Development of an EMG+IMU Driven Musculoskeletal Model and its Applications in
Medical Training Assessment
➽㟁ሗጼໃሗࡶ࡙ࡃ➽άື᥎ᐃ
ࣔࢹࣝࡢ㛤Ⓨࡑࡢ་⒪ᡭᢏホ౯ࡢᛂ⏝
July 2013
Luca BARTOLOMEO
ࣂࣝࢺ࣓ࣟ࢜ ࣝ࢝
Development of an EMG+IMU Driven Musculoskeletal Model and its Applications in
Medical Training Assessment
➽㟁ሗጼໃሗࡶ࡙ࡃ➽άື᥎ᐃ
ࣔࢹࣝࡢ㛤Ⓨࡑࡢ་⒪ᡭᢏホ౯ࡢᛂ⏝
July 2013
Waseda University
Graduate School of Advanced Science and Engineering Major in Integrative Bioscience and Biomedical
Engineering, Research on Biorobotics
Luca BARTOLOMEO
ࣂࣝࢺ࣓ࣟ࢜ ࣝ࢝
Alla mia cara Nonna
ACKNOWLEDGMENTS
Studying and working full time is an epic mission, hardly possible without the support of other people. During the past four years, I have had the pleasure to study in Japan, while working in STMicroelectronics as an Application Engineer, surrounded by many enthusiastic colleagues and friends, who helped me in managing my time and in succeeding in my research. Here, I would like to express my gratitude to all of you who were involved in my study and life, and who made me a better researcher and especially a better person.
First of all, I would like to gratefully thank my supervisor Prof. Atsuo Takanishi for his confidence in my ability to complete the PhD course. He motivated me during many tough periods; his bright guidance and warm encouragements, together with his positive atmosphere, made my experience in his laboratory outstanding.
My distinct gratitude goes to Prof. Massimiliano Zecca for his guidance, patience, and friendship. He has been always next to me, giving me the right pressure to write papers and complete the research. He has been my mentor, encouraging me to grow not only as an engineer but also as a methodical thinker, with continuous and precious advices.
During the period under which this research was completed, the advice and guidance from Dr. Salvatore Sessa, Dr. Hiroyuki Ishii, Dr. Yohan Noh and Dr. Zhuohua Lin were of paramount importance to overcome technical and logistic issues. I would like to sincerely thank them for their on-going support. I would also like to express my gratitude to Mrs. Sarah Cosentino and Mr. Usama Imtiaz for their kind supports in the experiments setup and hardware development.
A particular thankfulness goes to Mrs Hisako Ohta for helping me solve a lot of problems on regular university affairs, which made me be capable of concentrating on my research.
I would like to express my deepest gratitude to Prof. Hiroshi Fujimoto, Prof. Mitsuo Umezu and Prof. Masakatsu G. Fujie who gave me a lot of advices on how to complete my thesis and provided corrections of my dissertation.
It is my sincere pleasure to acknowledge the Department of Advanced Medical Initiatives at Kyushu University, especially Prof. Makoto Hashizume, Prof. Morimasa Tomikawa, and other colleagues who supporting me with valuable discussions of laparoscopic training and experiment organization.
I would like to thank gratefully Dr. Yusuke Kasuya and Dr. Mirei Nagai at Tokyo Women’s Medical University, for the medical knowledge support in endotracheal intubation and the organization of experiments in ETI training.
It is very difficult to find fearless volunteers that allow you to measure and assess their skills. Most of the measurements in this research had been performed in Kyushu University, Tokyo Women’s Medical University and Waseda University. Therefore, I would like to thank all the surgeons, medical students, and engineering students for participating in my studies.
This work has been also supported in part by Global COE Program "Global Robot Academia", MEXT, Japan; and by a grant from STMicroelectronics. I would also like to express my gratitude to RoboCasa, Okino Industries LTD, Japan ROBOTECH LTD, SolidWorks Corp, Dyden Corp, and the Humanoid Robotics Institute for their supports to the research.
In particular, I would like to thank my dear friend Dr. Hisako Niko, who supported me during these years, with advices, corrections and undisputable professionalism.
Finally, I would like to thank my family. The support and encouragement of my mother and my grandmother have been fundamental to complete this experience. The love and patience of my wife Chizuko have contributed every single day to the accomplishment of this work, on top of her huge effort to take care our beloved son Leon, born during the second year of my PhD.
ABSTRACT
The main objective of medical education is to guarantee that the graduating physicians are competent to practice in their selected field and that the preparation among them is independent of the medical school. An unbalance of preparation among medical doctor of different hospitals is translated directly into a difference of treatment for the patients.
In order to increase the homogeneity among the medical schools, many countries are recently adopting a competency-based training, in which the residents are evaluated on their acquired skills, eliminating the concept of years-in-training. Each trainee has the autonomy to proceed based on his or her capability, with some intermediate steps to provide evidence of the mastery of what is required. The evaluation of competency is assured by skilled impartial observers, judging who performs a procedure adequately and who does not. However, there is a high risk of the assessors subjectively interpreting the results, with the outcome depending on background, skill, and experience of the assessors. This makes the evaluation highly variable from place to place, and from assessor to assessor. Additionally, it is difficult to secure the time of senior surgeons, because they are extremely busy for their own work and not all facilities can count on such skilled personnel. The increased complexity of modern medical technologies and equipment has made the assessment even more problematic.
Definitely, without an objective evaluation of competency to practice, the homogeneity of preparation cannot be guaranteed.
Training devices, such as box trainers and virtual reality simulators, have already been developed to learn fundamental operative skills outside the operation room and to measure the performance during the training. However, the science of objective evaluation of operative performance is still in its early stages. Currently, the objective skill evaluation systems on
1) In the cases of virtual reality or dedicated simulators, they provide only low-level skill scoring by using the execution time and instrument’s motion information for completing the training tasks; additionally they cannot be extended to other medical training systems.
2) Existing general objective skill evaluation methods use only motion analysis or only muscle force analysis, missing one of the two information. To date, there is no common methodology capable of integrating motion analysis and muscle force estimation to achieve objective skill evaluation in medical applications.
In this thesis, the road towards the realization of a common objective skill evaluation system for multiple medical applications is presented. The specific goal of this work is to develop a new integrated biomechanical model for the objective assessment of medical skills, and to provide it to the assessors for an objective and exhaustive evaluation and coaching of the trainees. More specifically, the proposed system aims at answering the questions: how to discover and analyze objectively the trainees’ weak points, and how to overcome them in the best possible way. The advantage is that virtually all the surgeons in all the hospitals in the world can have the same high level of training/evaluation as the top ones, with an evident benefit for the patients all around the world.
In this work the aims are achieved by:
1) developing a common skill evaluation system, which is independent from the training devices and can be adaptive for various medical training scenarios;
2) combining human motion tracking system and surface electromyography in an EMG- driven musculoskeletal model suitable for analyzing the biomechanics of trainee’s upper body during practical medical training;
3) verifying that the proposed skill evaluation system can be implemented in multiple medical applications for evaluating the surgical operative skills and assisting clinical practice.
At the end, this research demonstrates a general methodology for objectively evaluating medical operative skills. The model can be used not only for regular operative skill trainings, but can be also further implemented for clinical practice and other medical scenarios.
The validity of the resulting skill evaluation system is verified in the field of laparoscopy and endotracheal intubation, covering applications in both Operating Room and Emergency Room. The evaluation for surgery is based on the assumption that expert surgeons have better operative skills than novices. Additionally, a chapter is dedicated on the evaluation of the mental stress using biomechanical information, based on the hypothesis that induced mental stress can affect the learning curve of trainees. The performance evaluation for the intubation is analyzed with different laryngoscopes and physicians, given the hypothesis that modern video-laryngoscopes help in improving the performance of the practice. The results are extremely promising, and show that the skill dexterity and competence could be effectively assessed by using the developed systems.
TABLE OF CONTENTS
11 Introduction... 1
1.1 Background ... 1
1.1.1 Competency-based Training in Medical Practices ... 1
1.1.2 Modern Technologies for Surgical Operation: Laparoscopy ... 3
1.1.3 Modern Technologies for Endotracheal Intubation (ETI) ... 5
1.1.4 Training for Operating Modern Medical Technologies ... 8
1.1.5 Assessment of Medical Practices: Limitations and Challenges ... 11
1.2 Biomechanical Analysis for Operative Skill Evaluation ... 12
1.2.1 Motion Analysis as Assessment tool ... 12
1.2.2 Electromyography as Assessment tool ... 16
1.3 Problem Statement ... 17
1.4 Goal of this Thesis ... 18
1.4.1 Aims ... 18
1.4.2 Innovation ... 19
1.4.3 Contribution of this Research ... 19
1.5 Methodology ... 20
1.5.1 Objective Assessment Methodology: Previous Research ... 20
1.5.2 Proposed Objective Assessment Methodology ... 21
1.5.3 Protection of Human Rights ... 21
1.6 Thesis Outline ... 22
2 Motion Analysis: Inertial Measurement Unit WB-4R ... 25
2.1 Introduction ... 25
2.2 Inertial Measurement Unit WB-4R ... 27
2.3 Online Magnetic Calibration ... 31
2.6.1 WB-4R Hardware and Online Calibration Algorithm ... 42
2.6.2 Future work ... 43
2.7 Conclusion of this Chapter ... 43
Part I. Development of Biomechanical Model 3 Analysis of Muscle Activation: Surface Electromyography ... 45
3.1 Introduction ... 45
3.2 Wireless surface Electromyography Sensor ... 47
3.2.1 Design of the Wireless sEMG sensor ... 47
3.2.2 Characterization of the Wireless sEMG sensor: test signal ... 52
3.2.3 Characterization of the Wireless sEMG sensor: practical experiment ... 53
3.3 Denoising of Electromyographical Signal ... 55
3.3.1 Wavelet Denoising Algorithm ... 55
3.3.2 Thresholding ... 56
3.3.3 Baseline Adaptive Technique ... 59
3.3.4 Evaluation Method ... 60
3.3.5 Task and Protocol ... 61
3.3.6 Evaluation Indexes ... 62
3.3.7 Comparison with Standard Denoising Techniques... 63
3.4 Discussion ... 70
3.4.1 WB-EMG Development ... 70
3.4.2 WB-EMG: Future work ... 70
3.4.3 Denoising Algorithm ... 71
3.4 Conclusion of this Chapter ... 71
4 Integration of WB-4R and surface Electromyography: Biomechanical Model ... 73
4.1 Introduction ... 73
4.2 Materials and Methods ... 74
4.2.1 sEMG setup and analysis ... 74
4.2.2 IMU setup and analysis ... 75
4.2.3 Experiment protocol ... 76
4.3 Muscolotendon Model ... 76
4.3.1 Model Description ... 76
4.3.2 Muscle Activation Dynamics ... 78
4.3.3 Force-Length and Force-Velocity relationships ... 79
4.3.4 Estimation of LM(ȟ,t) ... 81
4.3.5 Estimation of torque and calibration ... 82
4.4 Results ... 83
4.5 Discussion ... 84
4.5.1 Biomechanical Model ... 84
4.5.2 Future work ... 85
4.6 Conclusion of this Chapter ... 86
P Part II. Applications 5 Evaluation of Laparoscopy Operative Skills ... 87
5.1 Introduction ... 87
5.2 Materials and Methods ... 89
5.2.1 Surface Electromyography hardware and setup ... 89
5.2.2 Inertial Measurement Unit hardware and setup ... 90
5.2.3 Preparation ... 90
5.3 Laparoscopic Training ... 91
5.3.1 Peg Board ... 91
5.3.2 Pipe Cleaner ... 93
5.3.3 Circle ... 94
5.3.4 Ligation ... 95
5.3.5 Needle Insertion ... 96
5.3.6 Waseda Kyotokagaku Suture-No.2RII ... 96
5.3.7. VR Suturing ... 97
5.3.8. In-vivo Suturing ... 98
5.4 Results ... 99
5.5 Discussion ... 102
5.5.1 Laparoscopy Training Evaluation ... 102
5.5.2 Future work ... 102
5.6 Conclusion of this Chapter ... 103
6 Evaluation of Induced Mental Stress ... 105
6.1 Introduction ... 105
6.2.3 Preparation ... 107
6.2.4 Task and Mental Stress Induced Protocol ... 108
6.2.5. sEMG Data Analysis ... 110
6.2.6 WB-4R Data Analysis ... 112
6.3 Results ... 112
6.4 Discussion ... 117
6.4.1 Mental Stress Analysis in laparoscopic training ... 117
6.4.2 Future work ... 117
6.5 Conclusion of this Chapter ... 118
77 Evaluation of Endotracheal Intubation Skills ... 119
7.1 Introduction ... 119
7.2 Materials and Methods ... 121
7.2.1 Sensor Hardware ... 121
7.2.2 Laryngoscopes ... 121
7.2.3 Protocol ... 122
7.2.4 Data Analysis... 123
7.3 Results ... 124
7.4 Discussion ... 129
7.4.1 Force Analysis for the ETI training evaluation ... 129
7.4.2 Future work ... 129
7.5 Conclusion of this Chapter ... 130
8 Conclusions and Future Work ... 131
8.1 General Discussion ... 131
8.1.1 Common Skill Evaluation System for Different Medical Applications ... 132
8.2 Conclusions ... 133
8.3 Future work ... 135
Appendix A Electronic Design of Wireless EMG Sensor... 137
References ... 145
Research Achievements ... 163
LIST OF ABBREVIATIONS
BADA baseline adaptive denoising algorithm
BB biceps brachii
CCD charge-coupled device
CS corrugator supercilii
DSP digital signal processor
DWT discrete wavelet transform
ECU extensor carpi ulnaris
EF error function
EFE elbow flexion/extension
EKF extended Kalman filter
EMG electromyography
ER emergency room
ET execution time
ETI endotracheal intubation
FCR flexor carpi radialis
FPS forearm pronation/supination
FTP free time practice
GC generalized coordinate
GUI graphical user Interfaces
ICI isometric contraction index
ICSAD Imperial College surgical assessment device
iEMG integrated electromyography
l-TP left trapezius
MEMS micro-electro-mechanical system
MIS minimally invasive surgery
MVC maximum voluntary contraction
NR noise ratio
OR operating room
OSATS objective structured assessment of technical skills
OSCE objective structured clinical examination
PCB printed circuit board
PSD power spectral density
RMS root mean square
ROM range of motion
r-TP right trapezius
sEMG surface electromyography
SIP stress induced practice
SWT stationary wavelet transform
TB triceps brachii
TRA total repetition average
VR virtual reality
WB Waseda bioinstrumentation
WD wrist deviation
WDA wavelet denoising algorithm
WFE wrist flexion/extension
WKA Waseda Kyotokagaku airway
WKS Waseda Kyotokagaki suture
ZM zygomaticus major
LIST OF FIGURES
Figure 1.1 Laparoscope used for gynecological investigation. 3 Figure 1.2 Laparoscopy: before and after the introduction of CCD camera. 5
Figure 1.3 Endotracheal Intubation (ETI). 6
Figure 1.4 Laryngoscope with Macintosh type curved blades. 7 Figure 1.5 Video Laryngoscope: GlideScope® (left) and McGRATH® MAC (right). 8
Figure 1.6 Laparoscopic training with box trainer. 10
Figure 1.7 VR simulator for laparoscopic training. 10
Figure 1.8 Airway WKA-4 (Waseda Kyotokagaku Airway-No.4). 10 Figure 1.9 Conventional skill evaluation model of box trainer. 12 Figure 1.10 Conventional skill evaluation model of VR simulator. 12
Figure 1.11 Vicon motion capture system. 14
Figure 1.12 Optotrak motion tracking system. 14
Figure 1.13 Waseda Bioinstrumentation system WB-2R. 15
Figure 1.14 WB-2R IMU vs WB-3 IMU. 15
Figure 1.15 Waseda Bioinstrumentation WB-4 IMU. 16
Figure 1.16 Proposed skill evaluation methodology in previous research. 20
Figure 1.17 Proposed skill evaluation methodology. 21
Figure 1.18 Flow chart of thesis chapters. 24
Figure 2.1 WB-3 system. 27
Figure 2.2 IMU of WB-4R system. 28
Figure 2.3 Configuration Block Diagram of the IMU in WB-4R. 30 Figure 2.4 Block Diagram of Online Calibration Algorithm. 32
Figure 2.7 Results of the Offline and Online Calibration at time t=80s. 35 Figure 2.8 Results of the Offline and Online Calibration at time t=130s. 35 Figure 2.9 Plot of Error Function EF for Online Calibration and Offline Calibration. 36 Figure 2.10 Block diagram of the EKF algorithm implemented for WB-4R. 38 Figure 2.11 Position of IMU and calculation of the wrist joint angle. 42 Figure 3.1 Delsys Bagnoli TM 16-channel system (Delsys Inc.). 46 Figure 3.2 Block diagram of the proposed wireless sEMG sensor. 48
Figure 3.3 AC Coupling Schematics. 49
Figure 3.4 Driven Right Led Circuit. 50
Figure 3.5 WB-EMG Sensor. 51
Figure 3.6 Copper core Dry electrodes with 100nm Gold plating. 51 Figure 3.7 Transient response of the circuit, DRL, input and noise. 52
Figure 3.8 Analog Front-end Transfer function. 53
Figure 3.9 Raw EMG Signal for wrist curl exercise. 54
Figure 3.10 FFT of baseline noise (0-20 seconds). 54 Figure 3.11 FFT of muscle extensions (35-45 seconds). 55 Figure 3.12 Flow chart of the Wavelet denoising algorithm. 56
Figure 3.13 Daubechies db2 mother wavelet. 56
Figure 3.14 Spectrum of the Baseline noise. 59
Figure 3.15 Flow chart of BADA algorithm. 60
Figure 3.16 Portions to(T) of the rectified signal. 63 Figure 3.17 Comparison of the algorithms for the R-ECU. 68 Figure 3.18 Original signal (a); difference between the original signal and the signal
denoised by BADA HT (b), UT HT (c), SURE HT (d), SLMU HT (e) and
GSMU HT (f). 69
Figure 4.1 Position of IMU and calculation of the wrist joint angle. 75
Figure 4.2 IMU+sEMG-driven model. 77
Figure 4.3 OpenSIM simulation. 83
Figure 4.4 Wrist Joint Angle and ECU EMG Signal for one exercise. 83
Figure 4.3 Comparison of torque calculated by proposed model and OpenSIM. 84
Figure 5.1 Hardware setup with IMU and sEMG. 89
Figure 5.2 Operative sequence of peg-board training. 92
Figure 5.3 Peg Board platform. 92
Figure 5.4 Operative sequence of pipe cleaner training. 93
Figure 5.5 Pipe Cleaner Board platform. 94
Figure 5.6 Circle Cutting Training environment. 94
Figure 5.7 Ligation Training environment. 95
Figure 5.8 Needle Insertion Training environment. 96
Figure 5.9 WSK-II Training environment. 97
Figure 5.10 VR Suturing Training environment. 97
Figure 5.11 In-vivo Training Suturing and Burning. 98
Figure 5.12 In-vivo Training environment. Kyushu University. 99 Figure 5.13 Comparison between Novices and Expert surgeons for Peg-Board 99 Figure 5.14 Force of the right extensor carpi ulnaris r-ECU. Comparison between (a)
Novice and (b) Expert surgeon for Peg-Board exercise 100 Figure 5.15 Comparison between Novices and Expert surgeons for WSK-No2RII. 101 Figure 5.16 Comparison between Dry boxes and In vivo experiment for novices 101
Figure 6.1 Hardware setup with IMU and sEMG. 107
Figure 6.2 Flow chart of the proposed protocol. 109
Figure 6.3 Averaged values of sEMGmTRA for (a) right side and (b) left side. 113 Figure 6.4 Averaged values of sEMGmMVC for (a) right side and (b) left side. 114
Figure 6.5 diff(iEMG(t)) for the r-ECU and l-ECU. 115
Figure 6.6 Left and right shoulder angular speed, comparison for FTP and SIP. 116 Figure 6.7 Total number of errors during the FTP and SIP practices. 116 Figure 7.1 Location of the electromyography and IMU sensors. 121 Figure 7.2 Different Laryngoscopes used in the experiment. 122 Figure 7.3 Example of the three phases for (a) wrist |ω(t)|WR and (b) L-ECU sEMG. 124 Figure 7.4 (a) Averaged sEMG and (b) ICI for L-ECU muscle. 125 Figure 7.5 (a) Averaged sEMG and (b) ICI for L-FCR muscle. 126 Figure 7.6 (a) Averaged sEMG and (b) ICI for L-BB muscle. 127
Figure A.1 Circuit schematics of WB-EMG. 138
Figure A.2 Top layer of WB-EMG PCB. 139
Figure A.3 Signal layer of WB-3 PCB. 140
Figure A.4 GND layer of WB-EMG PCB. 141
Figure A.5 Bottom layer of WB-EMG PCB. 142
LIST OF TABLES
Table 1.1 Comparison of the traditional Years-in-training approach to residency
education with Competency-based training. 2
Table 2.1 Main Characteristics of the inertial sensors of WB-4R IMU. 28
Table 3.1 Wireless sEMG Sensor Specification. 48
Table 3.2 DQ% Hard Thresholding – Right Arm. 64
Table 3.3 DQ% Hard Thresholding – Shoulders and Face. 64
Table 3.4 DQ% Hard Thresholding – Left Arm. 65
Table 3.5 DQ% Soft Thresholding – Right Arm. 65
Table 3.6 DQ% Soft Thresholding – Shoulders and Face. 66
Table 3.7 DQ% Soft Thresholding – Left Arm. 66
Table 3.8 Hard and Soft Thresholding with αNR=1 and αER=0. 67 Table 4.1 Generalized Coordinates, with intervals and Range Of Motion (ROM). 82
Table A.1 Bill of Materials of WB-EMG. 143
Chapter 1
Introduction
1.1 Background
1.1.1 Competency-based Training in Medical Practices
The main objective of medical education is to guarantee that the graduating physician is competent to practice in his or her selected field of medicine. The evaluation of a resident’s competency to practice, however, has never been clearly defined [1]. Usually, after a fixed amount of years, the program director states if the trainee is ready to practice independently;
the period depends on the medical specialization. Yet, no objective data are provided to verify the real competence of the resident. While it is obvious that physicians should be skilled in the procedures they perform, how to ensure mastery of procedural skills is still a matter of considerable discussion [1]. More and more countries are recently adopting a competency- based training, in which the residents are evaluated on their acquired skills eliminating the concept of years-in-training [2]. This model gives autonomy to each trainee to proceed based on his/her capability, with some intermediate steps to provide evidence of the mastery of what is required: finally, only the residents who proved a real professionalism should be allowed to practice in the specific medical field. One of the goals of the competency-based training is to create a professional physician able to perform independently [3]. Table 1.1 [1] shows the main differences between the traditional years-in-training curriculum and the competency- based training concept, as defined by the American Society of Neurological Surgeons in 1999.
The central point of the Competency-based training is of course the “competence”, which makes the difference between a resident ready to apply medical procedures and one who needs more time. The natural question is “how competence can be measured?” Dr. Donlin M.
Long, Director of the Department of Neurosurgery at the John Hopkins Hospital, Baltimore, USA, has been the pioneer in introducing a real competency-based training for the neurosurgery residency period at his department. In [4] he dedicated a paragraph on
“measures of competency” and he stated that it is relatively simple to assess the procedural skills of a surgeon because skilled impartial observers certainly will know who performs a procedure adequately and who does not. Indeed, the skill level of a doctor is determined by several factors, including cognitive capabilities, decision-making, and operative dexterity [5].
The first two can be taught in classroom-style settings and are to a large degree evaluated by using traditional paper or oral examination methods. However, methods to differentiate and standardize operative skill levels for the purposes of teaching and assessing skill have proven elusive [6].
Table 1.1 Comparison of the traditional Years-in-training approach to residency education with Competency-based training, Society of Neurological Surgeons, 1999 [1].
Years-in-training approach Competency-based training Requires specified number of years in
training, geared to attainment of specific skills
Time taken to acquire knowledge and skills based on the abilities of individual trainees
rather than on the number of years in training
Resident evaluated by certifying opinion of the program director that the trainee is ready to practice; evaluation may be supplemented
by required examinations during training
Provision of an algorithm of the training experience as a blueprint for trainees No specific measures for training in each
specialty; no specific standardized measures for ensuring that competency has been
achieved in the time allotted
Training in each specialty by recognized experts
The methodology for assessing medical operative skill now is strongly motivated to change from subjective scoring to a more objective, quantitative analysis [7]. Especially for complicated hospital environments like surgery settings and emergency care, continuous advances in technology require very specific skill and competences, and their current training and assessments techniques present limitations and challenges.
1. Introduction
1.1.2 Modern Technologies for Surgical Operation: Laparoscopy
The Operating Room (OR) has been changed dramatically during the last Century, with many innovations in the way to operate as well as tools. One of the most important improvements has been the introduction of the Minimally Invasive Surgery (MIS), in which the operation is performed through tiny incisions instead of one large opening, while the visualization of the surgical area is guaranteed by an endoscope, consisting of a flexible or rigid tube with a lens system transmitting the image from the objective lens to the viewer (Figure 1.1).
Laparoscopic surgery is one of the practices of the MIS, referring in particular to the examination and surgery of the abdomen and pelvis [8], even if the terms are often considered synonymous [9]. The term laparoscopy comes from the combination of two Greek words, λαπάρα (lapara) that indicates the soft part of the body between the ribs and hip, and σκοπέω (skopeó) that means "to see". In the laparoscopic surgery the endoscope, called laparoscope, is composed by a rigid telescopic rod lens system usually connected with a video camera; the straight-line body of laparoscopic instrument normally offers 5 mm in diameter and more than 330 mm in length [10]. Made with high quality stainless steel and durable modern materials,
Figure 1.1 Laparoscope used for gynecological investigation.
these instruments are designed to accommodate various surgical procedures. Some additions to the instruments are the rotating and non-rotating slide lock graspers, which offer an ergonomic and precise ratcheting mechanism. Practically, in order to create space for working and visualizing the internal surgical area, the abdomen is filled by carbon dioxide (CO2) through a procedure called pneumoperitoneum [11]. Among the applications of laparoscopy for human surgery, there are gynecological procedures [12], bariatric procedures [13], cholecystectomy [14], appendectomy [15], and pancreatic surgery [16].
The pioneer of modern Laparoscopy is Georg Kelling (1866-1945) from Dresden (Germany). On 23 September 1901, he performed a celioscopy with a Nitze cystoscope on a dog in Hamburg [17], insufflating adbomen with air. In 1910 Hans Christian Jacobaeus (1879–1937), a Swedish internist, reported on his experience with laparothorascopic technique in humans [18]: it was the first time the technique was adopted on a human patient.
However, for the first half of the 20th Century, very few surgeons adopted MIS techniques:
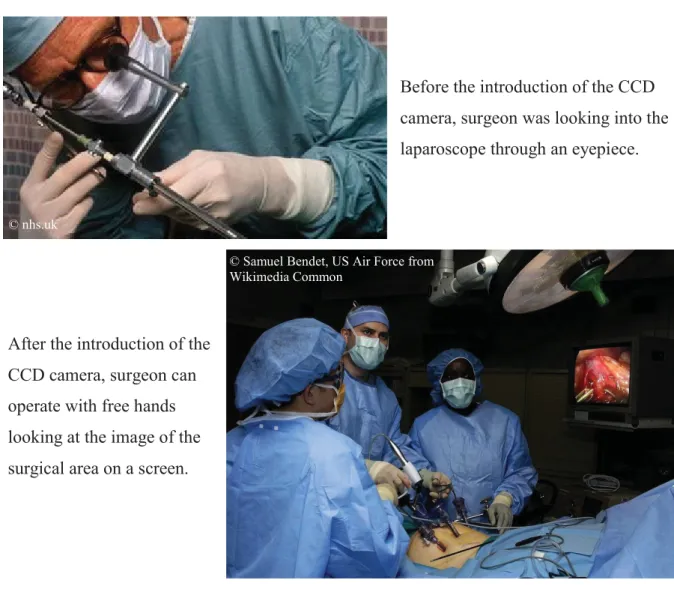
the main reason was the lack of dedicated instruments and the difficulty to operate while looking into an eyepiece; indeed, the laparoscopic technique was used just for diagnosis. In the Sixties’ Dr. Kurt Semm tried to enhance the endoscopic techniques, inventing different laparoscopic instruments to accommodate various surgical procedure, but he struggled to establish the foundation of minimally invasive surgery among his contemporary surgeons [19]. The real pivot moment in laparoscopy was the commercialization of the charge-coupled device (CCD) video cameras in the Eighties’: with the possibility to reflect the image of the laparoscope on a screen, the surgeon could free the hands and establish a more comfortable position (Figure 1.2). The benefits of laparoscopy for the patients are now evident compared to the open surgery: a net immunologic advantage [20], a decreased postoperative pain, less scarring, less intra-operative bleeding, shorten hospital stays and recovery time [21]-[22].
These advantages for the patients are balanced by a huge effort of the surgeons: it has proved that the surgeons practicing the laparoscopy are affected by an augmented mental stress [23], increased technical difficulties [24] and forearm fatigue [25], compared to the open operation. In particular, the technical effort is a consequence of the laparoscopic tools [26] and the difficulty in operating within minimal space without direct vision. The mental and physical stress is the results of the limited vision, requiring additional concentration compared to an operation with direct visualization. Additionally, the force to be applied
1. Introduction
during a laparoscopic surgery is bigger than the one in an open surgery and the tools, due to their lengths, require more force [27].
1.1.3 Modern Technologies for Endotracheal Intubation (ETI)
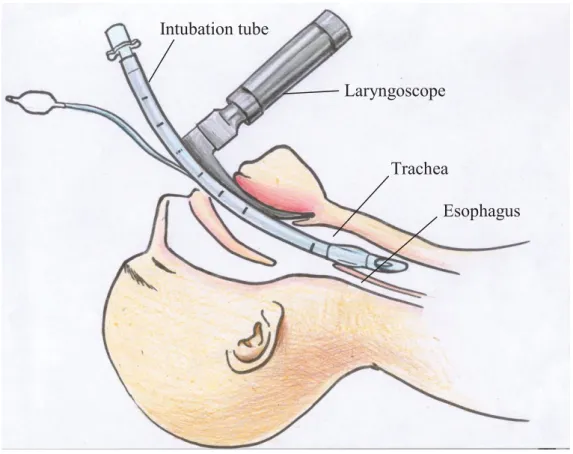
Under emergency situations, in particular after traumas of traffic accident, people could have the impossibility to breath because of obstructed connection between the larynx and the lungs. The first aid should be assured by paramedical personnel or physicians in the Emergency Rooms (ER). Common procedure to connect the larynx and the lungs is the Endotracheal Intubation (ETI) [28]: a tube is inserted to create an airway and to allow a regular breathing after traumas (Figure 1.3). This practice is carried out using a laryngoscope:
Figure 1.2 Laparoscopy: before and after the introduction of CCD camera.
Before the introduction of the CCD camera, surgeon was looking into the laparoscope through an eyepiece.
After the introduction of the CCD camera, surgeon can operate with free hands looking at the image of the surgical area on a screen.
© Samuel Bendet, US Air Force from Wikimedia Common
© nhs.uk
it is a medical instrument used to support the placement of the windpipe. In particular, the laryngoscope is placed at the base of the epiglottis and, once the vocal chords can be visualized, the endotracheal tube is inserted beyond the trachea until the mid-trachea is achieved; at this point, the endotracheal tube cuff is inflated.
The term laryngoscope comes from the union of two Greek words, λάρυγξ (lárynx), which means larynx, and σκοπέω (skopeó) that means "to see". Same as in the laparoscopy, the laryngoscopy is used to facilitate the direct view of internal organ, in this case the oral cavity.
And, same as in the laparoscopy, the laryngoscope has evolved in the years to help the practitioner to perform the operation in shorter time and with reduced damages.
The pioneer of the modern laryngoscopy was Alfred Kirstein (1863-1922) from Berlin, Germany: he was the first to report a direct examination of the interior of the larynx on 23rd April, 1895. During his activity, he proposed different kinds of blades for the laryngoscopes and showed that removal of foreign objects from the trachea was easier by using a laryngoscope than a more invasive tracheostomy. In 1941 Sir Robert Reynolds Macintosh
Figure 1.3 Endotracheal Intubation (ETI).
Laryngoscope Intubation tube
Trachea
Esophagus
1. Introduction
(1897-1928) from Timaru, New Zealand proposed a revolutionary curved shape for the blade of laryngoscopes, with different sizes to be adopted by neonates and adults; the Macintosh blade is still the most-used today (Figure 1.4).
Even if the practice of ETI by the use of laryngoscope is now a common procedure, still the statistics show a high number of consequences and complications after the intubation [29]- [30], especially because the operation is usually performed in emergency situations, with limited time and unpredictable external agents. Also in this case, similarly to laparoscopy, but with some delay in the commercialization, the video laryngoscopes have started to be common from the beginning of 2000. Equipped with a small camera connected to an embedded or external LCD screen, they allow have a better vision of the oral cavity and facilitate the insertion of the tube. The first commercial product, GlideScope Video Laryngoscope® was released in 2001 by Verathon® (Canada) (Figure 1.5).
Figure 1.4 Laryngoscope with Macintosh type curved blades.
Licensed under the Creative Commons Attribution 3.0
175 mm
173 mm
1.1.4 Training for Operating Modern Medical Technologies
Traditionally, trainees learn basic psychomotor skills while performing real operations under the supervision of an expert doctor [31]. However, the modern operative medical procedures require technical skill that needs long time to be acquired [24] and it is not possible to practice directly on the patients, especially if repeated trainings to gain the right dexterity are required. At the same time, hospitals are facing financial issues due to growing costs of malpractice insurance, surgical equipment and personnel salaries: a consequence is the reduction of the investment for training young doctors. These intrinsic problems, together with the fact that many medical schools have started shifting to competency-based curricula, have led to efforts to find alternative methods for teaching medical skills. In particular, the last several years have seen the rapid growth of simulation centers in medical schools,
GlideScope® first video laryngoscope
connected to a LCD screen McGRATH® MAC Video Laryngoscope with embedded LCD screen
Figure 1.5 Video Laryngoscope: GlideScope® on the left and McGRATH® MAC from Aircraft Medical Limited (Edinburgh, United Kingdom) on the right.
Licensed under the Creative Commons
Attribution 3.0 License Licensed under the Creative Commons Attribution 3.0 License
1. Introduction
community colleges, and other health-care training programs [32]: they include warm simulators (e.g., standardized patients or SPs) and cold simulators (box trainers, virtual reality (VR) simulators and robotic systems).
SPs are individuals trained to act the roles of patients, and they are also applied during standard assessment curricula, like the Objective Structured Clinical Examination (OSCE) [33]. The advantages are the possibility to simulate different pathologies in a safe environment and the standardization of the assessment.
A box trainer is a box that is used to simulate the surrounding and a part of a patient’s body (e.g., abdomen in case of laparoscopy). The content of the box can vary between different synthetic inanimate models (e.g., simple physical objects such as pegs), synthetically produced organs, and animal parts. Box trainers provide an environment with natural force feedback, which is obtained due to the use of conventional instruments and equipment (Figure 1.6). The advantages are the possibility to train manual skill repeatedly and the standardization of the exercises.
VR simulators can be defined as a collection of technologies, which allow an interaction with a computer-simulated environment (Figure 1.7) [34], [35]. VR simulators are used to simulate real or imagined environment that can be experienced in various ways (e.g., visually).
Some of current VR simulators are equipped with mimicked force feedback. Force feedback in VR simulators, however, is costly and not very similar to the feedback obtained when using the conventional instruments during operation.
Robotic systems are fully sensorized structures that present improved mechanisms with high-fidelity simulated human anatomy. Figure 1.8 shows the Waseda Kyotokagaku Airway- No.4 (WKA-4) robotic system developed in Waseda University [36] for airway management training. WKA-4 provides high fidelity of human anatomy: for example, it presents a mechanical lung system to simulate active and passive chest movements and a complete nasal cavity mechanism. Additionally, it is equipped with a set of sensors to measure various kinds of skill, and high variety of patients’ patterns can be simulated.
Studies have shown that training on simulators can improve the doctors’ operative skills [37]. Skill evaluation methods in these current training facilities, however, are still far from being objective or even missing in some regular training. Moreover, they do not provide general and common assessments for qualifying skill competences of doctors in different
Figure 1.6 Laparoscopic training with box trainer.
Figure 1.7 VR simulator for laparoscopic training.
Figure 1.8 Airway WKA-4 (Waseda Kyotokagaku Airway-No.4).
1. Introduction
1.1.5 Assessment of Medical Practices: Limitations and Challenges
Operative skill evaluation methods basically can be divided into two categories: subjective and objective. In most of the current training facilities, such as box trainers used in routine training courses, evaluation of medical operative skills heavily relies on subjective measures and scoring by an expert, which may be a variably biased opinion using vague criteria (Figure 1.9). For example, also in the Objective Structured Assessment of Technical Skills (OSATS), residents perform a series of standardized surgical tasks on inanimate models under the direct observation of an expert surgeon [38]; in this case the term “objective” refers to the repeatability of the tasks using simulators. However a) there is a high risk of the assessors subjectively interpreting the results due to the visual inspection, with the outcome depending on background, skill, and experience of the assessors. This could make the evaluation highly variable from place to place, and from assessor to assessor. Also, b) it is difficult to secure the time of senior surgeons during the training, because they are extremely busy for their own work; besides c) not all facilities can count on such skilled personnel. These problems a) - c) translate into a big unbalance of preparation among surgeons of different hospitals and consequently among communities [39], which in turn translates directly into a difference of treatment for the patients.
The main challenge is to help assessors in changing from subjective scoring to a more objective, quantitative analysis [7], and overcome the limitations a) - c). The advantage is that virtually all the physicians in all the hospitals in the world can have the same high level of training/evaluation as the top ones, with an evident benefit for the patients.
Among the current technologies, the VR simulators, which are now commercially available, have been comprehensively validated as an objective surgical data analysis tool.
However, these simulators, which are embedded with objective skill evaluation methods, provide only low-level scoring results by using the execution time and instrument trajectory information recorded during the training to assess operative skills (Figure 1.10). Additionally, the embedded skill evaluation methods of VR simulators are just for those specific training devices, which cannot be used for other training devices and medical applications. Moreover, no matter how exhaustive or excellent the VR simulator might be, they can still only serve as a good complementary solution to training on real-world scenarios [40].
Figure 1.9 Conventional skill evaluation model of box trainer.
Figure 1.10 Conventional skill evaluation model of VR simulator.
1.2 Biomechanical Analysis for Operative Skill Evaluation
1.2.1 Motion Analysis as Assessment Tool
In the literature, posture and motions analysis has demonstrated to be an indicator of the performance in simulated medical procedures [41]-[42]. This follows the school of thought that psychomotor skill is learned and that the movements made by the trainees will eventually become more efficient. Motion analysis 1) can provide numerical data of performance, 2) can feedback wrong postures, 3) does not need constant visual inspection by the assessors [43]- [44], 4) can help to distinguish which physician performs the procedure more efficiently, 5) can identify what kinds of movements are important in each step of the procedure, and then 6) let the experts improve the lessons for training more junior surgeons. Therefore, from the clinical point of view, it is necessary to find appropriate parameters that can measure the
Experience-based evaluation
Subjective suggestion Box trainer
Trainee
Expert doctor
Scoring
Trainee Time and instrument
motion analysis VR simulator
( with embedded skill
evaluation methods)
1. Introduction
quality of movements for supplementing the assessment of medical operative skills, and it is also necessary to determine how these parameters should be combined.
From the mere hardware point of view, most widely used motion tracking systems are optical camera-based systems which determine position by using multiple cameras to track predetermined points on moving objects within a working volume, such as Vicon (Figure 1.11) [45] and Optotrac (Figure 1.12) [46]. In these systems the performer wears markers that are followed by several cameras and the information is triangulated between them. The markers themselves may be either passive (retroreflective) or active (light-emitting diodes).
The performer is then free to move due to no cables connecting body to the equipment, and more performers are possible in the same configured environment. In general, most of the marker-based optical sensing technologies for motion tracking suffer from occlusion problems whenever a required light path is blocked. Interference from other light sources may also be a problem. Lighting conditions must be controlled in order for the camera to consistently see objects in the environment. Depending upon the type of light in use, there may be severe range limitations. Therefore, these systems in fact can be used only in the calibrated room, but not outdoor.
Some specific hardware with embedded modeling for the kinematic analysis of medical procedure has been introduced to overcome the limitations of the optical tracking systems.
For example, Moorthy et al. [47] introduced a motion analysis system called Imperial College Surgical Assessment Device (ICSAD) for evaluating dexterity of surgical competence. This system analyzed the number, speed and the distance traveled of hand movements to discriminate surgeons, but the motion analysis of other parts of surgeon’s upper limbs was still lacked, which is also considered to be an important feature for skill evaluation. Chmarra et al. [48] developed a four degrees of freedom, low-cost device called TrEndo for tracking laparoscopic instruments. This device consisted of a gimbal mechanism with three optical computer mouse sensors, to guide and measure the instrument movement. This system can classify the subjects as experts, intermediates, and novices according to their basic laparoscopic skills. However, the movement analysis of surgeon’s upper limbs was still missing in this study. Moreover, this system can only be used in the routine training course to evaluate the surgical skill, but cannot be further performed and evaluated in the real operation theater.
Figure 1.11 Vicon motion capture system.
Figure 1.12 Optotrak motion tracking system.
More recently, the use of miniaturized Inertial Measurement Units (IMUs) is becoming popular, because they are cheap, small, and relatively maintenance-free [44],[49]. In a previous work, our scientific group proposed to use Waseda Bioinstrumentation system WB- 2R (Figure 1.13). It was demonstrated that it could objectively measure the movements of the head, the arms, and the hands, to evaluate laparoscopic skill improvement after the subject finished a two days’ routine laparoscopic training course [50]. Results showed that motion analysis of surgeon’s upper limbs can efficiently identify the performance improvement after
1126 mm 161 mm
1. Introduction
the training course. However, the previous system was still not wearable enough, and the classification methods between expert surgeons and novices were missing.
Figure 1.13 Waseda Bioinstrumentation system WB-2R.
Figure 1.14 WB-2R IMU vs WB-3 IMU.
Upper Body:
Inertial sensor x 12
Lower Body:
Inertial sensor x 8
A more recent study proposed a new hardware, named WB-3, and a novel methodology of defining a processing model to objectively evaluate surgical movement performance, to be used practically and efficiently in routine laparoscopic training course for supplementing the assessment of operative skills [42]. While WB-3 system, in combination with a dedicated suit, was more wearable than WB-2R, with over 40% reduced size and 50% reduced weight (Figure 1.14), still it had some limitations due to the wires connecting each IMU.
Finally, at the end of 2010, our group proposed a new wireless IMU, named WB-4 (Figure 1.15): it has been used successfully for the evaluation of mastication [51]; in Chapter 2 an evolution of this platform, named WB-4R, is presented.
Figure 1.15 Waseda Bioinstrumentation WB-4 IMU.
1.2.2 Electromyography Analysis as Assessment Tool
As assessment tool, the electromyographic signal analysis has been used for the biomechanical analysis of human movement [52]. In particular, the Surface Electromyography (sEMG) provides a safe, easy and non-invasive method to qualitatively and quantitatively analyze the activity of the muscles [53] [54]: unlike needle EMG, where the procedure is performed invasively by inserting needles through the skin into the muscle, the sEMG examination evaluates muscle function by recording activity from the surface above the muscle on the skin. Currently, sEMG is widely applied for the assessment in sport
1. Introduction
[55] [56], rehabilitation [57] [58], ergonomic design [59] [60], and medical robotics [61]. If the setup and the analysis of the signals are carried out following standard procedures, the sEMG can be used for an objective evaluation of the performances. For example, in [62] and [63] the authors used the surface Electromyography to analyze in particular the ergonomics of surgeons and found the relation between wrong postures and fatigue. More recently Judkins et al. [64] showed the results of the electromyographic response in case of training with robotic surgical training with on screen feedback on the muscles activation. They also measured the performance of the surgical activity under the hypothesis that muscle activation and fatigue should decrease after short-term training as they observed previously with long-term training [65]. Electromyography has been studied from many years and its signal has been analyzed from different points of views [66]; however, the use of sEMG for assess the medical practices is still limited, and all the works published at today, 2013, show only the possibility to apply it, but not a real application on the field. Among the limitations that make the use of sEMG in practical trainings and inside the ORs, there are: 1) the commercial sEMG are mostly wired system, with very reduced wearability; 2) they have not Graphical User Interfaces (GUIs) to easily support the assessors in analyze the data off line or real time; 3) the sEMG has not information of the kinematics of the subject. Even if recently some wireless sEMG have been commercialized, still their cost is very high and they present closed protocols to access directly to raw data for a customized post-processing.
1.3 Problem Statement
Evaluation of operative skills heavily relies on subjective measures and scoring by an expert doctor, which may be a variably biased opinion using vague criteria. Consequently, among all the current trainings for the medical practices, there is one common need, which is the objective skill evaluation system. Objective skill assessment could provide discernment of doctors’ operative skill competence and validate whether the doctors have qualified abilities for the real operation on the patients. This concept is compliant with the Competency-Based Training system in which the assessment of the competence is the key point for residents to become independents in their medical practices. Additionally, more effective trainings can be developed and objective feedbacks can support the assessors in evaluating and correct the
Currently, the objective skill evaluation systems on most of the current training facilities have several limitations, which can be basically summarized into two main aspects:
1) In the cases of Virtual Reality (Figure 1.10) or dedicated simulators, they provide only low-level skill scoring by using the execution time and instrument’s motion information for completing the training tasks; additionally, they cannot be extended to other medical training systems.
2) Existing general objective skill evaluation methods use only motion analysis or only muscle force analysis. There is not a system that combines both of them and one information is always missing.
1.4 Goal of this Thesis
1.4.1 Aims
In this thesis, the road towards the realization of a common objective skill evaluation system for multiple medical applications is presented. The specific goal of this work is to develop a new integrated biomechanical model for the objective assessment of medical skills, and to provide it to the assessors for an impartial and exhaustive evaluation and coaching of the trainees. More specifically, the proposed system aims at answering the questions: how to discover and analyze objectively the trainees’ weak points, and how to overcome them in the best possible way. The advantage is that virtually all the physicians in all the hospitals in the world can have the same high level of training/evaluation as the top ones, with an evident benefit for the patients.
In this work the aims are achieved by:
1) developing a common skill evaluation system, which is independent from the training devices and can be adaptive for various medical training scenarios.
2) combining human motion tracking system and surface electromyography in an EMG- Motion model suitable for analyzing the biomechanics of trainee’s upper body during practical medical training.
3) verifying that the proposed skill evaluation system can be implemented in multiple medical applications for evaluating the surgical operative skills and assisting clinical practice.
1. Introduction
At the end, this research demonstrates a general methodology for objectively evaluating medical operative skills. The model can be used not only for regular operative skill trainings, but can be also further implemented for clinical practice and other medical scenarios.
1.4.2 Innovation
This thesis tackles several fascinating challenges. From the scientific point of view, it shows the development of an original biomechanical model, fusing the data from sEMG and IMU. It will help in identifying new significant neuromusculoskeletal parameters never noticed until now. From technical point of view, it challenges the development of a new wireless EMG sensor and its synchronization with the existing IMU sensor. This novel proposed combined model of motion analysis and sEMG is used for the first time for the performance evaluation.
At the end, this research demonstrates a general methodology for objectively evaluating medical operative skills. The model can be used not only for regular operative skill trainings, but can be also further implemented for clinical practice and other medical scenarios.
1.4.3 Contribution of this Research
This research develops a biomechanical model combining the information of the motion and muscle force that overcomes the limitations of medical skill training and evaluation systems currently in use. The final goal is to help assessors in objectively evaluate the performance of young surgeons during trainings and define better curricula; a fully automatized measurement system reduces the time of the assessment and increases its objectivity. Additionally, the proposed system, composed by a low-cost IMU and sEMG (developed by off-the-shelf components) can be used virtually everywhere, also by facilities with reduced budget.
Two different medical applications of laparoscopic surgery and endotracheal intubation analysis are assessed in this thesis, which verifies that the proposed skill evaluation system can be implemented in various medical fields. Eventually, it will be presented the study on combined motion and sEMG, together with additional physiological parameters (heart beat rate, blood pressure), to evaluate the effects of induced mental stress in laparoscopic training.
1.5 Methodology
1.5.1 Objective Assessment Methodology: Previous Research
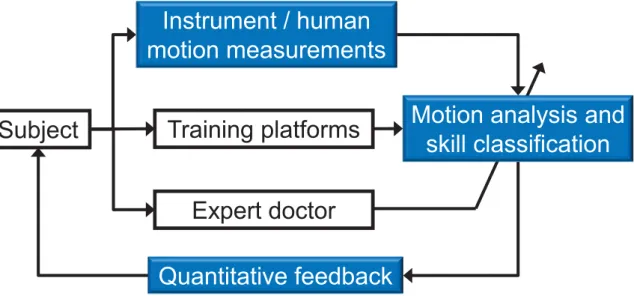
In previous research an objective assessment methodology based on the only motion analysis was proposed by our group, as showed in the block diagram in Figure 1.16. The Subject block in the diagram indicates the doctors whose operative skill needed to be trained and evaluated, or the patients whose motion performance needed to be assessed for clinical practice. The blocks with blue color were the primary novel items and contributions.
Figure 1.16 Proposed skill evaluation methodology in previous research.
In particular, the block of Instrument/human motion measurements records the motion data of the subjects or the manipulated instruments during various skill training tasks, and provides this information as the basis for skill evaluation. The block of Training platforms can be the box trainers and VR simulators in different medical applications; in the previous research our group concentrated mainly on laparoscopic surgery and neurosurgery training.
The block of Motion analysis and skill classification extracts the significant motion features and classifies the skill levels of the subjects based on a statistical pattern recognition model.
Finally, the block of Quantitative feedback provides the motion information of the significant features to the subjects, and presents which motion still has, for example, poor performance and needs to be improved.
Instrument / human motion measurements
Motion analysis and skill classification
Quantitative feedback Training platforms Subject
Expert doctor
1. Introduction
1.5.2 Proposed Objective Assessment Methodology
Figure 1.17 Proposed skill evaluation methodology.
The block diagram of the new proposed methodology in this thesis is presented in Figure 1.17. Common block with previous research are related to the subject, the expert doctor and the training platforms. About the training platform, in this thesis the airway training system has been added. The main innovations of this work are the combination of motion and muscle force measurements and the biomechanical analysis for skill evaluation. In particular, the Measurement block is composed by wireless IMU and sEMG sensors developed in our group, presented respectively in Chapters 2 and 3. The Biomechanical analysis is performed by an original EMG+IMU driven musculoskeletal model described in details in the Chapter 4.
Finally, the expert doctor takes advantage of the results from the skill evaluation and from the quantitative feedback.
1.5.3 Protection of Human Rights
The experimental activities with human subjects have been conducted with healthy adult volunteers, with no invasive device and without any risk for the health of the participants.
Some experiments have involved residents and expert surgeons. In any case, the experimental
protocol has been discussed and agreed in advance with the Ethical Committee of Waseda University and with the other institutions involved.
The right to privacy of the subjects has been fully respected. They have been extensively informed and asked for the consent to the experiment, also taking into account their age and their health conditions, according to the existing national and international laws and regulations. The experimental data and all personal information, whether electronic, written, or oral, have been anonymized and used only for statistical analysis. All the data communication with the data servers have been encrypted and password protected by using the state of the art standards to ensure maximum protection and reliability.
1.6 Thesis Outline
This thesis contains two primary parts: Part I introduces the development of the hardware and biomechanical model, together with the methodology used in the experiments, and it is composed by Chapters 1-4; Part II deals with the evaluation of medical operative skills based on analysis of subject’s upper body biomechanics in the fields of laparoscopic and airway trainings, and it is composed by the Chapters 5-7. Chapter 8 concludes. Figure 1.18 shows the research flow in this thesis and the relation between each chapter.
The thesis is laid out as follows:
Chapter 1 introduces the research background with a detailed analysis of the state of the art of related researches on the assessment for medical operative skill evaluation by motion analysis and muscle force analysis.
Chapter 2 is dedicated to the improvement of the WB-4 IMU developed in previous research. In particular, it is presented the new WB-4R system, based on hybrid wired-wireless approach with larger battery, able to sustain experiments up to five hours. A new online calibration of the magnetic sensor is then introduced, to make the sensor more robust to the presence of external ferromagnetic material interference, with the advantage of real time capability. Finally, an algorithm for the joint angle estimation is presented, based on Extended Kalman Filter.
Chapter 3 introduces the development of a new low-cost wireless sEMG sensor and the experimental results for its characterization. Additionally, the Chapter tackles a problem that usually affects the sEMG signal: the baseline noise. It is presented a new method to denoise
1. Introduction
real-time the sEMG signal using the same baseline to estimate the thresholds of the Wavelet denoising algorithm, named Baseline Adaptive Denoising Algorithm (BADA).
Chapter 4 presents a new biomechanical EMG+IMU driven model, developed to go beyond the two main limitations that restrict those models in real applications: the first is the space limitation, because optical tracking systems are usually used; the second is the absence of real-time capability. The wireless inertial measurement units and the surface EMG sensors described in the previous chapters help in overcoming the first limitation. A simplified original algorithm is described to achieve real time capability. The chapter closes with the experimental validation of the model.
Chapter 5 describes the use of the biomechanical model to evaluate the expert and novice surgeons’ surgical operative skills during regular laparoscopic training tasks. In collaboration with Kyushu University Medical Department, this is the first work in the world assessing a complex curriculum based on dry boxes, Virtual Reality and in-vivo surgical training. The results show significant differences not only between the novice and expert surgeons, but also between the training tasks.
Chapter 6 presents the application of the proposed evaluation system in case of induced mental stress during laparoscopic training. Standard trainings are carried out to improve only the manual skill of the doctors, without any additional mental stress, that is actually present during the real operation. In this chapter a novel protocol to induce mental stress is introduced and verified experimentally, showing finally that the mental stress had significant effects on the learning curve and number of errors.
Chapter 7 presents the application of the biomechanical model to the endotracheal intubation medical practice, in which novice and expert physicians are compared together with different kinds of laryngoscopes. It is demonstrated that video-laryngoscopes reduce significantly the force applied during the insertion of the tube in both novices and experts.
Chapter 8 concludes the evaluation results and considerations in this thesis, and discusses about future works, which are proposed as a perspective to continue the research direction; in particular, a further miniaturization of the system and the enhancement of the real-time capability, could lead to real application also inside the operating and emergency room.
Figure 1.18 Flow chart of thesis chapters.
Chapter 2
Motion Analysis: Inertial Measurement Unit WB-4R
2.1 Introduction
Recently, the interest on motion tracking systems is increased in many fields; for example, in medical applications they are used to obtain more effective rehabilitation therapies [67], and to develop networks able to monitor patients and elder people in hospitals and in their own home [68]. Wide interest comes also from the game industry, where the market trend is going to the augmented reality with more interactive platforms, in which the entire body, with the use of motion tracking systems, could participate to the game scenario with virtual avatar [69]. Furthermore, the manufacturing industry is very interested in small motion systems, to track in reliable and affordable way the human operator and enhance the human-robot interaction in a robotized environment, as most of the modern factories [70]. In all the mentioned fields, the crucial points in the development of a motion tracking system are 1. the dimensions, 2. the wearability, 3. the cost and 4. the performances. The first two points are related to the possibility to be worn by a person: if an additional object is felt as a disturbance, it can affect the executions of the user; also, the cost is linked to the commercialization and the extensive use in an application; finally, the performances are necessary to have an objective and reliable measurement of the motion.