近畿大学学術情報リポジトリ
25
0
0
全文
(2) Doctoral. Determination. in Body. of. Fluid. and. Dissertation. Trace. its. Levels. Kinki. of. University. (Director. C-Reactive. Clinico-pathological. Yasuro. Department. of. : Prof. April. Importance. Obana. Clinical. School Yasuhiro. 1996. Protein. Pathology,. of Medicine. Ohba).
(3) Determination. of. Trace. in. and. its. Body. Fluid. Levels. C-Reactive. Protein. Clinico-pathological. Department. Importance. Obana. Yasuro. of Clinical Pathology,. Kinki University (Director. of. School of Medicine. : Prof.. Yasuhiro. Ohba). ABSTRACT A new, highly sensitive counting. immunoassay. has facilitated. fluids. The established /ml. for adults. ng/ml. reference. and 2 ng/ml, and. intracranial. hemorrhage,. serum. renal. CRP. levels and in those. determination syndrome.. sensitivity The. transudate.. The. cerebrospinal. CRP. diabetic. after. characteristics. especially. cerebrospinal. in chronic. level in puncture. fluid. in the rather. of diseases.. slightly. to that. The determination. protein. body. fluid. (CRP),. spinal. fluid. 9 to 73. cord. diseases. high in patients. it was. acute. was. in serum.. in. higher. other than that. low, less and. the. serum. than. that. there. of low CRP levels in body. than in the. were no fluids,. helps to analyze. cerebrospinal. particle. immunoassay. diseases.. microdetermination,. the. nephrotic. exudate. than. However,. in. with urinary. and high. nephritis. higher. tumors,. whereas. transplantation,. nephritis,. puncture. similar. tract. and. increased,. However,. was. and. fluid was low in viral. and neurological. fluid and urine, as well as in blood,. : C-reactive (PCIA),. operations.. body. was 15 to 3,063 ng. for females). brain. kidney. particle. of CRP in various. was significantly. nephropathy,. as well as renal and urinary. Words. pressure. ( 2 ng /ml). fluid or urine, and. In. using. fluid and urine was less than. CRP level was slightly. various. CRP concentration. diagnostic. meningitis.. (CRP). CRP in serum. in cerebrospinal. fluid. The urinary. failure,. determination. 11 to 1,672 ng/ml. intracranial. the CRP level in cerebrospinal. infection,. protein. The CRP level in cerebrospinal. bacterial. increased. tract. Key. in. was not changed.. diseases. for males,. respectively.. increased. for C-reactive. values were as follows:. The CRP concentration. meningitis,. tumors,. method. more accurate. (26 to 3,992 ng/ml. for newborns.. 10 ng/ml. determination. counting.
(4) INTRODUCTION C-reactive. protein. (CRP). is a blood plasma. and Francis 1 in 1930, which causes wall of Streptococcus serum. in response. measuring. commonly. method'. or. the. established. immunoassay. (TIA)4.. turbidimetry. (LPIA)5,. and. method. including. or semiquantitative. developed. as determination. new clinical importance. clarified.. latex. methods. I evaluated. photometric. of trace. I clarified. to clarify. the intracapillary ( SRID)2. has. been. examination. nephelometry3. and. turbidimetric. immunoassay. immunoassay. with near. infrared. immunosorbent ( CIA )9-". CRP levels. Some studies. assay. have. been. have reported. the. CRP'. particle. counting. CRP levels in various. immunoassay. body fluids. Clinical importance. its importance. the kinetics. In. serum. counting. fluid).. destruction.. in immune. enzyme-linked. the newly developed. in the patient's. tissue. method. by Tillett. C in the cell. appearing. (EIA)8,. of trace. fluid, urine and puncture. values. including. for trace. of determination. In this study,. reference. years,. ( RIA )8 and. it to the determination. (cerebrospinal. methods. enzyme immunoassay. , radioimmunoassay. In this study,. immunodiffusion. However, the advance. quantitative. (ELISA)7. applied. tumors. radial. reported. with polysaccharide. such as inflammation,. single. In recent. reaction. first. substance. used for routine examination. has. component,. It is an acute reactive. CRP levels, a qualitative. precipitation. methods. precipitation. pneumoniae. to conditions. protein. in laboratory. of CRP. (PCIA),. other than. and. serum. has not sufficiently. been. medicine, that is, to establish. in various. diseases. and. the diagnostic. importance.. SUBJECTS Examination between. specimens. January. examination. studied. using. 168 samples. Measurement PAMIA-30" latex. domestic follows:. was. buffer. by. solution. PCIA". healthy. humans. reference. bound to antibodies. (blood,. serum. serum. of our on. using. an. An anti-human. (maleic. values. Various. (derived. from. human. solution, blood,. The principle. are mixed with test solutions. —2—. basic. of healthy. diseases. were. fluid.. measurement. CRP rabbit. acid buffer. physical. was used for. and 150 samples. immunoassay. hospital. cerebrospinal. fluid, 129 of urine and 88 of puncture. Co., Ltd.).. solution. adult. products)15' 16were used as reagents.. Latex particles. from. Laboratory. pooled patient. of healthy. for reaction. and CRP standard. standard. words,. of cerebrospinal. Electron. Clinical. specimens. were used to establish. performed. (Towa Medical. reagent,. 3 % gelatin). fluid) . In other. 40 females). Central. were used as body fluid specimens. of blood, and 482 samples. (110 males,. the. 1993 and. and staff. fluid, urine and puncture. urine. to. 1992 and April. for students. examination. submitted. AND METHODS. device,. antibody. binding. pH 7.5, containing in accordance. with. of this method. is as. containing. antigens..
(5) The. antigen-antibody. irradiated. reaction. to the mass. light. The scattered T%) is calculated of aggregated respectively.. occurs. within a sheath. light is converted with the number. latex particles. a latex. aggregated. flow structure. of unaggregated. can be calculated. based. is formed.. the intensity. Laser. M +. (monomer;. P being. to antigen. regarded. is. of scattered. pulse, and the aggregation latex particles. P) , and. rate is proportional. mass. to measure. into an electric. (polymer;. The aggregation. in the test solution. and. rate. (P/. M) , number. as. T (total). ,. CRP, and the CRP concentration. on the determination. line.. METHODS Basic examination The features solution curve). of determination. of the calibration. curve were examined. ( 0 , 10, 30, 90, 270, 810 and and the dilution. 5 specimens. test. of serum. (Fig.. Concerning. of 10 consecutive. determinations. were examined. using. collection /ml. rate. of specimens influencing. and. (. was serially. of diluted. bilirubin. solution. of serum. specimens. (97 mg/dl). were diluted. To examine. using a Millipore. concentrations. of 569.4 ng/ml. ethylaminoethanol. of. detection. detection. days. was added. 4 : 1 , and. sensitivity),. the. 10 ng. where the mean. sensitivity.. solution. (prozone. value. ng / ml). immediately. of turbidity,. In the study. of changes. of prozone high urine. solution'. buffer. solution. , borate. pH. standard. (pH 10.0). The collection. —3-. phenomenon. value. were. serum CRP. 'samples. specimen. specimens. and were. was filtered. value was compared. pH, urine. (pH 7.11) and 106.8 ng/ml. buffer. solution. CRP in each. and carry-over,. after. each turbid. with. reaction-. hemoglobin. to measure. phenomenon). 2 n-fold, and the presence. (0. To examine. ( 0 , 12.5, 25, 50 and 100 W/V%). filter (0.2 #1 and 0.8 g 1), and the pre-filtration. value.. McIlvaine's. reproducibility. (low concentration. at a ratio. (minimum. using. of urine (243. (30, 270 and 810 ng/ml). , 12.5, 25, 50 and 100 mg/dl),. excess. the influence. post-filtration. with. of serum. (132, 235, 379 and 642 ng/ml),. of antigen. in specimens. (. and Intrafat. In the study. investigated.. was examined. on 10 consecutive. diluted, and the concentration. as the minimum. specimen.. the carry-over. test. (calibration. solution did not cross the mean value + 3 SD of 0 -concentration. was regarded. to 4 specimens. of differences. solution. line. the simultaneous. of less than 1,000 -ng/ml. In the sensitivity. , 12.5, 25, 50 and 100 mg/dl). added. reproducibility. of standard. and 2 specimens. (169, 452, 718 and 1,328 ng/ml). solution. factors,. test, the linearity. of determination,. test, a standard. was examined.. - 3 SD of P/T%. 7 concentrations. in the determination. 1 ). In the dilution. 3 specimens. of serum. of standard. 2,430 ng/ml). the accuracy. zone). In the addition-collection 4 specimens. using. (166, 438, 784, 1,374 and 3,135 ng/ml). and 1,620 ng/ml).. to. method. showing. to the CRP. (pH 7.19) were used to adjust pH solution. ( pH. 9.18). test was performed.. and. 2 -. In the study.
(6) of anticoagulant ration;. agents,. CRP levels were compared. 58.1, 111.4 and 339.2 ng/dl). Na (25, 50 IU/ml). heparin. 2 K (200, 400 mg/dl).. after loading. were observed.. Examination. in CRP levels before. The. calibratin. The. calibration. of CRP in various of reference. The reference. value. adults. examination 19 items. Analyzer. (261. for. of blood chemical. curve. adults. loading. ( 2 males,. was performed. 30 minutes,. Werke, Marburg,. heparin. and EDTA-. 3 females,. between this method. (BNA; Behring. of the. agents,. and. age:. 23. and 1 hour nephelometry. Germany)".. PAMIA-30. of PAMIA-30. was. like. a sigmoid. curve. body fluids. values serum. males,. by the staff. curve. exercise. and immediately,. There was a correlation. Nephelometer. Determination. healthy. 4 anticoagulant. (CRP concent-. EDTA- 2 Na (200, 400 mg/dl). two step test in 5 healthy. The changes. 1. with. To examine the influence of exercise,. to 38 years).. Fig.. and those treated. Li (25, 50 USP/ml),. using the double Master's. using a Behring. between serum specimens. CRP. was established. 221 females). of our hospital examination). who (thoracic. showed. no. parametric. abnormalities. radiography,. and 63 healthy. -4-. by the. neonates. 9 items. method. in 482. upon. physical. of urine. analysis,. (cord blood)..
(7) The reference submitted. value for cerebrospinal. to the. cerebrospinal. Central. fluid. specimens. without. headache. clinical. such as. brain. rigidity,. specimens. and. value of urinary adults. staff. radiography,. at. blood. (10 items). Measurement. of body values. using patients'. examine. 1. of puncture deaminase examination,. Kawasaki. lactic. stimulating clinical. the. tryptophan. were. total. method. in 150 urine. examination. items by. and. percussion,. thoracic. revealed. ascites. and the changes. blood. no abnormalities.. examination. fluid, puncture. 1 specimen. , CRP. edema,. 1. of gallbladder. levels. were. measured. of puncture. fluid. ( appearance,. culture. examination. and precipitate), ( LDH). of pleural effusion,. 1 case of scrotal. fluid,. name, general. effusion). in CRP levels were examined. effusion,. puncture. dehydrogenase. and pericardial. fluid (55 specimens. drainage). bacterial. level. in puncture. fluid protein. fluid,. fractions,. rate and serum CRP. The puncture. fluid were measured. tumors,. and. of cerebrospinal. reaction),. for. to. adenosine. peripheral. blood. fluid CRP/serum. was also examined.. clinical. symptoms,. cell classification,. condition. ( 19 items ) , peripheral. effusion,. of pericardial. sedimentation. various. examinations. examination. the. diseases. total protein,. acid. cord. disease,. of. clinical. physical. ( 9 items),. intraperitoneal. level in puncture. spinal. Simultaneously,. urine analysis. specimens,. reaction,. erythrocyte. and. examination. of liver abscess. of. levels in cerebrospinal. ( brain. chemical. 6 specimens. CRP ratio as a CRP-index CRP. in whom auscultation. fluid CRP (pleural. diagnostic. Revalta. (ADA). reference. 59. symptoms,. on various. by the parametric. In 88 specimens of puncture. specimen. fluid,. healthy fluid,. cord-stimulating. were found. as. inquiry,. fluid CRP in various. 2 specimens. the clinical. specific gravity,. blood. and general. of ascites,. and. university,. using healthy. case of renal cyst, contents,. our. specimens.. 20 specimens. regarded. (110 males, 40 females). for puncture. were not obtained. were. CRP was calculated. pressure,. examination. Reference. They. collecting. of cerebrospinal. and spinal. abnormalities. specimens. values.. of healthy. students. in which no. selected.. reference. The reference. because. Of 168 specimens. findings. using patients'. of our hospital. difficult.. were. establishing. Laboratory. was extremely. and cervical. examinations,. Clinical. fluid CRP was established. subarachnoidal. neurological diagnostic clinical performed:. peripheral. and. use. findings. were. bacterial. fluid (pressure,. protein,. hemorrhage,. diseases name,. in 168 specimens. culture. of. Nonne-Apelt. blood examination,. -. 5-. degrees. of antibiotics,. Queckenstedt's. 'Dandy reaction,. Guillain-Barre. various. examined.. of cerebrospinal. of. presence. syndrome, meningitis ) . of. meninges-. Furthermore,. the. cerebrospinal. fluid,. test, tone, turbidity, reaction,. measurement. sugar,. fluid. following general. cell count, chloride. of erythrocyte. and. sedimen-.
(8) tation. rate. and serum CRP.. CRP levels in urine with various. (hematuria,. diseases. (various. tumor and transplantation urine. analysis,. creatinine, urinary. pyuria, renal. diseases. as well as other. bacteriological. uric acid). proteinuria. and. such as. diseases). examination,. measurement. CRP (ng/m1)/urinary. and. bacteriuria). renal. and. urinary. were measured.. blood. chemical. from. tract. infection,. Simultaneously,. examination. of serum. CRP. were performed.. (mg/dl). ratio. was examined.. creatinine. 129 patients. general. ( serum. BUN,. In addition,. the. RESULTS Basic examination. of determination. Good reproducibility The calibration. method. of differences. with the day was obtained. curve was like a sigmoid. showing the direct. connection. specimens.. However,. curve was noted.. The good. simultaneous. than. 1,000 ng/ml. difference. was obtained. until around. at the higher. reproducibility. detection. sensitivity. substance. reaction. system. was. 2 ng/ml.. protein.. No prozone. samples. showing. samples. was less than 0.006%. The collection. specimens. (antigen. high levels (97 mg/di).. using a Millipore. were obtained.. excess). was. Carry-over rate. chyle (turbidity), observed. of anticoagulant. at most 4.0%. No influences in CRP levels in 5 patients There was no difference I obtained n=139).. a high correlation However,. the determination. a comparison sensitivity. urine. was observed.. 6.01 to 10.04, and a. Na, heparin. Li, EDTA- 2 Na and EDTA- 2 K) was. exercise. coefficient. of turbid. of. 1 ). The CV% of CRP levels after the. of anticoagulant. between males. using. pH 3 (Table. (heparin. after. and M. it was low (less than 80%) at less than pH 5.50, and. at around. agents. RF protein. of turbidity. was obtained.. addition. test, the. on the coexisting. filtration. good. was impossible. test, the. even in the study. and after. filter was 97 to 93%. No influence. However,. of. between high and low concentration before. to. of less. reproducibility. was observed. rate was 95.2 to 103.1% within the urine pH range from. determination. range. In the sensitivity. The collection outcome. in both. zone, a slight tendency. 3 %, and the good. hemolysis,. 3 %.. linearity. was obtained. in the determination. No influence. such as bilirubin,. phenomenon. test, good. at CV of less than 4 %. In the addition-collection. was 96.3 to 105.5% and good results. minimum. 1,000 ng/ml. concentration. at CV of less than. among days was obtained. collection rate. curve (Fig. 1 ). In the dilution. to the origin. urine and serum. at CV of less than. agents. were observed.. loading. by the double Master's. and females. In comparison (r-0.991). two. test.. (BNA),. (y =1.026x +7.214,. at the low concentration. of BNA (less than 0.3 mg/di).. step. to other methods. with a close regression. could not be made. —6—. There were no changes. zone. below.
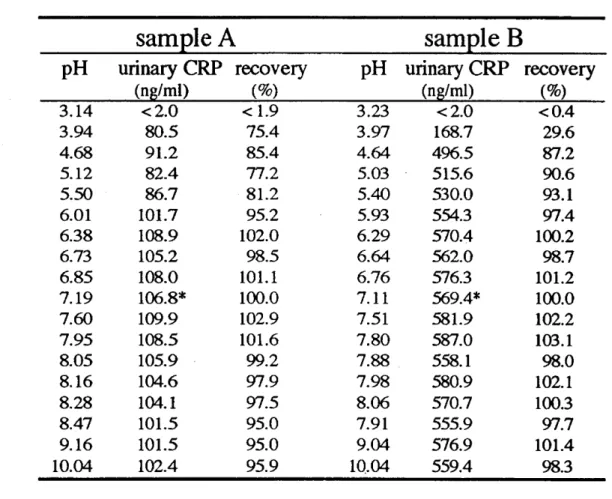
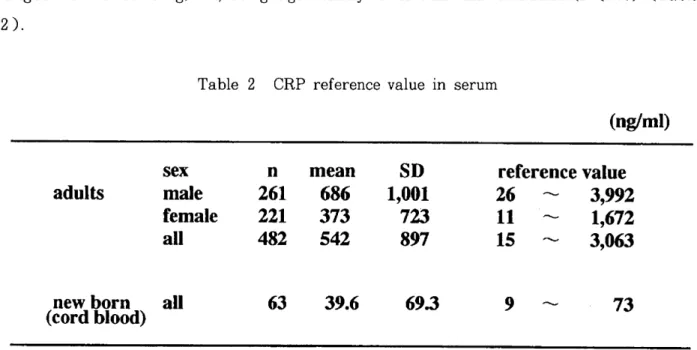
(9) Table. sample pH. 1. Influence. of pH. A. urinary CRP (ng/ml). sample recovery. B. pH. urinary CRP (ng/ml). recovery (%). < 2.0. < 0.4. (%). 3.14. < 2.0. < 1.9. 3.23. 3.94. 80.5. 75.4. 3.97. 168.7. 29.6. 4.68 5.12. 91.2. 85.4 77.2. 4.64. 496.5. 87.2. 5.03. 515.6. 90.6. 5.50. 86.7. 5.40. 530.0. 93.1. 6.01 6.38. 101.7 108.9. 81.2 95.2. 5.93 6.29. 554.3. 97.4. 102.0. 6.73. 105.2. 98.5. 6.64. 570.4 562.0. 100.2 98.7. 82.4. 6.85. 108.0. 101.1. 6.76. 576.3. 101.2. 7.19. 106.8*. 100.0. 7.11. 569.4*. 100.0. 7.60. 109.9. 102.9. 7.51. 581.9. 102.2. 7.95. 108.5. 101.6. 7.80. 587.0. 103.1. 8.05. 105.9. 99.2. 7.88. 558.1. 98.0. 8.16. 104.6. 97.9. 7.98. 580.9. 102.1. 8.28. 104.1. 97.5. 8.06. 570.7. 100.3. 8.47. 101.5. 95.0. 7.91. 555.9. 97.7. 9.16. 101.5. 95.0. 9.04. 576.9. 101.4. 10.04. 102.4. 95.9. 10.04. 559.4. 98.3. * original. Establishment. of reference. The reference ranged. values for serum. from 15 to 3,063 ng/ml. CRP for males 1,672 ng/ml. (P<0.01).. values for body. ranged. from. The reference. CRP based. fluids on 482 healthy. by the parametric 26 to 3,992 ng/ml,. value for males. urine. method. and that. was significantly. adults. (261 males,. The reference for females higher. value for. ranged. than. 221 females). that. from. serum 11 to. for females.
(10) In ranged. 63. specimens. from. of. cord. 9 to 73 ng/ml,. blood being. from. healthy. the. significantly. lower. the. neonates,. than. that. in adults. reference. value. (P<0.05). (Table. 2).. Table. 2. CRP. reference. value. in. serum. (ng/ml) sex male female all. adults. new born (cord blood). The based. reference. value. laboratory. The reference ng/ml). all. on 59 specimens. and various. for. healthy. 482. 542. of cerebrospinal findings. 39.6. fluid. reference 26 — 11 — 15 —. 69.3. CRP. 9. ( 2. fluid showing. value 3,992 1,672 3,063. to. 73. 10 ng. ml). no abnormalities. which were comprehensively. regarded. CRP was less than the minimum. was. established. in clinical. findings. as basic individuals.. detection. sensitivity. (2. in both male and female adults.. puncture. could not be established.. 686 373. cerebrospinal. SD 1,001 723 897. mean. 261 221. 63. value for urinary. of this method. However,. n. fluid specimens. were. not. obtained,. and. the reference. value.
(11) Changes. in body. Cerebrospinal CRP. fluid. CRP. fluid:. were examined. The. (Fig.. in. diseases. various. changes. in cerebrospinal. fluid. 2. lupus erythematodes. decompression),. spinal. (i) , cerebral. significantly. cord. (SLE). tumors. contusion. (h),. metastatic. subarachnoidal. hemorrhage. atresia. (e) showed. 2). (d: continuous. serum. and polyneuritis. (20.6 to 279.5 ng/ml). fluid (1,000 ng/ml. Eosinophilia ventricular. (a),. and slightly. 1 mg/di).. showed. blood. Guillain-Barre. drainage,. (k). syndrome. lung. showed. and high. on antibiotics), fluid. from. CRP. (b, c),. and newborn. (61.9 to 970.1 ng/ml). diseases. such as Guillain-. high CRP levels in cerebrospinal. high CRP levels in serum. —9—. tumors. or more). 3) Neurological. moderately. died after external. vertebral. of peripheral. high CRP levels in cerebrospinal. and low CRP levels in serum (less than syndrome. (g: the patient. thoracic. contamination. high CRP levels in cerebrospinal (6.0 to 43.2 mg/di).. Barre. and. in serum (mold!). CSF: cerebrospinal fluid. (f), brain tumors. (j) , and. levels in serum. tricuspid. diseases. Correlation of CRP levels in CSF with in serum An increase in the CRP level in cerebrospinal fluid in these conditions, Guillain-Barre syndrome and polyneuritis, may not solely result from the increased permeability into the blood-brain barrier of serum CRP or leakage.. 1) Systemic. cancer. in various. 2 ).. a : systemiclupuserythematodesCRP b : braintumor c : spinalcord tumor d : metastaticthoracicvertebraltumorfrom lungcancer e : cerebralcontusion f : contaminationof peripheralbloods hg : eosinophilia : Guillain-Barresyndrome i : Guillain-Barresyndrome j : subarachnoideal hemorrhage k : tricuspidatresia. Fig.. CRP. (0.6 to 0.9 mg/dl). (Table. fluid 3)..
(12) 4). Viral. (Table sp.,. meningitis. 3 ).. showed. However,. low levels of both. bacterial. methicillin-resistant. meningitis. Staphylococcus. showed. the high level of cerebrospinal. tumors. normally. slightly. high level of cerebrospinal. increase. in the cell count. cerebrospinal. showed. caused aureus. 3. an increase. in the. by Staphylococcus (MRSA). and. cerebrospinal. fluid CRP. sp.,. of CRP. diagnosis. Neurological disorders without infection Guillan-Barre syndrome Guillan-Barre syndrome Guillan-Barren syndrome. tumors. in CSF with. other. S - CRP. 279.5 68.4. 0.9 <03 <03. 15.8 43.2 23.4 20.6. polyneuritis multiple sclerosis multiple sclerosis Intraspinal tumor spinal cord tumor lung cancer metastasis in vertebra acute lymphocytic leukemia lung cancer metastasis in vertebra intraspinal invasion of AML cerebellar folium tumor intraspinal invasion of ATL. or intraspinal. level as well. ml) , but. there. WBC. of. laboratory. cell counts. 8500 12400. 1. 5200 6200. 5 5. 103. 1.4 1.1 0.6. 5000 7700. 6 4. 43 44. 13. 34. 4400. 52. 37. 7736.9. 11.2 17.5. 7300 7300. 0 26. 900. 16.8. 9400. 6. 173 26. 62.4 47.8. 1.7 2.3. 5500 3700. 0 1. 46 43. 35.0. 0.4. 7500. 0. 140. 34.6. 1.9 4.8. 21800 13000. 0 512. 280 52. 2.1. 7800. 88. 178. <03 <0_3. 7300 10400. 1404 596. 12 22. <2.0. 19200. 124. 20. 2.9 <2.0. 7200 4400. 77. 15. 52. 37. <2.0. (Table. 3 ).. 68. 12700. <0.3. in the. 268 157. 1. <0.3. 2.5. no. rotein. <0.3. <2.0. as. tests. 1.7. 144.7 12.9. was. was an increase. 0.4. 1792.2 396.5. parasella chondroma meningioma (postoperative state) Viral meningitis. aeruginosa. with meningitis. parameters. CRP. Corynebacterium. Brain. protein. there. complicated. C - CRP. paralytic exophthalmos alcoholic cortical cerebellar atrophy. fluid. fluid. However,. and serum. Pseudomonas. (34.5 to 7,736.9 ng/. in the cerebrospinal. Correlation. fluid CRP. fluid CRP (230.7 to 944.5 ng/ml).. fluid cell count in parasellar. Table. cerebrospinal. 33. 19. CSF : cerebrospinal fluid C-CRP : CRP in CSF ( ng/ml ) S-CRP : CRP in serum ( mg/d1 ) WBC : peripheral white blood cell count cell counts : cell counts in CSF ( / p 1) protein : total protein in CSF (mg/d1 ) AML : acute myelocytic leukemia ATL : adult T-cell leukemia. There. was a moderate. erythrocyte. sedimentation. administration increase. correlation. of antibiotics,. in the cerebrospinal. rate. between the peripheral ( Table. adrenal fluid. 4 ) . However,. cortex. hormones. CRP level regardless. --10. -. white blood in. cell count. granulocytopenia. and anticancer. drugs,. of the peripheral. and. caused there. was. white blood. /pi). the by an cell.
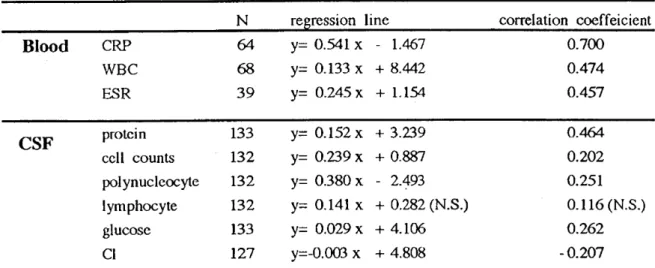
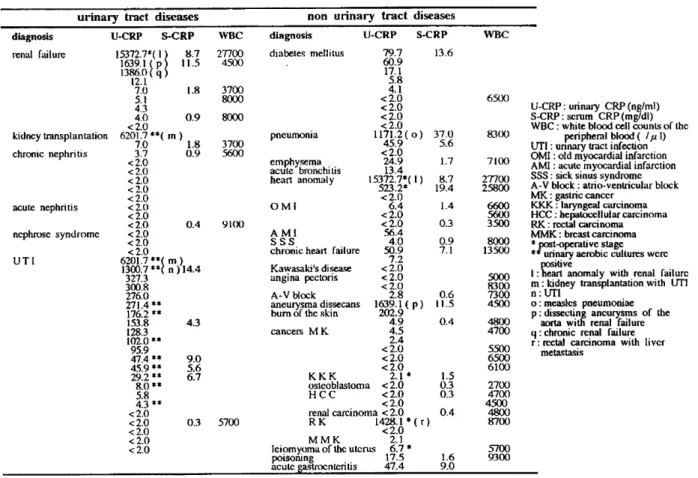
(13) count.. There was no significant. the cell count, moderate positive. polynucleocyte. correlation. reaction. However,. the cerebrospinal. 4. in patients. CSF. the cerebrospinal. count,. sugar. in the cerebrospinal. reaction. and. disease. fluid CRP level and chloride. Correlation. other. than. fluid. The cerebrospinal. and Nonne-Apelt. with Kawasaki. for globulin. reaction),. or intraspinal. a. fluid. had a slightly high invasion. of leukemia,. although. cerebrospinal. reaction.. of CRP. laboratory. Blood. monocyte. protein. (Pandy. between. fluid CRP level was high (115.0 to 446.8 ng/ml). fluid was negative. Table. count,. with total. for globulin. CRP level.. correlation. levels. in CSF. and. blood. with. other. parameters. of. tests. N. reffession. line. correlation. coeffeicient. CRP. 64. Y= 0.541. x. -. 1.467. 0.700. WBC. 68. y= 0.133. x. + 8.442. 0.474. ESR. 39. Y= 0.245. x. + 1.154. 0.457. protein. 133. y= 0.152. x. + 3.239. 0.464. cell counts. 132. y= 0.239. x. 0.202. polynucleocyte. 132. y= 0.380. x. + 0.887 - 2.493. 0.251. lymphocyte. 132. y= 0.141. x. + 0.282 (N.S.). 0.116 (N.S.). glucose. 133. y= 0.029. x. + 4.106. CI. 127. y=-0.003. x. + 4.808. 0.262 - 0 .207. CSF : cerebrospinal fluid WBC : peripheral white blood cell counts ( /,a I) ESR : erythrocyte sedimentation rate (mm/h) protein : total protein (mg/dl) protein : total protein in CSF (mg/di ) cell counts : cell counts in CSF ( //2 1) polynucleocyte : polynucleocyte counts in CSF( I lymphocyte : lymphocyte counts in CSF ( I fz 1) glucose : glucose concentration in CSF (mg/d1) Cl : chloride concentration in CSF (mmol/l) ( p<0.05 ) N.S. :not significant. Urine: renal. Of 129 urine. failure. infection. failure CRP. as a postoperative. following. pneumonia. kidney. (o) , dissecting. (q),. and rectal. (1,000 ng/ml. or renal. specimens. failure. patients. complication. transplantation aneurysms. carcinoma. or more), and. from. patients. with various. in heart. anomaly. ( m ) , urinary. of the aorta. receiving. tract. (r). 7. infections failure. showed. those urinary. with tract. ( n ) , measles. (p) , chronic. renal. high levels of urinary. in Table. 5 . In patients. with urinary. kidney. transplantation,. urinary. — 11 —. from. (1), complicated. with renal. with liver metastasis. as shown. diseases,. tract CRP. infections levels were. ).
(14) slightly. or moderately. high. However,. urinary. levels were. syndrome,. CRP. in chronic less than. nephritis,. with high serum CRP levels. Other. tract. diseases,. postoperative. slightly. high. levels of urinary. urinary. CRP. levels were. determination increases. slightly. sensitivity. in urinary. In diabetics. with. However,. urinary. high.. ( 2 ng / ml). CRP. with. in the. other. high. with renal. serum. diabetic. CRP. nephropathy. CRP levels. diabetics.. Furthermore,. test-positive. 5 ), but the relationship. with the volume. was not demonstrated.. CRP /urinary. ratio,. creatinine. (mg/dl). was examined. The ratio. may be useful. correlation urinary. and serum. diagnosis. kidney transplantation nephritis. acute nephritis nephrose UTI. syndrome. CRP (Table. 5. Urinary. 1639.1( p11.5 1386.0( q 12.1 7.0 1.8 5.1 4.3 4.0 0.9 <2.0 6201.7 **( m ) 7.0 1.8 3.7 0.9 <2.0 <2.0 <2.0 <2.0 <2.0 <2.0 <2.0 <2.0 0.4 <2.0 <2.0 <2.0 6201.7 1300 **( m ) .7 **( n )14.4 327.3 300.8 276.0 271.4** 176.2 **. diagnosis. 27700 4500. diabetes. 3700 8000 8000 3700 5600. 91(X). 4.3. " ** ** **. 5.8 4.3 ** <2.0 <2.0 <2.0 <2.0 <2.0. CRP. non. S-CRP. 9.0 5.6 6.7. 0.3. ml). x. 5700. ng / ml). and urinary levels. showed. or infection, than. there. the were. ( * * in Table The urinary. 100/urinary. creatinine. was 1,245 or more in 5 of 6 deaths. the prognosis.. There was no significant other. than. between. 6 ).. WBC. 15372.7*( 1}8.7. 153.8 128.3 102.0 95.9 47.4 45.9 29.2. The ratio. (ng/. CRP and various blood and urine parameters. diseases. U-CRP. renal failure. chronic. tract. CRP. as an index for evaluating. Table. urinary. is, urinary. in 129 specimens.. between urinary. CRP. that. specimens. nephrotic. ( 2. were lower. levels in all 10 urine culture of bacteria. and. sensitivity. than the patients. and patients. CRP.. nephritis. the determination. except patients. patients. acute. level. urinary. in various. tract. U-CRP. diseases S-CRP. 79.7 60.9 17.1 5.8 4.1 <2.0 <2.0 < 2.0 < 2.0 1171.2(0) 1171.2( pneumonia 45.9 <2.0 emphysema 24.9 acute bronchitis 13.4 15372.7*( 15372.7*( I) heart anomaly 523.2* <2.0 OMI 6.4 <2.0 <2.0 AMI 56.4 SS S 4.0 chronic heart failure 50.9 7 .2 <2.0 Kawasaki's disease <2.0 angina pectoris < 2.0 2.8 A-V block 1639.1 ( p) 1639.1( aneurysma dissecans bum of the skin 202.9 4.9 cancers M K 4.5 2.4 <2.0 <2.0 <2.0 2.1 * KKK osteoblasto osteoblastoma ia <2.0 <2.0 HCC <2.0 renal carcinoma carcin ma <2.0 renal <2.0 RK 1428.1 * ( r ) 1428.1 <2.0 <2.0 M M K 2.1 2.1 leiomyoma of the uterus ut rus 6.7 6.7 * 17.5 poisoning acute Qastrocnteritis 47.4 mellitus. -12-. diseases. WBC. 13.6. 6500. 37.0 5.6 1.7 8.7 19.4 1.4 0.3 0.9 7.1. 0.6 11.5 0.4. U-CRP : urinary CRP (ng/ml) S-CRP : scrum CRP (mg/di) WBC : white blood cell counts of the 8300 UTI peripheral blood ( /pi) : unnary tract infection OMI : old myocardial infarction 7100 AMI : acute myocardial infarction SSS : sick sinus syndrome 27700 A-V block : atrio-ventricular block 25800 MK : gastric cancer KKK : laryngeal carcinoma 6600 5600 HCC: hepatoccllular carcinoma 3500 RK: rectal carcinoma MMK : breast carcinoma 8000 *post-operative stage 13500 **urinary aerobic cultures were positive I 5000 8300 : heart anomaly with renal failure m : kidney transplantation with UTI n : UTI 7300 4500 o : measles pneumoniae p : dissecting aneurysms of the 4800 aorta with renal failure 4700 q : chronic renal failure r: rectal carcinoma with liver 5500 metastasis 6500 6 100. 1.5 0.3 0.3 0.4. 1.6 9.0. 2700 4700 4500 4800 8700 5700 9300.
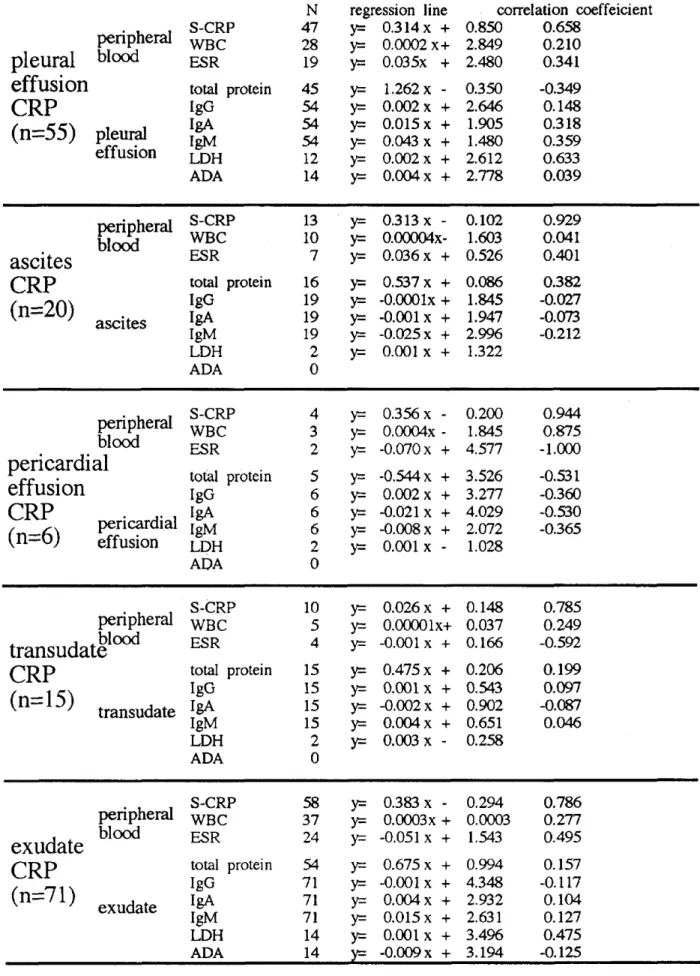
(15) Table. 6. Correlation. between. reuession CRP. Blood. WBC ESR BUN Uric acid protein. CRP. line. and. other. correlation. parameters. coeffeicient. n. Y= 0.249 Y= 0.039. x + 0.130*. 0.798. x + 8.738. 0.400. 57. Y= 1.089 Y= 0.040 0.016*. x + 0.063 x + 2.947. 0.217 0.318. 21. x + 1.708. 0.207. x - 0.046*. 0.250. 47 53. x - 0.203*. 0.363. 116. creatinine. Urine. urinary. 0.030* y = 0.401. 37. 55. WBC : peripheral white blood cell counts ( 1p 1) ESR : erythrocyte sedimentation rate (mm/h) BUN : blood urea nitrogen in serum (mg/dl) uric acid (mg/dl) creatinine (mg/dl) ( p < 0.05 ) * not significant. Puncture fluid: Eighty-eight specimens of puncture fluid (53 specimens of pleural effusion, 17 specimens of ascites, 6 specimens of pericardial effusion, 12 specimens including abscess puncture fluid) were examined. Fifty-five specimens were exudate, 15 were transudate, 18 were unclear. The underlying diseases for the transudate nephrotic syndrome, liver cirrhosis carcinoma). and. were congestive heart failure,. (including liver cirrhosis complicated with hepatocellular. and acute myocardial infarction. The underlying diseases for the exudate were. pleuritis and peritonitis caused by malignant tumors in most cases. The puncture fluid CRP level was correlated with the serum CRP (S-CRP) level, with no difference between exudate and transudate,. but there was no correlation. with total protein (TP), IgG, IgA, IgM, LDH,. ADA, white blood cell count of peripheral blood (WBC) and erythrocyte. sedimentation. rate. (ESR) (Table 7 ). All CRP-indices of exudate were more than 50%, and the CRP level in the exudate (mean; 34,245.9 ng/ml, transudate. (mean; 8,133.6 ng/ml,. characteristic. SD; 42,526.6 ng/ml). SD; 15,744.0 ng/ml).. findings.. — 13 —. =. was 4 times higher than that in. However, there were no diagnostically.
(16) Table. 7. peripheral. pleural effusion CRP (n=55). blood. pleural effusion. peripheral. ascites CRP (n=20). blood. ascites. Correlation. between. N 47 28 19. regression y= y= y=. total protein IgG IgA IgM LDH ADA. 45 54 54 54 12 14. S-CRP WBC ESR total protein IgG IgA IgM LDH ADA. other. parameters. correlationtion coeffeicient. line. 0.314 x + 0.0002x+ 0.035x +. 0.658 0.210 0.341. y= y= y= y= y= y=. 1.262 0.002 0.015 0.043 0.002 0.004. + + + + +. 0.350 2.646 1.905 1.480 2.612 2.778. -0.349. 13 10 7. y= yr-y=. 0.313 x 0.00004x0.036 x +. 0.102 1.603 0.526. 0.929 0.041 0.401. 16 19 19 19 2 0. yz-- 0.537x y= -0.0001x y= -0.001 x y= -0.025 x y= 0.001 x. + + + + +. 0.086 1.845 1.947 2.996 1.322. 0.382 -0.027 -0 .073 -0.212. 4 3 2. y= y= y=. 0.356 x 0.0004x -0.070 x. +. 0.200 1.845 4.577. 0.944 0.875 -1 .000. 5 6 6 6 2 0. y= y= y= y= y=. -0.544 0.002 -0.021 -0.008 0.001. + + + + -. 3.526 3.277 4.029 2.072 1.028. -0 .531 -0 .360 -0 .530 -0.365. 10 5 4. y= 0.026 x + yz-- 0.00001x+ r= -0.001 x +. 0.148 0.037 0.166. 0.785 0.249 -0 .592. IgM LDH ADA. 15 15 15 15 2 0. y= y= y= y= y=. 0.475 0.001 -0.002 0.004 0.003. x x x x x. + + + +. 0.206 0.543 0.902 0.651 0.258. 0.199 0.097 -0 .087 0.046. S-CRP WBC ESR. 58 37 24. y= y= y=. 0.383 x 0.0003x -0.051x. + +. 0.294 0.0003 1.543. 0.786 0.277 0.495. total protei n IgG IgA IgM LDH ADA. 54 71 71 71 14 14. y= y= y= y= y= v=. 0.675 -0.001 0.004 0.015 0.001 -0.009. + + + + + +. 0.994 4.348 2.932 2.631 3.496 3.194. 0.157 -0 .117 0.104 0.127 0.475 -0.125. protein. ADA S-CRP. peripheral WBC ESR transudate total protein CRP IgG (n=15) transudate IgA. exudate. and. 0.850 2.849 2.480. S-CRP. exudate CRP (n=71). CRP. S-CRP WBC ESR. peripheralWBC blood ESR pericardial total effusion IgG IgA CRP IgM (n=6)i.rdialiefruicasio LDH. peripheral blood. puncturn. -. 14 -. x x x x x x. x x x x x. x x x x x x. 0.148 0.318 0.359 0.633 0.039.
(17) DISCUSSION The CRP level in normal phase. reactive. serum. substance. is extremely. which significantly. tumors. or necrotic. lesions.. Therefore,. tumors. and tissue destruction. has an isoelectric consists. of. The methods. as is other. of measuring. immunonephelometry5,. at the unit of mg/dl. Recently, nation. highly. serum. non-RIA. of determination. remains. to be evaluated.. sensitive. determination. Therefore,. I examined. of CRP to clarify. CRP. 110,000. CRP. 21,50021, and. is mainly. immunoassay. (TIA)4,. (SRID)2. as a usual. assay. of CRP at the unit of it g/dl. have facilitated. a clinical index in early period. of CRP in cerebrospinal. as a crystal. acid sequence".. turbidimetric. immunodiffusion. the administration. of inflammation,. proteins'.. ETA', ELISA7 and CIA'". order, providing. inflammation,. is approximately. RIA9 is used for the determination. sensitive. amino. of approximately. acute phase reactive. radial. to acute. CRP was isolated. weight. CRP levels include. as well as in determining. importance. molecular. CRP is an acute. used as a marker. the complete. weight. and single. of CRP at the ng/ml. infections. et al. reported. with a molecular. in hepatocytes. in response. clinical examination.. of 6.2, and the. 5 subunits. synthesized. laser. point. increases. it is commonly. in routine. by Wood et al.". In 1979, Oliveira. low (less than 0.5 mg/di).. fluid'. the determi-. diagnosis. of antibiotics5.. and urine". of newborn However,. the. other than in serum. the CRP in serum and body fluid by highly. its importance. in the perspective. of laboratory. medicine. I examined. the methodology. concentrations. from. 2 to 1,000 ng/ml.. sensitivity). was. Concerning. the determination. and. 2 ng/ml,. the reproducibility. collection. test,. Furthermore,. chyle (turbidity),. used. accuracy,. of difference rate. in this. to or higher. the simultaneous among. days. of coexisting. RF, and M protein or carry-over. In addition,. the collection. adults. (261 males,. ml, females; established. 221 females). 11 to 1,672 ng/ml).. value. detection. was less than. 3 %,. 4 % . In the. addition-. outcome. obtained.. was. phenomenon. hemolysis,. (antigen. excess. rate was 95.2 to 103.1% within the pH range. of the determination. The reference. at. of EIA6 and ELISA7.. No prozone. to be an appropriate. value was established.. less than. CRP. (minimum. such as bilirubin,. 0.991). Therefore,. the importance. than that. quantitate. substances. to nephelometry. To clarify. sensitivity. reproducibility. was. from 6.01 to 10.04. In comparison PCIA appeared. It could. was 96.3 to 105.5%, and a good. was no influence. zone) was observed.. study.. The determination. which was similar. the collection there. of PCIA. (BNA), there was a good correlation methodology. was 15 to 3,063 ng/ml. fluid, each reference. CRP that. I established. for adults. (males;. The value was similar. using RIA by Claus et al.", ELISA by Okamoto. — 15—. for this study.. of CRP in the body. for serum. (r=. to the reference. on. healthy. 26 to 3,992 ng/ values. previously. et al.", LPIA by Ohtake. et al.',.
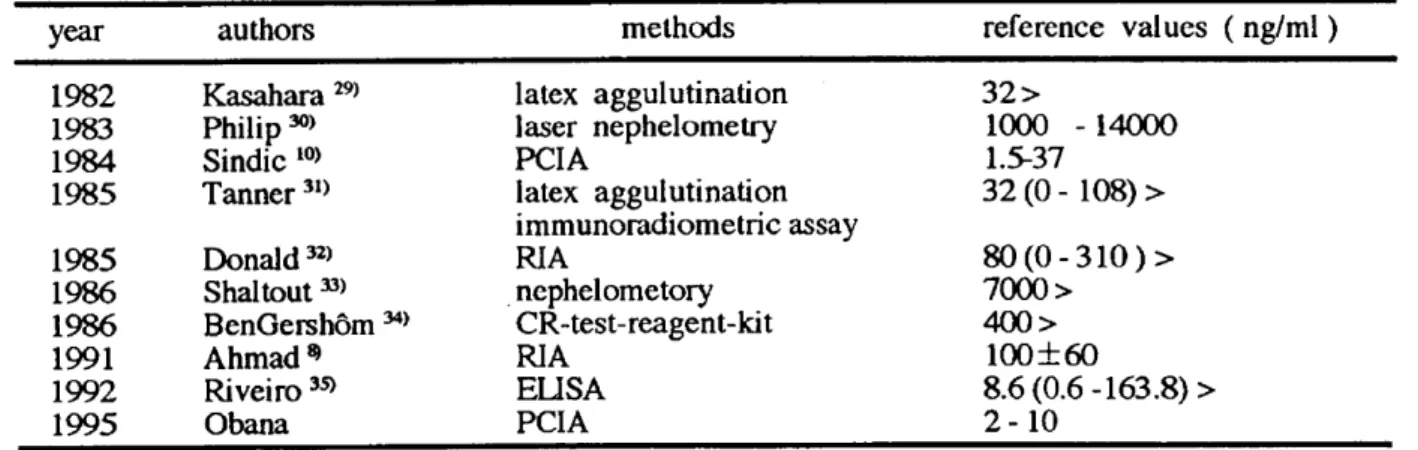
(18) CIA by Kitahashi females. et al." and Sasaki. as in other. reports'.. on CRP measurement formation. of oral. infections. newborns. serum. and intestinal. there. flora. host'.. However,. on. to that. method,. fluid CRP using 59 specimens. and various. ng/ml.. However,. was 1.5 to 37 ng/ml. 1985 1986 1986 1991 1992 1995. Donald 32) Shaltout 33) BenGershom Ahmad* Riveiro 35) Obana. In bacterial infection,. decreased. before before. cerebrospinal nation. 8. of CRP. the the. fluid. for establishing. findings.. The reference. Raference. the CRP. value. was. (Table. 8 ) . Since. the reference. the reference. value. of. regarded. value based. value ranged. a. from. on. 2 to 10. fluid CRP by PCIA of Sindic et al.'. reference values ( ng/ml ). fluid. cerebrospinal before. in cerebrospinal. 32> 1000 -14000 1.5-37 32 (0 - 108) > assay. level in cerebrospinal. cerebrospinal. changes. The. values of CRP in CSF. latex aggulutination laser nephelometry PCIA latex aggulutination immunoradiometric RIA nephelometory CR-test-reagent-kit RIA ELISA PCIA. 34). meningitis,. birth. I determined. fluid comprehensively. methods. Kasahara 29) Philip 3°) Sindic 10) Tanner 31). after. in. value of 9 to. neonates.. I established. of cerebrospinal. range of cerebrospinal. authors. 1982 1983 1984 1985. immediately. the reference. of healthy. Therefore,. 8 ).. Table year. Therefore,. infection. In this study,. and established. was not available,. laboratory. (Table. not completed. index of newborn. value has been established. the conditions. the reference. have. loading. fluid CRP varied with the study8. 10,29,35and neither. cerebrospinal. findings. of exercise. than. in adults.. fluid of healthy adults. clinical. value. to a severe condition".. diagnostic. blood. higher. is immature.. such as false negativity. nor unified reference. satisfying. function. exacerbated. of cord. cerebrospinal. as basic individuals. Newborns. birth have been indicated'.. value for cerebrospinal. determination. a slightly. was no influence. and immunological. problems. 63 specimens. low compared. showed. reports".. used as the most reliable. a few days after. based. The reference. of. in other. CRP level in cord blood of neonates,. 73 ng /ml extremely. Furthermore,. once develop may rapidly. and false positivity the serum. Males. values as described. CRP is commonly. the compromised. et al.".. fluid. cell cell. count count. the cerebrospinal fluid. is important. — 16 —. 80(0 -310)> 7000 > 400> 100±60 8.6 (0.6 -163.8) > 2-10. fluid. increased. increased.. At. the. decreased.. In. other. fluid cell. count.. in early. diagnosis. at. the. initial. recovery words,. Therefore, and. stage. stage,. it. CRP. in. the determifollow-up.. The.
(19) CRP level in cerebrospinal 100 ng/ml). was. low. fluid Donald et al.' at. the initial. diagnostic. importance. sensitivity.. In viral meningitis,. than 2.9 ng/ml. was small,. (mean;. index in differentiating. Hansson. et al." , BenGershOrn. cerebrospinal bacterial. fluid in patients. meningitis. level was also increased invasion. of leukemia,. Abramson. bacterial. or viral infection diseases,. and polyneuritis while that between. However,. sclerosis,. permeability there. CRP. cerebrospinal there. no. significant. polynucleocyte. cerebrospinal. with TP or serum. than. there. The cerebrospinal. spinal cord tumors,. Kawasaki. in. most fluid. CRP. of. level was. was an albuminocytologic. cerebrospinal showed. syndrome increased dissociation. CRP. or leakage.. fluid as described. protein. in cerebrospinal. was a moderate. cerebrospinal monocyte. a correlation. between. In. correlation. blood or ESR.. fluid. cell. count,. count,. sugar. cerebrospinal. and fluid. several studies revealed a correlation. 41, but others. did not"' ". The relationship. to be clarified.. of urinary. of urinary. such as. may not solely result. of serum. with total. the. in. fluid cell count. Therefore,. fluid. have not". In addition,. fluid CRP and serum CRP'. CRP remains. value. with. low. diseases. In Guillain-Barre. There. and SLE.. intracranial. fluid was markedly. barrier. CRP. intraspinal. disease. cases. value. fluid. metastasis,. in the CRP level in cerebrospinal. count,. have previously. the determination. determination. a median. fluid in these conditions. correlation. between. showed. meningitis.. coefficient. in. meningitis. as well as noninfectious. in aseptic. levels. et al. 8, Donald. fluid CRP and the white blood cell count of peripheral. was fluid. CRP. Ahmad. positive. was 0.464 and 0.700, respectively.. Some studies. The reference. brain. et al.",. In addition,. meningitis.. into the blood-brain. CRP and TP32,33,23,41'while others between. the differentiation. level and the cerebrospinal. was no increase. Corrall. that. cerebrospinal. not. Furthermore,. fluid may be. and reported. than meningitis. fluid protein. were low, less. examined. is. the. by Sindic et al.10. The correlation. cerebrospinal chloride.. other. CRP. that. and serum. also. hemorrhage,. the. in determination. al.'. tuberculous. in the CRP level in cerebrospinal. fluid and serum between. was. the cerebrospinal. previously. fluid. and spinal cord tumors,. reported. of problems. in my study, the CRP level in cerebrospinal. from the increased multiple. et. and aseptic. that. considered. from viral meningitis.. was possible.. being similar to that. in serum. an increase. with meningitis,. reported. et al.". Gray. that. They. sensitivity;. the CRP level in cerebrospinal. meningitis. and. meningitis. have. Gray. neurological. et al.'. subarachnoidal. et al.'. hemorrhage.. bacterial. in brain. be because. Therefore,. et al." described. bacterial. meningitis.. levels in cerebrospinal. and viral meningitis. et al." and Vaishnavi of CRP between. CRP. by RIA (determination. of purulent. but this may. 1.2 ng/ml).. a useful. stage. obtained. sensitivity,. CRP based 2 ng/ml.. CRP by this method. —17--. on 150 specimens. of healthy. CRP was not present showed. a good. urine. in healthy. collection. rate. was. less. urine.. The. between. the.
(20) urine. pH 6.0 and 10.0. However,. less than pH 6.0, and was (Table. 1). There was. 6) was adjusted in acid-range. clarified.. no correlation. tract. for. urinary. irreversible. of laboratory. the detection. However, this may be because. infections. tract. and. infection culture. diagnostic. (77.3%), test. CRP as well as the urinary CRP level was. renal. nephritis,. the urinary. 9 diabetics, without. the urinary. nephropathy. 7 ng/ml. confirming. CRP /urinary. appear. urine,. ultrafiltration. reaction. creatinine that. in. In 2 patients. therapy.. suggesting. the ratio since. transude. was. higher. study. in severe. cases. the. CRP. molecular. weight. basement. of. membrane. than approximately. is. CRP. level and permeability. this does not appear. serum. CRP. with. diabetic CRP. CRP. for. the effect. performed.. of. The urinary. more. in deaths). ,. CRP may not normally. for. 110,0002' , and. substances. with. level. Therefore,. of the glomerular. basement. a. urinary. or more, and there. to be a simple transudation. ----18. Of. in 4 patients. 50,000 daltons47. However, in my study,. with serum CRP levels of 0.9 mg/dl. the urinary. level was. of urinary. approximately. is selective. failure,. the urinary. ( 1,245 or. the prognosis.. In my. 5 patients.. and evaluating. was not. of. CRP level of 0.9. 5 diabetics. the usefulness. rate. with chronic. sensitivity. transplantation,. kidney transplantation a follow-up. into urine due to the increased. of the kidney. However,. in. is an index for evaluating. CRP was detected in patients between. et al." reported. However, ratio. kidney. CRP. in the remaining. or more. receiving. after. at the glomerular. weight of less. a correlation. it was 4.1 ng/ml. or more. Kaden. the rejection. immunosuppressive. molecular. However,. or infection.. level was. with a serum. CRP level was less than the determination. complications.. Kuramochi. with renal. Of 6 patients. sensitivity. urinary. failure.. syndrome.. than the determination. reported. that the detection. the determination. but it was less. leakage,. in. less than. mg/dl,. 8. CRP was detected. The urinary. in 1 patient. of. of. or more).. CRP level was 3.7 ng/ml. been. rate. or more in 8 of 9 patients. in nephrotic. CRP.. 6. et al.". and the serum CRP level was also high (0.9 mg/dl sensitivity. in. tract infections.. CRP level were high in chronic. 2 ng/ml. CRP. 100%). Therefore,. and reported. occurs. not. The detection. and urinary. method for urinary. with renal diseases,. has. of nonspecific. CRP.. (specificity;. than pH. of urinary. Voghenzi. urinary. ELISA. of CRP. of urinary. was also high. Furthermore, tract. (less. medicine. infections.. auxiliary. aciduria. degeneration. reported. the association. study, the urinary. when. et al." using. have been made on the determination. the bacterial. CRP may be an effective et al." indicated. that. in the acid range. by De Fazio. previously. urinary. positive. reported. decreased. in the CRP concentration. CRP concentration between. gradually. CRP in the perspective. CRP was high in urinary. all specimens. with that. Few studies. et al.'. with urinary. rate. pH 7 , suggesting. of urinary. since the blood. urinary. no increase. specimens.. Okamoto. patients. consistent. to around. The importance. the collection. CRP. was may. membrane. along with urinary.
(21) protein. since there. (r =0.363). However,. was no significant. The kidney. is partially. the urinary. was higher. components. in puncture. and the CRP-index. production. of CRP.. transudate.. There. level in. into. hypotheses. in topical. Kushner. and Kaplan". serum. infarction.. supporting. 2 classes,. local production. tract. CRP. of CRP.. was 0 to 17.7%, and there. than. or. was. level. fluid or urine,. 1.7 to 340% (mean;. 50% were from. the exudate.. fluid CRP level was higher. lobar. was. pneumonia,. 4 times. higher. than. suggesting than. local. that. in the. fluid CRP level and the. serum. were observed.. where CRP is produced in the liver. However,. or reticuloendothelial indicated. The CRP. free CRP or mucopolysaccharide-binding. synthesized. tissues. the potential effusion,. the puncture. CRP.. and the regulation the possibility. has not completely. local production. that. CRP. been. ruled. myocardial. fluid CRP level was also higher infarction. of. of CRP since a high. joint fluid, or necrotic. of acute myocardial. or small. fibers than. in the. cell lung carcinoma,. of CRP.. of low CRP. as well as in blood, helps. urinary. and excretion. CRP). the puncture. findings. in pleural. 2 cases. The determination urine,. 100/serum. cancer. between. In my study,. CRP level in. and urinary. than in cerebrospinal. of more. on the region. organs. level of CRP was present myocardial. protein. to those in serum.. is, the puncture. of lung. no disease-specific. CRP may be mainly. is synthesized out"-".. 100%, that. was a correlation. are several. x. a CRP-index. 2 cases. Serum CRP is classified. metabolism.. fluid were similar. The CRP level in the exudate. CRP level. However,. There. CRP ratio (CRP-index). fluid (CRP. showing. was more than. CRP. urinary. with the metabolism. fluid (138.2 to 150,507.0 ng/ml). for puncture. the serum. between. of CRP. in puncture. 40%). All the specimens The CRP-index. associated. CRP x 100/serum. may be no local production The protein. correlation. levels in body to analyze. fluids,. especially. cerebrospinal. cerebrospinal. diseases. fluid. and. as well as renal. and. diseases.. ACKNOWLEDGEMENTS I wish to thank advice and editing. Laboratory A part Automation. Professor I thank. Yasuhiro. Ohba. my laboratory. (Department staff. for their help, and Towa Medical of this study Society. (1993, Hiroshima),. was presented. (1993, Chiba),. and technologists. Electron. of Clinical. of Clinical Pathology. — 19 —. Pathology). of Japan Pathology. Association. for. of the Central. Co., Ltd. for technical. at the 25th Meeting. 40th Meeting. and 41th Meeting. of Clinical. Clinical. Clinical. support. Examination. Association of Japan. his. of Japan. (1994, Iwate)..
(22) References 1.. Tillett WS and Francis somatic. 2.. fraction. T Jr (1930) Serological. of pneumococcus.. Suzuki H (1985) C-reactive. reactions. in pneumonia. with non-protein. J Exp Med 52: 561-571. protein. (CRP).. Nihon Rinsho. 535 (Syuki. rinji zoukangou). :. 481-483 3.. Manabe. S (1980). Measurement. of C-reactive. protein. by Behring-laser. nephelometer.. Igaku No Ayumi 115: 398-401 4.. 5.. Nakagawa. E,Ikeda. TIA, latex. agglutination. Nishida. K, Akari. A, Ohtani. method.. Kasahara. of a CRP assay. Rinsho Kensa. Jidouka. quantitation. using various. Gakkai. kits;. Kaishi 12: 66-71. of C-reactive. protein.. Nippon. Kaishi 15: 627-63. K, Sato M, Kimura. of C-reactive. Nippon. H (1992) High sensitive. Rinsho Meneki Gakkai 6.. T (1987) An evaluation. Y, Nakano. M, Fukamachi. protein by EIA one-step sandwich. I, Suzuki K (1988) Measurement. method. using monoclonal. antibody.. Eisei. Kensa 37: 16-23 7.. 8.. Abe A, Kawade. M, Maeda. linked immunosorbent. assay. Rinsho Kensa. Gakkai. Jidouka. (ELISA). serum,. for C-reactive. protein. (CRP). sensitive. enzyme-. in serum.. Nippon. J (1991) C-reactive. protein. in CNS infection.. Indian. 28: 1167-1170. Collet-Cassart particle. S, Makino K (1987) A highly. Kaishi 12: 39-43. Ahmad P, Ali SM, Fakhir S, Chadra J Pediatr. 9.. M, Seishima. D,. counting. Mareschal immunoassay. and cerebrospinal. of C-reactive. fluid samples.. 10. Sindic CJM, Collet-Cassart. in serum. JC, Sindic CJM, Tomasi protein. JP, Masson. PL (1983) Automated. and its application. to serum,. cord. Clin Chem 29: 1127-1131. D, Depre A, Laterre. and cerebrospinal. fluid in various. K, Itoh Y, Nakamura. F, Yamagishi. EC, Masson. neurological. PL (1984) C-reactive. disorders.. J Neurol. protein. Sci 63: 339-. 344 11. Sasaki. assay 12. Nishida. of C-reactive. of neonatal. Y, Takenaka. of C-reactive. significance.. Nippon Rinsho. 14. Obana Y, Takenaka. evaluation. infection.. K, Nakamura. determination. assay.. by PAMIA-30. Rinsho Kensa. A, Ohtani H, Saito M, Ohmori N, Nishida. early diagnosis 13. Obana. protein. Y, Itai Y, Abe T, Kawai T (1994) A sensitive. protein. Nippon. Rinsho. Kensa. Gakkai. T, Furuta. in the cerebrospinal Gakkai. Y, Yamazumi. for C-reactive Jidouka. Gakkai. — 20—. system. for. Zasshi 90: 2691-2700 I, Ohba. Y (1994). Micro-. fluid and it's clinico-pathological. Kaishi. T, Furuta. protein. 17: 132-138. H (1986) New monitoring. Syonika. Y, Yamazumi. Kensa Jidouka. K, Nakamura. of measurement. Nippon. Kiki Shiyaku. 19: 716-721 I, Ohba Y (1995) Fundamental. in urine by particle. Kaishi 20: 93-96. counting. immuno-.
(23) 15.. Baudner S, Haupt H, Hubner R, Kawai T, Saitoh K (1994) Establishment reference preparation. for 14 plasma proteins/CRM. of a new. 470= RPPHS Lot 5. Rinsho Kensa. Kiki Shiyaku 17: 465-483 16.. Itoh Y, Kawano K, Iwata S, Kanno T, Ohkubo A, Ichihara K, Sugahara Hirabayashi. Y, Saitho K, Kawai T (1995) Evaluation of national standard. T, Igarashi. S,. IFCC plasma. protein CRM470. It's property, safety and reaction. Rinsho Kensa Kiki Shiyaku 18: 1-12 17.. Sakagishi Y, Hosaki S, Konishi K, Okuyama T (1977) Rinsho Kensa Kohza 14 (2nd ed) Rinsho Kagaku,. Hosyasei Doigenso Rinshokensa. Gijutsu. Tokyo,. Ishiyaku. Syuppan,. pp405-406 18.. Hirabayashi Measurement. Y, Asano M, Uchida K, Kubono K, Tsukada of C-reactive protein by Behring-laser. Y, Takahashi. nephelometer.. M (1993 ). Rinsho Kensa Kiki. Shiyaku 16: 259-267 19.. Wood HF, McCarty M, Slater RJ (1954) The occurrence. during acute infection of a. protein not normally present in the blood. J Exp Med 100: 71-79 20.. Oliveira EB, Gotschlich EC, Liu T-Y (1979) Primary. structure. of human C-reactive. protein. J Biol Chem 254: 489-502 21.. Gewurz H (1983) The biology of C-reactive protein, In: Dixon FJ, Fisher DW (eds): The biology of immunologic disease. New York, HP Publishing Co.Inc.,pp139-153.. 22.. Claus DR, Osmand AP, Gewurz H (1976) Radioimmunoassay. of human C-reactive protein. and levels in normal sera. J Lab Clin Med 87: 120-128 23.. Okamoto H, Nishi A, Matsui A, Miyazaki R, Kuroda M (1984) A sensitive assay of Creactive protein in the serum and various body fluids by ELISA. Rinsho Byori 32: 651660. 24.. Ohtake T, Sekiguchi H, Tanaka K, Jinnouchi K, Hagiwara Determination. of CRP by latex photometric immunoassay. T, Kano S, Iri H (1987). with use of LPIA-300 system.. Nippon Rinsho Kensa Jidouka Gakkai Kaishi 12: 714-719 25.. Kitahashi S, Mizuhara Y, Komiya M, Matsui T, Okuda K (1993) Sensitive determination of human normal serum CRP by counting immunoassay CIA). Igaku Kensa 42: 136-140. 26.. Ohtake T, Ohtsuka Y, Ishibashi M, Kano S, Iri H (1992) Counting immunoassay. for. measuring C-reactive protein in serum. Rhinsyo Kagaku 4 : 259-265 27.. Shimetani N, Hachimura K, Nishida A, Ohtani H (1994) Quantitation protein. by a highly sensitive immunoassay. concentration 28.. in normal adult. Kitasato. (1). of serum C-reactive. Evaluation of the immunoassay. and. Igaku 24: 97-103. Nishida A (1986) High sensitive quantitation. of C-reactive protein and its change in. pathologic condition (II) Study of early diagnosis of neonatal infection. Kitasato. —21—. Igaku.
(24) 16: 402-403 29. Kasahara kensa. M, Nakamura. 0 (1982). Detection. Ann Trop Paediatr 31. Tanner. 32. Donald. in cerebro-spinal. in infective. Shaltout. meningitis. fluid. Ann Trop Paediatr 34. BenGersOm. fluid. Clinica Chimica. AF, Schoeman. A, EL-Shirbiny. cerebrospinal. A, Killander. (CSF). C-reactive. fluid. Eisei. diagnostic. 35. Ribeiro. MA, Kimura. RT, Irulegui. meningitis.. J Trop. CJ, Pepple JM, Moxon. 37. Hansson. with meningitis.. LO, Lindquist. cerebrospinal Methods. of rapid. C-reactive. protein. Acta 147: 267-272. A, Elheit. fluid C-reactive. SA (1986). in the diagnosis. Evaluation. of suspected. de Zegher F (1986) Cerebrospinal. value and pathophysiology. I, Colletto. of. meningitis.. GMDD,. fluid C-reactive. Eur J Pediatr. Ribeiro. IgM and C-reactive. 145: 246-249. CE, Farhat. protein. CK (1992). in the identification. Med Hyg 95: 87-94 ER, Hughes WT (1981) C-reactive. J Pediatr. protein. in spinal. fluid. 99:365-369. L, Linne T, Sego E (1987) Quantitation. fluid and serum. by zone immunoelectrophoresis. of C-reactive assay. (ZIA).. protein. in. J Immunol. 100: 191-195. BM, Simmons. of C-reactive other. J, Ragheb. fluid levels of lysozyme,. of children. meningitis.. J Lab Clin Med 106: 424-427. protein. GJJ,. in meningitis:. 36. Corrall. in neonatal. 6: 31-35. protein. of bacterial. protein. JF, De Beer FC (1985) Cerebrospinal. in childhood.. E, Briggeman-Mol. Cerebrospinal. fluid C-reactive. AL, Bull FG (1985) The clinical value. PR, Strachan. protein. 40. Abramson. UK, Dhand. profile. R, Agnihotri. meningitis.. JE. (1986). Quantitative. in patients. with. bacterial. N, Ganguly. NK (1992) C-reactive. levels. meningitis. and. antigens. Journal. in cerebrospinal. of Hygiene,. proteins,. fluid of patients. Epidemiology,. with. Microbiology. 36: 317-325. JS, Hampton. KD, Babu S, Wasilauskas. protein from cerebrospinal. nervous. system. Katayama. fluid. and mycobacterial. reactive. 41. Kawamura. S, Volanakis. 108: 665-670. and tuberculous. and Immunology. H, Barnum. in cerebrospinal. J Pediatr. C, Dhand. immunoglobulin pyogenic. DR, Mason. protein. conditions.. 39. Vaishnavi. Ozaki. in spinal. 102: 715-717. AR, Collins. measurement. 38. Gray. protein. 32: 656-661. 30. Philip AGS, BAker CJ (1983) Cerebrospinal. 33.. of C-reactive. diseases.. J Infect. K, Seo K, Saitoh A, Watanabe. fluid for differentiating. MJ (1985). meningitis. The use of C-. from other. central. Dis 151: 854-858. H, Matsunaga. M, Matoba. M, Sichijo K, Oikawa. M, Go T, Katsunuma. BL,Marcon. T, Ebisawa. M, Seki T, Nara. T, Kobayashi. N, Uekusa. M (1988) CRP in cerebrospinal. — 22—. T, Sakata. R,. T, Nakae. Y,. fluid. Syonika.
(25) sinryo. 51: 1763-1772. 42. Yamagishi. 43.. Y, Yamaguchi. of CRP by latex photometric. cerebrospinal. fluid and its clinical significance.. De Fazio SR, Monaco protein.. 44. Voghenzi. tract. Nenpou. quantitative. (3)Determination. of CRP in. Rinsho Byori 33: 797-801. (1983) An enzyme. Immunology. Sensitive. immunoassay. for. urinary. C-. 1: 276-283 in urinary. C-reactive. protein. in urinary. Boll Soc Ital Biol Sper 62: 925-930. M, Sawada. Measurement. T, Sasaki. of C-reactive. K, Tamura. protein. H, Shimada. in urine.. Jichi. I, Yamagishi. Ika. Daigaku. Y, Iwata H (1985). Rinsho. Kensa. Gishi. protein. in urine. 10: 68-71. 46. Kaden. VJ, Groth. serum. of. Nephrologie Kawai. J (1986) Simultaneous. patients. following. 49. Wood. protein,. HF, Montella. formation.. Gitlin. JD, Gitlin. In: Kawai. Tokyo,. urinary. S (1957) Studies. J, Thorbecke. protein. patients. of C-reactive. trasplantation.. Zeitschrift. T (eds). Igaku. K (1990) The mechanism. : How to think about. 50. Hurlimann. kidney. and clinical aspects.. M, Yokoyama. T (eds). determination. and. of urinary. proteins.. proteins.. Tokyo, Igaku. on the Cx-reactive. GJ, Hochwald. Their. In: Sugino. N, Kawai. Shoin, pp1-20. protein.. J Exp Med 106: 315-321. GM (1966) The liver as the site. of C-reactive. J Exp Med 123: 365-378 JI,Gitlin. with rheumatoid. D (1977) Localization arthritis.. MH (1961). Arthritis Studies. of C-reactive. Rheum. method. necrosis. in local inflammatory. lesions. J Exp Med 114: 961-973. I, Kaplan. Studies. for the localization. MH (1963). in heart. in induced. of acute. phase. of Cx-reactive. of acute. myocardial. 286-292. —23---. protein. in synovium. of. 20: 1491-1499. chemical. protein. proteins.. Shoin, pp 470-472. I, Kaplan. reactive. Urologie. : The plasma. Kushner. 53. Kushner. fur. and. 79: 87-91. T (1980) C-reactive. fundamental. 52.. Diagnostic. infections.. 48. Orita. AP, Gozzo JJ. immunoassay.. A, Camerini G, Mari R (1986) Changes. 45. Kuramochi. 51.. I, Iwata H, Kawai T (1985). determination. reactive. 47.. S, Shimada. protein.. protein. phase. in rabbits.. protein.. infarction. (1) An immunohistoAssociation. (2) Localization. in rabbits.. with. of Cx-. J Clin Invest 42:.
(26)
図


+5
関連したドキュメント
Analogs of this theorem were proved by Roitberg for nonregular elliptic boundary- value problems and for general elliptic systems of differential equations, the mod- ified scale of
Goal of this joint work: Under certain conditions, we prove ( ∗ ) directly [i.e., without applying the theory of noncritical Belyi maps] to compute the constant “C(d, ϵ)”
Then it follows immediately from a suitable version of “Hensel’s Lemma” [cf., e.g., the argument of [4], Lemma 2.1] that S may be obtained, as the notation suggests, as the m A
Correspondingly, the limiting sequence of metric spaces has a surpris- ingly simple description as a collection of random real trees (given below) in which certain pairs of
It provides a tool to prove tightness and conver- gence of some random elements in L 2 (0, 1), which is particularly well adapted to the treatment of the Donsker functions. This
[Mag3] , Painlev´ e-type differential equations for the recurrence coefficients of semi- classical orthogonal polynomials, J. Zaslavsky , Asymptotic expansions of ratios of
We formulate Wolfe-type dual and Mond-Weir- type dual problems for our nonsmooth multiobjective problems and establish duality theorems for weak Pareto-optimal solutions
In the operator formalism, we study how to make noncommutative instantons by using the ADHM method, and we review the relation between topological charges and noncommutativity.. In
