Quality of life of chronic myelogenous leukemia patients following BCR-ABL inhibitor therapy:
A multicenter study in Nara Japan using SF-8
Hitoshi Hanamoto1, Ko Fujimoto1, Aki Fujii1, Mariko Fujita1, Futoshi Iioka2, Haruyuki Tanaka3, Hideo Yagi4, Takashi Akasaka2, Itsuto Amano3,
Hitoshi Ohno2, Kazuo Tsubaki5
1 Department of Hematology, Kindai University Nara Hospital
2 Department of Hematology, Tenri Hospital
3 Nara Medical University 2nd Dept. of Internal Medicine
4 Department of Hematology and Oncology, Nara Prefecture General Medical Center
5 Japanese Red Cross Chugoku-Shikoku Block Blood Center
Abstract
Chronic myelogenous leukemia (CML) is caused by chromosomal translocation t (9;22) (q34;q11.2) forming a BCR-ABL fusion gene. Treatment of CML patients with tyrosine kinase inhibitor (TKI) led to a marked improvement in the survival rate.
However, when treating CML patients, adverse events of TKI may reduce the QOL. When we were able to use only Imatinib, we continued to use despite adverse events. However, we can now use Dasatinib, Nilotinib, Bosutinib, and Ponatinib.
Therefore, to examine the effects of TKI on the QOL of CML patients, we conducted a QOL sur- vey at three major facilities in Nara Prefecture.
For the QOL survey, we used SF-8. The results of the survey showed that there was no difference be-
tween the pretreatment QOL score and QOL score at the time of the survey. However, the QOL scores showed improved physical functioning, bodily pain, vitality, role-emotional, and mental health summary scores in the TKI switch group. The main reason for switching TKI was adverse events.
Therefore, these adverse events reduce the QOL of CML patients. Switching TKI improved the QOL.
Presently, five TKI are available, expanding the range of options. When adverse events appear, switching TKI and adverse event management are also important to maintain a patient’s QOL and continue the therapy.
Key words : QOL, TKI, CML
Introduction
Chronic myelogenous leukemia (CML) is caused by chromosomal translocation t (9;22) (q34; q11.2) in cells at the level of pluripo
tent hematopoietic stem cells, which leads to a BCR-ABL fusion gene generating P210 as constitu- tively active tyrosine kinase, causing increased cell survival and proliferation. CML comprises about 15 to 20% of all leukemia and is relatively rare, with an incidence rate of 1/100,000 a year.1-3 Treat-
ment of CML patients markedly improves with TKI. A BCR-ABL inhibitor, Imatinib, was admin- istered at the initial dose of 400 mg/once/day (QD) in the phase III randomized comparative trial IRIS (International Randomized study of Interferon) and STI571 trial with untreated CML-CP patients as the subjects, conducted in Western nations.4 Com- pared with the previous standard treatment, IFN-α + low dose-Ara-C, Imatinib led to clearly superior cytogenetic responses and progression-free surviv- al (PFS), and became the new standard treatment
Received April 17, 2019; Accepted September 18, 2019
for CML-CP.5 On the other hand, about 6% of en- rolled patients discontinued the trial due to adverse events (AEs), and the five-year summary shows a high incidence of adverse events.6 Subsequent- ly, second-generation therapeutic agents (Nilotinib and Dasatinib) were approved for patients resistant or intolerant to Imatinib, and their superior thera- peutic effects and low rare of cross-tolerance with Imatinib have been reported. Questionnaire results (321/384 responses) have been reported by the chronic myelogenous leukemia patient association (Group IZUMI). Symptoms that are particularly disturbing in life were muscle cramp, 57.6%, ede- ma, 41.8%, and fatigue, 39.9%. Only 6.4% of CML patients were asymptomaric.7 In contrast, the switch from Imatinib to the second-generation therapeutic agents led to same patients showing improvements in AEs of Imatinib. At the 2012 American Society for Clinical Oncology (ASCO), after switching to nilotinib for low-grade non-hematologic toxicity (grades 1 and 2) of imatinib were reported. Accord- ing to a report, 66.9% of patients (103/154 cases) achieved improvement in adverse events at 3 cy- cles (28 days/cycle) after switching, and the qual- ity of life improved in 61.8% of patients (103/154 cases).8
As second-generation therapeutic agents are be- coming available today, treatment options for CML patients have increased, contributing to a reduction in AEs, and greatly changing the environment sur- rounding CML treatment. The time has changed from administering Imatinib while allowing for AEs, to the selection of a therapeutic agent that suits the condition of each patient. As long-term survival of CML patients has become plausible, fu- ture treatment should consider the QOL of patients.
Since second-generation therapeutic agents have become available, the usefulness of TKI switch has been reported.9 In this report, switching to treat- ment with dasatinib showed that patients treated with imatinib with grade 1/2 AEs resolved and improved AEs and improved QOL. From this, we thought that a treatment strategy that considered QOL for CML patients was necessary. However, in poor transportation areas, it is difficult to vis- it hospitals frequently due to switching TKI, and CML patients allowed to reduce the QOL. CML patients in poor transportation areas may be able to improve the QOL through switching TKI. There- fore, we conducted a retrospective survey on the QOL of CML patients in Nara where transportation is a poor area.
Methods Subjects
CML-CP patients, for whom Philadelphia (Ph) chromosome had been confirmed in a chromo- some analysis, or were positive for the BCR-ABL gene, who also satisfied the patient selection cri- teria while not meeting the exclusion criteria.
Inclusion criteria
① Patients, who have been treated for at least a month with Imatinib, Nilotinib, or Dasatinib, and
② have provided written informed consent (patient, or a legal representative if the patient is a minor).
Exclusion criteria
① Patients with mental disorders or psycholog- ical symptoms, which makes their participation in the study difficult, ② patients with cognitive disor- ders, or ③ patient whose participation to the study was deemed difficulty for other reasons by the at- tending physician.
Survey facilities
1. Nara Medical University 2nd Dept. of Internal Medicine
2. Department of Hematology, Tenri Hospital 3. Department of Hematology Kindai University Nara Hospital
Survey duration
From February 2013 to March 2014 Endpoints
The primary endpoint:
Evaluation of the QOL at the end of the current treatment
The secondary endpoints:
Changes in the QOL before and after the start of CML treatment
Changes in the QOL before and after a change in medication
Profile of all adverse events Assessment of quality of life:
Scales to measure the health-related QOL are clas- sified into comprehensive scales and disease-spe- cific scales. In the present study, we used the SF-8 (8-Item Short-Form Health Survey) questionnaire method to summarize and analyze self-administered questionnaire results.
SF-8 is a comprehensive scale, and its reliabili- ty and validity have been scientifically verified.10
Furthermore, since SF-8 is based on the concept of the health-related the QOL, it is possible to mea- sure the health-related the QOL of patients with various diseases, allowing for comparisons be- tween the QOL of patients with different diseases or with the healthy public. With SF-8, responses to each question are scored based on the nation- al standard, allowing for measurements of eight health-related concepts. Therefore, even without a control group, scores can be interpreted. Based on the scores of eight health-related concepts,
“physical component summary scores” and “men- tal component summary scores” can be calculat- ed. The eight health-related concepts are physical functioning , role-physical, bodily pain, general health, vitality, social functioning, role-emotional, and mental health, and by analyzing the first four and the latter four concepts, the physical health summary score and mental health summary score can be calculated respectively. Norm-based scoring is 49.84, 50.07, 50.06, 49.96, 50.09, 50.00, 49.94, and 49.70, respectively. Norm-based scoring for physical and mental component summary scores are 48.6 and 49.44, respectively.
Statistical methods
Statistical analyses were performed using EZR software11. EZR is available on Jichi Medical Uni- versity Saitama Medical Center website (http://
www.jichi.ac.jp/saitama-sct/SaitamaHP.files/
statmed.html).
Results
We analyzed 98 CML patients registered at the three facilities in Nara Prefecture. (Table 1) The median treatment duration with TKI was 48.5 months (range: 1-168 months). TKIs being used at the time of the survey were Imatinib (45), Nilo- tinib (28), and Dasatinib (25). Their median doses were 400, 600, and 100 mg/day, respectively. Re- garding TKI switching, 60 patients had no switch, 33 patients had one switch, and five patients had two switches. The reason for a switch was mainly AEs, but for cases involving two TKI switches, the reason was an insufficient effect. The first- choice TKI was Imatinib for 69 patients, Nilotinib for 18 patients, and Dasatinib for 11 patients, and the rates of continued use were 60.8, 61.1, and 63.6%, respectively.
SF-8 results
The results for the pretreatment and survey
groups involving all cases, respectively, were as follows: physical functioning: 47.9/47.8, role-physical: 55.9/54.3, bodily pain: 47.4/49.3, general health: 48.6/49.8, vitality: 48.9/49.3, social functioning: 50.9/49.9, role-emotional:
48.2/48.3, mental health: 48.5/48.9, physical component summary score: 47.7/47.5, and men- tal component summary score: 47.9/49.3. A sig- nificant difference was only confirmed in bodi- ly pain (P = 0.008), and although there was no
Table 1 Patient’s characteristics
CML patients (N=98) Sex (n)
Female 35
Male 63
Age
Mean 62
Range 18-90
Duration of previous TKI treatment (mo)
Mean 48.5
Range 1-168
Curent treatment
Imatinib 45
Nilotinib 28
Dasatinib 25
Imatinib dose (mg)
Mean 40
Range 20-800
Nilotinib dose (mg)
Mean 600
Range 300-900
Dasatinib dose (mg)
Mean 100
Range 20-180
Disease response (n)
MMR 81
CCyR 11
Non CCyR 6
Number of treatment changes
None 60
Once 33
Twice 5
Abbreviations:
MMR: Major Molecular Response, CCyR: Complete Cytogenetic Response,
significant difference, general (P = 0.056) and mental component summary (P = 0.059) scores showed improvement during the survey. (Figure 1) In the group that did not switch TKI, pretreat- ment and survey results were as follows: physical functioning: 47.2/47.1, role-emotional: 55.6/53.8, bodily pain: 46.7/48.5, general health: 48.4/49.6, vitality: 48.9/49.3, social functioning: 50.5/50.1, role-emotional: 47.6/47.8, mental health: 48.3/47.8, physical component summary score: 47.1/47.8, and mental component summary score: 47.2/49.9.
There was no significant difference between QOL scores at pretreatment and based on the survey.
There was no difference in QOL scores among Imatinib, Nilotinib, and Dasatinib.
Pretreatment and survey results for cases that switched TKI once were as follows: physical functioning: 41.5/48.6, role-emotional: 51.8/55.0, bodily pain: 45.1/50.4, general health: 46.8/50.1, vitality: 44.0/49.0, social functioning: 46.5/49.6, role-emotional: 43.6/49.1, mental health: 44.7/48.2,
physical component summary score: 41.9/46.8, and mental component summary score: 41.6/48.1.
There were significant differences in physical functioning (P = 0.01), bodily pain (P = 0.01), vitality (P = 0.04), role-emotional (P = 0.02), or the mental component summary score (P = 0.03).
(Figure 2) The questionnaire results for AEs — swelling of face/hands and feet/around eyes, mus- cle cramp, muscle pain, fatigue, insomnia, diar- rhea, constipation, nausea, headache, rash, and itching—are summarized in Figure 3. Imatinib led to a higher frequency of AEs compared with other medications. In terms of the occurrence of AEs (with/without AEs), the respective results were as follows: physical functioning: 48.0/44.6, role-emotional: 55.7/51.3, bodily pain: 49.9/47.0, general health: 50.6/47.6, vitality: 49.6/48.7, social functioning: 51.0/48.4, role-emotional:
49.2/44.9, mental health: 49.7/48.5, physical component summary score: 48.7/44.7, and mental component summary score: 50.5/47.4. There was
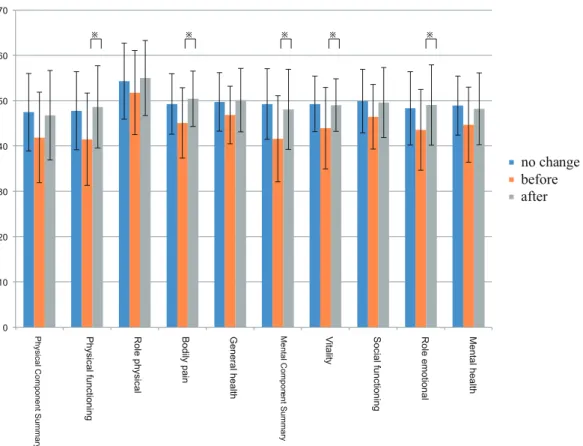
Figure 1. QOL score at pretreatment and survey
Figure 1 shows QOL comparison between standard, pretreatment, and investigation.
Standard shows the scoring based on national standard values.
※shows a significant difference of P<0.05.
0 10 20 30 40 50 60 70
回変更
no change before after
Physical
functioning
Role
physical
Bodily
pain
General
health
Vitality Social
functioning
Role
emotional
Mental
health
Physical
Component
Summary
Mental
Co
mponent
Summary
※ ※ ※ ※ ※
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Edema of face Fatigue Insomnia DiarrheaMuscle painMuscle crampsEdema around eyesEdema of limbs Constipation Nausea Headache ItchRash
dasatinib nilotinib imatinib Figure 2. QOL score at before and after change
Figure 2 shows QOL comparison between the no change drug group and change drug group (before, after). ※ shows a significant difference(P<0.05).
Figure 3. Frequency of side effects
Figure 3 shows the frequency of side effects of three drugs for 13 symptoms. Bars indicate drugs, gray is Dasatinib, orange is Nilotinib, and blue is Imatinib.
a significant difference only in role-emotional (P = 0.02), but generally, when there were AEs, the QOL tended to decrease. In terms of MMR, which is a therapeutic effect, results for cases with/without MMR achievement were as follows:
physical functioning: 47.5/47.7, role-emotional:
54.1/56.1, bodily pain: 49.2/50.1, general health:
49.6/52.3, vitality: 49.2/49.3, social function- ing: 49.8/51.7, role-emotional: 48.1/48.5, mental health: 48.9/50.3, physical component summary score: 47.3/47.7, and mental component summary score: 49.2/49.8. There was no significant differ- ence.
Discussion
Base on the present survey, AEs worsened the QOL of CML patients, and switching TKI improved the QOL. (Figure 2) For CML patients, long-term survival has become possible; thus, maintenance of the QOL is important. Therefore, when there are AEs, switching TKI must be considered. At the time of the survey, Imatinib, Dasatinib, and Nilo- tinib were available. However, uses of Dasatinib and Nilotinib were delayed compared with that of Imatinib. So, 45% of patients were treated with Imatinib. Currently, many patients begin treat- ments with Dasatinib or Nilotinib, and Bosutinib and Ponatinib are also available. In other words, management of AEs may change. In the present survey, with I imatinib used more frequently, 38%
of patients switched TKI. When Imatinib was the first choice, there was more burden on patients.12 Since options for TKI have broadened, the key to continue treatment while maintaining the QOL is to switch TKI when there are AEs. This is multicenter study on the first on the QOL conducted in Nara Prefecture. The study revealed that a survey of the QOL is important in managing CML patients.13 As a QOL survey, SF-8 was simple and useful. In the future, it would be a good reference for changes in medication if patients could complete the SF-8 QOL survey, for example, in a waiting room.14
However, although this study was analyzed ret- rospectively, we found that some CML patients had reduced QOL with AE. Knowing the results of the QOL survey in this study will help change the physician’s awareness of AEs in clinical practice.
However, this study was conducted only in Nara and needs to be investigated even in other poor transportation areas. We will think that it is neces- sary to investigate other poor transportation areas in the future.
Conclusions
In this survey, it was found that QOL was reduced by AE, and it was shown that QOL improved even for CML patients in Nara where transportation is a poor area by switching TKI. By investigating QOL, I think that switching TKIs early in patients with reduced AEs will improve QOL and lead to contin- ued treatment.
Conflict of interest
The authors have no conflict of interest to de- clare.
References
1. Cortes JE, Talpaz M, Kantarjian H. (1996) Chronic my- elogenous leukemia: a review. Am J Med 100:555-570 2. Jemal A, et al. (2004) Cancer statistics, 2004. CA Can-
cer J Clin 54:8-29
3. Redaelli A, et al. (2004) Clinical and epidemiologic burden of chronic myelogenous leukemia. Expert Rev Anticancer Ther 4:85-96
4. Roy L, et al. (2006) Survival advantage from imatinib compared with the combination interferon-alpha plus cy- tarabine in chronic phase chronic myelogenous leukemia:
historical comparison between two phase 3 trials. Blood 108(5):1478-1484
5. O’Brien SG, et al. (2003) Imatinib compared with in- terferon and low-dose cytarabine for newly diagnosed chronic-phase chronic myeloid leukemia. N Engl J Med 348:994-1004
6. Tauchi T, et al. (2011) Seven-year follow-up of patients receiving imatinib for the treatment of newly diagnosed chronic myelogenous leukemia by the TARGET system.
Leuk Res 35:585-590
7. Tamura H, et al. (2011) CML kanjyanoishiki-seikatunikans- uruanke-toKaramiruKanjya noomoi. JSH Abstract
8. Cortes JE, et al. (2016) Evaluating the Impact of a Switch to Nilotinib on Imatinib-Related Chronic Low- Grade Adverse Events in Patients With CML-CP: The ENRICH Study. Clin Lymphoma Myeloma Leuk 16:286- 296
9. Kim DW, et al. (2018) Outcomes of switching to da- satinib after imatinib-related low-grade adverse events in patients with chronic myeloid leukemia in chronic phase:
the DASPERESE study. Ann hematol 97(8): 1357-1367 10. Ellert U, Lampert T, Ravens-Sieberer U. (2005) [Mea-
suring health-related quality of life with the SF-8. Normal sample of the German population]. Bundesgesundheits- blatt Gesundheitsforschung Gesundheitsschutz 48:1330- 11. Kanda Y. (2013) Investigation of the freely available 1337
easy-to-use software ‘EZR’ for medical statisticsc. Bone Marrow Transplant 48:452-458
12. Unnikrishnan R, Veeraiah S, Ganesan P. (2017) Symp- tom Burden and Quality of Life Issues among Patients of
Chronic Myeloid Leukemia on Long-term Imatinib Ther- apy. Indian J Med Paediatr Oncol 38:165-168
13. De Marchi F, et al. (2017) How could patient reported outcomes improve patient management in chronic my- eloid leukemia? Expert Rev Hematol 10:9-14
14. Zulbaran-Rojas A, et al. (2018) A prospective analysis of symptom burden for patients with chronic myeloid leu- kemia in chronic phase treated with frontline second- and third-generation tyrosine kinase inhibitors. Cancer Med 7:5457-5469