Title Remifentanil is a suitable concomitant agent for propofol during dental outpatient anaesthesia Author(s) 前納, 允
Journal , (): ‑
URL http://hdl.handle.net/10130/3424 Right
Remifentanil Remifentanil Remifentanil
Remifentanil is a suitable is a suitable is a suitable concomitant agent is a suitable concomitant agent concomitant agent concomitant agent for propofol during dental
for propofol during dental for propofol during dental
for propofol during dental outpatient outpatient outpatient outpatient anaesthesia
anaesthesia anaesthesia anaesthesia
Makoto Maeno
Department of Dental Anesthesiology, Tokyo Dental College
Summary Summary Summary Summary
The purpose of this study was to examine which might be suitable as a
concomitant agent for propofol general anaesthesia during dental outpatient
anaesthesia. Eighty patients with severe dental avoidance were divided into
one of four groups: propofol/saline solution (PS, n=20), propofol/0.25 µg.kg-
1.min-1 remifentanil (PRe-0.25, n=20), propofol/0.125 µg.kg-1.min-1 remifentanil
(PRe-0.125, n=20), and propofol/66% nitrous oxide (PN, n=20). By maintaining
the BIS value between 40 and 60, body movement and haemodynamic changes
during the treatment, recovery process following the treatment, process
following discharge, and anaesthetic cost were investigated. Body movements
were observed in all cases in the PS group. Postoperative nausea was observed
in five cases (25%) in the PRe-0.25 group. Although PRe-0.125 and PN groups
were considered clinically available, the PRe-0.125 group was less expensive. In
conclusion, remifentanil (0.125µg.kg-1.min-1) is a suitable concomitant agent for
propofol during dental outpatient anaesthesia.
Introduction Introduction Introduction Introduction
In outpatient anaesthesia, rapid emergence, absence of complications such as
nausea and vomiting and delirium, no pain after treatments, and satisfaction
by the patient as well as low anaesthetic cost, can be considered as conditions
for selecting anaesthetic methods [1]. According to studies on the recovery
process after general anaesthesia on the same patient [2], it has been reported
that the awakening time is longer after anaesthesia with propofol alone than
after anaesthesia with sevoflurane alone, while no difference is seen in the time
for total recovery, and that patient satisfaction is superior after propofol
anaesthesia. However, during treatment under propofol alone anaesthesia,
body movement and haemodynamic fluctuations may be of clinical issues.
There have been reports of the usefulness [3,4] and problems [3,5] of
concomitantly used agents that have an analgesic action, such as nitrous oxide,
fentanyl, remifentanil, or ketamine for controlling noxious stimuli and
haemodynamic fluctuations during propofol anaesthesia. [3-5] However, there
are no reports examining the usefulness and problems of concomitant use of
agents having analgesic action in outpatient propofol anaesthesia under mildly
invasive conditions such as dental treatment. To examine which might be
suitable as a concomitant agent for propofol general anaesthesia for outpatients
undergoing dental treatment among 0.25µg.kg-1.min-1 remifentanil, 0.125µg.kg-
1.min-1 remifentanil, or nitrous oxide, we investigated body movement,
haemodynamic changes, postoperative recovery process, degree of satisfaction,
and the anaesthetic cost in patients with severe dental avoidance.
Method Method Method Method
Subjects
This study was approved by the Ethics Review Board of Tokyo Dental College
Ethics Committee (Approval number 267). The subjects were 80 patients with
severe dental avoidance including those with dental phobia and/or gagging
problems. All subjects gave written informed consent to the study. All subjects
received general anaesthesia for the first time in this department. They were
randomly divided into one of four groups: propofol/saline solution (PS group,
n=20), propofol/0.25µg.kg-1.min-1 remifentanil (PRe-0.25 group, n=20),
propofol/0.125µg.kg-1.min-1 remifentanil (PRe-0.125 group, n=20), and
propofol/66% nitrous oxide (PN group, n=20). All subjects were classified as
ASA physical status 1 or 2. Exclusion criteria included alcohol or drug
dependent patients, patients with psychiatric diseases, and patients who
underwent invasive treatments such as impacted tooth extraction.
Anaesthesia method
After patients entered the outpatient treatment room without premedication,
they were equipped with an ECG, noninvasive blood pressure (BP), SpO2, and
bispectral index (BIS) monitor. Thereafter, an intravenous line was established
in the left cephalic vein. Acetated Ringer’s solution was infused at 2-4 ml.kg-1.h-
1. Anaesthesia was induced with propofol (1% Diprivan® injection kit,
AstraZeneca, UK) by using a TCI pump (Terufusion TCI syringe pump TE-371,
TERUMO Corporation, Japan) set to a target effect-site concentration at 3.5
µg.ml-1 with oxygen inhalation at 6 l.min-1. Nasotracheal intubation was
facilitated with 0.9 mg.kg-1 rocuronium bromide (Eslax® Intravenous solution,
Schering-Plough, USA). Oxygen and nitrous oxide were delivered at 1 l.min-1
and 2 l.min-1, respectively, in the PN group during maintenance of anaesthesia.
In the other three groups, oxygen and air were delivered at 1 l.min-1 and 3
l.min-1, respectively. Propofol concentration was adjusted to keep BIS value
between 40-60. The administration rate of remifentanil and the inhalation
concentration of nitrous oxide were fixed during the treatment. Patients were
artificially ventilated, and tidal volume and respiratory rate was adjusted to
maintain end-tidal carbon dioxide tension between 35-45 mmHg. When body
movements were observed during the treatment, a bolus injection of 0.2mg.kg-1
rocuronium bromide was administered. When the mean blood pressure dropped
to 60 mmHg or less, a bolus injection of 4 mgephedrine hydrochloride was
performed. Local anaesthesia was administered by using lidocaine
hydrochloride solution containing 12.5 µg.ml-1 adrenaline during dental
treatment such as caries treatment, pulp extirpation, and tooth extraction. An
intravenous injection of 50 mg flurbiprofen axetil was administered at the
completion of anaesthesia. Extubation was performed after confirming
conditions such as recovery of spontaneous breathing, reaction to the verbal
commands, and appearance of the deglutition reflex.
Observation periods and measurements
There were four observation periods: the maintenance period, emergence period,
recovery period, and period after returning home. The maintenance period was
set as the period from induction of anaesthesia to the cessation of
administration of the anaesthetic drugs. Body movements, number of
rocuronium bromide administrations, and total dosage of propofol were
recorded during this period. Changes in blood pressure and heart rate over
time were also observed. Systolic pressure, diastolic pressure, and heart rate at
the time of entry into the treatment room were set as the preanaesthesia
values. Observations were made at 45 and 90 min after intubation, at the
completion of anaesthesia, and immediately before extubation.
The emergence period was set as the period from the cessation of
anaesthetic drug administration to extubation. The times to recovery of
spontaneous breathing, BIS value reaching 75 [6],eye-opening, and extubation
were observed during this period.
The recovery period was set as the period from extubation to discharge.
The times to ambulation and discharge were observed. Aldrete Score [7] and
modified Post Anesthesia Discharge Scoring System (mPADSS) [8] were
recorded every five minutes, and ambulatory tests were carried out when each
of the scores was 9 or greater. In addition, discharge time was determined on
the basis of the Clinical Discharge Criteria [8].
For the period after returning home, inquiries were made by telephone
about the patient's general condition 24 h after anaesthesia on the basis of a
post-general anaesthesia checklist given to the patient at the time of discharge.
Occurrences and frequency of postoperative nausea and vomiting were
evaluated.
Anaesthetic cost was estimated by an addition of each anaesthetic value
based on the used amount. Then, anaesthetic cost per anaesthesia time and
body weight was calculated.
Statistical analysis
Repeated measures analysis of variance (ANOVA) and Dunnett's test were
used for intragroup comparisons at the various times of haemodynamic
fluctuations. M × n χ2 test was used for comparison of the frequency of occurrence of nausea and vomiting. ANOVA without repeated measures and
the Student-Newman-Keuls test was used for comparison of other
measurements among the groups. P < 0.05 was considered statistically
significant. Twenty patients per group was the target sample size in this study,
because 18 was found to be sufficient for detecting differences with the power at
0.8 in an earlier study [2].
Results Results Results Results
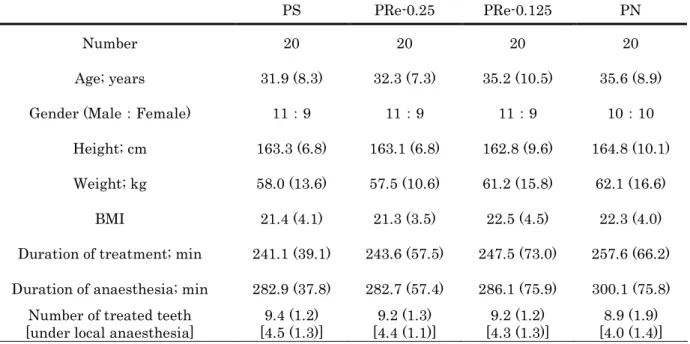
There were no significant differences in patient characteristics among the four
groups (Table 1).
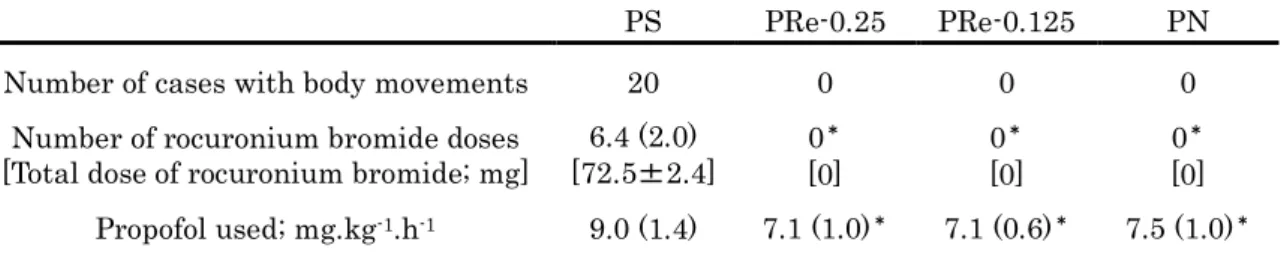
All patients in the PS group showed body movement during anaesthesia,
while no patients in the other three groups did it. Therefore, the doses of
rocuronium bromide and the amount of propofol were significantly higher in
the PS group than in the other three groups (Table 2).
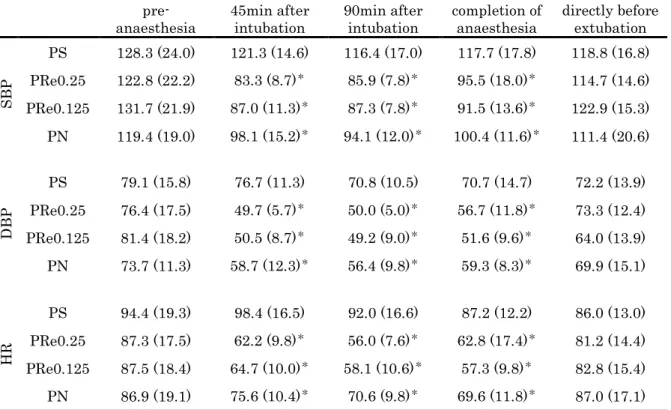
Systolic pressure, diastolic pressure, and heart rate were significantly
lower at 45 and 90 min after intubation and at the completion of anaesthesia
than those at preanaesthesia period in the PRe-0.25, PRe-0.125 and PN groups.
In contrast, no significant change was observed in the PS group at any time
point (Table 3). Ephedrine hydrochloride was not used in any of the cases.
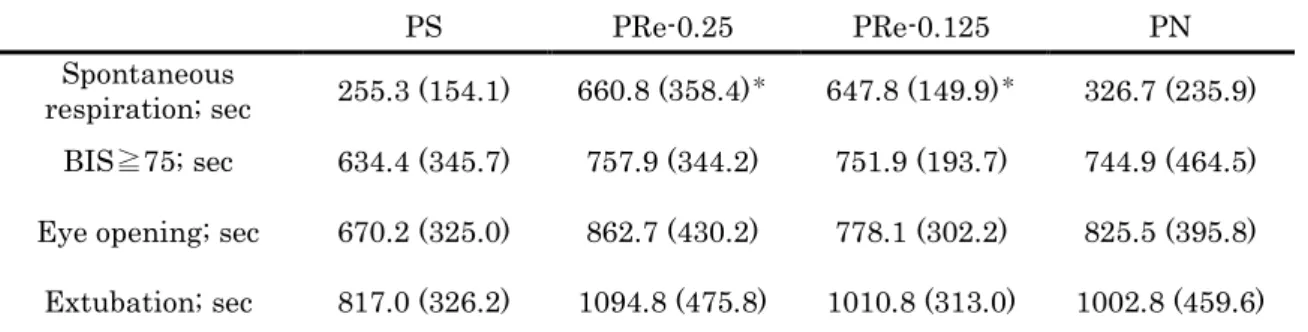
In the emergence period, the time to the recovery of spontaneous
breathing was significantly longer in the PRe-0.25 and PRe-0.125 groups than
in the PS and PN groups. No significant differences were observed among four
groups in the times to BIS value at 75, eye-opening, or extubation (Table 4).
In the recovery period, no significant differences were observed in the
time to ambulation and the discharge time among four groups (Table 5).
A significant difference in postoperative nausea was observed among
four groups within 24 h after anaesthesia, and there were five cases (25%) in
the PRe-0.25 group. There were no cases of other complications in any group
following discharge. (Table 5).
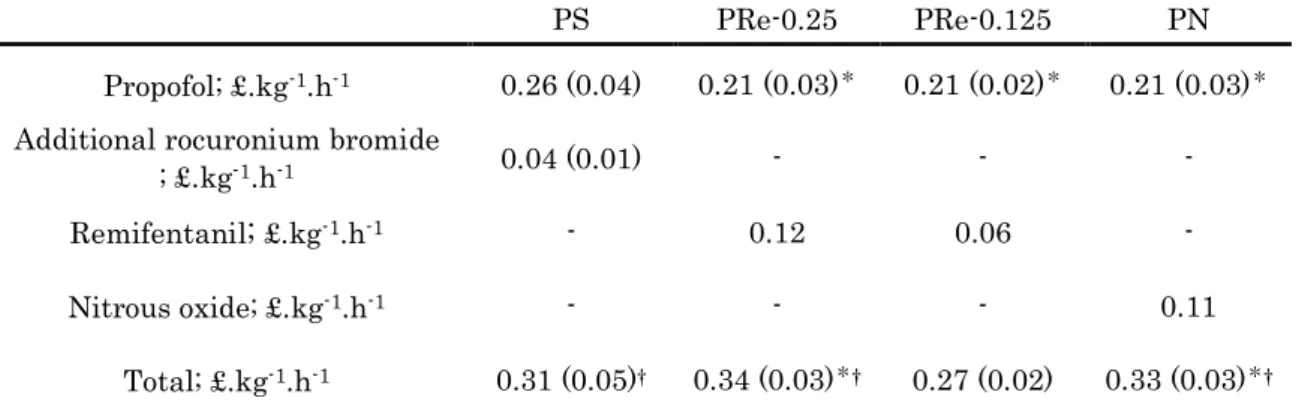
The anaesthetic cost was lowest in the PRe-0.125 group (Table 6).
Discussion Discussion Discussion Discussion
This study examined which was useful among 0.25 µg.kg-1.min-1 remifentanil,
0.125 µg.kg-1.min-1 remifentanil, and nitrous oxide, when used concomitantly
with propofol in general anaesthesia for outpatients undergoing dental
treatment. Anaesthesia with propofol and 0.125µg.kg-1.min-1 remifentanil
completely suppressed body movements without nausea after the treatment,
and was the least expensive.
Body movements were observed during the treatment in the PS group,
and rocuronium bromide was administered in all cases. In contrast, body
movements were completely suppressed by concomitantly using remifentanil or
nitrous oxide with propofol. Propofol increases inhibitory transmission via
GABA receptors and exhibits a hypnotic action without analgesia. Remifentanil
is a µ-receptor agonist and has an analgesic effect nearly comparable to that of
fentanyl [9]. In addition, nitrous oxide exhibits analgesic effects by inhibiting
the function of N-methyl-D-aspartic acid (NMDA) receptors [10] and by
activating α2B adrenoceptors [11]. Body movement was presumably inhibited
because of their analgesic effects which suppressed noxious stimuli not
inhibited by local anaesthesia, and because of increases in depth of anaesthesia
not reflected in BIS values [12-14]. Approximately 30% decreases in blood
pressure and heart rate was found in both PRe-0.25 and PRe-0.125 groups.
These results agree with past reports indicating that the haemodynamic
inhibition by remifentanil is dose-independent [15]. Remifentanil has been
reported to decrease heart rate and blood pressure through vagotonic and
sympatholytic effects [16]. In this study, ephedrine hydrochloride was not used,
and the severity of haemodynamic inhibition was not of clinical problems. In
addition, nitrous oxide produces haemodynamic activation by a
sympathomimetic effect [17]. However, in this study, haemodynamic inhibition
was also observed in the PN group as in PRe groups. In addition to
haemodynamic stability by the inhibition of noxious stimuli, the increase in
depth of anaesthesia not reflected in BIS values may have inhibited
haemodynamic fluctuations [12-14]. Ephedrine hydrochloride was also not used
in the PN group, and the severity of haemodynamic inhibition was not of any
clinical problems.
The time to the recovery of spontaneous breathing was faster in the PS
and PN groups. However, this delay was not critical since there were no
sustained effects on subsequent recovery in this study.
The cause of nausea and vomiting by opioids is attributed to stimulations
of central dopamine type 2 (D2) receptors, which in turn stimulates the
vomiting center in the medulla oblongata [18]. Among the opioids, nausea and
vomiting occur less often with remifentanil than with fentanyl [19]. In contrast,
propofol has been reported to reduce postoperative nausea and vomiting by an
antiemetic action mediated by antagonism of D2 receptor mechanisms [4]. In
this study, no nausea was observed in the PRe-0.125 group probably because of
the balance of the opposite pharmacological actions of remifentanil and propofol.
In contrast, nausea was observed in five cases (25%) in the PRe-0.25 group. The
effect of remifentanil on nausea may be dose-dependent. Nitrous oxide has an
emetic action [20]. The antiemetic action of propofol is reported to counteract
the emetic action of nitrous oxide [21,22]. No cases of vomiting and one case
(5%) of nausea in the PN group agrees with previous reports.
From the results of this study, we found that body movements were
sufficiently inhibited in the PRe-0.125 and PN groups, and that this did not
aggravate the emergence and recovery characteristics of propofol. In addition,
respiratory and haemodynamic depressions were minimal. However, when
anaesthetic cost is considered, PRe-0.125 group was less expensive. Therefore,
as a concomitant medication, 0.125 µg.kg-1.min-1 remifentanil was considered
the most useful. In addition, because nitrous oxide also might induce
environmental problems [23,24], 0.125 µg.kg-1.min-1 remifentanil may be
considered the most recommendable option.
In conclusion, anaesthesia with a combination of propofol and 0.125
µg.kg-1.min-1 remifentanil is suitable for general anaesthesia for outpatients
undergoing dental treatment.
Acknowledgements Acknowledgements Acknowledgements Acknowledgements
The author would like to thank Associate Prof. Ken-ichi Fukuda, Prof.
Yoshihiko Koukita, and Prof. Tatsuya Ichinohe for their assistance in this
study.
Competing interests Competing interests Competing interests Competing interests
No Competing interests declared.
References
1. Raeder J, Gupta A, Pedersen F. Recovery characteristics of sevoflurane- or propofol- based anaesthesia for day-care surgery. Acta Anaesthesiologica Scandinavica 1997; 41414141: 988-94.
2. Ohkushi K, Fukuda K, Ichinohe T, Kaneko Y. Comparison between sevoflurane-anesthesia and propofol-anesthesia for day-care dental
treatment. 87th General Session & Exhibition of the IADR, Program book, p173, San Diego, USA, 2011.
3. K. de Vasconcellos , J. R. Sneyd. Nitrous oxide: are still in equipoise? A qualitative review of current controversies. British Journal of Anaesthesia 2013; 111111111: 877-85. 111
4. Cillo JE Jr. Analysis of propofol and low-dose ketamine admixtures for adult outpatient dentoalveolar surgery: A prospective, randomized,
positive-controlled clinical trial. Journal of Oral and Maxillofacial Surgery 2012; 707070: 537-46. 70
5. Gen TJ, Meyer T, Apfel CC, Chung F, Davis PJ, Eubanks S, Kovac A, Philip BK, Sessler DI, Temo J, Tramèr MR, Watcha M: Consensus guidelines for managing postoperative nausea and vomiting. Anesthesia and Analgesia 2003; 97979797: 62-71.
6. Song D, Vlymen J, White PF: Is the bispectral index useful in predicting fast-track eligibility after ambulatory anesthesia with propofol and desflurane? Anesthesia and Analgesia 1998; 87878787: 1245-8.
7. Aldrete JA: The post-anesthesia recovery score revisited. Journal of Clinical Anesthesia 1995; 7777: 89-91.
8. Chung F, Chan VW, Ong D: A post-anesthetic discharge scoring system for home readiness after ambulatory surgery. Journal of Clinical Anesthesia 1995; 777: 500-6. 7
9. Guy J, Hindman BJ, Baker KZ, Borel CO, Maktabi MON, Kirchner J, Todd
Young WL, Warner DS: Comparison of remifentanil and fentanyl in
patients undergoing craniotomy for supratentorial space occupying lesions.
Anesthesology 1997; 86868686: 514-24.
10. Jevtovic-Todorovic V, Todorovic SM, Mennerick S, Powell S, Dikranian K, Benshoff N, Zorumski CF, Olney JW: Nitrous oxide (laughing gas) is an NMDA antagonist, neuroprotectant and neurotoxin. Nature Medicine 1998;
4 4 4
4: 460-3.
11. Sawamura S, Kingery WS, Davies MF, Agashe GS, Clavid JD, Kobilka BK, Hashimoto T, Maze M: Antinociceptive action of nitrous oxide is mediated by stimulation of noradrenergic neurons in the brainstem and activation of α2B adrenoceptors. Journal of Neuroscience 2000; 20202020: 9242-51.
12. Rampil IJ, Kim JS, Lenhardt R, Negishi C: Bispectral EEG index during nitrous oxide administration. Anesthesiology 1998; 89898989: 671-7.
13. Barr G, Jakobsson JG, Owall A, Anderson RE: Nitrous oxide dose not alter bispectral index: study with nitrous oxide as sole agent and as an adjunct to i.v. anaesthesia. British Journal of Anaesthesia 1999; 82828282: 827-30.
14. Yufune S, Takamatsu I, Masui K, Kazam T: Effect of remifentanil on plasma propofol concentration and bispectral index during propofol anaesthesia. British Journal of Anaesthesia 2011; 106106106106: 208-14.
15. Glass PSA, Gan TJ, Howell S: A review of the pharmacokinetics and
pharmacodynamics of remifentanil. Anesthesia and Analgesia 1999; 89898989: S7- 14.
16. Beers R, Camporeei E: Remifentanil update: clinical science and utility.
CNS Drugs 2004; 18181818: 1085-104.
17. Fukunaga A, Epstein RM: Sympathetic excitation during nitrous oxide- halothane anesthesia in the cat. : Anesthesiology 1973; 39393939: 23-36.
18. Wood GJ, Shega JW, Lynch B, Von Roenn JH: Management of intractable nausea and vomiting in patients at the end of life: “I was feeling nauseous
all of the time ... nothing was working”. Journal of the American Medical Association 2007; 298298298298: 1196-207.
19. Maceiras PR, Ferreira TA, Molins N, Sanduende Y, Bautista AP, Rey T:
Less postoperative nausea and vomiting after propofol + remifentanil versus propofol + fentanyl anaesthesia during plastic surgery.: Acta Anaesthesiologica Scandinavica 2005; 494949: 305-11. 49
20. Leslie K, Myles PS, Chan MTV, Paech MJ, Peyton P, Forbes A, Mckenzie D, EGIGMA Trial Group: Risk factors for severe postoperative nausea and vomiting in a randomized trial of nitrous oxide-based vs nitrous oxide-free anaesthesia. British Journal of Anaesthesia 2008; 101101101101: 498-505.
21. Ichinohe T, Kaneko Y: Nitrous oxide dose not aggravate postoperative emesis after orthognathic surgery in female and nonsmoking patients.
Journal of Oral and Maxillofacial Surgery 2007; 65656565: 936-9.
22. Fernández-Guisasola J, Gómez-Arnau JI, Cabrera Y, Valle SG: Association between nitrous oxide and the incidence of postoperative nausea and
vomiting in adults: a systematic review and meta-analysis. Anaesthesia 2010; 656565: 379-87. 65
23. Logan M, Farmer JG: Anaesthesia and the ozone layer [editorial]. British Journal of Anaesthesia 1989; 63636363: 645-7.
24. Wang WC, Yung YL, Lacis AA, Mo T, Hansen JM: Greenhouse effects due to man-made perturbations of trace gases. Science 1976; 194194194: 685-9. 194
Table 1 Patient characteristics.
No significant differences in patient background among the four groups. Values are the mean (SD).
PS PRe-0.25 PRe-0.125 PN
Number 20 20 20 20
Age; years 31.9 (8.3) 32.3 (7.3) 35.2 (10.5) 35.6 (8.9)
Gender (Male:Female) 11:9 11:9 11:9 10:10
Height; cm 163.3 (6.8) 163.1 (6.8) 162.8 (9.6) 164.8 (10.1) Weight; kg 58.0 (13.6) 57.5 (10.6) 61.2 (15.8) 62.1 (16.6)
BMI 21.4 (4.1) 21.3 (3.5) 22.5 (4.5) 22.3 (4.0)
Duration of treatment; min 241.1 (39.1) 243.6 (57.5) 247.5 (73.0) 257.6 (66.2) Duration of anaesthesia; min 282.9 (37.8) 282.7 (57.4) 286.1 (75.9) 300.1 (75.8)
Number of treated teeth [under local anaesthesia]
9.4 (1.2) [4.5 (1.3)]
9.2 (1.3) [4.4 (1.1)]
9.2 (1.2) [4.3 (1.3)]
8.9 (1.9) [4.0 (1.4)]
PS: propofol/saline solution
PRe-0.25: propofol/0.25 µg.kg-1.min-1 remifentanil PRe-0.125: propofol/0.125 µg.kg-1.min-1 remifentanil PN: propofol/66% nitrous oxide
Table 2 Body movements during anaesthesia.
Body movements were seen in the PS group during the procedure. Values are the mean (SD).
PS PRe-0.25 PRe-0.125 PN
Number of cases with body movements 20 0 0 0
Number of rocuronium bromide doses [Total dose of rocuronium bromide; mg]
6.4 (2.0) [72.5±2.4]
0* [0]
0* [0]
0* [0]
Propofol used; mg.kg-1.h-1 9.0 (1.4) 7.1 (1.0)* 7.1 (0.6)* 7.5 (1.0)*
*p < 0.05 versus group PS PS: propofol/saline solution
PRe-0.25: propofol/0.25 µg.kg-1.min-1 remifentanil PRe-0.125: propofol/0.125 µg.kg-1.min-1 remifentanil PN: propofol/66% nitrous oxide
Table 3 Haemodynamic parameters during anaesthesia.
Haemodynamic parameters during the procedure were significantly lower than the control.
Values are the mean (SD).
pre- anaesthesia
45min after intubation
90min after intubation
completion of anaesthesia
directly before extubation
SBP
PS 128.3 (24.0) 121.3 (14.6) 116.4 (17.0) 117.7 (17.8) 118.8 (16.8) PRe0.25 122.8 (22.2) 83.3 (8.7)* 85.9 (7.8)* 95.5 (18.0)* 114.7 (14.6) PRe0.125 131.7 (21.9) 87.0 (11.3)* 87.3 (7.8)* 91.5 (13.6)* 122.9 (15.3) PN 119.4 (19.0) 98.1 (15.2)* 94.1 (12.0)* 100.4 (11.6)* 111.4 (20.6)
DBP
PS 79.1 (15.8) 76.7 (11.3) 70.8 (10.5) 70.7 (14.7) 72.2 (13.9) PRe0.25 76.4 (17.5) 49.7 (5.7)* 50.0 (5.0)* 56.7 (11.8)* 73.3 (12.4) PRe0.125 81.4 (18.2) 50.5 (8.7)* 49.2 (9.0)* 51.6 (9.6)* 64.0 (13.9) PN 73.7 (11.3) 58.7 (12.3)* 56.4 (9.8)* 59.3 (8.3)* 69.9 (15.1)
HR
PS 94.4 (19.3) 98.4 (16.5) 92.0 (16.6) 87.2 (12.2) 86.0 (13.0) PRe0.25 87.3 (17.5) 62.2 (9.8)* 56.0 (7.6)* 62.8 (17.4)* 81.2 (14.4) PRe0.125 87.5 (18.4) 64.7 (10.0)* 58.1 (10.6)* 57.3 (9.8)* 82.8 (15.4) PN 86.9 (19.1) 75.6 (10.4)* 70.6 (9.8)* 69.6 (11.8)* 87.0 (17.1)
*p < 0.05 versus control PS: propofol/saline solution
PRe-0.25: propofol/0.25 µg.kg-1.min-1 remifentanil PRe-0.125: propofol/0.125 µg.kg-1.min-1 remifentanil PN: propofol/66% nitrous oxide
SBB: Systolic blood pressure DBP: Diastolic blood pressure HR: Heart rate
Table 4 Emergence profiles.
The time to the appearance of spontaneous breathing was significantly longer in the PRe-0.25 group and PRe-0.125 group than in the PS group and PN group. Values are the mean (SD).
PS PRe-0.25 PRe-0.125 PN
Spontaneous
respiration; sec 255.3 (154.1) 660.8 (358.4)* 647.8 (149.9)* 326.7 (235.9) BIS≧75; sec 634.4 (345.7) 757.9 (344.2) 751.9 (193.7) 744.9 (464.5) Eye opening; sec 670.2 (325.0) 862.7 (430.2) 778.1 (302.2) 825.5 (395.8) Extubation; sec 817.0 (326.2) 1094.8 (475.8) 1010.8 (313.0) 1002.8 (459.6)
*p < 0.05 versus group PS and PN PS: propofol/saline solution
PRe-0.25: propofol/0.25 µg.kg-1.min-1 remifentanil PRe-0.125: propofol/0.125 µg.kg-1.min-1 remifentanil PN: propofol/66% nitrous oxide
Table 5 Recovery profiles.
No significant difference was found among the four groups in the time to ambulation, the discharge time, or patient satisfaction. Postoperative nausea was observed in five cases (25%) in the PRe-0.25 group. Values are the mean (SD).
PS PRe-0.25 PRe-0.125 PN p value
Time to ambulation; min 43.7 (12.5) 51.4 (24.3) 44.3 (16.6) 49.6 (48.7) n.s.
Discharge time; min 193.9 (44.7) 198.2 (47.3) 161.5 (40.6) 169.2 (70.1) n.s.
Incidence of nausea; number 0 5 0 1 p < 0.05
PS: propofol/saline solution
PRe-0.25: propofol/0.25 µg.kg-1.min-1 remifentanil PRe-0.125: propofol/0.125 µg.kg-1.min-1 remifentanil PN: propofol/66% nitrous oxide
Table 6 Anaesthetic cost.
The anaesthetic cost was lowest for the PRe-0.125 group. Values are the mean (SD).
1 £ = 150 Japanese Yen
PS PRe-0.25 PRe-0.125 PN
Propofol; £.kg-1.h-1 0.26 (0.04) 0.21 (0.03)* 0.21 (0.02)* 0.21 (0.03)* Additional rocuronium bromide
; £.kg-1.h-1 0.04 (0.01) - - -
Remifentanil; £.kg-1.h-1 - 0.12 0.06 -
Nitrous oxide; £.kg-1.h-1 - - - 0.11
Total; £.kg-1.h-1 0.31 (0.05)† 0.34 (0.03)*† 0.27 (0.02) 0.33 (0.03)*†
*p < 0.05 versus group PS,† p < 0.05 versus group PRe-0.125 PS: propofol/saline solution
PRe-0.25: propofol/0.25 µg.kg-1.min-1 remifentanil PRe-0.125: propofol/0.125 µg.kg-1.min-1 remifentanil PN: propofol/66% nitrous oxide