Received October 24, 2013; Accepted December 11, 2013
The onset of heart failure is associated with the extent of LV fibrosis in hypertrophic cardiomyopathy:
insights from cardiac magnetic resonance analysis
Takashi Nakamura, Yoshitaka Iwanaga, Masakazu Yasuda, Tomoyuki Ikeda, Hanako Morooka, Shunichi Miyazaki
Division of Cardiology, Department of Internal Medicine, Kinki University Faculty of Medicine,
Osakasayama, Osaka, 589-8511, Japan
Abstract
Background: Patients with hypertrophic car- diomyopathy(HCM ) are frequently complicated with heart failure (HF), which is associated with the patientʼprognosis. However,the onsets are diverse and the causal factors remain un- clear. Therefore, we sought to determine the factors associated with the onset of HF in patients with HCM using cardiac magnetic resonance (CM R).
M ethods: HCM patients with new hospitaliza- tion due to HF (HCM -HF) underwent CM R
[cine, T2-weighted and late gadolinium-enhan- cement (LGE) imaging]. LV mass and fibrosis was quantified and the distribution /pattern of LGE/T2 was analyzed using a 17 segment model. The data were compared with those of HCM patients receiving regular outpatient treatment without HF (HCM -NHF).
Results: In all patients, mean maximal wall thickness was 20.9±3.9 mm and LGE was obser- ved in 48 (80%) patients. There were no signifi- cant differences in clinical characteristics between HCM -HF (n =17) and HCM -NHF
(n=43). Plasma B-type natriuretic peptide (BNP) level was significantly higher in patients with HCM -HF than HCM -NHF (p <0.01).
Although left ventricular (LV) myocardial mass (LVM ) was not different between them, LV ejection fraction were significantly decreased in patients with HCM -HF (p <0.01). Additionally, LV fibrosis mass was significantly higher in patients with HCM -HF (p <0.01). Receiver operating characteristics curve analysis indicat- ed good predictive performance of LV fibrosis mass for HF (AUC=0.783), which was similar to BNP (AUC=0.712).
Conclusions: In HCM patients,the onset of HF was independently associated with LV fibrosis mass,irrespective of LV myocardial mass per se.
Evaluation of LV fibrosis in individual HCM patients may help performing effective preven- tive strategies on HF.
Key words:B-type natriuretic peptide, heart failure, hypertrophic cardiomyopathy, magnetic resonance imaging, myocardial fibrosis
INTRODUCTION
Hypertrophic cardiomyopathy (HCM) is a complex and relatively common form of genetic heart disease and is the most frequent cause of sudden death in the young. It is also character- ized by a heterogeneous clinical course from
asymptomatic status to severe heart failure(HF), and HF is the main adverse outcome in elderly patients. Because of the slowly evolving nature of HCM,timely identification of patients at risk of developing advanced left ventricular (LV) dysfunction and HF is important. However, there is limited guidance to identify those at risk
of progressive HF, which affects up to 10% of patients.
Myocyte disarray, fibrosis, and microvascular dysfunction are the histological hallmarks of HCM. Myocardial fibrosis has been suggested as a key mechanism for adverse outcomes. Multi- ple post-mortem studies have documented myocardial fibrosis (interstitial or replacement) in HCM patients, which is distinct from the pattern observed in patients with coronary artery disease (CAD) or dilated cardiomyopathy.
Late gadolinium-enhancement (LGE) cardiac magnetic resonance (CMR) has been used to uniquely characterize the extent of replacement fibrosis and has prognostic value for HCM. A recent pooled analysis revealed that LGE on CMR appeared to possess significant prognostic power in predicting serious cardiac complica- tions in HCM. It demonstrated a significant association between the presence of LGE and HF death as 13 of 634 subjects(2.1%)with LGE on CMR died of HF, but no patients without LGE on CMR went on to die of HF. However, the necessity of developing more sophisticated techniques to quantify LGE in HCM was also suggested to improve its prognostic utility. The clinical significance of the LGE pattern,amount, and characteristics in HCM patients with HF remains unresolved. To characterize and iden- tify cardiac dysfunction and remodeling includ- ing fibrosis in individual HCM patients may allow effective preventive strategies to be perfor- med over a time span of several years before HF onset. Therefore,we performed a detailed analy- sis of cardiac fibrosis and function in HCM patients for hospitalized HF, and sought to determine the factors associated with the onset of HF in patients with HCM using CMR.
M ETHODS
Study protocol
HCM patients newly hospitalized due to HF (New York Heart Association classification III or IV) who underwent CMR between February 2010 and July 2013 at Kinki University Hospital (Osakasayama,Japan) were enrolled in the pres- ent study(defined as HCM-HF). HCM patients receiving regular outpatient treatment without HF were defined as HCM-NHF. All HCM patients were diagnosed based on conventional criteria; left ventricular hypertrophy 15 mm on two-dimensional echocardiography in the
absence of another disease that could account for this hypertrophy. The work-up at the initial diagnosis included electrocardiogram (ECG), echocardiography, coronary angiography, left ventriculography, 24-h Holter ECG and CMR imaging. Plasma B-type natriuretic peptide (BNP)was measured at the time of CMR evalua- tion. HOCM was defined as showing LV out- flow tract (LVOT)pressure gradient 30 mmHg at rest with echocardiography. This study was approved by the Institutional Review Board.
CM R Image Acquisition
CMR was performed using a 1.5-T scanner (Intera 1.5T ; Philips Medical Systems,the Neth- erlands)and standardized protocol. Cine images were acquired with a steady-state free-precession breath-hold sequence in 3 long-axis planes and contiguous short-axis slices(10-mm no gap)from the atrioventricular ring to the apex. Visualiza- tion of myocardial edema was performed using a T2-weighted triple inversion recovery breath- hold pulse sequence. LGE images were obtained 10-15 min after intravenous administration of 0.2 mmol・kg gadolinium-DTPA (Magnevist ; Bayer Schering Pharma,Germany)and standard breath-hold inversion recovery imaging perfor- med (repetition time 9.8 ms, echo time 4.6 ms, flip angle 15°,slice thickness 5 mm,and in-plane resolution 1.7×2.4 mm , typical breath-hold 10- 15 seconds),using an inversion recovery gradient echo sequence with 5-mm slice thickness at the same position as the long-and short-axis cines in end-diastole. The inversion time was adjusted per patient to an optimally null signal from a normal myocardium, typically between 250 and 350 ms.
Image Analysis
LV volume [end-diastolic volume(EDV)and end-systolic volume (ESV) ], ejection fraction (EF), LV mass, and wall thickness were calcu- lated using commercially available workstations (View Forum; Philips Medical System, the Netherlands; or Aze Virtual Place; Aze Ltd., Japan). To calculate LV mass, the endocardial and epicardial borders of the LV myocardium were manually planimetered on successive short- axis cine images at end-diastole. The most basal slice at end-diastole was visually inspected,and, if ventricular myocardium was present, it was planimetered and included in the mass calcula- tion. Particular care was taken to avoid includ- ing papillary muscles in the LV mass calcula- tion. LV mass was derived by summation using
the discs method and multiplying the myocardial muscle volume by 1.05 g /cm . To assess LGE, all short-axis slices from the base to the apex were inspected visually to identify areas of a normal (completely nulled) myocardium.
Mean signal intensity (and standard deviation
[SD]) was derived and a threshold of 6 SD exceeding the mean was used to define areas of LGE (Figure 1). Summing the planimetered areas of LGE in all short-axis slices yielded % LGE volume, which was expressed as a propor- tion of total LV myocardium. LV fibrosis mass (g) was calculated by multiplying %LGE area.
Local wall thickness, LGE, and T2-weighted images were also analyzed based on the AHA 17- segment model. All analyses were performed by one experienced reader and reviewed and con- firmed by a second expert reader, with both of the independent observers being blinded to patient identities and clinical profiles. Any discrepancies in analysis between the two readers were then adjudicated by a senior observer.
Statistical analysis
Groups were compared using the χ test for proportions and unpaired t-test or analysis of variance for continuous variables, as appropri- ate. The linearity of the relationship between two variables was assessed by linear regression analysis, and Pearsonʼs correlation coefficient was calculated. Cut-off levels of LV mass and BNP and the sensitivities and specificities of the cut-off levels were calculated using a receiver operating characteristics (ROC) curve analysis.
Multiple logistic regression analysis was used to adjust for age,gender,and the presence of other factors (model 1,EF ; model 2,EDV; model 3, LV mass; model 4,log BNP)using JMP version 10.0.P<0.05 was considered significant. Results are expressed as the mean ±standard deviation
(SD).
RESULTS
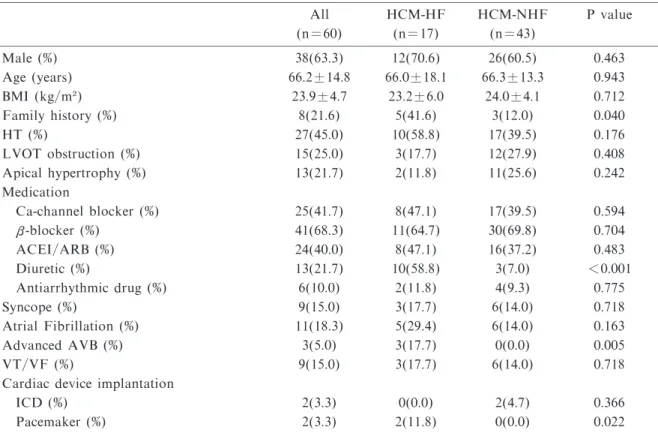
Baseline characteristics (Table 1)
We enrolled 63 consecutive patients diagnosed with HCM. Three patients were excluded due to previous myocardial infarction. The remaining 60 patients were grouped ; a HCM-NHF group of 43 patients (71.7%) and a HCM-HF group of 17 patients (28.3%). The mean age of the 60 patients was 66.2±14.8 years and 63.3% were male. No significant differences were observed in the prevalence of LVOT obstruction between the HCM-HF group and HCM-NHF group (P = 0.408). The patients with HCM-HF were more likely to receive diuretics (P <0.001)after hospi- talization. The family history of HCM or sud- den cardiac death was frequently observed in HCM-HF patients (P<0.05). The prevalence of advanced atrioventricular block (AVB) and pacemaker implantation were significantly higher in the HCM-HF group than in HCM- NHF group (P<0.01 and P<0.05). However, that of atrial fibrillation (AF), syncope, and ventricular tachycardia (VT) /fibrillation (VF) was not different between the two groups. As for diastolic parameters on two-dimensional echocardiography(E/A, E/ Eʼ, left atrial dimen- sion), no significant differences were observed, except for a diameter in left atrium (p<0.05).
CM R analysis (Table 2)
A LGE images from a representative case is shown in Figure 1; one patient with moderate fibrosis (fibrosis mass 43.7 g)had HF manifesta- tion and one without apparent fibrosis by LGE had no HF.
Of the 60 patients, quantitative analysis in LGE-CMR could not be performed in one patient due to poor image quality. Although there was no difference in LV end-diastolic volume,the HCM-HF group had a lower LV EF than the HCM-NHF group (P <0.01). No signif- icant differences were observed in LV wall thick- ness or LV mass between the groups. LGE was not confirmed in one HCM-HF patient(5.9%)in contrast to 11 HCM-NHF patients (25.6%).
Significant differences were observed in %LGE volume(34.1±18.3 vs.15.7 ±12.6%,respectively;
P<0.001)or the LV fibrosis mass(Figure 2: 60.
7±45.3 vs.24.6±25.7 g,respectively; P<0.001).
BNP levels were significantly higher in the HCM-HF group than in HCM-NHF group (Fig-
Fig.1 The short-axis LGE image in a representative cases with heart failure and quantification of the LGE image; the green line denotes the epicardial border and the red line denotes the endocardial border. A normal (completely nulled) myocardium is settled in the area denoted by the blue circle. The LGE area by 6SD method is delineated in yellow.
ure 2: 437.3±576.0 vs. 165.3±174.4 pg/ml, respectively; P=0.010).
Receiver operator characteristics curve analy- sis (Figure 2)
The areas under ROC curves (AUC) for LV
Table 1 Patient characteristics
All
(n=60)
HCM-HF (n=17)
HCM-NHF (n=43)
P value
Male (%) 38(63.3) 12(70.6) 26(60.5) 0.463
Age (years) 66.2 ±14.8 66.0±18.1 66.3±13.3 0.943
BMI (kg/m ) 23.9±4.7 23.2±6.0 24.0±4.1 0.712
Family history(%) 8(21.6) 5(41.6) 3(12.0) 0.040
HT (%) 27(45.0) 10(58.8) 17(39.5) 0.176
LVOT obstruction (%) 15(25.0) 3(17.7) 12(27.9) 0.408
Apical hypertrophy(%) 13(21.7) 2(11.8) 11(25.6) 0.242
Medication
Ca-channel blocker (%) 25(41.7) 8(47.1) 17(39.5) 0.594
β-blocker (%) 41(68.3) 11(64.7) 30(69.8) 0.704
ACEI/ARB (%) 24(40.0) 8(47.1) 16(37.2) 0.483
Diuretic (%) 13(21.7) 10(58.8) 3(7.0) <0.001
Antiarrhythmic drug (%) 6(10.0) 2(11.8) 4(9.3) 0.775
Syncope (%) 9(15.0) 3(17.7) 6(14.0) 0.718
Atrial Fibrillation (%) 11(18.3) 5(29.4) 6(14.0) 0.163
Advanced AVB (%) 3(5.0) 3(17.7) 0(0.0) 0.005
VT/VF (%) 9(15.0) 3(17.7) 6(14.0) 0.718
Cardiac device implantation
ICD (%) 2(3.3) 0(0.0) 2(4.7) 0.366
Pacemaker (%) 2(3.3) 2(11.8) 0(0.0) 0.022
Values are the mean±SD or number (%).
ACEI,angiotensin-converting enzyme inhibitor; ARB,angiotensin receptor blocker; BMI,body mass index;
HNCM, hypertrophic non-obstructive cardiomyopathy; HOCM, hypertrophic obstructive cardiomyopathy;
HT,hypertension ; ICD,implantable cardioverter defibrillator; VT,ventricular tachycardia; VF,ventricular fibrillation ; LVOT, left ventricular outflow-tract.
Table 2 CMR findings
HCM-HF HCM-NHF P value
LV EDV (ml) 141.8±53.2 121.9±31.2 0.077
LV ESV (ml) 82.3±58.8 53.4±19.9 0.006
LV EF (%) 46.6±2.8 56.3±1.8 0.005
LV wall thickness (mm)
average 12.3±1.7 11.4±1.9 0.107
maximal 20.9±3.9 19.9±2.9 0.284
LV mass (g) 162.3±57.0 142.8±40.5 0.141
LV volume/mass ratio 0.89±0.21 0.87±0.17 0.690
T positive 10(58.8) 20(46.5) 0.390
LGE positive 16(94.1) 32(74.4) 0.086
%LGE volume 34.1±18.3 15.7±12.6 <0.001
Values are the mean±SD or number (%).
EDV, end-diastolic volume; EF, ejection fraction ; ESV, end-systolic volume, HNCM, hypertrophic non- obstructive cardiomyopathy; HOCM, hypertrophic obstructive cardiomyopathy; LGE, late gadolinium en- hancement; LV, left ventricular.
fibrosis mass and BNP levels as an indicator of HF hospitalization were 0.765 (95% CI ; 0.619- 0.910) and 0.712 (95% CI ; 0.572-0.868), respec- tively. The optimal cut-off values of LV fibrosis mass and BNP were 23.1 g with a sensitivity of 88% and a specificity of 65%, and 155 pg /ml, with a sensitivity of 81%and a specificity of 58%.
M ultiple logistic regression analysis for LV fibrosis mass (Table 3)
LV fibrosis mass remained a significant predic- tor of HF hospitalization in models adjusted for age,gender,and LV EF (Model 1); age,gender, and EDV (Model 2); age,gender,and LV mass (Model 3); and age, gender, and log BNP (Model 4). LV EF and log BNP were not significant predictors for HF hospitalization in Model 1 and 4,respectively(P =0.081 and 0.094).
DISCUSSION
The stages that precede HF in HCM are still
relatively unknown, representing an important target for research. Therefore, we examined cardiac fibrosis and function in 60 patients with HCM by CMR to clarify the relationship between HCM and HF in the present study.
Consequently, no significant differences were revealed in clinical characteristics, except for AVB prevalence, family history and BNP levels.
No significant differences were observed in LV mass between patients with and without HF. In contrast, a significant correlation was observed between EF and LV fibrosis mass, and HF hospitalization. By ROC analysis, LV fibrosis mass showed a similar predictive performance for HF to plasma BNP levels. In addition, a multivariable regression analysis that took into account age,gender,and BNP levels demonstrat- ed a significant association between LV fibrosis mass and HF. The present findings suggest that evaluation of LV fibrosis in individual HCM patients may help to develop effective preventive strategies against HF development.
Some patients with HCM are complicated by clinical manifestations during the long-term clin- ical course. Traditionally, the focus of HCM literature has been polarized regarding two aspects of indisputable clinical relevance: the pathogenesis, clinical consequences, and man- agement of dynamic LVOT obstruction,and the issue of arrhythmic risk stratification and preven- tion of sudden cardiac death (SCD). By compar- ison, limited attention has been devoted to the life-long process of LV remodeling and progres- sive dysfunction that occurs in a substantial proportion of HCM patients and leads to the onset and progress of HF. Individual patient variability with regard to timing of the onset, phenotype, and clinical course is extreme, the reasons for which are poorly understood. In particular,both the extent and time course of LV remodeling are extremely heterogeneous:
adverse changes may be observed at any age, including infancy and adolescence,and may lead
Table 3 Odds ratio of LV fibrosis mass for heart failure hospitalization adjusting for pertinent covariates OR (per 1 g increase) 95%CI P value
Model 1 (age, gender, EF) 1.028 1.007‑1.055 0.007
Model 2 (age, gender, EDV) 1.032 1.011‑1.060 0.003
Model 3 (age, gender, LV mass) 1.058 1.025‑1.104 <0.001
Model 4 (age, gender, Log BNP) 1.025 1.003‑1.054 0.027 BNP,B-type natriuretic peptide; CI,confidence interval; EF,ejection fraction ; EDV,end-diastolic volume;
LV, left ventricular; OR, odds ratio.
Fig.2 Relationship between LV fibrosis/BNP, and heart failure admission. (A) Differences between patients with and without heart failure admission. (B) Receiver operating characteristic (ROC) curves for LV fibrosis mass and BNP as a predictor of heart failure admission. AUC,area under the ROC curve;
BNP, B-type natriuretic peptide; CI, confidence interval; HF, heart failure.
to overt dysfunction and advanced HF in a brief span of time but more often occur gradually over years or decades. Currently,to determine which patients are at high risk of the development of HF remains challenging. Principal determinants of HF progression in HCM patients have been reported to be LV systolic dysfunction, LVOT obstruction and AF. Additionally,determinants in some cases of preserved systolic function appear to be the absence of obstruction and diastolic dysfunction. Our cohort of HCM with new HF hospitalization did not show any differences in clinical characteristics, including age, gender, and co-morbidities including AF and LVOT obstruction, which may suggest the heterogeneity and difficulties in identifying patients at risk of HF. In addition,our analysis by CMR showed some differences between those with and without HF ; LV EF, %LGE volume, and LV fibrosis mass, and the present results in a multivariable regression analysis also support- ed a recent hypothesis that the clinical manifesta- tions of HCM may depend on the location and extent of myocardial fibrosis and the resultant myocardial dysfunction.
Although the origin of myocardial fibrosis has not yet been determined in HCM patients,it has been suggested as a key mechanism for adverse outcomes. Pooled analysis revealed that LGE on CMR appeared to possess significant prog- nostic power in predicting serious cardiac com- plications in HCM. The degree of fibrosis has not yet been a significant predictor of events in multivariate analysis, excluding major arrhyth- mic events. Recently, OʼHanlon et al. reported that the presence and amount of in vivo fibrosis detected by CMR was an independent predictor of adverse outcomes in patients with HCM dur- ing a follow-up for over 3.1 years. In addition, they have reported that the overall percentage of fibrosis was a stronger predictor in this cohort of HF outcomes than the presence of left ventricular outflow tract obstruction. By assess- ing and comparing the amount of the fibrosis mass in our cohort, we also indicated that myocardial fibrosis was a strong and indepen- dent contributing factor to HF outcomes, show- ing a similar performance to BNP levels in ROC analysis and a stronger predictive value than BNP levels or EF in multivariate analysis.
Some studies have proposed that the overall percentage of fibrosis correlates with LV func- tion. LGE may be associated with increased
myocardial stiffness and LV adverse remodeling leading to cavity dilatation and eventually systolic dysfunction. Significant differences were observed in LV EF between HCM-HF and HCM-NHF (P<0.01), and LV systolic function was reduced along with the extent of fibrosis covering a wide range of the myocardium in HCM-HF patients (P=0.004). Moreover, in previous reports,passive late diastole filling was also impaired due to increased interstitial fi- brosis. Tissue Doppler echocardiographic studies have demonstrated that myocyte disarray per se may affect both ventricular relaxation and stiffness. We did not try to assess diastolic dysfunction by other modalities; however, In the present study, 47% of the HCM-HF cohort showed preserved EF (EF>50%) and their % LGE volume was significantly increased compar- ed with that in HCM-NHF with preserved EF (29.1%vs.17.0%,P=0.027),suggesting that dias- tolic dysfunction in relation with the amount of fibrosis may be associated with HF development.
The role of biomarkers such as BNP and troponin for the diagnosis or risk stratification in HCM has been investigated. As the plasma BNP is a useful biomarker to assess disease severity and prognosis in patients with HF, it was also reported as a useful marker in HCM patients with HF. In the present study, plasma BNP was significantly increased in HCM-HF, and ROC analysis showed good pre- dictive performance for HF hospitalization (AUC=0.712). However, it has been suggested that BNP has a limited role in the diagnosis and management of HCM. The relationship between BNP and HCM may be complex because of various determinant factors,such as extensive LV hypertrophy, LVOT obstruction, LV fibrosis, and LV diastolic/diastolic dysfunction. In par- ticular,the relationship of LV fibrosis and BNP remains uncertain. In the present study, signifi- cant correlations between %LGE volume or fi- brosis mass and log BNP levels were observed in HCM patients (R=0.32 and 0.35, respectively).
However, the relationship was modest and fi- brosis %volume or mass as a determinant of the BNP level was not independent of other parame- ters such as EDV, EF, and LV mass (data not shown). Recent studies suggested that BNP was an independent predictor of morbidity and mortality in a large cohort of patients with HCM ; however, whether quantification of the fibrosis mass by CMR has additive or stronger
effects on the prediction of patientsʼprognosis needs to be elucidated in the large cohort.
Several limitations should be considered when interpreting our results. First,the study popula- tion was relatively small. Therefore, any nega- tive findings could have been caused by low statistical power. Second,the present study was a single-centered, retrospective, and cross-sec- tional study; thus,it had several inherent limita- tions, including selection and referral biases.
Third, the study population consisted of HCM patients who could undergo CMR ; patients who could not tolerate the procedure or would be at high risk were excluded. Lastly,we did not assess future clinical events. Although our find- ings suggest pathophysiological aspects in HCM with HF, clinical implications with respect to future HF outcomes may be limited. Recently, Todiere et al. demonstrated that the prevalence of LGE increased from 81.8%to 96.4%of HCM subjects after an average of two years by serial CMR evaluations and that the increment of LGE was higher in patients with worsening NYHA functional class. The findings in conjunction with our results may suggest that myocardial fibrosis in HCM is a progressive and preceding phenomenon and it may predict HF onset and worsening in the future. CMR in HCM may yield prognostic information above that of tradi- tional risk models,and further studies will reveal the clinical perspective of CMR in HCM more clearly.
Competing interests: None to declare.
Funding : S.M. received research support from Daiichi-Sankyo Pharmaceutical Co., Ltd., Eisai Co., Ltd., and Sanofi-Aventis K.K., Ltd.; how- ever, these companies played no role in the conception, conduct, or analysis of this study.
REFERENCE
1. Varnava AM, Elliott PM, Mahon N, Davies MJ, McKenna WJ. (2001) Relation between myocyte dis- array and outcome in hypertrophic cardiomyopathy.
Am J Cardiol 88: 275‑279
2. Leonardi S, et al. (2009) Usefulness of cardiac mag- netic resonance in assessing the risk of ventricular arrhythmias and sudden death in patients with hyper- trophic cardiomyopathy. Eur Heart J 30: 2003‑2010 3. Moon JC, et al. (2003) Toward clinical risk assess-
ment in hypertrophic cardiomyopathy with gadolinium cardiovascular magnetic resonance. J Am Coll Cardiol 41: 1561‑1567
4. Kwon DH, Smedira NG, Desai MY. (2009) Cardiac
magnetic resonance detection of myocardial scarring in hypertrophic cardiomyopathy. J Am Coll Cardiol.54:
242‑249
5. Maron BJ, Wolfson JK, Epstein SE, Roberts WC.
(1986) Intramural (“small vessel”) coronary artery disease in hypertrophic cardiomyopathy. J Am Coll Cardiol 8: 545‑557
6. Varnava AM, Elliott PM, Sharma S, McKenna WJ, Davies MJ. (2000) Hypertrophic cardiomyopathy: the interrelation of disarray, fibrosis, and small vessel disease. Heart 84: 476‑482
7. Ismail TF,Prasad SK,Pennell DJ.(2012)Prognostic importance of late gadolinium enhancement cardiovas- cular magnetic resonance in cardiomyopathy. Heart 98: 438‑442
8. Green JJ, Berger JS, Kramer CM, Salerno M. (2012) Prognostic value of late gadolinium enhancement in clinical outcomes for hypertrophic cardiomyopathy.
JACC Cardiovasc Imaging 5: 370‑377
9. Maron BJ, et al. (2003) Task Force on Clinical Expert Consensus Documents. American College of Cardiology; Committee for Practice Guidelines. Eur- opean Society of Cardiology.; Task Force on Clinical Expert Consensus Documents. American College of Cardiology; Committee for Practice Guidelines. Eur- opean Society of Cardiology. American College of Cardiology/European Society of Cardiology clinical expert consensus document on hypertrophic car- diomyopathy. A report of the American College of Cardiology Foundation Task Force on Clinical Expert Consensus Documents and the European Society of Cardiology Committee for Practice Guidelines. J Am Coll Cardiol 42: 1687‑1713
10. Kramer CM, Barkhausen J, Flamm SD, Kim RJ, Nagel E. (2008) Society for Cardiovascular Magnetic Resonance Board of Trustees Task Force on Standard- ized Protocols. Standardized cardiovascular magnetic resonance imaging (CMR) protocols, society for car- diovascular magnetic resonance: board of trustees task force on standardized protocols. J Cardiovasc Magn Reson 10: 35
11. Flett AS, et. al. (2011) Evaluation of techniques for the quantification of myocardial scar of differing etiology using cardiac magnetic resonance. JACC Cardiovasc Imaging 4: 150 ‑156
12. Vermes E, Childs H, Carbone I, Barckow P, Frie- drich MG.(2013)Auto-threshold quantification of late gadolinium enhancement in patients with acute heart disease. J Magn Reson Imaging 37: 382 ‑390
13. Bondarenko O,et.al.(2005)Standardizing the defini- tion of hyperenhancement in the quantitative assess- ment of infarct size and myocardial viability using delayed contrast-enhanced CMR. J Cardiovasc Magn Reson 7: 481‑485
14. Spiewak M, et al. (2010) Comparison of different quantification methods of late gadolinium enhance- ment in patients with hypertrophic cardiomyopathy.
Eur J Radiol 74: e149‑153
15. Olivotto I,Cecchi F,Poggesi C,Yacoub MH.(2012)
Patterns of disease progression in hypertrophic car- diomyopathy: an individualized approach to clinical staging. Circ Heart Fail 5: 535 ‑546
16. Melacini P,et.al.(2010)Clinicopathological profiles of progressive heart failure in hypertrophic car- diomyopathy. Eur Heart J 31: 2111‑2123
17. OʼHanlon R, et. al. (2010) Prognostic significance of myocardial fibrosis in hypertrophic cardiomyopathy. J Am Coll Cardiol 56: 867‑ 874
18. Maron MS, et. al.(2008) Clinical profile and signifi- cance of delayed enhancement in hypertrophic car- diomyopathy. Circ Heart Fail 1: 184‑191
19. Moon JC, et. al. (2003) Toward clinical risk assess- ment in hypertrophic cardiomyopathy with gadolinium cardiovascular magnetic resonance. J Am Coll Cardiol 41: 1561‑1567
20. Nagueh SF, et. al. (1999) Doppler estimation of left ventricular filling pressures in patients with hypertro-
phic cardiomyopathy. Circulation 99 : 254‑261 21. Iwanaga Y, et. al. (2006) B-type natriuretic peptide
strongly reflects diastolic wall stress in patients with chronic heart failure: comparison between systolic and diastolic heart failure. J Am Coll Cardiol 47: 742 ‑748 22. Kawasaki T,et.al.(2013)Usefulness of high-sensitiv-
ity cardiac troponin T and brain natriuretic Peptide as biomarkers of myocardial fibrosis in patients with hypertrophic cardiomyopathy. Am J Cardiol 112: 867
‑872
23. Coats CJ, et. al. (2013) Relation between serum N- terminal pro-brain natriuretic peptide and prognosis in patients with hypertrophic cardiomyopathy. Eur Heart J 34: 2529‑2537
24. Todiere G, et. al. (2012) Progression of myocardial fibrosis assessed with cardiac magnetic resonance in hypertrophic cardiomyopathy. J Am Coll Cardiol 60:
922‑929