿孔部にカリメート
®
と思わ
れる
堅固な便塊を認めた。
手術後回復。
筆本真由美, 平田純生, 他: 大阪透析研究会会誌, 15: 179-181, 1997
手術症例の便塊の性状
(我々の報告)
筆本真由美, 平田純生, 他: 大阪透析研究会誌15:179-181, 1997
年齢:63歳、女性、透析歴:2年5ヶ月、平成8年11月1日透析終了1時間後よ
り腹痛が発現
樹脂を含む多量の黄白色便塊
(Ca型resin 20g/日+リン酸ジヒドロコデイン1g/日+CaCO
3
2g/日投与、下剤の
投与なし)
年齢:65歳、女性、透析歴:3年7ヶ月、平成3年10月19日透析中便意を催し、
排便中に、冷や汗、強度の腹痛が発現
直腸後壁穿孔部に多量の堅固な便塊(最大直径7cm)
(Ca型resin 20g/日+CaCO
3
2g/日投与、下剤の投与なし)
年齢:51歳、男性、透析歴:7年8ヶ月、原疾患:DM、平成8年10月31日20時頃、
食事摂取1時間後に嘔吐が発現し、疼痛緩和したが、翌日再び腹痛が増強し緊
急手術
上行結腸に堅固な便塊(最大直径5cm)
(Ca型resin 20g/日+CaCO
3
3g/日投与、下剤の投与なし)
中毒性巨大結腸症
手術症例の便塊の性状
固形の便塊
(水酸化Alとケイキサレートの併用)
Minford EJ, et al: Postgrad Med J
68: 302, 1992
イオン交換樹脂を
含む2Kgの硬い便塊
(
Ca型resin 15~30g/日を経口投与
)
Foresti V: Clin Nephrol
41(4): 252, 1994
(モルヒネ、水酸化Al、ケイキサレートの併用)
多量の白く硬い便塊
Gracia-Pard G, et al: Nephrol
Dial Transplant 11(4): 751, 1996
樹脂を含む硬い便塊
(
Ca型resin 50g×2/日を注腸投与
)
.
Chatelain G, et al:
Ann Diagn Pathol
11:217-219, 2007
樹脂を含む硬い便塊
(
Ca型resin 50g×2/日を注腸投与
)
Courtney, et al: N Engl J Med
288(20): 1058-9, 1973
S状結腸に結晶を認める
(
Ca型resin を経口投与したPD患者
)
Kao CC, et al: J Formos Med Assoc
pii: S0929-6646(13)00091-0, 2013
0
10
20
30
40
50
虚血性腸炎発症群
(n=15)
対照群
(n=692)
P <0.0001
服
用
患
者
の
割
合
(
%
)
陽イオン交換樹脂製剤服用患者の割合
西原 舞, 平田純生, 他:透析会誌38: 1279-1283, 2005.
透析患者における虚血性腸炎(穿孔)の発症因子1
虚血性腸炎群
(n=15)
対照群
(n=692)
P値
陽イオン交換樹脂製剤
の服用患者(%)
46.7
9.1
<0.0001*
昇圧薬の服用患者(%)
40.0
16.9
0.0196*
ヘマトクリット(Ht値:%)
35.9±7.5
32.5±3.7
0.0009**
透析による体重減少率(%)
4.9±1.2
3.9±1.8
0.0323**
*:χ
2
検定, * *:unpaired t 検定
Ca・P積(mg
2
/dL
2
)
53.9±17.4
52.6±14.2
0.7306**
総Chol値(mg/dL)
152.5±35.9
154.8±32.8
0.7840**
ASO合併率(%)
33.3
24.0
0.4031*
西原 舞, 平田純生, 他:透析会誌38: 1279-1283, 2005.
透析患者の結腸壊死・穿孔はなぜ起こる?
食物繊維不足
便秘する薬剤投与
蠕動力・排便力の低下
結腸壊死・穿孔
常習便秘
硬便による結腸の通過障害
HDによる腸管虚血
HDによる腸間膜動脈血流障害
HDによる除水
Risk Factors
イオン交換樹脂服用者
昇圧薬服用者
Ht値の異常高値者
水分管理不良者
動脈硬化?
硬結便の形成から腸管穿孔を
起こす過程(平田の仮説)
1.硬結便の形成
2.宿便の貯留
3.結腸壊死
4.結腸穿孔
×
×
×
×
結腸穿孔
腸間膜動脈の血流不全
結腸壊死
宿便の貯留
硬結便
硬結便
回結腸動脈
上腸間膜動脈
下腸間膜動脈
透析患者の便秘は
「単なる便秘」
ではすまされない
キックリン
®
による腸管穿孔症例
75歳男性、透析暦11年。原疾患:急性間質性腎炎
入院3か月前、血清Ca9.8mg/dL、血清リン値6.3mg/dLの
ため、キックリン2,250mg/日から3,000mg/日に増量。
センノシド+ピコスルファートNaを内服するも排便状況は
4~5日に1回のみ。
17時より突然の腹痛が出現し(透析日か否かは不明)、
便秘による腹痛と考えピコスルファートNaを内服したが
排便なく
、腹痛も改善せず緊急入院。
腹部CTにて下部結腸に憩室が多発、
腹腔内にフリーエアー
を多数認めた
ため、緊急手術。直腸部分切除し、人工肛門
増設術施行。
上部直腸に腸管穿孔を認め、腹腔内に硬便を
認めた。
術後、敗血症ショックが疑われ、CHDF, PMX-DHP
施行により救命できた。
元 志宏,他: 透析会誌46: 1069-1073, 2013
噛み砕かずに服用したホスレノール
Ⓡ
錠が
原因と考えられる結腸虚血の1例
-70歳の男性患者。激しい右上腹
部痛を突然訴え、入院。
-臨床検査および症状などから、急
性腹症と診断され、開腹術を実
施。上行結腸の虚血を認め、結腸
半切除術を実施。
-結腸虚血は、噛み砕かずに服用
した炭酸ランタンの集塊による可能
性が高かった。
患者は主治医の注
意を無視し、本剤を噛み砕かずに
服用した
ことが明らかになった。
-回復は速く、良好な全身状態のも
とに退院。
薬剤性消化管穿孔の報告
CPS(カリメート
Ⓡ
・
アーガメイト
Ⓡ
など)
ホスレノール
Ⓡ
塩酸セベラマー
グリセリン浣腸
ビキサロマー
コレスチミド
バリウム
現像液
不明(イオン交換樹脂)
医中誌により透析患者、消化管穿孔など
により検索し非薬剤性のものを除外した
52
報62症例
PMDAの報告では
2009-2015で
CPSで
イレウス 消化管穿孔 結腸虚血
消化管穿孔 結腸穿孔
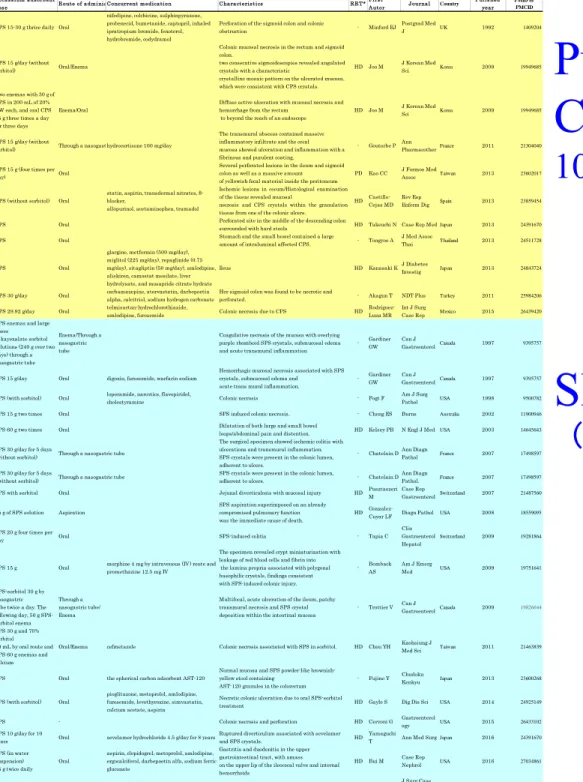
Table 3. Reported cases of fecal properties in patients undergoing calcium polystyrene sulfonate or sodium polystyrene sulfonate treatment.
AgeS ex
Potas s ium ads orbent
dos e Route of adminis trationConcurrent medication Characteris tics RRT* Firs t
Autor Journal Country Pulis hed
year
PMID or PMCID
62
M CPS 15-30 g thrice daily Oral
nifedipine, colchicine, sulphinpyrazone, probenecid, bumetanide, captopril, inhaled ipratropium bromide, fenoterol, hydrobromide, codydramol
Perforation of the sigmoid colon and colonic
obstruction - Minford EJ Postgrad Med J UK 1992 1409204 34 M CPS 15 g/day (without sorbitol) Oral/Enema
Colonic mucosal necrosis in the rectum and sigmoid colon.
two consecutive sigmoidoscopies revealed angulated crystals with a characteristic
crystalline mosaic pattern on the ulcerated mucosa, which were consistent with CPS crystals.
HD Joo M J Korean Med
Sci Korea 2009 19949685 34
M
Two enemas with 30 g of CPS in 200 mL of 20% DW each, and oral CPS 15 g three times a day for three days
Enema/Oral
Diffuse active ulceration with mucosal necrosis and hemorrhage from the rectum
to beyond the reach of an endoscope
HD Joo M J Korean Med
Sci Korea 2009 19949685 73
F
CPS 15 g/day (without
sorbitol) Through a nasogastric tubehydrocortisone 100 mg/day
The transmural abscess contained massive inflammatory infiltrate and the cecal mucosa showed ulceration and inflammation with a fibrinous and purulent coating.
- Goutorbe P Ann
PharmacotherFrance 2011 21304040 59
F
CPS 15 g (four times per day) Oral
Several perforated lesions in the ileum and sigmoid colon as well as a massive amount of yellowish fecal material inside the peritoneum
PD Kao CC J Formos Med
Assoc Taiwan 2013 23602017 73
M CPS (without sorbitol) Oral
statin, aspirin, transdermal nitrates, β-blocker,
allopurinol, acetaminophen, tramadol
Ischemic lesions in cecum/Histological examination of the tissue revealed mucosal
necrosis and CPS crystals within the granulation tissue from one of the colonic ulcers.
HD Castillo-Cejas MD
Rev Esp
Enferm Dig Spain 2013 23859454 90
F CPS Oral
Perforated site in the middle of the descending colon
surrounded with hard stools HD Takeuchi N Case Rep Med Japan 2013 24391670 52
M CPS Oral
Stomach and the small bowel contained a large
amount of intraluminal affected CPS. - Tongyoo A J Med Assoc
Thai Thailand 2013 24511728 78
M CPS Oral
glargine, metformin (500 mg/day), miglitol (225 mg/day), repaglinide (0.75 mg/day), sitagliptin (50 mg/day), amlodipine, aliskiren, camostat mesilate, liver hydrolysate, and mosapride citrate hydrate
Ileus HD Kanasaki KJ Diabetes
Investig Japan 2013 24843724 78
F CPS 30 g/day Oral
carbamazepine, atorvastatin, darbepoetin alpha, calcitriol, sodium hydrogen carbonate
Her sigmoid colon was found to be necrotic and
perforated. - Akagun T NDT Plus Turkey 2011 25984206 72
F CPS 29.92 g/day Oral
telmisartan-hydrochlorothiazide,
amlodipine, furosemide Colonic necrosis due to CPS HD Rodríguez-Luna MR
Int J Surg
Case Rep M exico 2015 26439420 66
M
SPS enemas and large doses of kayexalate sorbitol solutions (240 g over two days) through a nasogastric tube
Enema/Through a nasogastric tube
Coagulative necrosis of the mucosa with overlying purple rhomboid SPS crystals, submucosal edema and acute transmural inflammation
- Gardiner GW
Can J
GastroenterolCanada 1997 9395757 71
F SPS 15 g/day Oral digoxin, furosemide, warfarin sodium
Hemorrhagic mucosal necrosis associated with SPS crystals, submucosal edema and acute trans mural inflammation.
- Gardiner GW
Can J
GastroenterolCanada 1997 9395757 71
M SPS (with sorbitol) Oral
loperamide, narcotics, flavopiridol,
cholestyramine Colonic necrosis - Fogt F Am J Surg
Pathol USA 1998 9500782 53
F SPS 15 g two times Oral SPS induced colonic necrosis. - Cheng ES Burns Australia 2002 11900946 79
M SPS 60 g two times Oral
Dilatation of both large and small bowel
loops/abdominal pain and distention. HD Kelsey PB N Engl J Med USA 2003 14645643 46
M
SPS 30 g/day for 5 days
(without sorbitol) Through a nasogastric tube
The surgical specimen showed ischemic colitis with ulcerations and transmural inflammation. SPS crystals were present in the colonic lumen, adherent to ulcers.
- Chatelain DAnn Diagn
Pathol France 2007 17498597 46
M
SPS 30 g/day for 5 days
(without sorbitol) Through a nasogastric tube
SPS crystals were present in the colonic lumen,
adherent to ulcers. - Chatelain D Ann Diagn
Pathol. France 2007 17498597 87
M SPS with sorbitol Oral Jejunal diverticulosis with mucosal injury HD Pusztaszeri M Case Rep GastroenterolSwitzerland 2007 21487560 45 M 15 g of SPS solution Aspiration
SPS aspiration superimposed on an already compromised pulmonary function was the immediate cause of death.
HD
Gonzalez-Cuyar LF Diagn Pathol USA 2008 18559095 71
F
SPS 20 g four times per
day Oral SPS-induced colitis - Tapia C Clin Gastroenterol Hepatol Switzerland 2009 19281864 56 F SPS 15 g Oral
morphine 4 mg by intravenous (IV) route and promethazine 12.5 mg IV
The specimen revealed crypt miniaturization with leakage of red blood cells and fibrin into the lamina propria associated with polygonal basophilic crystals, findings consistent with SPS-induced colonic injury.
- Bomback AS Am J Emerg Med USA 2009 19751641 24 F SPS-sorbitol 30 g by nasogastric tube twice a day. The following day, 50 g SPS-sorbitol enema
Through a nasogastric tube/ Enema
Multifocal, acute ulceration of the ileum, patchy transmural necrosis and SPS crystal deposition within the intestinal mucosa
- Trottier V Can JGastroenterolCanada 2009 19826644
30 M
SPS 30 g and 70% sorbitol 60 mL by oral route and SPS 60 g enemas and calcium
Oral/Enema cefmetazole Colonic necrosis associated with SPS in sorbitol. HD Chou YH Kaohsiung J
Med Sci Taiwan 2011 21463839 66
M SPS Oral the spherical carbon adsorbent AST-120
Normal mucosa and SPS powder-like brownish-yellow stool containing
AST-120 granules in the colorectum
- Fujino Y Chudoku
Kenkyu Japan 2013 23600268 61
F SPS (with sorbitol) Oral
pioglitazone, metoprolol, amlodipine, furosemide, levothyroxine, simvastatin, calcium acetate, aspirin
Necrotic colonic ulceration due to oral SPS-sorbitol
treatment HD Gayle S Dig Dis Sci USA 2014 24925149 58
M SPS - Colonic necrosis and perforation HD Cervoni G Gastroenterol
ogy USA 2015 26433102 66
M
SPS 10 g/day for 10
years Oral sevelamer hydrochloride 4.5 g/day for 8 years
Ruptured diverticulum associated with sevelamer and SPS crystals. HD
Yamaguchi
T Ann Med Surg Japan 2016 24391670 70 F SPS (in water suspension) 15 g twice daily Oral
aspirin, clopidogrel, metoprolol, amlodipine, ergocalciferol, darbepoetin alfa, sodium ferric gluconate
Gastritis and duodenitis in the upper gastrointestinal tract, with amass on the upper lip of the ileocecal valve and internal hemorrhoids
HD Bui M Case Rep
Nephrol USA 2016 27034861 55
F SPS 30 g Oral heparin, broad-spectrum antibiotics Ischemic necrosis of the bowel HD Dunlap RH J Surg Case Rep USA 2016 27765805