mo\as?lklj!
fibllfs
ee
18
gee
4
e435
--
443S
(1991
a!
)
PhysicalTherapy
A
for
F
Case
acial
Palsy
after
Stroke:
Study
*MasamichiFURUSAWA*',
Noriko
SATO,
Fujio
KOMA,
andHidetakaReiko
TAKEMURA,
SHIINA
Abstract
Facial
palsy subsequent toa strokeinterferes
with nonverbal commuriication.Because
such facialpalsy isof central origin, itiseasily influencedby attenuation of balance reactionsor by abnQrmal postural tone from the shoulder girdles and the pelvis.Intreatment we thus
firstwork
to
normalize posturaltone
throughoutthe
wholebody
andto
foster
the
emergenceof normal
balance
reactions and posturalmotor patterns.Only
after thisinitial
stepdo
wedi-rectly approach thefacialpalsy itself.
To objectively examine this idea,we decided toclosely rnonitor the progress of a
57-year-eld woman admitted to our hospitalone year and one week after suffering a stroke resulting
in
facialpalsy. Both the physical therapy and the speech therapy departments worked in close collaboration teimprove formulation and symmetry of facialexpression, and towork on finely
grading movements involved infacialexpression. To monitor our progress we recorded
cha-nges by photographs inthe center of gravity,manual muscle testsof
facial
muscles, andelec-tromyographic
activity. To assess thedegree
ofdrooping
of the eyelids, we recorded changesinthe vertical distancebetween theupper and lower eyelids.
Treatrnent
continuedfor
five
months and three weeks.The
improvements
weindicated
approaching the whole body beforetrying to treatonly thefacialregion,Key
Words:
Stroke,
Facial
Palsy,
Physical
Therapy
1.
Introduction
Facialparalysisresulting from a stroke typically
involves
asymmetry of posturingfor
socializingbe-havior and thus an impoverishment of
gesturing,
due
mainly to poorlyfunctioning
balance
reac:.
fimaVas,Pacvafiexpt/NOpaMtazaOitst
"'・th'ewEpt,
rtma・as-
±M,
rrNn?,
vaieefi.:],
tieist-
1'.Ekfisc
BobathHospital
(Received
21 Octeber 1989/Accepted 26 1990)megptfi
・
Novembertions.
Because
an abundant repertoire offacial
ex-Pressions
is
important
for
communicatingideas
be-tween persons, the inabilityto
do
this togetherwith a prevailing asymmetry in
facial
expressionresulting from paratysisinterfereswith the
non-verbal communication and so adverse!y affects a
patienVs
iRteraction
with society,
We
have
previously advocated treating the pa-tientwhohas
facialparalysisdue
to a stroke orother central nervous disorder by noting that the
pos-436
ve\tsza#
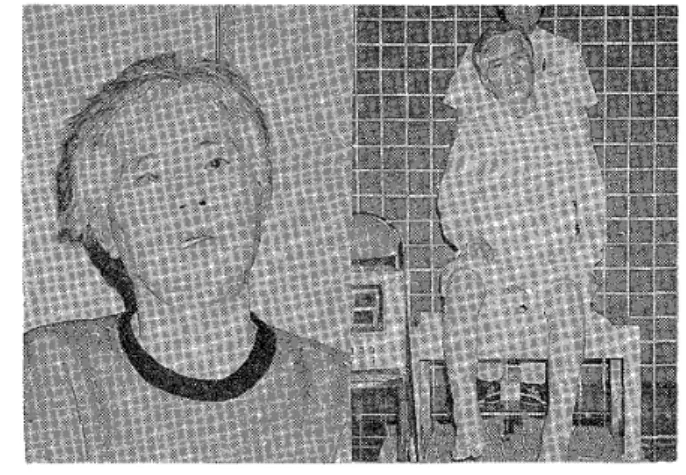
Fig.1 At the time of
hospitalization.
(Left)
Flaccidparalysisof the right side of the
face.
(Right>
Inability to remain seated because of fiuctuation andliability
to fallwards tothe left.
turaltone and posturalmotor patterns
in
theshoul-der
girctEeand trunk,andby
striving toremove ab-normalinfluences
and abnermal compensatoryad-justments
throughout thebody'Sl
In
thisstudy weclosely examined this
idea
by
studying a patientwho suffered paralysis inall four Iimbs as well as
inthe facialregion
following
ahemorrhage
inthebrainstem.
2.
Methods
The
subject was a 57-year-old woman who hadsuffered a hemorrhage inthebrainstem with
subse-quent ataxia,
Millard
Gubler
syndromee), fiaccid pa-ralysis on theright side of the face(Fig.
1,le'ft),andlefthemiparesis. Although she had undergone
sur-gicalrepair of
her
right eyelid, itdrooped
marked-ly. Computerized tomography taken immediateLy
after the onset had shown the hemorrhage to be
located in the right poFterior region of the pons.
She had undergone conservative treatment, whjch
included physical therapy
in
the laterstage. At one year and one week after the onset, thesubject was admitted to our hospital,We
chose to study a relatively "oldintractable"
case such as
hers
be-cause, asNikiiO'
has
pointed out, after a certainperiod of time
has
elapsed, ifa treatmentis
in-eg
18tseg4
ig
itiatedand produces a change, such change can be attributed to the treatrnentitselfeven though no
control group
is
inciuded
as partof the study.To study thissubject we performed the following
assessment.
1) A video camera recorded the subject sitting on the edge of a bench,and pictureswere produced
on
thermosensitive
paper via a special video camera processor. From the resulting photographswe measured
inclinations
of thehead
and trunkin
'
the frontalplane and in the leftparasagittalplane.
These
measurements were takenin
accordancewith standards published by the Physical
Dis-cibilities
Committee
of theJapanese
Orthopaedic
Association.
2) With the subject in thesame seated position,
but with
both
subject andbench
on alarge
plat-form thatcould measure the center of vertical pres-sure, we measured
fiuctuations
in
thecenter ofgra-vity
over a period offive
seconds.・A
videorecord-ing
of the subjeces p6sition was also taken at thistime and synchronized to the analog
center-ef-gravity information via a custom-macle device. 3) Photographs were taken of the subject's face
during
relaxation, during smiling, and during pro-nunciations ofthe
sounds/a:Lli:/
and./ua:f.
We performed manual muscle tests according toDanieLs'"
on the anterior portion of theoccipito-frontalisas thesubject triedtowrinkle herforehead, on the corrugator supercilii as she triecltofrown so
as
te
produce wrinklesbetween
her
eyebrows, onthe zygomaticus major as $he triedto smile, and
the
depressoranguli oris as she triedto
frown.
4) We measured the vertical distance between
the eyelids
to
as$ess the diMculty inclosing of herright eye.
5)
With
surface electrodes, we recordedelec-tromyograms bilaterallyof thefrontalis, zygomatic-us major, and depressor anguli oris. Video
record-ings
were synchronized with the electromyogramsby the aid of thedevicernentioned in2)"'.
6) Retention of food introduced intothe mouth was asse$sed using a four-stepscale
(Table
1)be-PhysicalTherapy forFacia
Table
1
Ability
totakefood
into
the mouth1Palsyafter Stroke
3
iNothing spitled or tiropped.2
lVery littlespilled ordropped
1 1Occasionalspilling or dropping
O
lMost food spMed ordropped
cause thissubject had diMculty keeping her iips
closed.
The above assessment was performed at both
ad-mission and discharge so that we could see what changes took placeduring the hospitalization.
3.
InitialAssessment
When firstadmitted to our hospitag,thesubject
had diMculty'in maintaining sitting because of
no-ticeablefluctuating movements arising from the
pelvic region while the
left
trunk musculatureap-peared
fiaccid.
She
tended tofall
posteriorly
and toher
left,
se she compensatedfor
thisby
fiexing
thetrunk
forward
tokeep
her
center of gravity low, and bytilting
herhead totheright with hyperexten-sion at thene ¢k(Fig.
1,righO,Because
ofdi'Mculty
in
cLosing her mouth(Fig.
1,
lefO,food would tend to
fall
out of the right-handcorner of the mouth
(score==O>.
When
trying to pronounce!a:f,
her
head would tiltevenfurther
to the right and go into further hyperextension, andher mouth would open wider than normal
(Fig.
2,left).
The
subiecthad
little
selective movement of hermandiblc, and could not carefully grade the speed
of her movements with it,Ifshe triedto pronouce
li:L
her lipswould be pulledstrongly over to theleft
(Fig.
3,
lefO.
This
maiked asymmetry wasdue
to the
inability
to grade movements of the left cheek musculature, the zygomaticus major, and thedepre6sor anguli oris, which would contract in an
all-or-none
fashion,
as we!1 as a poor abilityto
pro-duce contractile activityin
the eor'responding mus-cles on the right.Attempts topronounce
/u.L:f
revealed weakactiv-ity
in
the orbicularis oris,renderingher
unable toadequately round her lipson the right side of the
:A Case
Study
437mouth
(Fig.
4,left).When
smiling, the right zyg-omaticus major could not contract suraciently, sotheright corner of the mouth wou}d
・sag
while the mouth as a whole wouldbe
pulledtothe
left
(Fig,
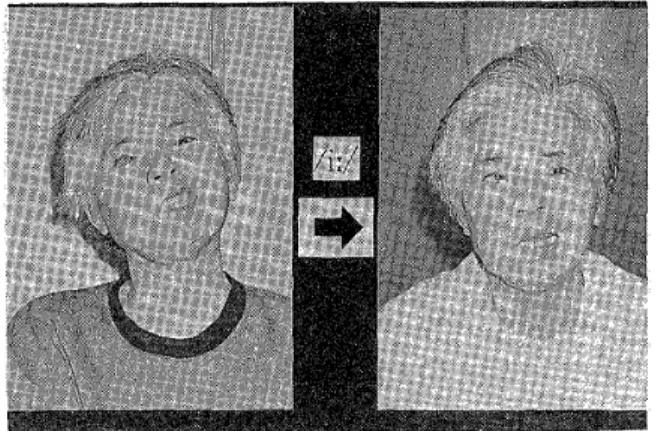
5,left).The results of initialmanual musc!e testingFig.2 Pronouncing the
la:/
sound.{LefO
Before
thetreatment,(Right)
Five months and three weeks treatment.after the
Fig.
3
Pronouncing theli/1
sound.
(LefO
Beforethe treatmenL(Right)
Afterthetreatment.Fig.4 Pronouncing the
fui:/
sound,CLeft)
Beforethe treatment,(Right)
Afterthetreatment.438 wa*tszae#
are shown inTable 2.
Drooping
ofthe
lower
eyelid,in
spite of asurgi-cal procedure to correct this
problem,
was asno-ticeableas ever.
Contraction
ef theorbital portionof the orbieularis oculi was absent.
As
a result ofthis,conjunctivitis was evident.
4.
Treatment
While
the subject was in our hospital,she hadfivephysical therapy sessions per week, 40 minutes
per session,
for
five
months and threeweeks.The
physical therapistnot enly worked on regaining
her abilities to waik and to sit, but also streve to
improve her facial expressions. Because the subjecV$ ataxia and
dysfunction
ofliP
rnusculatureimpaired
her abilityto
speak well, a speechthera-Fig.5
Smiling,
(Left)
Before
thetreatment.<RighO
Afterthe treatment,Table 2 Eyelid;manual muscle test;ability
to take food intothemouth
(Beginning
:thebeginning
of thetreatment,End
:theend ofthe treatmenOBeginningEnclRight eyelid vertical distance
when closed
5mm 3rnm
Eyelid dreoping COIISPiCUOUSinild
MMT
Rt.frontalis
Rt.corrugator supercilii
Rt.zyg'omaticus major
RL depressor anguli oris
RL orbicularis eris oloo1 1-3 3 3 3 4 Abilitv to take foed intethc
mouth
o 3
eg
18igce
4e
pistworked with her
three
timesweekly, 40 minutesper session, The following account
briefiy
summa-rizes hertreatment principallyinphysicaltherapy.
The
first
task was toregain symmetrical sittingby encouraging trunk extension while maintaining
cocontraction of pelvic and trunk musculature.
The two principalproblems were
lack
of tonein
the lefttrunk muscles and poor balance reactionsinsitting. Having thesubject try toassume sitting
from a position of lyingon her right side was one way to bring activity
into
her
lefttrunk muscles(Fig.
6,right}. This task al$o induced her tobringher head from a right-tilted position
(Fig.
1,
right)tothe midline.
Then,
by
having
the subject stand and attemptshallow squats, cocontraction of
the
pelvic and trunk musculature could beencouraged ina differ-ent way(Fig.
6,lgfO.When she elevated her right arm, the lefttrunk musculature was induced to maintain activity throughout the task.
As
shebecame
able to perform shallew squatsmore easily, she was then
instrueted
to performthem arbitrarily
faster
or slower,for
thiswould re-quire careful grading control of many musclesthroughout thebodyi3-ie]t8'.
Such
sensorimotor expe-rience served as a preparationfor
thecarefulgrad-ing
control ofher
teft
facial
muscles.As
thecon-tro]oyer shallow squats improved, fluctuationsin the
locus
of thesubject's standing center of gravityFig.6
<LefO
Shallew squatting to increase postural tone.(Rjght)
Coming up from tyingon the right sideto augment tonic activity in the left
Physical Therapy forFacia
began todecrease,and she was more easily able to assume a symmetrical posture when seated,
Through
the
above activities, shebecarne
ableto
maintain her head ina midline positionand to hold her mouth closed,
The therapist then directed treatment to facial expression. Most of the
facial
muscles attach tothefacial
skin, requiringdelicate
methods of making expressions.This
part of treatment began with thesubject
in
supine,because
her
head
could easilybe
stabilized and the effects of gravity were elimi-nated,The
right platysma was overly shortened,tending topulltheright cheek and right side ofthe
mouth downward. Any movement requires an
ap-propriate degree of fixation.Inthe case of the
rig-ht-hand corner of the mouth being pulled during enunciation of the
li:/
sound or of the zygomaticus major contracting during a sniile, the levator labiisuperioris alaeque nasi and zygomaticus minor
must play the role of central fixators.The
thera-pist thus induced contractile acti"ity with his
fingers
on Lhe upper cheeks alongboth
sides ofthe
nose
(Fig.
7,
left).Fingers were also used toinhibitexcessive activity on the
left
side ef theface
due
todysmetria.
The
next task was tohave
thesubject shapeher
mouth for the
fi:f
sound and to have her smile(Fig.
7,right). By having her phonate with theli:!
sound weakly so that only mild muscular contrac-tions could beobserved, the tendency forthe lipstobe pulledleftward could
be
prevented. The subject was then to shape her mouth forthe!ua:/
sound(Fig
8,
lefV.The therapist manuaHy assisted her inrounding
her
right side ofher
mouth.The therapi$t likewise provided manual
assis-tance tothe
drooping
right eyelid tohelp
elicitac-tivity
from
the orbitarportion
of the orbicularis ocutiby
helping
elevate thelower
eyelidduring
eye closure
(Fig.
8,
right),The
therapistalsohelped
bring
about activity inthefrontalis
toproducehor-izontalwrinkles across the
forehead
and in thecor-rugator supercilii to produce vertical wrinkles
be-tween the eyebrows. Ineach of these instancesthe
1Palsy after Stroke:A Case Study 439
facialmusculature on theleftside was hyperactive and nbeded tobe inhibited,so only slowly perform-ed contractions were elicited,with gradual stepwise
increments of effort.
Sometimes
the subject used a mirror inorder to control herfacialexpressions easily by herself.
5.
Results
'
At
first
the subject haddiMculty
insitting, butby
the time ofdischarge
she could sit on the edgeof a chair and elevate both arms. She became
capa-ble
of walkingif
given support underher
left
arm.Anteroposterior
fiuctuation
of thelocus
ofher
center of'gravity over a period of five seconds
while seated improved from 12,5cm to 3.3 crn
(Fig.
9). Analysis of head and trunk angles during
Fig.
7
(Left)
Facilitationof stabilizing eontractiletivityinsuch muscles as the levater
labii
superioris alaeque nasi and zygomaticus
rnlnor.
・
(Right)
Trainingfor
enunciating thefi:/
sound and forsmi!ing.
Fig.8
(LefO
Trainingfor
enunciating the/ui:/
sound.(Right)Treatment toassist
in
closingthe
right eye,440
ue\thza\
sitting, as recorded
by
thevideo
copy processor, showed thathyperextensioll
of the head decreasedfrom,27
degrees
to9
degrees,
and that the tiltofthe
head
tothe right improved from13
degrees to3
degrees,
and that a sevendegree
tiltof the trunktothe leftwas corrected toa two degree tilttothe right
(Fig.
10).
Along
with this,closure of thelips
and mandible became
possible
when the subjectwas not under stress, and so her scere foringesting
food
improved
frorn
zero tothree(Table
2).When she attempted to close hei eyes, the verticaldis-tance
between
eyelids on theright decreased fromfiveto three millimeters, and the drooping of the eyelid
became
less
apparentThe
conjunctivitis in that eye had inthemeantime abated.
The
manual muscle test revealed changesin
strength of the
frontalis,
corrugator, zygomaticusmajor,
depressor
anguli oris,and orbicularis oris,asshown
in
Table
2.
Photographic
evidencecen-firmed
thatasymmetrydecreased
when thesubjectshaped
her
mouthfor
the/a:L
/i:L
andfur:/
sounds, as well as when she smiled
{right
picturesin Figs.2-5). Electromyographic activities of the
depressor
anguli oris muscles exhibited a shift froma marked asymmetry situation. The right frontalis
and zygomaticus major muscles, on
the
otherhand,
showed no substantial changes(Fig.
11).
6.
Discussion
The factthat the mouth of thissubject
continual-ly
remained open was particularlyapparent whenaccompanied
by
hyperextension
at the neck.As'
control of the extension of the trunk
improved,
ataxic
fiuctuations
in
movement decreased, whichin
turn enabled thehead
to assume a more erectpositions.AIIef thesechanges appear to
have
con-tributed to helping her maintain closure of the
mouth more easily.
The
exaggeratedflexion
of theh6ad
to theright,which
interfered
withthe
subjecVs socializingbe-havior,resulted ina shortening of the right
platy-sma. As
the
leftward leaning ofthe
trunk
wascor-rected toward the midline, the head and neck
as-za
18ges
4・g
[Beginning]
Front
Lt
Fig.9 m Rearduring
sitting,[End]
Frgnt
.,.tt,'rfff・・・1,y.・v'f''7,/t/tttN
e・'[..t{・Ftttt't.3.3cm
.3.1cm
.O.05V/CM)iIRear
Rt,Fluctuation
inlocusof center of gravityli1
1
Fig.10
Changes
inposture after fivemonths andthreeweeks of treatment.
sumed a more symmetrical position,suggesting
that
the
positionof thehead
had
belen
establishedas a compensatory result to orientate the trunk.
This
case illustrateswell the observation thatfacial paralysisaccompanying a central nervous disorderPhysical Therapy forFacialPalsyafter
Strokei
ACase
Study
441'Rt.
Frontalis
Lt,
[Beginning]
tttttt
l'L...IT.'ttl.//・ 1t---1--・tit/ttt/ttt11・.'-ett''...'--t
i・ 1--IF-'L..(Fg.fe.headtttttttwrinkl[/.n.g)g./tt:--5oollT/tt.11 i'1l,....
'2sec・''ttttttt/itattrttttttttt//t""1"'rL,.#.I--I=;,':・ir;'...
//・t,・/・,・/-,
.-
,・.[
'
---
1-
-L
.
---
I t.l,・t//t..
.//.
/. ,hi,"i'-lt1./-t'Yt/
ttt''/i''l"
''
i'/ttt/tt'ttt
'.1",/'',
tt/t
t
tt
'l""'
"''t'
;'.
[End]
-"
.--e-.'t'tTn':tt
Rt,
Zygomaticus
'
ma)orLt.
-L・.L=・-L..,IILL
s.-t-j---ttttf--ii-g"'11!..-:t・-:1tt-t
cr:・E・・I.I.-I'/t/ttttttltltt.ttttt/ttttttttttt..t....t.l../.L-..".t
・--fiN=.l--・-・l・.rmTmTLttt.
'-i(Smiling)
'/'t't''1'1'''''
tt'l"t---..tttlt.:tl--t-t--tt:-'J'l''-L.tLi:ttt
t
'Flil.tt・1"i]l"l--iIf
ttiIl
tt/ttt/t'
t'r'1'1-r,"tt
I---;--t,1/./..'tt'1/rt'ttttt//.././t.I/・・btt
lttttttT-:''l'.-.・tl
ll1
I...11...l,.1i1l':r'
r/1/t111
.
/N:.-,/
--・
111-1・1-''.G,・:].
i 1;--.ttt..tl..'...i'.I..1..t1-trrt../''
tt1・-,1-/・1t//itttl-.!L.i/=,1/'.i,..i,iElt.t.tl.rtttt"'1.'T''
2U.-tt-,-tt1 1''t'
l.,/F't''"/='''tl,li,ilri;.l,/..,,
tL.'・'/',・.・,'・'',.r.・・-,,.,1'./1./ttt/tlt・/
i,・,/.
il-l-!,1:,..tt,p・
・1titti1ir./..i1"'1i't'[・1-・
-t.
Rt.
Depressor
.
Fig. 11
Changeg
in electromyograms after five months and three weeks of treatment.・11
/..1-11/-t/.lttttttt..../I-
!/tttt'vll''
1・ttlt・-/tttttttt1/FT/ttlttt/tt./
,/.t.tt.tt'1'-..・ll・
1...t.'tt1tttt'tt
't'''
"'1'11,'/''/..m.'t'-'f'iTr'!l-tt..tt:tt-i4L.・''..t.tt..//illli,il/.・11111//-'
-ttttttt
tt'/
/・t.F-..V'tt.t...tt.t
.ttht..1'"t't't
.t.r:.tr''T"''rl-,.,'..1...1.'.t.-・.l./.,lt7-'.-・tt'--e
..t'
ttt・1/・,.il''
t/.
tt'
'L
-1-...t.4-t;,L.j''1.-e
;'ttttajI-i-:-t--.1-,..ttttttH-h.'::.h・/---.
l'4i'r-l:-l..t-tJ-''i:-iH:ll.'==itt.E
lllZ-,t-"iiti'2
',4--.,.・--・i・--・-can
be
easilyinfluenced
by
compensatory measuresor abnormalities ofthe trunk.
The fact that the leftfacialmuscles lacked the
fine
delicate
control necessaryfor
facial
expressionscan
be
attributed toabnormal
exaggeratedcontrac-tions
due
todysmetria.
To
obtain smooth gradedmovements of the facialmuscles needed for facial
expression, the subject practiced
delicate
move-ments of expression on the left$ide of the faceonly after reexperiencingthe
sensation of gradedmove-ment inthe whole body. Movements of fac.ial
ex-pressionon theright side of thefacewere practiced
in conjunction with the leftsided movements to
contribute to a more complete recovery. The right
frontalisand zygomaticus major showed no re-markable myoelectric changes, but manual-muscle
testsand photographic evidence indieatedsome
im-provement
in
thosemuscles.The
faintcontractions of the muscles on the right side of the face,com-b;ned with the exaggerated contractile activitie$ of
the corresponding muscles on
the
left,had !edtoan appearance of facialfeaturesbeing pulled leftward andthus
to
an inabilityfor
the
rightfacial
musclestoparticipateinfacial,expression.
Looking at the treatment as a whole,
442
ve\wtza#
posture, whichin
turnhelped
in
the treatmenteffect of aHeviating asymmetry
in
movements offacial
expression andlack
offinely
gradedmove-rnents.
The
fact
thatimprovements
were seen infacialexpression and in posture for thischronic case inwhich no more appreciable natural recovery could be expected corroborates the idea that treat-ment of facialpalsyina patientwho has suffered a cerebrovascular disorder should
best
be performedin
thecontext of treatmentfor
thewholebody.
Facial
expressions play animportant
role as a means of nonverbal cornmunications, so thatfunc-tion should
be
givenjust
as much attentionin
treatment as gaitand use efthe upper limb'jiT',
7.
Summary
When
facialpalsy accompanies central nerveusdysfunction, itneecls tobeevaluated and treatedin
the context of abnormal postural tone and abnor-mal postural motor patterns throughout the entire
body. We explored this
idea
by
following
theim-provement in a person whom we had not begun
treating until
6ne
year and one week after she hadsuffered a stroke. 1) Furusawa M, p$eudebulbar Ryeho,18(5)I 2) Furusawa M, facialmotor
(in
japanese).
3)Furusawa M, pseudobulbar Ryeho, 21(E)I ReferencesYamakawa'MIPrespeech therapy for
palsyafter stroke
Cin
Japanese).Ri-Sa-353-355,1984.
Sagasaki
J:Movement
therapy fororo-dysfunctiondue toParkinsonsyndronie
Ri-Sa-Ryoho,19CO :256-258,1985.
Yamakawa M 1Movement therapy for
palsy after stroke
(in
Japanese).
Ri-Sa-58-61, 1987.
eg
18
gas
4e
4)Furusawa M IMovernent therapy fororofacial motor dysfunction in cerebrovascular accidents (inJapanese).
Rigakuryoho,4<2)I139-145,1987.
5) Furusawa M,etat.:Movement therapy forfacialpalsy
after stroke
(in
Japanese}.Rigakuryohogaku(J.
nese PhysicalTherapy AssociationX150):39-44, 1988.6)
Furusawa M, et at.; Movement therapy for central
oral motor dysfunction:Resultsof treatments
{in
anese). Rigakuryohogaku
{J.
Japanese
Physica}py Association),16{2):77-83, 1989.
7)Tomita M [Orofacial approach
"n
Japanese).Journalof the Yamagata Chapterof
Japanese
Physicalpy Association,3[29-56, 1989.
8) DaviesPM :StepstoFollow.Tokyo,Springer-Verlag, 1985,pp 245-265.
9)Hirayama K :Shinkeishokogaku
(Neurological
ogy)
{in
Japanese}.
Tokyo,Bunkodo,1984,pp 992-997,IO)Niki R:Stroke
(in
Japanese).Igaku no Ayumi, i16
<s>:439-450,1981.
11)Daniels L,et aL : Muscle Testing, 2nd ed,,
phia. W.B.SaundersCompany, 1968,pp 162-・l74.
i2)Yeshida T, Andrew PD1A timerforsynchronizing analog signals and visual images. Bulletin of Allied
MedicalScience,Kobe,3:67-72, 1987,
13)Reder BD,et al:A Neuro-DevelopmentalAnalysisDf
Normal Movement Patterns:Neonate-TwelveMonths.
Ci]cinnatiOhio,Children'sHospital Medical Center,
1985,pp 29--32.
14)Sone M :MovemenE therapy forstroke patientwith
ataxia (in
Japanese).
Rigakuryoho,4{2):127-132,1987.
15)Manabe K:Case report:Improvement of functionby learning of principalmotility inataxia
(in
Japanese).Rigakuryoho,5(2)I125--130,1988.
16)Furusawa M :Prespeech therapy foran ataxic patient
with achewing and swallewing disorder
(in
Japanese).
Rigakuryohegaku
{J,
JapanesePhysicalTherapyeiation}, 15{2)[126-129, 1988,
17) Takahashi T: Movement therapy rnethod forthe
stroke hemiplegia, past, present and future (in
nese), Rigakuryoho,4(2)I89-93,l987.
18)Bobath Bi Adult Hemiplegia:Evaluationand
ment. 3rd ed, Oxford,Heinemann MedicalBooks,l990,
Physical