Maxillofacial bone regeneration with osteogenic matrix cell sheets: An experimental study in rats
Yoshihiro Ueyama
a, Takahiro Yagyuu
a,*, Masahiko Maeda
a, Mitsuhiko Imada
a, Manabu Akahane
b, Kenji Kawate
c, Yasuhito Tanaka
d, Tadaaki Kirita
aaDepartmentofOralandMaxillofacialSurgery,NaraMedicalUniversity,840Shijo-cho,Kashihara,Nara634-8521,Japan
bDepartmentofPublicHealth,HealthManagementandPolicy,NaraMedicalUniversity,840Shijo-cho,Kashihara,Nara634-8521,Japan
cDepartmentofArtificialJointandRegenerativeMedicineforBoneandCartilage,NaraMedicalUniversity,840Shijo-cho,Kashihara,Nara634-8521,Japan
dDepartmentofOrthopedicSurgery,NaraMedicalUniversity,840Shijo-cho,Kashihara,Nara634-8521,Japan
ARTICLE INFO Articlehistory:
Received11December2015
Receivedinrevisedform15August2016 Accepted17August2016
Keywords:
Boneregeneration Mandibulardefect
Bonemarrow-derivedstromalcells Cellsheet
ABSTRACT
Objective:Regenerationofmaxillofacialbonedefects,characterizedbyrelativelysmallbutcomplicated shapes,posesasignificantclinicalchallenge.Osteogenicmatrixcellsheets(OMCSs)haveosteogenic abilityand goodshaping properties and maybe ideal graftmaterials. Here,we assessed whether implantationofOMCSscouldbeusedtorepairmaxillofacialbonedefects.
Design:Weadoptedaratmandibularsymphysismodel.Theratmandibleisformedbyapairedboneand thecentralportionconsistingoffibroustissue.Thereisnobonetissueatthesite;accordingly,thissite wasinterpretedasaphysiologicalbonegapandwasusedforevaluation.Ratbonemarrowcellswere cultured inmedium containingdexamethasoneand ascorbicacidphosphate tocreate OMCSs.The OMCSs were implanted into the rat mandibular symphysis without a scaffold. Microcomputed tomographyandhistologicalanalyseswereconductedafter2,4,and8weeks.
Results:Twoweeksafterimplantation,microcomputedtomographyimagesandhistologicalsections showedsomesparsegranularcalcificationtissuewithinthebonegapatthemandibularsymphysis.At4 weeks,thecalcificationtissuespread,andthegapofthemandibleswerecontinued.At8weeks,this continuousnewbonetissuewasmatured.Theexperimentalgroupshowedabundantnewbonetissuein thegroupwithOMCSimplantation,butnotinthegroupwithshamimplantation.
Conclusions:OurpresentresultsindicatedthatuseofOMCSsmaybeanoptimalapproachtowards achievingmaxillofacialregeneration.
ã2016ElsevierLtd.Allrightsreserved.
1.Introduction
Maxillaryalveolarcleft,facialtrauma,boneresectiondueto cancer, periodontal disease, and bone atrophy after tooth extractionmayresultinnon-healingmaxillofacialbonedefects.
Autologous bone grafts are considered the gold standard for
repairingsuchbonedefects(Behniaetal.,2009;Liu,Tan,Luo,Hu,
&Yue,2014; Xieet al., 2007;Yoshiokaet al., 2012).However, donorsitemorbidityisanimportantconsideration.Maxillofacial bonedefectsareoftensmallerthanthosecommonlyencountered in orthopedicsurgery, buthave morecomplicated morphology (d’Aquinoetal.,2009).Thus,theabilityofthegraftmaterialto assume a complex shape is essential for maxillofacial bone regeneration.
Recently,researchershavebeenworkingtodevelopcell-based bone repairmethods asa substitute forautologousbone grafts (Kawate et al., 2006; Morishita et al., 2006). We previously developed a cell transplantation method based on cell sheet technology with bone marrow-derived stromal cells (BMSCs), whichwereculturedinthepresenceofdexamethasone(Dex)and ascorbicacidphosphate(Akahaneetal.,2008).Thesecellswere liftedascellsheets,termedosteogenicmatrixcellsheets(OMCSs), Abbreviations: BMSC,bonemarrow-derived stromalcell;OMCS,osteogenic
matrix cell sheet; Dex, dexamethasone; H&E, hematoxylin and eosin; OPN, osteopontin; OCN, osteocalcin; micro-CT, microcomputed tomography; TCP, tricalciumphosphate.
*Correspondingauthor.
E-mailaddresses:[email protected](Y.Ueyama),
[email protected](T.Yagyuu),[email protected](M.Maeda), [email protected](M.Imada),[email protected] (M.Akahane),[email protected](K.Kawate),[email protected] (Y.Tanaka),[email protected](T.Kirita).
http://dx.doi.org/10.1016/j.archoralbio.2016.08.017 0003-9969/ã2016ElsevierLtd.Allrightsreserved.
ContentslistsavailableatScienceDirect
Archives of Oral Biology
j o u r n a l h o m e p a g e : w w w . e l s e vi e r . c o m / l o c a t e/ a o b
2.Materialsandmethods 2.1.Animals
Allanimalstudieswereapprovedbytheanimalcareanduse committee of Nara Medical University before beginning the experiments.Fischer344(F344)ratswerepurchasedfromJapan SLC,Inc.(Hamamatsu,Japan).Seven-week-oldmaleratswereused asdonorsformarrowcellpreparation,and15-week-oldratswere usedasrecipients.
2.2.Cellcultureandcellsheetpreparation
OMCSs were used in this study and were prepared as previouslyreported(Akahaneet al.,2008;Inagaki et al.,2013;
Nakamura et al., 2010). In brief, rat bone marrow plugs were flushed out and resuspended in basic culture medium, i.e., minimumessentialmedium(NacalaiTesqueInc., Kyoto,Japan) containing15%fetalbovineserum(Gibco,Invitrogen,CA,USA) and1%antibiotics(100U/mL penicillinand100
m
g/mLstrepto-mycin;NacalaiTesqueInc.).CellswereculturedinT-75flasksina humidified atmosphereof 95% air with 5% CO2 at 37C. After reachingconfluence, theprimaryculturedcellswereharvested using trypsin/ethylenediaminetetraacetic acid (Gibco, Invitro- gen).TogeneratetheOMCSs,theharvestedcellswereseededata celldensityof1104cells/cm2in6-cmculturedisheswithbasic culture medium, 10nM Dex (Sigma-Aldrich, MO, USA), and 0.28mM ascorbicacidphosphate (WakoPure ChemicalIndus- trials, Kyoto, Japan) and then subcultured. After reaching confluence,thecellswererinsedtwicewithphosphate-buffered saline(Gibco,Invitrogen)andthenformedintoa sheetusinga scraper(Fig.1A).
2.3.InvitroevaluationofOMCSs
SamplesoftheOMCSswerefixedin10%formaldehydeneutral buffer solution for 1 week and embedded in paraffin. Each specimen was cut into 5-
m
msections, and the sections werestainedwithhematoxylinandeosin(H&E).Immunohistochemi- cal staining for type I collagen, osteopontin (OPN), and osteocalcin (OCN) was performed on 5-
m
msections mountedonglass slides.To enhance antigenretrieval,all sections were treated with 3% hydrogen peroxidase for 10min to block endogenous peroxidase activity and subsequently blocked for 10min at 37C with 1% bovine serum albumin, followed by overnight incubation at 4C with specific primary antibodies, including anti-typeI collagen (LB1102; LSL, Inc., Japan;1:500 dilution), anti-OPN (01-0091; ARP, Inc., USA; 1:100 dilution), and anti-OCN(M186; TaKaRa Bio, Inc., Japan;1:100 dilution).
left and right mandibles, the periosteum was incised and separated. The fibrous tissue between the left and right mandibles was then curetted, creating space for the implant (Fig.1D).Finally,weimplantedalumpofOMCSsintothespace (Fig.1E)andclosedtheperiosteumandskinlayersseparately.We performed thisprocedure in 30 rats (experimental group); an additional 10 rats underwent surgery without implantation (controlgroup).Tenanimalsweresacrificedateachtimepoint (2,4, and8weekspostoperatively)intheexperimental group, and10animalsweresacrificedat8weekspostoperativelyinthe control group. The mandibles were compared using micro- computed tomography(micro-CT) and histologicalanalyses to evaluatetheabilityofOMCSstofilltheboneatthemandibular symphysis.
2.5.Micro-CTanalyses
Theharvestedratmandibleswereanalyzedusingamicro-CT (Toscaner–32300
m
-FPD; Toshiba ITand Control Systems Corp.,Tokyo,Japan).Eachmandiblewasscannedatintervalsof10
m
mat70kVand 200
m
A. Three-dimensional images wereconstructed using VG Studio software (Volume Graphics, Heidelberg, Germany). Theimageswereevaluatedsemiquantitatively using a radiological union scale (Table 1) (Yagyuu et al., 2015).Furthermore,weevaluatedthenewbonevolume.Wemeasured an areaof calcification inthemandibularsymphysisasa high- densityarea,definedasadensityequaltoorgreaterthan220CT units,withintheregionofinterest(ROI).TosettheROI,wefirst establishedtheaxialplaneperpendiculartotheocclusalplaneof themolarteethandonthedistalside,2mmfartherthantheplane includingthelowestpointofthechin,i.e.,thementon.Inthisplane (transverseplane),wedefinedanROIasasquarearea1.0mmin height and 1.0mm in width positioned in the mandibular symphysis. The calcification area (mm2) was measured using ImageJsoftware(v.1.49;NIH,USA).
2.6.Histologicalanalysis
After micro-CTanalysis, mandibles from eachgroup of rats werefixedin 10%formaldehydeneutralbuffer solution,decal- cified(K-CX;FalmaInc.,Tokyo,Japan),embeddedinparaffin,and stained with H&Eand toluidine bluesolution. The histological sectionswereevaluatedusingahistologicalunionscale(Table1) (Yagyuu et al., 2015). Next, we performed histomorphometric analysis.WeestablishedanROIasasquarearea1.0mminheight and 1.0mm in width positioned between the left and right mandiblesinthehistologicalslideofthetransverseplane,andthe new bone formation area (mm2) was measured using ImageJ software.
2.7.Statisticalanalysis
Radiologicalandhistologicalunionscalescoresforthesamples were evaluated using Mann-Whitney U-tests. The statistical significance of differences in the calcification areadetermined bymicro-CTanalysisandnewboneformationareadeterminedby histomorphometricanalysisweredeterminedusing Student’st- tests.Differenceswithpvaluesoflessthan0.05wereconsidered significantforbothtests.
3.Results
3.1.InvitroevaluationofOMCSs
H&E-stained sections revealed that the OMCSs comprised several cell layers laminated along the sheet with abundant extracellular matrices (Fig. 2A). Immunohistochemical studies revealed that type I collagen was strongly expressed in the Fig.1.Implantationtechnique.(A)OMCSswereeasilydetachedfromtheculturedishusingascraper.(B)OMCSswerefoldedtoformalump,2-mmindiameter.(C)An incisionofabout10-mmwasmadeintheskinovertheinferiormarginofthemandible(circle).(D)Thefibroustissueoccupyingthemandibularsymphysiswascurettedto createspacefortheimplant.(E)OMCSswereimplantedintothemandibularsymphysis(arrow).
matricessecretedbytheculturedBMSCs(Fig.2B).Furthermore, OPNandOCNwereexpressedintheculturedcells(Fig.2CandD).
3.2.Comparisonofmicro-CTimages
Twoweeksafterimplantation ofOMCSs,themicro-CTscans exhibitedsparseareasofcalcificationwithinthebonegapatthe mandibular symphysis (Fig. 3A). At 4 weeks, calcification had spreadthroughoutthegapofthesymphysis,andaporouscalcified masshadformed,creatingcontinuousbonetissuebetweentheleft andrightsidesofthemandibles(Fig.3B).In5of10rats,theshape of the newly formed calcified mass resembled an OMCSlump implantedinthebonegap(Fig.3B,upperimages).At8weeks,the surface of the newly formed bone was smoother and more harmonizedwiththeparentbone(Fig.3C).Inthecontrolgroup8 weeksaftershamimplantation,allratsshowedirregularcortical bonethickeningandresorptionalongthebordersofthemandibles facingthemandibularsymphysis;noratsexhibitedboneunion (Fig.3D).
Next,wecomparedeachgroupbysemiquantitativeevaluation ofboneformation.Twoweeksafterimplantation,eightratsinthe experimentalgroupreceivedaradiologicalunionscoreof1,and theremainingtwo ratsreceived a scoreof 0.Four weeks after implantation, nine rats in the experimental group received a
radiologicalunionscoreof2,andtheremainingratreceivedascore of1.Eightweeksafterimplantation,sixratsintheexperimental groupreceivedaradiologicalunionscoreof3,andtheremaining fourratsreceivedascoreof2.Ontheotherhand,all10ratsinthe controlgroupat8weeksaftershamimplantationreceivedascore of 0.Thus,ratsin theexperimentalgroupat2,4, and8 weeks receivedsignificantlyhigherradiologicalunionscoresthandidrats in the control group at 8 weeks (p=0.002, p=0.0002, and p=0.0002,respectively,versusthecontrolgroup;Table2).
Inaddition,weevaluatedthevolumeofnewboneformation withintheROIinthemandibularsymphysis.Themeanvaluesof thenewboneformation areawere0.290.18mm2at2 weeks, 0.700.12mm2at4weeks,and0.930.06mm2at8weeksafter implantation of OMCSs,compared with0.080.05mm2 in the control groupat 8 weeks aftersham implantation. There were significantdifferencesbetweentimepointsin theexperimental group(p=7.3E-6for 2versus4weeks,p=5.4E-5for4 versus8 weeks;Fig.4A)
3.3.Comparisonofhistologicalanalyses
Histological analyses revealed that remnants of immature cellularosteoidsoccupiedthemandibularsymphysis2weeksafter implantationofOMCSs(Fig.5AandB).AlthoughtheCTimages Fig.2.invitroevaluationofOMCSs.(A)H&E-stainedsectionofOMCSsshowinganabundanceofcellsandextracellularmatrices.(B)StronglypositivestainingfortypeI collagenwasobservedintheextracellularmatrix.(C)Positivestainingforosteopontinwasobservedinthecytoplasmoftheculturedcells.(D)Positivestainingforosteocalcin wasobservedintheextracellularmatrix.
showed sparse areas of calcification within the bone gap, histological images demonstrated cartilaginous bone union betweentheleft and rightsides of themandibles.Four weeks afterimplantationofOMCSs,anastomosingwovenbonetrabecu- laehadformed,rimmedwithcuboidosteoblasts(Fig.5CandD).
Bone continuation between the left and right sides of the mandibles was observed. Eight weeks after implantation of OMCSs,calcificationhadadvancedfurther,andtheanastomosing, thickbonytrabeculaewerefirmlyattachedtotheadjacentparent bone(Fig.5E–G).Cracksandfissureswereobservedinthenewly formedbonebymicro-CTanalysis(Fig.5H,arrow;corresponding toascoreof2ontheradiologicalunionscale)andwerecausedby
cartilagetissueformation,asevidencedbyH&Eandtoluidineblue staining(Fig.5EandG).Additionally,thisstainingcorrespondedto anareaofcracksandfissuresinthenewboneontheCTimages.On the other hand, bone continuation was not observed in any mandiblesinthecontrolgroup(Fig.5I–L),andfibroustissuefilled themandibularbonegap.Similartotheresultsofsemiquantitative evaluationofmicro-CTanalyses,theexperimentalgroupat2,4, and8weeksreceivedsignificantlyhigherradiologicalunionscores thandidthecontrolgroupat8weeks(p=0.0002,p=0.0002,and p=0.0002,respectively,versusthecontrolgroup;Table2).
Inthehistomorphometricanalysis,themeannewboneforma- tionareaswere0.050.12mm2at2weeks,0.340.14mm2at4 Fig.3.Micro-CTanalysisaftersurgery.(A)Newboneformationwasobservedat2weeksintheexperimentalgroup.Theimagesshowedsparseareasofcalcificationinthe mandibularsymphysis.(B)Micro-CTscans4weeksafterimplantationshowedbonecontinuationbetweentheleftandrightsidesofthemandibleswithaporouscalcified mass.(C)Micro-CTscans8weeksafterimplantationshowedabundantboneformationoccupyingthemandibularsymphysis.Sixratsinthisgroupshowedcompletebone union.(D)Thecontrolgrouphadlittleboneformationinthemandibularsymphysis.
Table2
Resultsofradiologicalandhistologicalunionscales.
Score Radiologicalscale Histologiacalscale
Control 2weeks 4weeks 8weeks Control 2weeks 4weeks 8weeks
0 10 2 0 0 10 0 0 0
1 0 8 1 0 0 5 0 0
2 0 0 9 4 0 5 1 0
3 0 0 0 6 0 0 9 10
p=0.002* p=0.0002* p=0.0002* p=0.0002* p=0.0002* p=0.0002*
*vsControl.
Fig.4. Thevolumeofnewboneformation,asdeterminedbymicro-CTdataandhistomorphometricanalysis.(A)Trendinthemeanvolumeofnewboneformationinthe mandibularsymphysisat2,4,and8weeksafterimplantationofOMCSs,showinganincreaseinvolumeovertime.Theincreasewasonlyslightinthecontrolgroupat8weeks aftershamimplantation.(B)Thenewlyformedboneareainthemandibularsymphysisincreasedwithtimeinthehistomorphometricanalysis.Theerrorbarrepresentsone standarddeviation.
weeks, and 0.860.10mm2 at 8 weeks after implantation. In contrast,inthecontrolgroup,theareawasminimalat8weeksafter sham implantation. In the experimental group, the new bone formationareaincreasedovertime(Fig.4B).
4.Discussion
Cellsheettechnologyisatissueengineeringapproachthatdoes notrequirescaffolds(Matsuda,Shimizu,Yamato,&Okano,2007;
Matsuura,Utoh,Nagase,&Okano,2014).Confluentculturesofcells can be harvested as a cell sheet without protease treatment.
Avoidingprotease treatment preserves complete cell–celljunc- tions,cellsurfaceproteins,andtheextracellularmatrixinthecell sheet.Cellsheetsarealsosoft,malleable,andeasilymolded.Cell sheet technology has been applied clinically in ocular surface disease(Burillonetal.,2012),heartdisease(Sawaetal.,2012),and esophagealmucosaaftersurgery(Kobayashietal.,2014).Cellsheet implantationhasalsobeenperformedclinicallyfor bonerepair associated with artificial bones (Iwata et al., 2015; Kaushick, Jayakumar, Padmalatha, & Varghese, 2011; Okuda et al., 2009;
Yamamiyaetal.,2008).However,itisunclearwhethercellsheets canbeusedtorepairnaturalbonedefectswithoutscaffolds(Ma etal.,2011).Inthisstudy,wesoughttoexaminethetherapeutic potentialofOMCSsusedaloneforbonedefects.
OMCSs are prepared from BMSCs originating from the mesoderm. Although theefficacyof OMCSs for regeneration of long bones, whose origins are thesame as that of BMSCs,has previously been reported(Nakamura et al.,2010), it is unclear whetherOMCSscanbeappliedforrepairofmaxillofacialbones.
Thedevelopmentalcascadeandoriginsoflongbonesaredifferent fromthoseofmaxillofacialbones.Longbonesareofmesodermal originand aregenerated byendochondralossification, whereas maxillofacial bones are of neuroectodermal origin and are generated bymembranousossification. Therefore,in this study, weadoptedaratmandibularsymphysismodelandinvestigated whetherOMCSscouldrepairmaxillofacialbone.
Our current model made use of the mandibular symphysis (Yagyuuetal.,2015).Theratlowerjawdoesnothavecontinuous bone.Instead,fibroustissueispresentbetweentheleftandright sides of the mandibles in the mandibular symphysis. In other words,thesymphysiscanbeconsideredanaturalbonedefectthat neverheals.Thus,wesimplycurettedtheinterposedfibroustissue and implanted the OMCSs. Micro-CT and histological analyses demonstratedbonecontinuationbetweentheleftandrightsides of themandibles 4weeks afterOMCSimplantation, but not in shamimplantation,evenat8weeks.Thesedatademonstratedthe therapeuticpotentialofOMCSsaloneforrepairingbonedefects.
Moreover, OMCSs could be used in maxillofacial bones that originatefromtheneuroectoderm.
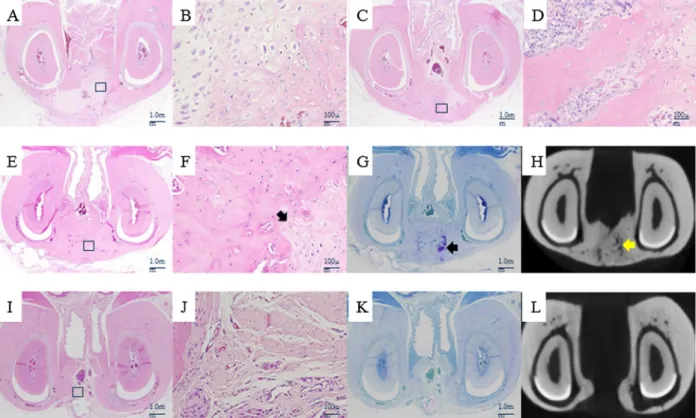
Fig.5.Representativehistologicalandradiologicalsectionsofthetransverseviewaftersurgery.(A)RepresentativeH&E-stainedsections2weeksafterimplantation, showingabundantfibrocartilagetissueinthemandibularsymphysis,whichformedacartilaginouscontinuationbetweentheleftandrightsidesofthemandibles.(B) Magnifiedviewof(A)showingimmaturecellularosteoids.(C)H&E-stainedsections4weeksafterimplantationshowingbonecontinuationbetweentheleftandrightsidesof themandibleswithwovenbonetrabeculae.(D)Magnifiedviewof(C)showingnewlyformedbonerimmedwithmanycuboidosteoblasts.(E)H&Estaininginthe experimentalgroupat8weeksafterimplantation,showingformedbonecontinuationbetweentheleftandrightsidesofthemandibles.(F)Magnifiedviewoftherectangular areain(E)showingthickbonytrabeculae.Theblackarrowindicatescartilagetissue.(G)Toluidinebluestainingintheexperimentalgroup,showingcartilagetissue(black arrow)inthenewlyformedbone.(H)Across-sectionalimageapproximatelycorrespondingtothehistologicalsectionsin(E)and(G)reconstructedfromthemicro-CTimage.
Cracksandfissures(yellowarrow)inthenewlyformedbone,appearingasbonedefects,weredeterminedtobecartilagetissuebyH&Estaining[blackarrowin(F)]and toluidinebluestaining[blackarrowin(G)].(I)H&Estaininginthecontrolgroupshowednobonecontinuationbetweentheleftandrightsidesofthemandibles.(J)Magnified viewoftherectangularareain(I)showingfibroustissuewithsmallvesselsandlittleinfiltrationofinflammatorycells.(K)Toluidinebluestainingofthecontrolgroupdidnot detectcartilagetissueinthemandibularsymphysis.(L)Cross-sectionalimageapproximatelycorrespondingtothehistologicalsectionsin(I)and(K),reconstructedfromthe micro-CTimage.Unlikeintheexperimentalgroup,bonecontinuationwasnotobserved.
Inthisstudy,weusedmicro-CTforradiologicalanalysis.Micro- CTis a usefuland reliablemethodforevaluatingbone healing.
Alternatively,histomorphometryisconsideredthegoldstandard forevaluatingbonehealingasitfacilitatesinsituanalysisofbone cellsaswellastheiractivities(Acaretal.,2015,2016).Ezirganlı, Polat, Barış, Tatar, and Çelik (2013) reported that there was a correlationbetweenmicro-CTandhistomorphometricanalysis.In this study, according to the results of both micro-CT and histomorphometry, new bone formation in the mandibular symphysis increased over time; both analyses yielded similar results.
Atime-seriesevaluationoftheimplantedOMCSsrevealedthat theOMCSsbecamebonetissue andthatthemorphologyofthe ossified OMCSs reflected local mechanical stress. That is, bone tissueformedfromOMCSscouldremodelitselfinaccordancewith Wolff’slaw(Wolff,1891).
Previously, we implanted cultured bone (rat BMSC-ceramic composites)intothepresentratmodel;boneunionbetweenthe left and right sides of the mandibles occurred following implantationoftheculturedbone(Yagyuuetal.,2015).Wealso performedaclinicaltrialinwhichweimplantedtheculturedbone into maxillofacial bone defects (approved by the Ministry of Health,LabourandWelfareofJapan,May28,2010).Tomanufac- turetheculturedbone,wefirstexpandedthenumberofBMSCs collectedfromtheiliaccrestofeachpatientandthenculturedthe cellswith
b
-tricalciumphosphate(TCP)granulesinosteoinductive mediumforgenerationofaBMSC–b
-TCPcompositeasculturedbone.Themanufacturingprocessfortheculturedbonerequired about6weeks.Aprocessthislongnotonlyincreasestheriskof contaminationorinfection,butalsosignificantlyincreasescosts.In thisregard,OMCSshaveadvantagesoverculturedboneandcanbe createdinamuchshortertimeperiod.TocreateOMCSs,BMSCsare simplyexpandedinosteoinductivemedium,anditisnotnecessary toculturecellsonartificialbone.Therefore,weestimatethatthe processcouldbeshortenedtoabout4weeks.
Additionally,usingOMCSs,thenumber ofcellsnecessaryfor implantation may be less than that required to manufacture culturedbone,althoughadirectcomparisonwasnotperformed.In ourprevious studywith cultured bone,1107 implanted cells wereneededforboneunioninthepresentratmodel(Yagyuuetal., 2015), whereas only 2105 cells were requiredtoachieve the sameresultsinthepresentstudy(datanotshown).Theseresults arelikelyduetothepropertiesofOMCSs,whichareharvestedwith many intact bone matrix components and cell–cell contacts (Akahaneetal.,2008;Nakamuraetal.,2010).Invitroevaluation of theOMCSs also revealedthat thecells were surroundedby abundantproteinmatrices containingtypeIcollagen,OPN,and OCN,whichmaypromoteosteogenesis.
AlthoughourdatademonstratedthatOMCSsmayhaveuseful and promising applications in bone regeneration, OMCSs have poor mechanical properties. Indeed, previous studies have recommended theuse of artificialbone along with OMCSs for this reason (Nakamura et al., 2010). However, we believe that OMCSscanbeusedforbonedefectswithlowmechanicalstress.
Maxillofacial bone defects occur in low stress-bearing bones comparedwiththoseinorthopedicsurgery.Moreover,maxillofa- cialbonedefectsaregenerallysmallerthanorthopedicdefects,but canhavemorecomplicatedshapes.Therefore,OMCSs,whichhave poormechanicalpropertiesbutgoodshapingproperties,maybe anoptimalgraftmaterialfor regenerationofmaxillofacialbone defects.FurtherstudiesareneededtodeterminewhetherOMCSs haveapplicationsintheclinicaltreatmentofmaxillofacialbone defects.
Inconclusion,weconfirmedtheefficacyofimplantingOMCSs aloneusingaratmandibularsymphysismodel.OMCSsmaybean
optimal graft material for regeneration of maxillofacial bone defects.
Funding
This work was partially supported by JSPS KAKENHI Grant NumberJP24792245.
Competinginterests
Noneoftheauthorshaveanyconflictsofinterestregardingthis research.
Ethicalapproval
Thisstudywasapprovedbytheanimalcareandusecommittee ofNaraMedicalUniversity(protocolNo.10483).
References
Acar,A.H.,Yolcu,Gül,M.,Keleş,A.,Erdem,N.F.,&AltundagKahraman,S.(2015).
Micro-computedtomographyandhistomorphometricanalysisoftheeffectsof platelet-richfibrinonboneregenerationintherabbitcalvarium.ArchivesofOral Biology,60,606–614.
Acar,A.H.,Yolcu,Altındiş,S.,Gül,M.,Alan,H.,&Malkoç,S.(2016).Bone regenerationbylow-levellasertherapyandlow-intensitypulsedultrasound therapyintherabbitcalvarium.ArchivesofOralBiology,61,60–65.
Akahane,M.,Nakamura,A.,Ohgushi,H.,Shigematsu,H.,Dohi,Y.,&Takakura,Y.
(2008).Osteogenicmatrixsheet-celltransplantationusingosteoblasticcell sheetresultedinboneformationwithoutscaffoldatanectopicsite-.Journalof TissueEngineeringandRegenerativeMedicine,2,196–201.
Behnia,H.,Khojasteh,A.,Soleimani,M.,Tehranchi,A.,Khoshzaban,A.,Keshel,S.H., etal.(2009)Secondaryrepairofalveolarcleftsusinghumanmesenchymalstem cells.108,e1–e6.
Burillon,C.,Huot,L.,Justin,V.,Nataf,S.,Chapuis,F.,Decullier,E.,etal.(2012).
Culturedautologousoralmucosalepithelialcellsheet(CAOMECS) transplantationforthetreatmentofcorneallimbalepithelialstemcell deficiency.InvestigativeOphthalmologyandVisualScience,13,1325–1331.
d’Aquino,R.,DeRosa,A.,Lanza,V.,Tirino,V.,Laino,L.,Graziano,A.,etal.(2009).
Humanmandiblebonedefectrepairbythegraftingofdentalpulpstem/
progenitorcellsandcollagenspongebiocomplexes.EuropeanCells&Materials, 12,75–83.
Ezirganlı,S.,Polat,S.,Barış,E.,Tatar,I.,&Çelik,H.H.(2013).Comparative investigationoftheeffectsofdifferentmaterialsusedwithatitaniumbarrieron newboneformation.ClinicalOralImplantsResearch,24,312–319.
Inagaki,Y.,Uematsu,K.,Akahane,M.,Morita,Y.,Ogawa,M.,Ueha,T.,etal.(2013).
Odontgenicmatrixcellsheettransplantationenhancesearlytendongraftto bonetunnelHealinginrabbits.BioMedResearchInternational.http://dx.doi.org/
10.1155/2013/842192,2013.
Iwata,T.,Washio,K.,Yoshida,T.,Ishikawa,I.,Ando,T.,Yamato,M.,etal.(2015).Cell sheetengineeringanditsapplicationforperiodontalregeneration.Journalof TissueEngineeringandRegenerativeMedicine,9,43–356.
Kaushick,B.T.,Javakumar,N.D.,Padmalatha,O.,&Varghese,S.(2011).Treatmentof humanperiodontalintrabonydefectswithhydroxyapatitebetatricalcium phosphatebonegraftaloneandincombinationwithplateletrichplasmaa randomizedclinicaltrial.IndianJournalofDentalResearch,22,505–510.
Kawate,K.,Yajima,H.,Ohgushi,H.,Kotobuki,N.,Sugimoto,K.,Ohmura,T.,etal.
(2006).Tissue-engineeredapproachforthetreatmentofsteroid-induced osteonecrosisofthefemoralhead:Transplantationofautologousmesenchymal stemcellscultureswithbeta-tricalciumphosphateceramicsandfree vascularizedfibula.ArtificialOrgans,30,960–962.
Kobayashi,S.,Kanai,N.,Ohki,T.,Takagi,R.,Yamaguchi,N.,Isomoto,H.,etal.(2014).
Preventionofesophagealstricturesafterendoscopicsubmucosaldissection.
WorldJournalofGastroenterology,7,15098–15109.
Liu,C.,Tan,X.,Luo,J.,Hu,M.,&Yue,W.(2014).Reconstructionofbeaglehemi- mandibulardefectswithallogenicmandibularscaffoldsandautologous mesenchymalstemcells.PUBLICLIBRARYOFSCIENCE,25,e105733.
Ma,D.,Yao,H.,Tian,W.,Chen,F.,Liu,Y.,Mao,T.,etal.(2011).Enhancingbone formationbytransplantationofascaffold-freetissueengineeredperiosteumin arabbitmodel.ClinicalOralImplantsResearch,22,1193–1199.
Matsuda,N.,Shimizu,T.,Yamato,M.,&Okano,T.(2007).Tissueengineeringbased oncellsheettechnology.AdvancedMaterials,19,3089–3099.
Matsuura,K.,Utoh,R.,Nagase,K.,&Okano,T.(2014).Cellsheetapproachfortissue engineeringandregenerativemedicine.JournalofControlledRelease.http://dx.
doi.org/10.1016/j.jconrel.2014.05.024.
Morishita,T.,Honoki,K.,Ohgushi,H.,Kotobuki,N.,Matsushima,A.,&Takakura,Y.
(2006).Tissueengineeringapproachtothetreatmentofbonetumors:Three casesofculturedbonegraftsderivedfrompatients'mesenchymalstemcells.
ArtificialOrgans,30,115–118.