著者(英) 綾 渡邉, ロレイン サッカ journal or
publication title
福井大学医学部研究雑誌
volume 17
page range 1‑11
year 2017‑01
URL http://hdl.handle.net/10098/9997
Listening to Foreign Patient Voices: A Narrative Approach
WATANABE, Aya, SAKKA, Lorraine
※1Language Center, University of Fukui
ナラティブからみる外国人患者の医療体験
渡邉 綾,サッカ ロレイン※1 語学センター
Abstract:
Background: With over 2 million foreign residents in Japan and the increased number of visitors from abroad, Japan must provide healthcare for the non-Japanese speaking population. The government has also implemented a plan to establish 30 medical institution hubs in and around the larger metropolis cities to have language services for visitors who are expected to come for the 2020 Tokyo Olympics. Though a small growing body of research has investigated communication difficulties between foreign patients and the healthcare institutions, there is much to be addressed. Our current study approaches this issue through a narrative-based approach. Method: Two researchers individually interviewed a total of 13 foreign residents who agreed to participate in interviews that were audio-recorded. Three main questions were asked: previous medical experiences in their own home country, reason for living in Japan (primarily Fukui) and their experiences and insights from their encounters with the healthcare system. These recorded sessions were transcribed and analyzed into categories of concerns expressed through the interviews.
Results: Experiences were categorized into five main areas: 1) Privacy and confidentiality, 2) Cultural differences, 3) Mismatch in expectations, 4) Differences in medical systems, and 5) Language-related issues both spoken and written.
Conclusion: This study found that while language problems exist, there are other concerns that make accessing healthcare in Japan a challenge for non-Japanese speaking residents. Previous experiences as well as cultural expectations of what should occur within a healthcare setting are discussed.
Key Words: Narrative approach, interview studies, foreign patients, healthcare settings
要旨:
本研究の目的は,インタビュー調査から 13 名の外国人患者のナラティブ(語り)を通して当事者に関する問 題を考察することである。近年,外国人患者が日本の医療機関を利用する機会が増加している。また,日本政府 は 2020 年東京オリンピック・パラリンピックの開催に向け,地域ごとに拠点病院を指定し外国人向けコーディ ネーターや医療通訳を派遣できる体制を整備している。これまでの外国人患者に関する医療の研究調査では,医 療従事者側からの分析が多く,外国人患者が直面してきた問題やニーズを含めた患者自身の視点からの分析は少 ない。このインタビュー調査では,5 カテゴリー(プライバシー,文化的相違と誤解,医療サービスへの期待,
医療システムの相違,言語関連の問題)に分け分析した。調査の結果,言語面以外でも過去の受診経験や医療に ついての文化的な価値観も医療サービスを受ける上で当事者の満足感に影響することが明らかにされた。
キーワード:ナラティブ・アプローチ,インタビュー研究,外国人患者
※1 福井県立大学学術教養センター
Center for Arts and Science, Fukui Prefectural University
I. Introduction
With over 2 million foreigners scattered throughout Japan, it becomes imperative to provide medical care for the growing number of non-Japanese speaking population.
In addition to the foreign residents, the tourist industry of Japan has announced that the number of foreigners visiting the country had exceeded 10 million in 2013. The Nikkei Newspaper reported that the current political administration plans to establish 30 medical institution hubs to provide healthcare services to prepare for the expected number of tourists visiting Japan during the 2020 Tokyo Olympic games1). These hubs must have healthcare workers or medical interpreters who can help hospital staffs communicate with patients in English, Chinese, Portuguese and Spanish. This trend of tourists flooding Japan is expected to flow over into other parts of Japan. The recent establishment of the Hokuriku Shinkansen on March 14, 2015 has brought attention to the western region of Japan with the hopeful increase in the number of both Japanese and foreign visitors to the Hokuriku areas of Toyama, Ishikawa and Fukui. Japan Railways has estimated over 20,000 visitors per day, possibly making the Hokuriku region a potential booming tourist destination2). According to the 2010 nation-wide census, Tokyo, Aichi and Osaka were the top three prefectures with the most foreign residents. For the Hokuriku region, Fukui ranked 18th, followed by Toyama (ranked 20th) and Ishikawa (23rd) 3).
Research of Japanese healthcare institutions and their treatment of non-Japanese patients have received some interest both nation-wide and on a prefectural level. In 2011, The Mitsubishi UFJ Research and Consulting (MURC) conducted a nation-wide survey of hospitals throughout Japan regarding the treatment of foreign patients at that time4). Of the 507 hospitals participating in this survey, close to 75% responded having accepted foreign patients and that the majority of the patients treated were foreign residents rather than tourists.
According to the report, 25.4% of the hospitals responded that in principle, they do not examine foreign patients who cannot speak Japanese. About 50% responded that
some hospital staff members were able to speak in a foreign language, e.g., English, Chinese, and Korean, therefore they could accept foreigners who speak those languages. Around 15% said that they request for an interpreter either from a municipal service or private interpreters. Regardless of language support systems within the hospitals or outside support, 27% of the hospitals claimed difficulty in the use of foreign languages when communicating with non-Japanese patients.
Nakagawa and Takuwa’s questionnaire study focused their research on Ishikawa Prefecture5). A questionnaire was sent to 125 medical institutions with a response rate of over 50% (33 local clinics and 32 hospitals). Of the 65 institutions participating in the study, 63 of them claim dealing with non-Japanese patients mainly from China, the United States (US), Brazil, the Philippines and Korea.
Difficulties reported by at least 10 of the healthcare facilities included providing adequate explanations of the illness or treatment, processing patient intake/reception, conducting medical examinations and prescribing medication.
These studies provide insights of the status quo of receiving foreign patients nation-wide as well as at the local level. They also provide perspectives from the medical standpoint and the needs felt by the healthcare providers.
Several research focusing on foreigners’ perspectives regarding seeking medical attention in Japan have provided some interesting insights. Kawauchi and Ogasawara reported their findings of responses by foreigners living in a prefecture where the number of foreign residents was relatively small6). They chose a rural area as opposed to metropolitan area, in order to investigate what language barriers foreign patients’ face.
A questionnaire was sent out to foreign residents regarding communication concerns they encountered when getting medical treatment. 280 questionnaires were distributed and 206 responded (73.6% response rate). The nationalities of the participants consisted of people from China (47.6%), Korea (10.2%), Malaysia (8.2%), the US (7.3%), Vietnam (5.3%) and others. The majority of the participants were students studying at the local universities, thus the majority of the respondents were in
their twenties and have lived in Japan for about a year to less than 5 years. The top three areas of communication anxiety during medical interviews that were expressed included: 1) explaining symptoms (49.0%), 2) inquiring about prescribed medicines (30.1%) and 3) asking about treatment methods (19.9%). In their study, the majority of their participants had at least intermediate level of Japanese. However, majority of them responded that anxiety will decrease if they can receive support from medical interpreters. The authors concluded that by providing professional healthcare interpreters, patients will feel less apprehensive when communicating in a medical setting with this added language support.
Dodo and Nagasaka examined the issues in Japanese healthcare experienced by Chinese female patients within Yamanashi prefecture7). Yamanashi prefecture was ranked 30th for the number of Chinese residents in the 2015 survey of Japan’s Chinese population8). Their data was gathered from a focus group interview which included an interpreter to help communicate with the Chinese participants and the research team. Through a focus group interview with an interpreter present to help with the communication between the research team and the Chinese participants, the women were asked to share what they felt were problems in Japanese medical institutions. Some of the issues included differences in medical systems of Japan and their own country, provision of medical services during the weekend and holidays, concerns and mistrust of the treatment plans and miscommunication due to difficult vocabulary and general communication style. The participants in the study also pointed out issues of discriminatory behavior of the medical staff and a lack of understanding of their culture.
In a similar study conducted by Nagasaka and Dodo, they approached foreign patients’ perspective of Japanese medical services in a different manner9). Participants for this research took part in an English class to share with the students about their medical experiences in Japan.
Their interactions and comments were recorded and later analyzed. Nagasaka and Dodo categorized the foreign participants into two categories according to whether
their home country was a “medically developed” or
“medically developing” country. According to their study, those from “developed” countries wanted to be treated as equal partners in the treatment process, expressed their concerns directly and made requests for certain types of treatments. On the other hand, patients who were categorized as coming from medically “developing”
situations wanted doctors who were perceived as being kind and friendly, to “feel close to and easy to talk with (like a family member)” (p.54). These two studies provide deeper understanding regarding foreign patients by investigating a specific group of patients and their needs.
Moreover, the latter study deepens our understanding of the characteristics and expectations of foreign patients who come from different cultures, belief systems, and expectations toward what “good” healthcare should be.
The Present Study
The idea of listening to “patient voice(s)” is quite new, though not a novel idea. The New York Times online newspaper, for example, features real life stories from actual patient dealing with various health issues10). University of Oxford’s website, Database of Patient Experience (DIPEx) is a collection of real patient’s experiences with health issues provided free to the public to stimulate discussion among a wide audience of healthcare providers and recipients11). Nuance Communications gathered a sampling of patients from different healthcare markets including the United States, the United Kingdom and Germany12). They categorized the survey responses into three areas: overall patient-physician experience, patient engagement and behavior, and patient awareness and preferences for technology. Research from the healthcare consumers, namely patients, helps to improve doctor-patient care and quality of health care services. This present study is small in scale, but provides some initial groundwork to give foreigners living in Fukui, especially those who live in the northern part of the prefecture, an opportunity to “voice”
their concerns and perspectives of how they are treated in Japanese medical settings.
II. Methods Data Collection
Participants were recruited through researcher’s local network and announcements in public gatherings.
Participants were given an explanation about the purpose of the study and were asked to fill out a simple background questionnaire and to sign a consent form allowing the interviews to be recorded and used as data for this project. Data collection was conducted between November 2014 and February 2015. A total of 13 foreign residents agreed to be part of this study.
Each participant met with one of the two researchers for the interview session, some lasting as short as 45 minutes to 2 hours. All interviews were conducted in English though not all participants spoke English as their native language. Open-ended interview questions guided the participants to share their perspectives of their experiences in Japanese medical institutions and allowed the narratives to be co-constructed with the interviewer (Holstein and Gubrium) 13). The recorded interviews were transcribed and reviewed to define and categorize the relevant concerns shared by the participants.
Ethical Considerations
As the study was a preliminary research, it did not go
through the official process of the Research Ethics Committee of the University of Fukui. However, the researchers adhered to professional and academic regulations of fairness and took appropriate measures of obtaining consensus from each participant to use the information shared for the purpose of this research. The purpose of the research, method, expected results and the issue of confidentiality were verbally explained to each participant. They were asked to sign a consent form stating they understood what the research was for and how the data was to be used. Furthermore, they were also informed the right to withdraw from the research at any time during the duration of the project.
Participants
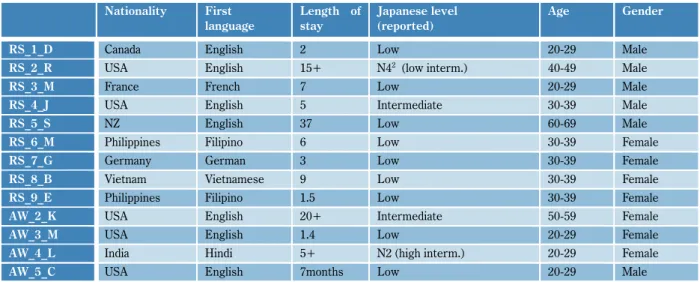
The following table summarizes the participants’
information based on the background questionnaire. Six male and seven female participants age ranged between 20 to over 60. Length of stay in Japan was from 7 months to 37 years. Though English was used during the interview, we had participants whose spoke French, Filipino, German, Vietnamese or Hindi as their native language. Participants’ self-assessment of their Japanese level revealed that most of them consider their Japanese language ability as low.
Table 1 A summary of the participants’ background
2 N4 is a level from Japanese Language Proficiency Test (JLPT). JLPT is a standardized test that evaluates Japanese language proficiency for non-native speakers. It consists of 5 levels: N1 (advanced) to N5 (Basic).
Nationality First language
Length of stay
Japanese level (reported)
Age Gender
RS_1_D Canada English 2 Low 20-29 Male
RS_2_R USA English 15+ N42(low interm.) 40-49 Male
RS_3_M France French 7 Low 20-29 Male
RS_4_J USA English 5 Intermediate 30-39 Male
RS_5_S NZ English 37 Low 60-69 Male
RS_6_M Philippines Filipino 6 Low 30-39 Female
RS_7_G Germany German 3 Low 30-39 Female
RS_8_B Vietnam Vietnamese 9 Low 30-39 Female
RS_9_E Philippines Filipino 1.5 Low 30-39 Female
AW_2_K USA English 20+ Intermediate 50-59 Female
AW_3_M USA English 1.4 Low 20-29 Female
AW_4_L India Hindi 5+ N2 (high interm.) 20-29 Female
AW_5_C USA English 7months Low 20-29 Male
Method of Analysis
The interviews were recorded and analyzed by both researchers. The process of analysis began retrospectively after all the data collection was completed and transcribed. Thematic analysis was carried out to seek and identify themes within the narratives14). First, both researchers individually looked over the transcribed data of each interview and identified episodes mentioned by participants that represented issues faced by foreign patients. Next, researchers met to discuss how these episodes will be categorized into several themes for consistency between the two researchers. Categorization was carried out separately by individual researchers.
Then, extracts from the data were examined and placed into these themes. Extracts were chosen for this study that would best illustrate the theme. As a result of these steps, five themes were identified and defined as reported below.
III. Results
Observations expressed by the participants from the interviews were categorized into the following five themes: Privacy and Confidentiality, Cultural Differences, Mismatch in Expectations, Differences in Medical Systems, and Language-related issues. These are defined below and excerpts from the data are provided.
Privacy and Confidentiality
Privacy and confidentiality are often used interchangeably but there are some differences. Privacy, for example, is considered a right of every individual and refers to having control over personal information about oneself and to have the assurance that unauthorized access to such information is protected15). The Hippocratic oath, one of the oldest documents outlining how doctors are to treat their patients places importance of nondisclosure. One modern version declares the following, “I (healthcare worker) will respect the privacy of my patients, for their problems are not disclosed to me that the world may know.” 16) It is expected by patients then, that healthcare workers at all levels will extend the same level of respect of one’s private information,
regardless of where patients receive medical care.
Nondisclosure, then, of a person’s physical (body) or any health information (orally expressed, electronically or non-electronically stored data) are seen as an inherent right for patients receiving medical attention17). All participants voiced concern over the issue of how private information and exposure of their body parts were handled during their visits to hospitals and clinics in Japan.
Participants expressed that they were uncomfortable when their private body parts were not treated with respect. This was especially true in the case of gynecological exams. An American female participant who has been in Japan over 20 years (AW_2_K) shared her concern that during a pap exam, anyone walking near the exam room could easily see what was going on. Her gynecologist was a Japanese female doctor who had lived and studied in the US:
Excerpt 1: Physical privacy
She (doctor) also spoke English. She studied in the US…then when I had to have the cervical exam, one time I noticed that the door at the back where the doctors and nurses are walking by is open. So, I said to her, I am like I noticed the door is open. She goes, well your face is covered and I said it’s not my face I am worried about, I always show my face. (AW_2_K)
K stressed the fact that she noticed that the exam room door was “open” during her exam. When K brought this to the doctor’s attention, she expected her doctor to close the door. The doctor responded that since the patient’s face was covered, it should not be a problem. To K, however, the exposure was not a matter of her face, but rather the “lower portion” of her body. While it may be a common practice for Japanese doctors to leave their doors open during an exam or to allow other hospital staff to walk into the room during the exam, K felt that this was offensive and showed unconcern for not respecting the patient’s dignity.
Our male participant from France (RS_3_M) described his distress of getting his blood taken in a room full of other patients during an annual health check-up. He felt that even a simple blood exam should have been done in a
private room rather than in a big room. This sense of having “no physical privacy” included annual health checks at schools and workplaces where data such as weight, height and blood pressure were often announced aloud in front of co-workers, school staff or even fellow students.
Lack of confidentiality, especially how personal medical information is accessible to people within the community was further emphasized by the following participant who felt uncomfortable because he was already somewhat known in his surrounding neighborhood. A male patient (RS_2_R) stressed the importance of ensuring foreign patients’ privacy as much as possible. In the case of foreigners living in smaller communities, they already
“stand out” so even a casual mention about seeing “such and such” at a certain hospital can identify the foreigner, even if names are never mentioned. To somewhat distance himself from his own community, R felt he needed to seek medical attention further away from home rather than go to a nearby hospital. Similarly, another male participant (RS_4_J) talked about how he was concerned that his employers learned of his visit to the hospital or about his medical condition because a hospital staff just “happened to mention” seeing him at the hospital. As a former Assistant Language Teacher (ALT) who came to teach for the Japan Exchange and Teaching (JET) Programme, his experience with Japanese colleagues knowing the reason for his hospital visit, no matter how minor, made him feel vulnerable to the gossip, even if there was no intent to harm him. As ALTs, they often rely on Japanese faculty members, foreigners who speak better Japanese or someone from the community to communicate at hospitals when they need medical attention. These volunteers are pressured into taking the role of an interpreter and are not necessarily trained or obligated to treat any information shared at the hospital as privileged information. The doctor-patient and “ad hoc interpreter” interaction therefore adds the risk of including an additional “ear” into the exam room. The concern here was how health-related information will spread through the helpful third-party. One interviewee
discovered that other faculty members had already heard about his medical condition and expressed genuine concern about his wellbeing. While this may be taken as Japanese kindness, not all foreigners welcome this extra care.
Cultural Differences
Cultural differences, especially how communication is conducted and expected as appropriate between doctor-patient and the power inequality experienced were mentioned as being concerns for the foreigners in this study. The doctor’s willingness to explain in detail for the patient makes the patient feel the physician has understood his condition. Inviting the patients to ask questions is another notably good doctor-patient communication skills. The lack of information and not allowing the time to ask questions are discussed below and are seen as power inequality and the passive role that the patient must take within Japanese hospital settings.
Excerpt 2: Power inequality
I realize that’s huge cultural difference too…If you are asking questions then maybe you stick out so just kind of do what you’re told and don’t ask questions…but I think in a setting where a Japanese people has a senior, especially a doctor, they don’t ask questions. They just sit and listen and do what they are told. (RS_1_D)
D (RS_1_D), a male Canadian felt that his time with the doctor gave him no room to ask questions. He notes that this was not because he couldn’t communicate adequately in Japanese but it seemed inherent in the culture. He commented that his Japanese wife and others have told him that this power difference was not just towards foreigners. Not wanting to “stick out” or further bother the doctor, they (Japanese people) “just sit and listen and do what they are told.” rather than to take time to discuss the treatment plan. D chose to passively do what the doctor ordered him to do without taking the time to press for more discussion time.
G (RS_7_G), a patient originally from Germany noted that the time it took for the doctor to decide on how to treat her condition was done quickly. The patient just reports to the doctor her symptoms. In turn, the doctor
decides on the treatment plan without the back and forth communication she was used to in her own country.
Excerpt 3: One-way communication
In Germany, I would like to explain what is wrong with me and so on and he (the doctor) would ask something or she would… and here (Japan) it’s much faster, like often it feels to me that it’s just like you just say the symptom and then oh, that’s it. (RS_7_G)
The communication between a Japanese doctor and the patient is uni-directional (doctor to patient) instead of interactive and the passive attitude Japanese patients have seems to contribute to this unequal power balance.
D (RS_1_D) observes that North American patients are more proactive in taking a role in their medical treatment and doctors provide an environment in which patient questions are a welcome aspect of the communication between physician and patient. Expecting longer and a more interactive communication time with the doctor but not having that type of interaction can lead to disappointment. Compliance, adherence to treatment and trust-building are known to increase when doctors spend more time and involve patients to have some say in their medical situation. Not doing so only builds suspicion and non-compliance or the seeking of treatment elsewhere18).
Nagasaka and Dodo reported a similar perspective told by foreigners who they interviewed in their study9). As mentioned earlier, patients who come from “medically developed countries” require equal relationship with the medical practitioners through expressing their concerns and requests. Back in their home country, these participants felt open to express their concerns to the doctors and to ask questions when they need more explanation. Thus, there was a sense that doctor and patient were on equal footing rather than unequal power balance. As Nagasaka and Dodo noted, however that Asian patients from countries like Thailand, China, Korea, and Afghanistan, seem to experience similar doctor-patient power structure as Japan and therefore either do not mention this as a negative aspect when seeing a physician in Japan.
Mismatch in Expectations
Our participants talked about what they expected or imagined would be the norm in a hospital visit and finding out differently. One interesting factor emerged from the interviews was how foreign patients’ preferred, at least initially, to seek medical attention at larger hospitals as opposed to smaller clinics. Reasons given include the assumption that larger hospitals will have more specialized physicians and will have someone who can communicate in your own language or at least have services that are provided to help you communicate with the hospital staff. In larger hospitals, they will be able to access English-speaking doctor or staff who are more globally trained or have a wider understanding of the concerns foreign patients. When this is not the case, then disappointment occurs. M (RS_6_M), a female Filipino interviewee expressed her thoughts below:
Excerpt 4: Big hospitals 1
I had to search for a big hospital because I know if it’s big, it’s more facilities maybe and the possibility of getting more chances of getting specialist that can speak English…and there is like English website. (RS_6_M)
A related expectation regarding larger hospitals is that they will have the same type of medical services that could be compared with a global business product that people in general are familiar with. J (RS_4_J) below was sharing that going to a Red Cross hospital in Japan should be the same as going to one in his own country. Like McDonald’s, the “product” will be the same quality world-wide:
Excerpt 5: Big hospitals 2
It’s like walking into McDonald’s here. You would hope that the service would still be about the same or the type or quality of food would be about the same. But walking to that hospital in particular, you are kind of like – it’s part of that cog of the Japan Medical System. (RS_4_J)
J notes his disappointment that his experience at a local Red Cross Hospital was not what he would have expected from a well-reputed organization and that it was “part of the cog of the Japan medical system.” Going to a bigger hospital did not guarantee access to hospital personnel who can communicate adequately in English or other
foreign language but instead meant longer wait time, higher cost (extra fee for services rendered if you do not come to the hospital with a doctor’s referral letter) and shorter outpatient clinic hours compared to the private clinics. Unmet expectations may lead to reduced trust, especially when there is gap between what they think should happen and what actually happens.
Differences in Medical Systems
Differences in medical systems have led to inconvenience, confusion and frustration for foreign patients. Two areas:
getting prescription for medication, and paying the medical bills are discussed below. The first difference is related to getting prescriptions filled at a pharmacy. At least in the US, regularly prescribed medicine can be refilled several times without having to see the doctor after the initial visit. Here in Japan, patients are required to set up an appointment to see their physician every time in order to continue receiving prescribed medication.
The visit may last only a few minutes to receive a quick check-up, however, patients have to endure long wait times just to see the doctor. In addition, prescription orders must be filled within four days after receiving the prescription document. Failure to explain this to the patient results in frustration at being denied the medicine because he/she did not go to the pharmacy right away.
Regarding the payment of the medical expenses, some patients expressed their confusion on when to pay and what was included in the payment. For instance, it is uncommon for patients from the US to pay upfront on the same day of the hospital visit because the bill is usually sent to their insurance company. After deductions, the insurance company sends the bill to the patient. Thus, patients from this type of system are not always prepared to pay on the same day as the hospital visit. The additional fee for services at the larger hospitals proved to be another point as mentioned in the previous section.
Participants who have talked about this noted that if they could communicate with a doctor in a smaller clinic, they would not go to a larger hospital, thus not having this extra fee. In addition to this problem, not knowing how to ask for a letter of referral makes the task of getting
medical treatment expensive, time-consuming and frustration. In sum, what may be a “natural” or “common sense” information for the Japanese or well-informed foreigners may not be true for the foreign patients who are new to the community.
Language-related issues
Kawauchi and Ogasawara among others have noted the language barrier as one of the common problems facing foreign patients6). In the case of our interviewees, they have either experienced misunderstandings due to their lack of the Japanese language or they mistrust the physician’s treatment because of inadequate explanation.
Such language problems result in non-compliance to the doctor’s instruction, improper use of prescription medicine, inadequacy in communicating their symptoms and medical concerns, and delay on the part of the patient to get the treatment. In this category, we would like to add that the language-related communication problems are not limited to oral communication but also in written form.
Excerpt 6: Literacy
The first time (at the reception) you need to write all this information which are all in Kanji and especially the medical Kanji are pretty high like all those, do you have allergy? Did you have main surgery? All those questions, it’s all written in Kanji. I can have easy conversation in Japanese, but writing, reading I can’t. (RS_3_M)
M was among the many foreigners who found the written instructions and information difficult to understand because everything was in Japanese. M notes that his Japanese level is good enough for daily conversation, but his reading ability was not adequate enough to comprehend and to complete medical forms and other literature. Furthermore, medical documents are even more challenging since the content is technical and unfamiliar vocabulary is used.
Another point that requires more attention is the English used by foreign patients for whom English is not their first language. Of the 13 foreign residents we interviewed, English was not their mother tongue for 6 of our participants. Not having adequate Japanese, they must
use English to communicate with the hospital personnel and doctors. However, as one of them pointed out, being a nonnative speaker of English often made it difficult to be understood because of her pronunciation, grammar and word choice and vice versa:
Excerpt 7: Being a nonnative speaker of English
When I am asking questions he (the doctor) cannot give me the right answer… maybe my pronunciation is not good, so he couldn’t understand (RS_9_E)
As in the excerpt above, non-native English speaker blamed herself as the cause of the communication breakdown. She believed that if she spoke English more fluently or more grammatically, then the doctor would understand.
Speaking and literacy skills may be a challenge for foreign patients, even if they can speak Japanese. To make it easier for foreigners, bilingual documents can be made or by adding furigana, or simplifying the Japanese can lower the language-based problems at the hospitals.
Secondly, there is a need to become aware that many non-native English users may not necessarily understand what is being said to them due to their own English speaking skills as well as the hospital personnel’s skills.
As one of our participants expressed, healthcare personnel should be aware that it is not always easy for the patients to use English, so there is a need to use clear, easy to understand English.
IV. Discussion and Conclusion
In this paper, foreign patient narratives were analyzed and categorized into five themes in order to understand what foreign patients experienced from the participants’
perspectives. Five themes were Privacy and Confidentiality, Cultural Differences Mismatch in Expectations, Differences in Medical Systems, and Language-related issues. First, how to handle physical and informational privacy is a delicate issue that concerns many foreign patients. Physical privacy in the examination rooms and informational privacy both inside and outside the consultation room should be handled with great care, since it can either develop or break the
patient’s trust in the doctor/healthcare workers. Second, cultural background of the patients changes the perspective and communication. It is important for the medical professionals to be aware of the different stance each patient might bring to the consultation rooms. Third, patients’ expectations of how they feel they will be treated at larger hospitals need to be addressed. These expectations might be a step to understand how foreign patients make decisions or adhere to the medical treatment. Fourth, differences in medical systems can lead to confusion and frustration. The norms for Japanese are not necessarily norms for foreign patients. Lastly, language challenges in a hospital setting include oral and literacy. Non-native English speaking foreign patients use English if they cannot communicate adequately in Japanese. However their pronunciation, grammar and vocabulary may not be easy to understand for the hospital staff. Conversely, they use English but not comprehend doctors and other hospital staff who use English. Thus, medical professionals should understand that English is not the almighty tool to address all foreign patients who come to the hospitals for treatments and that patients might not always be confident in using English as the main tool of communication. It is important for the healthcare professionals to be aware of the above aspects when encountering and providing supports for foreign patients.
Language issues are often pointed out as most important factor to be addressed in previous literatures.
However, it is important to note that language related issues are not the only concern when caring for foreign patients. As reported in this paper, handling privacy and confidentiality, understanding cultural differences and expectations they bring in, and explaining the differences in medical systems were also important factors to consider. Through accumulating narratives from the foreign residents, we found that stories provide us with specific details as experienced by the participants. Thus, it is beneficial to continue accumulating stories to understand the foreigner’s perspectives.
Limitations for this type of research must not be
ignored. First and foremost, interviews collected in this study are stories or perspectives of just a limited number of foreigners living in Japan. In this study, we had 13 participants who agreed to be interviewed by us. There is a need to take a look not only of patients who have limitations with the language but those who are fluent as well to see if their experiences are similar. In addition, there is a need to explore patients from diverse nationalities and languages that are not represented in this present study. For instance, what other factors cause the dissatisfaction or frustration at receiving medical attention at Japanese hospitals for foreign patients? How do foreign patients prepare for their visits? Where do they access information or what steps do they take to ensure that their medical needs are met?
In sum, this pilot study of the foreign patients’ stories has given several stepping-stones for further exploration.
At the educational level, for example, we could analyze how some of the issues mentioned in our research could be addressed. As part of the compulsory courses offered at universities, are issues such as confidentiality, cultural competency and the empowerment of patients discussed?
At the hospital level, are Japanese hospital personnel trained to deal with foreign patients? To what extent should the patient be involved in preparing ahead of the visit to the hospital? What are the resources easily accessible for the patients and how current are these resources? What are other factors make a hospital visit for a foreigner a positive or negative experience? How to systematically support foreign residents in the community who needs medical care is an important issue we need to tackle. Further research is needed to answer these questions and to find workable solutions to put research findings into practice.
Acknowledgement
We would like to express our deep appreciation to all the participants who shared their stories with us. This research was supported by Fukui Prefectural University Special Research Fund: Regional Contribution Research in 2014.
References
1) The Nikkei Newspaper: Asian Review: Japan to set up hub medical institutions for foreign patients.
<http://asia.nikkei.com/Politics-Economy/Policy-Politics/Ja pan-to-set-up-hub-medical-institutions-for-foreign-patients?
page=1> 2014 (Access: March 29th, 2015)
2) The Japan Times: Hokuriku shinkansen setting tourists abuzz.
<http://www.japantimes.co.jp/news/2015/03/02/reference/h okuriku-shinkansen-setting-tourists-abuzz/#.V33g_fmLSU k> 2015 (Access: April 25th, 2016)
3) Statistics Japan prefecture comparisons: Foreign Residents in Japan
<http://stats-japan.com/t/kiji/11639> 2010 (Access: April 25th, 2016)
4) Mitsubishi UFJ Research & Consulting: MURC Research Report ―The status quo of medical services for foreigners
~The results from the questionnaire on accepting foreign patients~
<http://www.murc.jp/thinktank/rc/politics/politics_detail/
120829> 2012 (Access: August 4th, 2014)
5) Nakagawa, K.., Takuwa, N. A study on the present status and prospect on medical care for foreign patients in Ishikawa Prefecture: Based on a questionnaire survey for registered medical institutes for foreigners. Ishikawa Journal of Nursing. 9: 23-32, 2012
6) Kawauchi, K., Ogasawara, M. Communication issues in medical settings for foreigners residing in Z prefecture:
Examining ways to improve the current state of medical interpreter service. Kyushu Communication Studies. 11:
1-18, 2013.
7) Dodo, M., Nagasaka, K. Issues on acceptance of residents rooting in foreign countries at medical institutions: Case of people from China living in Yamanashi Prefecture. Journal of Yamanashi Prefectural University Nursing Department. 15:
1-9, 2013.
8) Prefectural Ranking: The number of Chinese residents.
<http://todo-ran.com/t/kijis/11582> 2015 (Access: March 29th, 2015)
9) Nagasaka, K., Dodo, M. Multiculturalism in Medicine:
Issues in the Medicine found in narratives of foreign
residents in Yamanashi. Journal of Yamanashi Prefectural University Nursing Department. 13: 47-60, 2011.
10) The New York Times: Patient Voices.
<http://www.nytimes.com/interactive/2009/09/10/health/Pa tient_Voices.html?_r=1&> 2014 (Access: April 25th, 2016) 11) DIPEx International.
<http://www.dipexinternational.org/> (Access: May 28th, 2016)
12) Nuance Communications: Healthcare from the patient perspective.
<http://www.nuance.com/ucmprod/groups/healthcare/@we b-enus/documents/collateral/nc_031636.pdf> 2015 (Access:
April 25th, 2016)
13) Holstein, J. A., Gubrium, J. F. The active interview.
Thousand Oaks, CA: Sage Publications, 1995.
14) Bold, C. Using Narrative in Research. Los Angeles, USA:
Sage Publications. 2012.
15) TheInformatician.com
<http://www.hayajneh.org/glossary/vocabulary/p/PrivacyDe finition.html> (Access: June 20th, 2016)
16) MedicineNet.com: Definition of Hippocratic Oath.
<http://www.medicinenet.com/script/main/art.asp?articleke y=20909> 2016 (Access: June 20th, 2016)
17) What IS HIPPA?
<http://www.subr.edu/assets/docs/HealthCenter/What_IS_
HIPPA.pdf> (Access: June 20th, 2016)
18) Shukla, A. K., Yadav, V. S., Kastury, N. Doctor-Patient Communication: An important but often ignored aspect in clinical medicine. Journal of Indian Academy of Clinical Medicine. 11(3): 208-11, 2010.