>
Originat
Pmper
<Comparative
Study
on
the
Outcomes
of
for
Japanese
Females
with
Eating
D
with
or
without
Alcoholism
Treatment
isorders
Aya
Takeda,
MD'Kenji
Suzuki,
MD
Katsuyuki
Shirakura,
MD
Abstract
Few $tudies on the outcome of patients with eating disordersassociated with alcoholism have appeared
intheliterature.This report isthe first comparative study en the results of treatment foreating disorders with and without alcoholism, The subjects were 42 femaleswith eating disorderswith alcoholism and 88 without alcoholism. They were 30years old or younger, admitted to Kurihama National Hospitalin
1990-1998and subjected to semi-structured interviewsconcerning symptoms of eating disorders,alcohel
depen-dentsyndromes, and other psychiatric disorders.
The
survey was conductedfrom
October
toDecember
2000
byinterview, mail or telephone. Seventy-eightpercent of the subjects responded to thesurvey, and the mean
follow-upperiod was 4.6years.The subjects with eating disorders and alcoholism were c]inically
different
from
thosewithout alcoholism at firstadmission. The former were older, had more personalitydisorders,had
more experience of marriage anddivorce
and had lessanorexia nervosa restricting type than the latter.At
follow-up,
a quarterof the subjects with alcoholism had recoveredfrom
eating disordersbuta quarter of themhad
died.
On
theother hand,a quarterof thesubjects without alcoholism had recovered from eatingdisorclersand a quarter of them had shifted to the mild ferm. Many of the subjects with alcohorism experienced divorcesand continued problem drinking.
The
outcome forpatients with eatingdisorders
withalcoholism was worse than that forthose witheut alcoholism. A common factorfora good outcome
for
patients with and without alcoholism was lessvomiting among the eating disordersymptoms.-
Kley tvoTrts :eating disorder,alcoholism, comorbidity, outcome studyReceived December 5,2001:accepted March 15,2002
'Kurihama National Hospital
(Mdiliug
Address
IAya Takeda, 5-3-1Nobi,Yokosuka-shi,
Kanag-awa 239-0841,Japan)
Japanese Society of Psychosomatic Medicine
NII-Electronic Library Service Japar ユese Soclety of Psychosomatlc Medlclr ユe
摂
食
障
害
と
ア
ル
コ ール
依
存
症
の
武 田合 併 例
の
転
帰調
査
綾* 鈴 木 健二臼倉 克
之 〔抄 録 〕 アルコール 依 存 症を合 併し た 摂食障 害 (合 併 群 ) の転 帰につ い て摂 食 障 害 単 独 群 (単 独 群 ) と の 比 較 研 究である.1990
〜1998年に 受 診 し た 30歳 以 下で半 構 造 化 面 接 ので き た 摂 食 障 害 患 者130
名 に 対 し,2000
年10
〜12月 に ア ン ケート と電 話で追 跡 調 査 を行った.対 象 者 の う ち102
名 (ア8
% )が回答し, 平均追跡 期 間は4
.6
年 で あった.2
つの群 は 初 診 時 に おい て,初 診 年齢, パーソ ナ リ ティ障害,AN
−R
の割 合,結 婚・離 婚 経 験 な ど 多 く の 点で違いが あっ た.調 査時点 で合 併群は非常に高い死 亡 率 (25
% )が あ り,離 婚 経 験 は38
%,問 題 飲 酒 も42
% がもっ て お り, 症状 消失とED
−NOS
が 半 数 を 占 め た 単 独 群 と 比 較し て, 合 併群の長 期転帰は非 常に悪 かっ た,両 群に共 通 した 転 帰 良 好因 子 は嘔 吐 が 少な い こ と で あっ た. ■K 砌ω o脇 :摂 食 障 害,ア ルコール 依 存 症,合 併,転 帰 調 査 はじ
め に 摂 食 障害の転 帰につ い て は, 近 年, 長期 化 ・ 慢性化の傾 向に あ るこ と が明 らか にな り, 欧 米 諸国におい ては, その調査 が盛んに行われ て い る1)2).しか し , わ が国に お い て は, 加茂 ら 3)が こ れ らの文 献につ いて, 長期 的な転 帰 と他の精神 障害の合 併に関して ま と め た もの が唯一存 在す る だ けで, 摂食障害の長期 経過の ま と まっ た年 数の転帰調査 は, い ま だに発表されて いない の が現 状である. ま た わ れ わ れ4)“’6〕は以前 , アル コ ール 依存症 を合併す る摂食障害は , 摂食障害 の 中で も ま た アル コ ール 依存症の中で も治療 困 難な サ ブ グル ープで ある と報告し た.今回は, 摂 食障害単独群 (以下, 単独群 ) とアル コ ール 依存症合併群 (以 下, 合 併群 )との比較を行い, 合 併 群の転 帰に つ い て明 らか に し たい と考 え た.対
象 お よび方
法1990
〜1998
年まで の 間に国立 療 養 所 久 里 浜 病院を受診 し て摂 食 障害と診 断さ れ, 治療を受 け た患者の う ち, 治療期 間 内に半構 造化 面接が で き た30
歳以下の女 性 患者 を対 象 と し た.対 象者は単 独群88
名と合併群 42名で あっ た.調 査時 点でDSM
−IV
に基づ い て摂 食障 害の 診 断 を確定し た.対象者に対して,2000
年10
〜12
月 の問に面接や郵送, 電 話に よ る聞き取 り を実施 し, 現在の病 状や 日常 生活, 社会適 応 状態 な ど を, 「摂食障害の治療状況, 予後等に関 する調 査 研 究 」班の中井らの予後 調査票に基づい て判定を行っ た.ま た,
EAT
26
(Eating
Attitude
Test
),SDS
(Self
−rating
Depression
Scale
)な どのバ ッテ リーも組み合わせた. 200ユ年12月 5日 受稿,2002年
3
月 15日受 理 * 国 立療 養所 久 里 浜病院 (連 絡 先 :武田 綾,Sb 239−084
】横 須 賀 市 野 比 5−3−1) 514 心身 医 ・2002年8月 ・第42巻 第8号 N工 工一Electronlc LlbraryTab且e 1Comparison of symptoms and sociodemographic characteristics at first admission between
eating
disorder
patients with and without alcoholismEatingdisorders without alcoholism (n==70)
Eating
d
正sorders with alcoholism (n= 32)Mean age at first admission (yr)り
Mean age of onset of eating disorders(yr )
Mean
age Qf onset of problem drinking (yr )Diagnosis of eating
disorders
at first admission (% )2 )
AIlorexia
nervosa restrictjrlg type (AN −R)Anorexia nervosa billge−purging type (AN −BP )
Bulimia
nervosa not purging type (BN −NP )Bulimia nervosa purging type (
BN
−P)
Eating
disorders
not otherwise specified (ED −NOS )Mean BMI at first admission
Mean maxiln BMI
Mean minimum
BMI
Co −morbid psychiatric disorders(% )
Depression
Anxiety
disorders2
,Borderline personality disorder”)
Presence
of one of personality disorders3}Family
history(% ) Mooddisorders
AlcoholismEating
disorders3
}Education
(% ) ≦9 ユ0≦ ≦ 12 ≧13Experienced marriage (% )1 ) Experienced divorce (% )2レ Living situation (% )り With husbandWith
parentsAlone or with others
Social
status (% )1 ) HousewifeSfudent
Unemployed Employed 20 .9:辷4.4 17.1±3.7 27 .1 24.310
.0
34.3 4,317 .9±4 .222
.4±3
.6
14 ,8±2.6 30.038 ,610 ,058 .6 12.918 .67 .1 1367 ・ 4 718 匚 J1 447CU7
匚 JQO 匚 」 8 2.945 .734 .317
.1 25 .1±3.8 18.2±3.2 22 .2±2.7 3 .125
.0
9 .4 40 .6
21 .919 .0±4.1 22.5±2 .9 15.3
±2
.6
28.112 .528 .1
ロ 81 .8 ρ 000 匚 」55
122 6 .243 .850
.046 .918 .8 28 .150 .021
.9 25 .09 .452 。ll2 .5 yr :years old , 1 }p〈0 .OOI , 2, p〈0.Ol, 3 }pくO .05結 果
対 象者130
名の うち, 回答が あっ た の は102
名で, 追跡率は78
%,平 均追 跡期 間は4
.6
年で あっ た.回答 者の内訳 と し て は,単独群が70
名, 合併群は32
名で あっ た. 国 初 診 時に お け る対象の特徴 (Table
1
) 1 .年齢 単 独 群に お け る摂食 障害の平 均 発 症 年 齢 は17
.1
±3
.7
歳, 合併 群は18
.2
±3
.2
歳で, 合併 群に お け る問題 飲酒の開始年齢 (アル コ ール 依 存症 発症年齢 ) は22
.2
±2
,7
歳であっ た.初 診 時 年齢 は単独群20
.9
±4
.4
歳 ,合 併 群25
.1
±3
.8
歳で有 意差 (t
=4
.62
,df
=100
, p<0
.001
) 心身 医・2002年 8月 ・第 42巻 第8号 515Japanese Society of Psychosomatic Medicine
NII-Electronic Library Service Japar ユese Soclety of Psychosomatlc Medlclr ユe
があっ た.単 独群は発症 後平 均約
3
年で医療機 関を 受診し てい るの に対して, 合 併群は初診ま で に約7
年を要して い た が, こ れ は合 併群がア ル コ ール症セ ンターで あ る当院に, アル コ ール 依存症の治療を求めて受 診 して い る た めで あ る. 2 .初診時の病状 当院初診時の摂食障害の病状につ い て は, 単 独群で は神 経 性食欲 不 振 症 制 限 型 (AN
−R
)27
.1
%, 神経性食欲不振症 む ちゃ食い/排 出型 (AN
−BP
)24
.3
%と,AN
が半数を占めて お り, 神経性 過食 症排 出型 (BN
−P
)は34
.3
%で あっ た.合併群は,AN
−R
は3
.1
%と少な か っ た が,BN
−P
40
.6
%,AN
−BP
25
.0
% と排 出型 が 多 く, 特定不能型 (ED
−NOS
)も21
.9
%と単独群 の4
,3
%を大 幅に上回 り, 両 群の間に は有 意差 (X2
=13
.6
,df
=1
,p
くO
.Ol
)が認 め られ た.3
。初診時の合併精神疾 患 両群 と も, 初 診の段 階で摂食 障害 以外に も別 の精神 疾 患を抱えて い る こ とが多か っ た. うつ 病は両群ともに約30
% もっ て お り, 不安 障害は 単独群で38
.6
%, 合併群で12
.5
%と単 独 群が 有意に高 く(X2=・9
.9
,df
=1
, p〈O
.Ol
), な ん らか のパ ーソナ リ ティ障害を合併して いる者 も 単 独群58
.6
%, 合併群81
.8
%と合 併 群が有 意 に多 く(X2=5
.0
,df
=1
,p
<0
.05
), さ らに, 合 併 群 に お ける境 界 性 人 格 障 害 (borderline
persenality
disorder
;BPD
)は28
.1
% と, 単 独 群10
.0
%よ り も有 意 に多 く存 在 して い た (λ:2=5
.5
,df
=1
, p<0
.05
)。 4 .初 診 時の家族 的 ・社会的状 態 家 族の既往歴 として は, 気 分 障害や アル コ ー ル依存 症 な ど がみ ら れ た が, 摂食 障害 を抱えて い る者が 家 族の 中に存在してい る割合は, 単独 群7
.1
%に対 し, 合 併 群は25
.0
%と有 意 に 多 か っ た (X2 =6
.3
,df
=1
, p〈0
.05
). ま た, 結 婚 経 験や離 婚 経 験 におい て は, 前者が単 独群5
.7
%, 合併群46
.9
% (X2
=24
.5
,df
= =1
,p
〈0
.001
)で, 後者は単独 群1
,4
% ,合併群18
.8
% (x2=10
.3
,df
=1
,p
<O
.Ol
)と有 意差が認め ら れ た.それ に伴っ て生活形 態に も差があり, 単 独群で は両 親 と同 居 して い る者が88
.6
% と大 半を占め た が, 合併群で は両親 との同居は半数 に と ど まり, 夫 との同 居28
.1
%, 一人 暮 ら し21
.9
%な ど多彩で あっ た(X2・ ・18
.2
,df
=2
,p
〈O
.0041
).初診時の社会的立 場 と し て は, 単 独群 は学生が45
.7
% と多か っ たが, 合併群は 単 独群 に比 べ る と 主 婦が25
.0
% と多 か っ た (X2=22
.3
,df
=3
,p
く0
.001
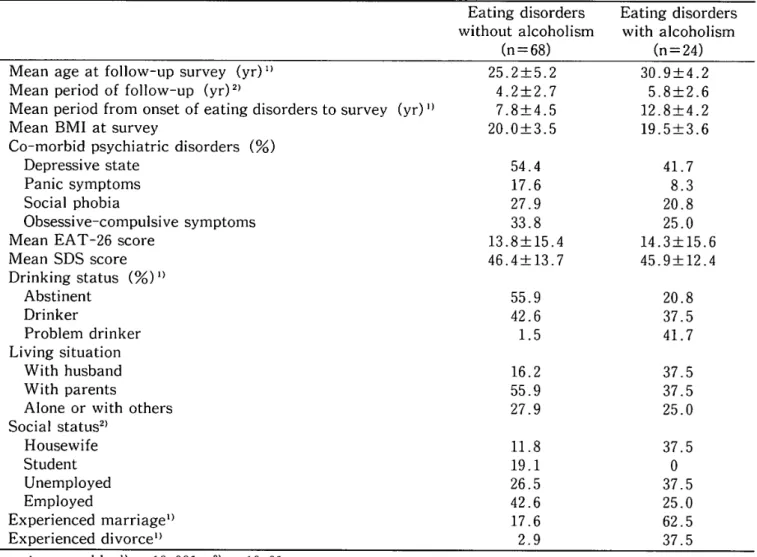
). 圍 調 査時に おけ る対象の特徴 (Table
2
>1
.年齢 調査時に おける対 象の年齢は,単独群25
.2
±5
.2
歳で,合 併群30
.9
±4
.2
歳で有 意差 が あっ た (t
= 4 .79
,df
=100
,p
〈0
.001
).平均追 跡期 間は単 独群4
.2
±2
.7
年, 合 併群5
.8
±2
.6
年で あっ た (t=2
.49
,df
=100
,p
<O
.Ol
). 2 .調査時の合併精神疾患 アル コ ール 問 題で は, 合 併 群に問 題 飲 酒が41
,7
%に存在 し, まっ た くな ん の問題も な かっ た単 独群の間に有意 差 (X2=24
.7
,df
=2
,p
<0
,001
)がみ ら れ た.3
.調査時の社会的状態 単独 群は,調 査時も両親との同居が55
.9
% と 最 も高い 割合を占めて い るが, 初 診 時よ りも30
% 近 く減 少し, その ぶ ん, 夫 と の同居16
.2
% や一人暮らし27
.9
%に移 行して いた.合併群 も 両親 と の同居が37
.5
%に減 少 し て, 夫 との同居 が増加して い た.調査時の社会 的立場で は, 単 独群は学生 が19
.1
%に減少 して, 定職に就い て い る者が42
.6
%と増加して い た.結婚 して主婦 にな る者もll
.8
%に み られ た.一方, 合併 群に は学生がい な くなっ た が, 主婦や定職に就 く者 も減少 し,無 職が52
.1
%と初 診時よ りも増加し ていた (X2=13
.1
,df
=3
, p<0
.005
).ま た, 合併 群は62
.5
%が結婚を経験してい て, これ は 単独群の17
.6
%を大 幅 に上 回っ て い る (X2=17
.2
,df
=1
, p<0
,001
)が, 離婚経験も37
.5
% 516 心 身 医 ・20e2年 8月 ・第42巻 第8号 N工 工一Electronlc LlbraryTable 2Comparison of responses in fol璽ow −up survey between eating disorder
patients with and
without alcoholism
Eating disorders Eating disorders
without alcoholism with alcoholism
(n=
68
) (n==24
)Mean age at follow−up survey (yr )1}
Mean period of follow−up (yr)2)
Mean period from onset of eatjng disorders to survey (yr)1 )
Mean BMI a亡survey
Co
−morbid psychiatricClisorders
(% )Depressive state
Panic symptoms Social phobia
Obsessive
−compulsive symptomsMean EAT −26 score
Mean
SDS
score Drink{ng status (% )1} Abstinent Drinker Problemdrinker
Living situation With husbandWith
parentsAlone or with others
Social
status2 , HousewifeStudent
Unemployed Employed Experienced marriagei 〕 Experienced divorcel) 25 .2±5
.2 4.2±2.77
.8
±4.5
20 .0±3.5 54 .417
.6
27 .9 33 .813 .8±15.4 46.4±13.7 55.942 .61 .5
16.255 .927 .9 11 .819 .126 .542 .617 .62 .930
.9
±4.2
5 .8±2 .6 12 .8
±4 .2 19 .5±3 .6 41 .78
.3
20 .8 25 .014 .3± 15.6 45 ,9±12.4 20.837 .541 .7
37 .537 .525 .037
,5037
.525 ,062
.537 .5 yr:years old, ]) p〈0,001, 2)p〈0 .01 と単 独群の2
.9
% を 上 回 り, 両 群 間に は有意 差 (X2=17
.0
,df
=1
,p
<0
.005
)が認め られ た. すな わ ち, 合併 群は結婚 経験 者の うち約60
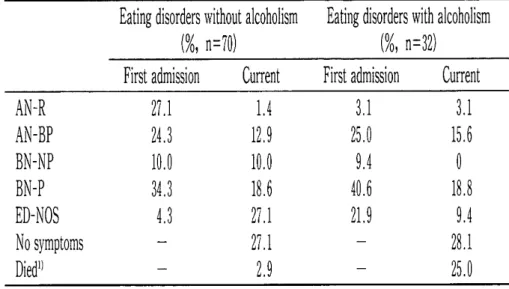
%が 離 婚し て い る とい う, 非常に高い離婚 率を有 し て い た. 圄 単独群 と合併 群の病 態変化 (Table
・3
) 初診 時と調査時に おけ る両群の病態変化を調 べた.約5
年を経 過 した調 査時 点で は, 単独 群 の27
.1
%,合併 群の28
.1
%に症状消失が み ら れ た.さ らに 単 独群で は,AN
−R
がL4
% と減 少し たの をは じめ, い ずれ の病態も割 合は減 少 し てい た.ま た ,EI
} −NOS
が初診時の 4 .3
%か ら27
.1
%と増加 し, ここ に も症状軽 快の徴候が 確認さ れ た.合併群も同様の傾向が認め ら れ た が, 初診 時に は単 独群よ り も多くの割 合を占め て いたEI
}NOS
も一緒に減少し た.一方,合併 群の 死亡率は25
.0
%に上 り, これ は単 独 群の2
.9
% を 大 き く上 回 る結果と なっ て いて,死亡 者 の割合 は両 群 に有 意 な差が認 め られ た (κ2=9
.8
,df
=1
, p〈0
.005
). 囚 転帰不 良因 子の抽 出 (Table
4
) 単 独群で有 意差の あ る転帰不良因 子 は, 初診 時年齢が高い こ と(t=2
.3
,df
=68
,p
〈0
,05
),AN
−R
以 外の病 態で ある こ と ( X2=8
.O
,df
=68
, p<O
.05
), 過食の頻度 (X2 =4
.1
,df
=1
,p
〈O
.05
)や嘔吐の頻度が高い こ と (X2=5
,0
,df
=1
,p
〈0
.05
), パ ーソナ リ ティ障害を保有し てい るこ と (X2=6
.6
,df
=1
, pく0
.05
)の5
項 心 身 医・2002年8月 ・第 42巻 第 8号 517Japanese Society of Psychosomatic Medicine
NII-Electronic Library Service JapaneseSociety of PsychosomaticMedicine
Table
3Cemparison
of
outcome
between
eating
disorder
patients
withandwithoutalcoholism"Nca
Eating
disorders
witheutalcohelism(%,
n=70)Eating
djsorders
withalcoholism(%,
n=32)First
admissionCurrent
First
admissionCurrent
AN-RAN-BPBN-NPBN-PED-NOSNo
symptoms
Diedi)
27,124,3le,o34,34,3
L412,910,O18,627,127,12,9
3,125,O9,440,621,9
3,115,6o18,89,42S,125,O
i)
p<o,O05
ij,Npss"gN"oc,tu,uskex
encoq]
Table4Comparison
of
clinical
characteristics
atthe
first
admissionbetween
good
outcomegroup
andbad
outcomegroup
amongtwo
subjectgrollps
Eating
disorders
withoutalcoholisrnEatingdisorders
withalcoholismGood
eutcemes(n=38)
Bad
outcomes(n=32)
Good
outcomes(n=12)
Bad
outcomes
(n=20)
Mean
ageoithe
first
admission(yr)i)
Mean
ageoionsetofeatingdiserders
(yr)2)
Mean
ageofonsetofpreblem
drinking
(yr)
Diagnosis
ofeatingdiserders
at
the
first
admission
AN-R
AN-BP
BN-NP
BN-P
ED-NOS
Binge
eating
more
than
2
times
per
week(%)`]
Vemiting
more
than
2
times
per
week(%)5)
Mean
BMI
at
first
admission
Presence
of
one
ef
persenality
disorders
(%)G)
(%)3)
19,9
±i4,216,6
±3,7
34,2
15,8
13,2
28,9
7,9
60,8
36,817,9
±3,8
44,7
22,3
±4,417,7
±3,7
18,8
34,4
6,2
40,6
o
75,O
62,517,8
±4,7
75,O
25,3
±3,819,4
±3,421,8
±3,1
8,3
25,O
8,3
16,7
41,7
58,3
41,719,6
±3,4
75,O
25,4
±3,17,7
±・3,22,3
±2,
4o2
o
25,e
10,O
55,O
10,O
89,5
78,918,7
±3,6
85,O
Good
outcemesInosymptomandED-NOS,
Bad
eutcomes1AN,BN
anddied,
i)
Good
outcomesvs,
bad
outcomesamongsubjectswithoutalcoholism(p<O,05),
!)
Geed
outcomesvs,bad
outcomesamongsubjectswithalcoholism(p<O,1),
3)Goed
outcomes
vs,bad
outcomesamongsubjectswithoulalcohe]ism(p<O,1),
`)Goed
outcomes
vs,bad
eutcomesamongsubjectswithalcoholism(p<O,05),
i)
Good
outcomesvs,bad
eutcomesamongsubjectswithoutalcoholism(p<O,05),
E)Good
outcomes
vs,bad
eutcomesamongsubjectswithoutalcoholism(p<O,05),
amongsubjectswithalcoholism
amengsubjectswithalcoholism
(p<O,1),
(p<O,05),
目で あっ た.一方,合併 群に お い て は,
ED
−NOS
以外の病態を 示 してい るこ と(X2=7
.8
,df
=4
,p
くO
.1
),過食の頻度が高い こ と(X2 =4
.1
,df
= =1
,p
〈0
.05
), 嘔 吐の頻 度が高い こと(X2 =4
.5
,df
=1
, p<0
.05
)の3
項 目で あっ た.す なわ ち, 両 群に共 通 す る転帰 不良因子 と し て は, 過 食や 嘔 吐が頻 繁 に行わ れ るタ イ プ とい うこ と が わ か っ た.考 察
本研究は, わ が国の摂食障害の転帰に関す る 研究であるが, 同時に, ア ル コ ール 依 存症が合 併し た摂食障害を一つ の集団と して ま と め, そ の転 帰 を明 らか に した もの と して は, 国際 的に も初めて の研 究で あ る.欧米諸 国の転 帰調査を 総合的に み て み る と, 追跡期間に幅は あ る も の の ,5
〜10
年の調査で は,AN
もBN
も少な く と も半 数以上が 良好な転 帰 をた どっ て い る と の 報 告が な さ れ てい る8).今回のわ れ わ れの結 果 に お い て も, 単独群の半数 は 同様の傾 向を 示 し た が, その 一方で , 合 併群の転帰は深 刻な もの で あっ た.そ れ は, アル コ ール依 存症とBPD
と い うど ち ら もハ イ リス ク な疾患が関与し てい る こ とにある と推 測さ れ る.わ れ わ れ4)’−6)は以前 , 合併例の 臨床的特徴に関す る論 文の中で, 合併 o 群は臨床 的に治療 困難で ある とい うこ と も発表 し たが, 転 帰調査に も そ れが 表れて い る とい え る. しか し, なに よ り も特筆すべ きこと は, 合 併群が 示 す25
% とい う死 亡率の高さで あ ろ う. 一般 的な精神 疾患 と比べ る と , 比較 的その死亡 率が高い と さ れて い るAN
で も, そ の割 合はTheander
らs)の 報 告で20
年で20
%で あ る.BN
に お いて は1
〜3
%にすぎず,AN
よ り も さ らに少ない7).これ ら従 来の値 を大 き く上回 っ てい る合併群の死亡率に関して は, 今後死因な どを含め た検 討の余地 が あ ろ う.ま た, 単独群 と合 併群の転帰 不良群 を検 討 する と, いずれ も, 発症か ら医療機 関受診まで の期 間が 長い こ と や,過食や 自己誘 発 嘔吐が頻 回で ある こ と,パ ー ソ ナ リ ティ障害が存在す るこ と, とい う条件が あ げら れ る が,欧米で報 告さ れ たAN
,BN
に お ける もの9)と同様であ っ た.これ らの こ とか ら, 疾 患の早期発 見が摂食 障害の治療に お いて も, 転帰に影響を及ぼ す一つ の要素と し て あげられ る. 本 研 究は,平 成12年 度 厚 生 労 働 省 精 神・神 経 疾 患 研 究 委 託 費 補 助 金に よっ て行っ た.ま た, 本 論文の一部は第 42回N本心身 医 学 会 総 会 (2001,鹿 児 島 )に おい て発 表 し た. 文 献1)
Zipfel
S
, Lowe B , Reas DL , et a1 :Long −termpregnosis in anorexia nervosa :1essons from
a21 −year
follow
−up study 、 Lancet355
:721
−722,2000
2)
Fairburn
CG
,Cooper
Z
,Dell
HA , et al :Thenatural course of bu]imla nervosa and binge
eating disorder in young women . A rch Cen
Psychiatry 57 :659−665,2000
3) 加 茂 登 志 子, 笠 原 敏 彦 :摂 食 障 害の長 期 転 帰 と
Comorbidity .精 神 医 学 40 :234−246, 1998
4)Higuchi
S
,Suzuki
K , Yamad 且 K , et al :Alcoholics with eating
disorders
;prevalenceand clinical course . A study from
Japan
. Br /Psychiat門)」 162:403−406,1993
5)
Suzuki
K , HiguchiS
, Yamada K, et al :Bulimia nervosa with and witho しlt alcohol −
ism
:acomparative study inJapan . Int/EatI)isord 16:137−146,1994
6)
Suzuki
K , HiguchiS
, Yamada K, et al : Young female alcoholics with and withouteating
disorders
: a comparative study in
Japan
. Am /Psychiat2s
, 150:1053−1058,
1993
7)Keel PK , Mitchell
JE
:Outcome
inbulimia
nervosa . Am /Pミychiat疋y 154;313−321,1997
8)
Theander
S
:Outcome
and prognosis in anor −exia nervosa and bulimia:some results of previous investigations, compared with those
of a
Swedish
long−term study ./Psychiatr
Res
19:493−508,1985
9
)Steinhausen
HC
, Rauss −MasonC
,Seide
R :Follow −up studies of anorexia nervosa :a review of four decades of outcome research .