はじめに
遺伝子解析法の発展とともに中枢神経先天奇形の画像 診断の臨床的意義はますます重要性を増している.しか し,形態発生がまったく異なる奇形であっても形態的特 徴が類似する奇形群があり,診断上混乱を招くことも少 なくない.本稿ではこのような紛らわしい中枢神経の奇 形群を取り上げ,特に胎児 MRI における鑑別診断のポイ ントを発生学的事項に基づいて概説する. 形態的特徴が類似する奇形群として,①脊椎の囊胞性 奇形(脊髄髄膜瘤と終末脊髄囊胞瘤),②後頭蓋窩囊胞性 奇形(Dandy Walker cyst/variant と Blake s pouch cyst), ③テント上正中囊胞性奇形(全前脳胞症と脳梁欠損を伴 う半球間裂囊胞)を取り上げる.腰仙部囊胞性奇形の鑑別診断
症例提示(Fig. 1,Fig. 2)腰仙部に囊胞を有する胎児 MRI をFig. 1とFig. 2に示 した.腰仙部囊胞の形態は類似しているが(Fig. 1A,Fig.
2A)おのおのの症例の頭蓋内構造は大きく異なってい る.すなわち,症例 1(Fig. 1)の後頭蓋窩は小さく,小 脳,脳幹周囲のくも膜下腔が狭小化し同定できない.ま た,第四脳室も狭小化し同定が困難である(Fig. 1B). 一方,Fig. 2に示す症例 2 の後頭蓋窩構造は正常である (Fig. 2B).後頭蓋窩形態から症例 1 は Chiari Ⅱ型奇形を 伴う腰仙部の囊胞であり一次神経胚の形成異常に起因す る脊髄髄膜瘤と診断することができる.一方,症例 2 は 二次神経胚の形成異常に起因する終末脊髄囊胞瘤と診断 1 連絡先:宇都宮英綱,〒 569 1192 高槻市古曽部町 1 3 13 高槻総合病院小児神経センター
Address reprint requests to:Hidetsuna Utsunomiya, M.D., Ph.D., Center for Pediatrlc Neurology, Takatsuki General Hospital, 1 3 13 Kosobe cho, Takatsuki shi, Osaka 569 1192, Japan
胎児期中枢神経奇形の MRI 診断
宇都宮 英綱
1),山崎 麻美
2)1)高槻総合病院小児神経センター,2)同 小児脳神経外科
MRI Diagnosis of the Central Nervous System Anomalies in the Fetus
Hidetsuna Utsunomiya, M.D, Ph.D.,1), Mami Yamasaki, M.D., Ph.D.2)
1)Center for Pediatric Neurology, Takatsuki General Hospital, 2)Department of Pediatric Neurosurgery, Takatsuki general Hospital
With recent advances in molecular genetics, MRI diagnosis of congenital CNS malformations has become more important. In this review, to promote more accurate MRI diagnoses, we present some anom-aly groups such as spinal cystic anomalies with or without Chiari II malformation, infratentorial midline cystic malformations(i.e. Dandy Walker cyst/variant vs. Blake s pouch cyst), and supratentorial dorsal cyst malformations(i.e. Callosal agenesis/hypogenesis with communicating interhemispheric cyst vs. holo-prosencephaly with dorsal sac), that have similar morphological features, and explain the morphogenetic differences in these anomalies based on embryologic considerations.
(Received November 16, 2015;accepted December 3, 2015) Key words:fetal MRI, central nervous system anomalies
Jpn J Neurosurg(Tokyo)25:338 345, 2016
することができる. Chiari Ⅱ型奇形と脊髄髄膜瘤(McLone の統一 仮説について) 脊髄髄膜瘤は一次神経胚(神経管)形成の過程で神経 外胚葉と表皮外胚葉の分離(disjunction)が障害され, 神経管の一部が欠損し体外に露呈した状態の脊髄奇形で ある(神経管欠損:neural tube defect)4).神経管(中心
管)は欠損部で体外に開放されており,胎児期には羊膜 腔と交通している.したがって,脊髄髄膜瘤があれば脳 脊髄液は欠損した神経管から羊膜腔に漏出する. 脊髄髄膜瘤には Chiari Ⅱ型奇形が併発することは古く から知られていたが,1989 年に McLone ら9)により, Chiari Ⅱ型奇形の発生は胎児期における脊髄髄膜瘤から の羊膜腔への髄液漏出に起因するとする統一仮説(uni-fied hypothesis)が発表された.この説によれば髄液漏出 により第四脳室が膨らまず後頭蓋窩が縮小した状態で留 まることに端を発し,くも膜下腔内髄液の減少によるテ ント上頭蓋の縮小,およびその状態下での大脳の成長が 後頭蓋窩構造(脳幹・小脳)を下方に偏位させ,Chiari 2
Fig. 1(case 1) Lumbosacral myelomeningocele with Chi-ari II malformation, 20weeks gestation A: Lumbosacral T2 weighted midsagittal image shows a cystic
mass within a streak shaped structure which suggests the neural placode(arrow).
B: Cranial T2 weighted midsagittal image shows a small and fun-nel shaped posterior fossa with an obliterated subarachnoid space and 4th ventricle.
A B
Fig. 2(case 2) Terminal myelocystocele, 28 weeks gestation
A: Lumbosacral T2 weighted midsagittal image shows a cystic mass within a streak shaped structure which suggests the neural placode(arrow).
B: Although, the spinal cystic lesion is similar to the myelomeningocele shown in Fig. 1A, cranial midsagit-tal T2 weighted image shows normal posterior fossa structures.
C: Sagittal T2 weighted image also shows a mass indicating cloacal exstrophy, which protrudes from the pelvic cavity(white arrows).
Ⅱ型奇形の原型が形成されるという.さらに脳幹(中脳) の変形(tectal beak)により中脳水道狭窄が生じ,内水頭 症が顕在化することで,後頭蓋窩構造の下方偏位が助長 され,Chiari Ⅱ型奇形の形態異常が完成する.この学説 の発表後,米国を中心に胎児期の脊髄髄膜瘤の閉鎖術が 行われるようになり,手術を受けた胎児には出生後の水 頭症や Chiari Ⅱ型奇形の発生頻度が減少するという事実 から,今日では,Chiari Ⅱ型奇形は神経管閉鎖不全(神 経管欠損)により二次的に形成される脳および頭蓋の形 態異常とする考え方が支持されるようになった5)13). Chiari Ⅱ型奇形の胎児診断 胎齢早期∼中期(第 1∼2 三半期間)の Chiari Ⅱ型奇 形の MRI 診断は,矢状断で後頭蓋窩が小さく漏斗状を呈 し,脳幹と小脳は下方に偏位する.また,第四脳室はほ とんど同定できないほど狭小化している(Fig. 1).同時 に第三脳室の狭小化と中脳水道の閉塞化が生じるため, 側脳室は拡張し,胎児期水頭症をきたす.胎児期水頭症 の診断の目安は側脳室の三角部幅(atrial width:AW)が 10 mmを超えているかどうかで判断する(Fig. 3A)1)2). ちなみに胎児の AW は全胎齢をとおして原則 10 mm を超 えることはない.加えて,テント上のくも膜下腔も狭小 化するため,前頭部の頭蓋が陥凹し,軸位断で頭蓋がレ モン型を呈するのも特徴である(Fig. 3B)11). 一方,胎齢後期(第 3 三半期間)になると水頭症が進 行し,脳幹,小脳の圧迫と下方偏位により,medullary kinkなどの定型的 Chiari Ⅱ型奇形の所見が認められるよ うになる. 終末脊髄囊胞瘤(terminal myelocystocele)の 発生と胎児診断 終末脊髄囊胞瘤は神経管欠損とは異なり,神経管閉鎖 が完了したのちに神経管の尾側に発生してくる caudal cell massの分化異常によって生じる二次神経胚の形成異 常である4)8).二次神経胚の形成は表皮外胚葉と神経外 胚葉の分離(disjunction)が終了した後に起こるため, 囊胞はまったく健常な表皮で覆われている.したがっ て,髄液の漏出が生じることはなく Chiari Ⅱ型奇形が発 生することもない(Fig. 2).なお,caudal cell mass は総 排泄腔の形成にも関与するため,終末脊髄囊胞瘤には総 排泄腔外反(extrophy of cloaca)を伴うことがある.そ の他,臍ヘルニア(omphalocele),鎖肛(imperfect anus), 仙骨形成不全(spinal anomaly)を合併することがあり, OEIS連合とよばれる6).これらの奇形を把握することは 正確な診断につながるので重要である.
後頭蓋窩囊胞性奇形の鑑別診断
症例提示(Fig. 4∼6) 形態発生の異なる 3 例の代表的後頭蓋窩正中囊胞性奇 形の胎児 MRI 正中矢状断像をFig. 4∼6に示した.症例 3(Fig. 4)は第四脳室室頂(fastigium)の形成がなく尾 側小脳虫部の形成不全が明瞭な囊胞で Dandy Walker 奇 形と診断される.一方,症例 4(Fig. 5)と症例 5(Fig. 6)は fastigium が形成されていることから,小脳虫部形 成不全のない囊胞で Dandy Walker 奇形からは除外され る.症例 4 は Magendie 孔が拡張し小脳虫部が囊胞によ り上方に回旋しており,Blake s pouch cyst と診断され,症例 5(Fig. 6)は正常に形成された小脳が前方に圧排さ れており,小脳背側くも膜囊胞(retrocerebellar arachnoid cyst)と診断される. 小脳の発生と菱脳蓋板の変化 小脳は菱脳第一分節(rhombomere 1)から発生し,第 四脳室は菱脳蓋板の変化により形成されるが,最近で は,rhombomere 1 の両外側部の菱脳唇(rhombic lip)か ら小脳半球が発生し,中央の小脳虫部は中脳・後脳境界 すなわち菱脳峡(rombencephalic isthmus)から派生する と考えられている7). 3 4 1 2 Fig. 3 Fetal MR imaging of Chiari II
malforma-tion:same case as shown in Fig. 1
Axial T2 weighted image at the slice of the trigone of the lateral ventricle(A)shows a ventricular dilatation of 13 mm atrial width(AW). Since the atrial width is less than 11 mm throughout gestation, this ventriculomegaly indicates fetal hydrocephalus. A slice just upper level of A shows the tightening of the subarachnoid space with depressed frontal bones(arrows), which is the so called ‘lemon shaped cranial deformity’, that results in reduced
cerebrospinal fluid volume in the supratentorial subarach-noid space(B).
AW=13mm AW=13mm
A
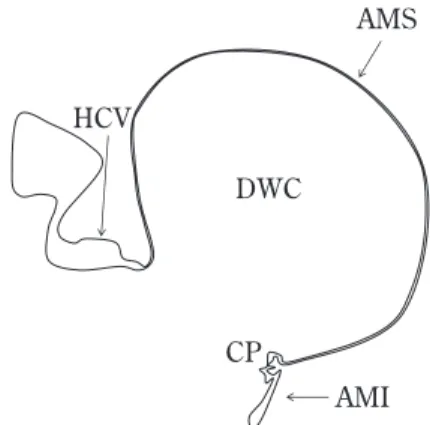
菱脳蓋板は中央に横走する脈絡雛壁(plica choroidea) により,頭側の上膜性部(area membranacea superior: AMS)と尾側の下膜性部(area membranacea inferior: AMI)に分けられる.小脳の発達により AMS は退化し消 失するが,AMI は残存し第四脳室脈絡組織になる.AMI には発生初期に Blake s pouch とよばれる一過性の囊胞 状の膨らみが生じるが,やがて apoptosis により消失し Magendie孔となる(Fig. 7)3). 囊胞の形態発生 Dandy Walker 奇形は小脳虫部の発生に何らかの障害 が生じた結果,本来ならば消失するべき AMS が残存し, 囊胞状に拡張した奇形と考えられており,囊胞状に拡張 した AMS は Dandy Walker Cyst とよばれる(Fig. 8)12)15).
したがって,Dandy Walker 奇形の診断は小脳虫部の形成 不全を同定することが基本となる.一方,Blake s pouch cystは 第 四 脳 室 と 交 通 す る 囊 胞 腔 で あ る こ と で は
Dandy Walker Cystと共通しているが,小脳虫部は正常
に形成される.この囊胞は,Magendie 孔が開口しないか 開口の遅れが生じ,Blake s pouch すなわち AMI が囊胞状 に拡張したものと考えられており,時に第四脳室脈絡叢 が囊胞の上壁に沿って囊胞内に伸長することがある (Fig. 9)10).
くも膜囊胞はくも膜由来の囊胞腔であり,菱脳蓋板の 一部が囊胞状に拡張した Dandy Walker cyst や Blake s
pouch cystとは発生起源が根本的に異なる.すなわち,
神経軸の発生には異常はないため,小脳の形成異常は認 められず,第四脳室は小脳とともに前方に圧排されるの みである.囊胞が大きい場合は,小脳テントの沈下が障 害され,Dandy Walker Cyst でみられるような,静脈洞 交会や直静脈洞の高位を認めることがあるので注意が必 要である(Fig. 6)15).
3
Fig. 4(Case 3) Dandy Walker malformation;32 weeks gestation
Midsagittal T2 weighted image shows no formation of the fastigium of the 4th ventricle, which indicates that the inferior vermis is defective. A markedly hypo-plastic superior vermis(SV)is presented(arrow). The Dandy Walker cyst(DWC), which characterizes expansion of the primitive fourth ventricular roof due to persistence of the area membranacea superior (AMS).
DWC AMS
SV
Fig. 5(Case 4) Blake s pouch cyst;33 weeks gestation
Midsagittal T2 weigted image shows formation of the fastigium of the 4th ventricle(F), which indicates that the cerebellar vermis is completely formed. The foramen of Magendie is widely open and continues to the Blake s pouch cyst(BPC), which is defined as per-sistent and cystic evagination of the area membranacea inferior, beneath the inferior vermis.
F
BPC
Fig. 6(Case 5) Arachnoid cyst;33 weeks gesta-tion
Midsagittal T2 weighted image shows formation of the fastigium of the 4th ventricle(F), which indicates that the cerebellar vermis is completely formed. The cerebellar vermis is displaced anteriorly by the expanded arachnoid cyst(AC). The torcular herophili (T)and the straight sinus(SS)are located in a high
position, since the fusion of the tentorial membrane occurs in a high position due to the upward pressure of the cyst.
F
AC
T SS
テント上正中囊胞性奇形の鑑別診断
症例提示(Fig. 10,Fig. 11)形態発生の異なるテント上正中囊胞性奇形(背側囊 胞:dorsal cyst17))の 2 例をFig. 10とFig. 11に示した.
症例 6(Fig. 10)は全前脳胞症にみられる dorsal cyst で 1
Fig. 8 Schematic drawing of the Dandy Walker cyst
The Dandy Walker cyst(DWC)is characterized by expansion of the primitive fourth ventricular roof due to persistence of the area membranacea superior (AMS). Since persistence of the AMS may result from
incomplete formation of the cerebellar vermis, DWC always presents an absent or markedly hypoplastic vermis(HCV).
AMI:area membranacea inferior, CP:choroid plexus DWC AMS AMI CP HCV
Fig. 9 Schematic drawing of the Blake s pouch cyst
The Blake s pouch cyst(BPC)is defined as persistent and cystic evagi-nation of the are a membranacea infe-rior(AMI). In contrast to DWC, the cerebellar vermis(CV)is formed normally and the choroid plexus(CP) elongates along the superior cyst wall in some cases.
BPC AMI
CP CV Fig. 7 Schematic drawing of rhombencephalic
roof plate differentiation(modified by ref-erence No. 10)
After pontine flexure, the rhombencephalic roof plate(RRP)is divided into a rostral part(area mem-branacea superior:AMS)and a caudal part(area membranacea inferior:AMI)with the formation of a transverse vascular fold(plica choroidea), which invaginates into the lumen of the fourth ventricle and constitutes a choroid plexus(CP). With continued development of the cerebellum, the AMS disappears with the formation of the cerebellar vermis and the choroid plexus becomes attached to the caudal edge of the cerebellum.
Subsequently, the cerebellar vermis(CV)bends in the middle portion and forms the fastigium(F), which divides the vermis into a rostral part(superior lary vellum:SMM)and a caudal part(inferior medul-lary vellum:IMM).
On the other hand, the AMI, which consists of an ependymal membrane initially expands and forms a small diverticulum(Blake s pouch), which eventually disappears, leaving a median aperture that becomes the foramen of Magendie(FM). F Isthmus RRP AMS AMI CP CP AMI F FM Blake s pouch SMV IMV CV CV CV
翻転が障害された間脳蓋板,すなわち dorsal sac mem-braneが囊胞状に拡張した状態である.一方,症例 7(Fig. 11)は脳梁欠損症に伴った交通性半球間裂囊胞とよばれ るもので,第三脳室天蓋もしくは側脳室が憩室状に拡張 したものと考えられている(Table 1).両者の鑑別には大 脳が全球脳(holospheric brain)であるのか,半球脳 (hemispheric brain)であるのかを診断することが重要で ある15). 全球脳(holospheric brain)と半球脳(hemi-spheric brain)の形態発生 前脳は胎生 5 週ごろに頭尾方向に終脳と間脳に分離 し,同時に終脳には左右にそれぞれ新皮質の原基が発生 し,これが成長して左右の半球が形成される.一方,前 脳の腹側誘導が障害されると新皮質の原基が左右分離す ることなく発生するため,本来なら大脳半球間裂によっ て境界され連続性のない大脳新皮質が正中を超えてつな がる特徴的な大脳形態を示す(Fig. 10).これが全球 2
Fig. 11(case 7) Communicating interhemispheric cyst with callosal agenesis, 32 weeks gestation T2 weighted axial(A)and coronal(B)images show a huge interhemispheric cyst(IHC), which is communicated with the 3rd or left lateral ventricle. The agenesis of the corpus callosum is also shown. Since the interhemispheric fissure is completely formed (white arrow in A), this is a hemispheric brain. The left medial
cerebral mantle is displaced laterally by the interhemispheric cyst (arrow in B).
IHC
IHC
A B
Fig. 10(case 6) Alobar holoprosencephaly, 33 weeks ges-tation
A: T2 weighted axial image shows the midline continuity of the cerebral cortex(arrows). There is no interhemispheric fis-sure.
B: T2 weigted sagittal image shows the dorsal cyst(DC), which communicated with the prosencephalic ventricle(v).
DC v
(holosphere)とよばれる全前脳胞症に共通する特徴的終 脳形態である.すなわち,半球脳では左右に一対形成さ れる新皮質が成長し,それぞれに脳回,脳溝が形成され, これらは大脳半球間裂で分離されて決して正中を超えて 連続することはないのに対して(Fig. 11),全球脳では新 皮質の不対化があるために,脳回,脳溝は正中を超えて 連続する.この所見が全前脳胞症診断の決め手とな る14)∼17).
まとめ
形態発生は異なるが,MRI 所見が類似する代表的中枢 神経奇形を取り上げ,それぞれの胎児 MRI 診断の概要お よび鑑別診断のポイントについて述べた. 今後,さらに症例の蓄積を行うとともに,病理や遺伝 子診断との対比を積み重ねることで,中枢神経奇形にお けるより正確な胎児 MRI 診断法が確立されていくこと を期待したい. 著者および共著者は本論文に関して開示すべき COI はあり ません.なお,共著者(山崎麻美)は日本脳神経外科学会へ の COI 自己申告を完了しています. 文 献1) Alagappan R, Browning PD, Laorr A, McGahan JP:Distal lateral ventricular atrium:reevaluation of normal range.
Radiology 193:405 408, 1994.
2) Almog B, Gamzu R, Achiron R, Fainaru O, Zalel Y:Fetal lateral ventricular width:what should be its upper limit? A prospective cohort study and reanalysis of the current and previous data. J Ultrasound Med 22:39 43, 2003. 3) Blake JA:The roof and lateral recesses of the forth
ventri-cle, considered morphologically and embryologically. J Comp
Neurol 10:79 108, 1900.
4) Dias MS, Walker ML:The embryogenesis of complex dys-raphic malformations:a disorder of gastrulation? Pediatr
Neurosurg 18:229 253, 1992.
5) Grant RA, Heuer GG, Carrión GM, Adzick NS, Schwartz ES, Stein SC, Storm PB, Sutton LN:Morphometric analysis of posterior fossa after in utero myelomeningocele repair. J
Neurosurg Pediatr 7:362 368, 2011.
6) James HE, Lubinsky G:Terminal myelocystocele. J
Neurosurg 103(5 Suppl):443 445, 2005.
7) Louvi A, Alexandre P, Métin C, Wurst W, Wassef M:The isthmic neuroepithelium is essential for cerebellar midline fusion. Development 130:5319 5330, 2003.
8) McLone DG, Naidich TP:Terminal myelocystocele.
Neurosurgery 16:36 43, 1985.
9) McLone DG, Knepper PA:The cause of Chiari II malforma-tion:a unified theory. Pediatr Neurosci 15:1 12, 1989. 10) Nelson MD Jr, Maher K, Gilles FH:A different approach to
cysts of the posterior fossa. Pediatr Radiol 34:720 732, 2004.
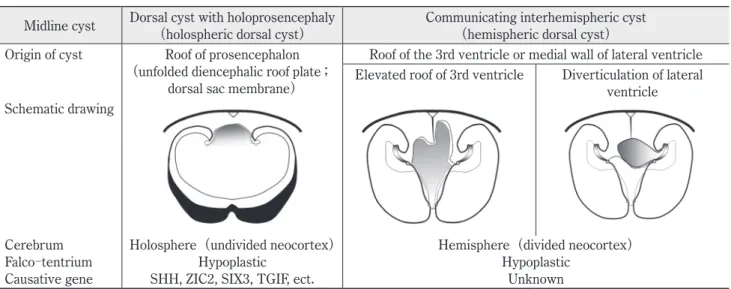
Table 1 Morphologic difference between a dorsal cyst with holoprosencephaly(holospheric dorsal cyst)and a communicating interhemispheric cyst(hemispheric dorsal cyst)
Midline cyst Dorsal cyst with holoprosencephaly(holospheric dorsal cyst) Communicating interhemispheric cyst(hemispheric dorsal cyst) Origin of cyst Roof of prosencephalon
(unfolded diencephalic roof plate; dorsal sac membrane)
Roof of the 3rd ventricle or medial wall of lateral ventricle Elevated roof of 3rd ventricle Diverticulation of lateral
ventricle Schematic drawing
Cerebrum Holosphere(undivided neocortex) Hemisphere(divided neocortex)
Falco tentrium Hypoplastic Hypoplastic
Causative gene SHH, ZIC2, SIX3, TGIF, ect. Unknown
The term“dorsal cyst”is used to refer to both cystic expansion of the dorsal sac membrane, which represents the unfolded diencephalic roof plate and covers the dorso caudal aspect of the prosencephalic ventricle of holoprosencephaly(holospheric dorsal cyst)and an elevated but folded diencephalic roof plate or diverticulation of the medial wall of the lateral ventricle (hemispheric dorsal cyst). Indeed, a hemispheric dorsal cyst is a communicating interhemispheric cyst with callosal agene-sis. In fact, while a holospheric dorsal cyst in holoprosencephaly represents primary failure of unfolded diencephalic roof plate invasion, a hemispheric dorsal cyst represents a failure of folded diencephalic roof plate inversion or cystic dilatation of the telencephalic ventricle secondary to intraluminal pressure in the prosencephalic ventricles after the completion of hemi-spheric cleavage of the telencephalic vesicle.
「読者の意見(Letters to the Editor)」原稿募集のお知らせ 本誌では「読者の意見(Letters to the Editor)」欄
を設けています.読者交流の場として意見交換にご利用 いただきたく,下記の要領で編集室宛に原稿をお寄せく ださい. 趣 旨: ①掲載論文に対する意見,②編集方針に対す る意見,希望などを掲載いたします.①に関 しては著者側からのコメントも掲載いたしま す. 執筆内容: ①本文は図表も含め 1,200 字以内(文献は 3 個以内,写真・図・表は 1 個以内とし,その 数に応じて本文を減じてください),②筆者 名,所属を明記,③著者側からのコメントは 600 字以内. 採 否: 編集委員会で決定いたします.不採用の場合 は速やかに連絡いたしますが,理由はお知ら せいたしません.また,採否のいかんにかか わらず,原稿は返却いたしません. そ の 他: 論文掲載後 3 カ月以内に意見をお寄せくださ い.文章は書簡の形式(口語体)としてくだ さい.採用の場合は掲載誌 1 部をお送りいた します. 「脳神経外科ジャーナル」編集委員会
11) Nicolaides KH, Campbell S, Gabbe SG, Guidetti R:Ultra-sound screening for spina bifida:cranial and cerebellar signs. Lancet 2:72 74, 1986.
12) Raybaud C:Cystic malformations of the posterior fossa. Abnormalities associated with the development of the roof of the fourth ventricle and adjacent meningeal structures.
J Neuroradiol 9:103 133, 1982.[Article in English, French]
13) Tulipan N, Sutton LN, Bruner JP, Cohen BM, Johnson M, Adzick NS:The effect of intrauterine myelomeningocele repair on the incidence of shunt dependent hydrocephalus.
Pediatr Neurosurg 38:27 33, 2003.
14) 宇都宮英綱:全前脳胞症における全球脳の形態発生と MRI所見.脳外誌 13:454 464,2004.
15) Utsunomiya H, Yamashita S, Takano K, Ueda Y, Fujii A: Midline cystic malformations of the brain:imaging diagno-sis and classification based on embryologic analydiagno-sis. Radiat
Med 24:471 481, 2006.
16) Yakovlev PI:Telencephalon“impar”,“semipar”and“totopar”. (morphogenetic, tectogenetic and architectonic definitions).
Int J Neurol 6:245 265, 1968.
17) Yokota A, Oota T, Matsukado Y:Dorsal cyst malformation. Part I. Clinical study and critical review on definition of holoprosencephaly. Child s Brain 11:320 341, 1984.
胎児期中枢神経奇形の MRI 診断 宇都宮英綱 山崎 麻美 遺伝子解析法の発展とともに中枢神経先天奇形の画像診断の臨床的意義はますます重要性を増し ている.一方で,今日の MRI の進歩は胎児期からの中枢神経の形成過程や,その異常をある程度正確 に把握することを可能にした.本稿では胎児期に診断できる代表的中枢神経奇形の中で,形態発生が まったく異なるにもかかわらず,MRI 所見が類似する奇形を取り上げ,その診断および鑑別診断のポ イントを発生学的知見に基づいて概説する. 脳外誌 25:338⊖345,2016 要 旨