NII-Electronic Library Service
Decision-Making
Process
Regarding
the
Use
of
Mechanical
Ventilation
by
a
Patient
with
Amyotrophic
Lateral
Sclerosis:
Interaction
of
the
Patient
withFamily
Members
and
Specialists
Ybshimi SUMIDA
NiigataUniversityFacultyDentistryDepartment of Oral Healthand Welfare
Abstract
Objective:Theobjective of thjsstudy was to examine how specialists should provide support tbramyotrophic lateral sclcrosis (ALS)patientsintheprocessof theirdecision-makingregarding the use of mechanicul ventilation.A case analysis was made focusedon thechangcs inapatient'sperceptionthrough thc processof herinteraction with her
farn-ilymembcrs and specialists.
Methods/ The author visited thepatient'shome rcgularly, and conducted interviewswith the patient,herfamilyand the specialistsinvolved.
Results:There were perceptual differencesregarding theuse of mcchanica] ventilation among thepaticnt,her famiLy und specialists. These differencesarose becauseof thedifferencesinthepatient'sperspectiyc,which focusedon the prescnt,and that of thc specialists, which focusedon futuredcvclopments,Problemsresulting from informationgaps wcrc resolved by ongoing professionalinvolvementincludingtheprovisionof information,while problems arising
fromdifferentva]ues were dienculttodealwith.
Conctusion:Specialistsshould be aware of thesedifferenccswhen offering suppert. Besidesprovidingaccurate infor-matien, theyshould facilitateinteractionbetwccn thepatientsand familymembers, thus helpingthem to reach a con-sensus.
Keywords
AmyotrophicLateralSclcrosis,Interaction,Mechanical Nlantilation,Decisien-making
1.
Introduction
This article discussesthe interactionof a patient
with amyotrophic lateralsclerosis
(ALS)
with herfamilyand specialists concerning herdecision-making
processregarding the use of mechanical ventilation.
ALS
is
a neurodegenerative diseaseof unknown etiol-ogy caused by progressivedegenerationof the motorneurons. The diseaseisusually fatalin two to four years unless mechanical ventilation isused
(Society
forPreventionand Care Management of Incurable
and ChrenicDiseases,2003,pp.295-6).Two hundred and fiftyseven special diseasecertificates were issued
forpatientswith ALS inJapan in1974,however,the number increasedto6,646in2002
(Society
for Preven-tionand Care Management of lncurable and ChronicDiseases,2003,p. 446).
Since the practiceof informed consent was
proposedinthe fieldof medicine, more importance
has been placed on supporting patientsregarding
theirchoice of treatment methods. The causes of
ALS and itstreatment methods are stM unknown
'
and quadriparesis,speech disorders,dysphagia, and
respiratory problemsdevelopas thc diseaseprogresses.
However, with regard to speech disorders,
com-munication devices enablc patientsto comrnunicate,
and syrnptoms management, such as tube feeding
for
-25-dysphagiaand artificiairespiration, helpprolongtheir
lives.In 1990the consultation and management fees
forhome ventilation were covered by thegovernment healthinsurance.In1992the Medical
Care
Law
was amended, and designatedthe patient'shome as a placefbrprovidingmedical treatment.In1994 when home-visitnursmg care programswere expanded tothe
non-elderly popu]ationthecare situation conceming patients with ALS also changed. The developmentof medical science and changes inmedical systems increasedthe choices conceming treatmentmethods
(symptoms
man-agement) and theplacefbrtreatment,either at home orhospitalforpatientswith ALS, which required them to
havethecapacity tomake decisions.
As ALS patientsbasicallyretain their intellectua] functions,self decision-makingispossibleforthem.
According to Kamo
(1)
adults who are capable ofmaking
judgments
havetheright(2)
tomake decisionsand toreceive infbrmationnecessary forsuch decision-making concerning
(3)
what belongs to them including theirbody
and qualityof life,(4)
as longas itdoes not harrnothers,(5)
even ifitresults inan irrationaloutcome forthe patient
(Kamo
1996, pp. 12-3.>. Kojima definesself determinationas making decisionsabout theirown lives
(Kojima
2002, p.210.).Decidingon mechanical ventilation isliterallya choice of ]ifefor
patientsand a difficultone tomake. Theyfeel
ambiva-lentbetweentheirwish to liveand sustaining their lives ina state of immobility.
Many differentperspectiveshave beenproposed by professionalsto support ALS patientsinmaking
the decisionregarding mechanical yentilation, but
there islittleresearch on whether the patientsmanaged
theirdiseaseas professionalshadexpected or how the patientsfeltabout theirsupport. ThisarticLe discusses
how specialists should providesupport forALS patients
by clarifying how such a patient changed through
herinteractionwith herfamilyand specialists during
the processof decidingon mechanical ventilation,
focusingon theperceptualgapof the patientand those
concerned with her regarding the use of mechanical
ventilation and thechanges inthepereeptualgapas the keywords,
The perceptualgap inthe helpingprocessresults
from the differencesin the standpoint of the patient, familymembers and specialists as well as differencesin
professionalismamong specialists. Infact,professional
differences
are importantinunderstanding theproblemsfrom differentangles. However, ifthe perceptualgap arises when common understanding isnecessary inthe
helping
process,problem solving becomes difficult.This research studies theperceptua]gapresulting from
the differentpositionsof the patient,family members,
and specialists intheprocess of thepatient's
decision-making concerning mechanical ventilation and whattriggeredthechanges intheirperception.
1.
Issues
of decision-makingcapacity and makingchoices concerning mechanical ventilation
Biestek listedthe princjpleof self-determination as one of the basicsocial work principles
(Biestek
1957-1996, pp. 160-89). According te Biestek, personalitydevelops and matures when peoplemake
decisionson theirown. Howeyer, Kojima refutes that itistaken forgrantedthatself-determination means
taking responsibiiity, butthatthere are situations in
which clients are unable toassume responsibility even
ifthey wish tobecauseof inadequacy or lackof social
resources or information
(Kojima
2002,p.230).ALS patientsbasicallyrequire 24-hourcare once
they become ventilator dependent.However, inthe
current situation inJapan,social resources are less
than sufficient for ALS patients.There are almost no hospitalsor institutionswhich can accommodate
ventilator dependent patientswho need long-term
hospitalization.Even ifpatients at home use
long-term care insurance,medical care insurance,and allthe
services available fbrspecified diseasesand disabilities
theycan use only a fewhoursof care services adayto
substitute theirprimarycaregivers, which imposescare
burdenson theirfamilyalmost all day.Inaddition, in
order forALS patientstochoose mechanical ventilation their familiesare required to have the capacity to take care of the patientat home. Inprinciple,thereshould
beconditions forthe
patients,
which enable them to choose mechanical ventilation ordeny
it,However, iftheirfamiliesare incapableof providingcare, not afew
patientsmust giyeup using mechanical ventilation.
-26-NII-Electronic Library Service
Family members must get up two to fivetimes during the night to suck inphlegm inaddition tothe daytime,They cannot sleep through the njght, and ac-cumulate fatiguefromcare giving.Thiscauses patients
to feelambivalent because they feelthattheirneed
forcare might change theirfamilymembers' lives, while atthe same time they havea desiretolive. Self-determinationunder such circumstances isnot really
self-determination as the patientisdependenton the
famity'scapacity toprovidecare.
2. Interactioninthe
process
ofdecision-making concerning mechanical ventilationInprinciple,selfdecision-makingisbasedon the patient'sautonomy, butvarious value orientations of the peoplewhom patientsinteractwith and social values
infiuencetheirdecision-making.There are reports that when ALS patientsmake decisionsregarding medical
treatmentpreferencesseveral factorsaffect the process:
provision of information
(Young
1994;Moss 1993;Mark 1996), physician'sattitude
(Ybung
1994;Albert1999; Moss !993), family
(Ybung
1994;Moss t993; Mark 1996),attachment to life(Albert
1999),abilitytocontrol discontinuationof ventilation
(YOung
1994;Mark 1996),costs
(Moss,1993),
and insurancecover-age
(Albert
1999;Moss 1993).Accurate information isessential when patients make decisionsabout treatment preferences. There
are two kinds of informationconcerning medical
treatment and patients'lifewith the illness.
Physi-cians playan importantrole forpatientsto obtain
medical information,and theirattitudes influencethe patient'sdecision-makingAccordingto the treatment
guidelinesof the Japanese Society of Neurology
(Japanese
Societyof Neurology,2002) physiciansmust give patientsboth positive and negatiye
inforrnationconcerning mechanica] ventilation and
giye explanations without imposingtheirown values. "Physicians
who had a positivepersonal attitude
toward home ventilation and remained neutral intheir presentationof ithad a higherpercentageof patients on home ventilation"
(Moss
1993).Tateiwastates thatthe basicstance of society should support patientsto sustain their livesand thatphysiciansshould not take
aneutral positionbutprovidepatientswith a structure which enables them to live,while givingthem the
freedomto reject it
(Tateiwa
2003, pp.33-6).Timing isalso
important
concerning the givingof inforrnation."Physicians
said thatitwas bestto
discussthe option of home ventilation soon after the
diagnosis
ofALS"(Moss
1993)."Patientpreferences
may change over time,and clinical education efforts are required throughout the course of disease
(Albcrt
l999).
Besidesinformation,familyand social yalues are
influencingfactors.A family's way of thinking and
theirrelationship with the patientaffect the patient bothpositively and adversely. Many patients with
ALS hesitate to depend on mechanical ventilation
because of burdeningtheirfamilymembers, butin some cases they decidetouse itbecause they feel
they are needed by their family.Japanese social values do not approve assisted suicide or stopping
mechanical ventilation even ifpatientswish it.Since
they cannot be incontrol of stopping mechanical ventilation they have no choice togiveita try.This
isthe main reason why patientshesitateto decide on
home ventilation.
As faras social factorsare concerned, costs and
insurancesystems influencetheprocessof thepatient's decision-making.Inthe UnitedStates,"In
general,
pa-tients inour study had more comprehensive insurance coverage and significantly higherincomes than does
average American"
(Moss
1993).InJapan,asmcchani-cal ventilation iscovered
by
publichealthinsuranceand apolicyfordeveloping home medical care services
hasbeenpromoted, the number of patientson home ventilation has beenincreasing
(Sumida
2002).How-ever, thereare gapsbetweenmunicipalities becauseof
thediffk)rentattitudes of physicianstowards mechanical ventilation as well as the self-help group activities in
each area
(Shimizu
2001).The levelof a patient'sattachment to lifeisalse an
influencingfactor.`'Patients who stated thatthey had
a strong will tolive,had something to lookforward toeach day,continued to looktothefuture,ete,,were
more likelytofavortracheostomy and PEG placement"
(Albert
1999).
Decisionson how patients liveshould be made
based on theirinitiative,but are often influenced by their interactionwith their families and specialists.
Socialvalues and institutionalfactorsalso influencethe
process.Thisstudy focusesmainly on the interaction
among the patient,herfamilyand specialists.
11.
Methods
Surveysby interviewsnormally focuson the past
feelingsof patients.However,the datadoesnot
neces-sarily reflect pastfeelingsbutmay be affected by pres-ent feelings.Thisresearch ischaracterized byitsfocus on the presentfeelingsof the patient,which arise from
physical changes as well as changes inthe patient's environment and discussesthe patient'spsychological
changes by continuing interviewsconcerning her
presentfeelings.Secondly,interviewswere not carried out with the patientonly, butalso with herfamilyand
specialists. Whenever the physical and environmental conditions of thepatientchanged, attention was given
toherthoughts and feelings,herfamilyand specialists, whether the support was providedas the patienthad
wished and whether thesupport providedbyspecialists
was effective were reviewed frem the perspectiveef
the perceptualgapbetweenthe patientand specialists,
Thirdly,intheinterimprocessof analysis thepatient
and herfamilywere asked to provide input,thus re-viewing the support fromthe perspectiveof the patient
herself.Withregard tothechoice of a candidate fbrthis
research, takingintoconsideration thecharacteristics of
theresearch, thepatient,who cou]d cooperate with this
research fromthetime of beinginfbrmedof the disease
not long before,and herfamily were asked to cooperate
with thisresearch.
Ms.A
(in
her60s)liveswith herhusband,daughterand thedaughters'chiLd. The familyruns a shop from their home, and Ms. A didmost of thehousework and
took care of the shop, There are two more daughters who havetheirown families.Ms A became aware of
hersymptoms in1998,and visited a number of
hospi-talsuntil she was diagnosedas suffering fromALS at
thedepartmentofneurology atHospitalA inMay 200i.
However, she changed hospitals
because
she lostcon-fidenceinherdoctor.InJuly2002,she was admitted
toHospitalB formedical examinations, and herchief
physicianpLanneda visit by herto a non-ventilator
dependentALS patientwhile she was inhospital.In
ad-dition,heelicited PEG and tracheostomy since bulbar
palsywas progressingmore than quadriplegia.The patientrejected bothof them, butdecidedtohavePEG
at thestrong request of herdaughter.Atthe time of her
dischargefromthehospitala network meeting was held
by the staff from a specialty hospital,an Intractable
DiseasesInformationCenter,and a healthcenter, and
theyplannedfbrhertolivewith ALS at home. At the
end of 2002, interventionswere begun to elicit her
decision-makingregarding mechanical ventilation. The
fo11owinginterventionplanswere made: home visit by
anurse fromtheIntractableDiseaseslnformation Cen-tertoconfirm herand herfamily'spreferences;visitto
aventilator dependentpatientwith ALS; and admission
tohospitaland confirmation of herpreferencesby her chiefphysician.
For thisresearch, the author visited thepatient's home regularly tointerviewthepatient,herfamilyand specialists. SinceOctober2002,the author made visits once or twice a month, asking herand herfamilyif there were any difficultiesor changes, and made field
notes followingeach visit,InJanuary2003,
special-istsplannedinterventionsregarding herpreferences
concerning the use of mechanical ventilation.
Aceord-ingly,semi-structured interviewswere eonducted twice
forthe patientbothbeforeand after the intervention
and forthe family after the intervention.Regular
visitstothepatient'shome were continued after these
semi-structured interviews.Inaddition, inorder to
compare the perceptionsof the patientand herfamily
by identifyinghow professjonalswere involvedand
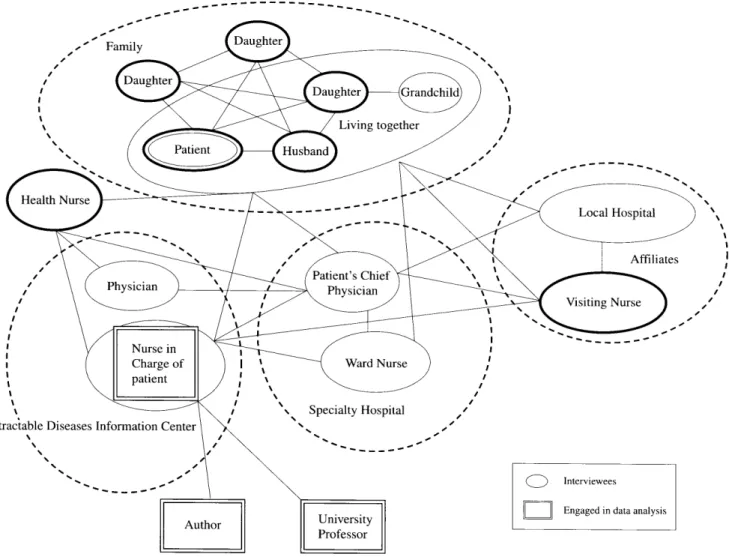
from what perspectives,interviewswere conducted with herchief physicianat the specialty hospital,a
nurse at the IntractableDiseasesInfbrmationCenter'),
a visiting nurse, and a healthnurse
(Fig.
1).While thepatientwas hospitalizedthe author attended a meeting of the physicianand herfamilywith permission from
thepatient,herfamilyand herchief physician,At the beginning,the author visited thepatientwith thenurse
-28-NII-Electronic Library Service
from
the lntractableDiseasesInformation Center,butafter the author made an official request tovisit the
patientforresearch, they visited thepatientseparately todistinguishthe visits regarding research and care. Interviews were recorded with consent from the
persons who cooperated inthe research and a verbatim record was made. The patientanswered questionsin writing and the author recorded partof the answers
while reading them aloud. The author, the nurse from
the IntractableDiseases Inforrnation Center,and a university professoranalyzed the transcript,identified
theproblemsand discussedwhat kindof support the
patient
wouLd need. The dataconcerning the patient,herfamilyand specialists was organized in chrono]ogi-cal order and puttogether toexamine the perceptual
gap among thepatient,herfamilyand specialists and
analyzed how theirinteractionchanged thegap.
Per-mission concerning the sharing of dataamong theteam
members was also obtained fromthosewho cooperated
intheresearch. The nurse from the IntractablcDiseases
Information
Center
continued heractual interventions.We analyzed the datausing the grounded theory
approach. Grounded theoriescreate concepts by
mak-ingcompEll:isons of multiple data.
Since
thisresearch analyzed thedataof several personswho were involvedwith a single case thisisnot exactly a groundedtheory.
However, groundedtheoryfocuseson the process and
interactionintheprocessof bui]dingtheory. Sincethis
research aimed todiscussthechanges intheinteraction
among the patient,her family and spccialists, the
analysis using grounded theoryseems releyant.
AccordingtoStrauss"to bring
proccssintoanalysis
isan essential featureof a grounded theory analysis"
(Anselm
L. Straussand JulietCorbin 1990-l999,p.157);"By
process we mean the linkingof sequences of actionfinteraction as they pertaintothemanagement oL control over, or responsc to,a phenomenon. This linkingof sequences isaccomplished by noting;
(a)
the change inconditions influencingactionAnteraction over time;(b)theactionlinteractional response tothat
change;
(c)
theconsequences thatresult from thatac-tionfinteractionalresponse; and finallyby
(d)
describinghow those consequences becornepartof the conditions
influencing the next actionlinteractional sequence."
(Anselm
L. Strauss and Ju]ictCorbin 1990-1999,p.143).Inthe revised M-GM
proposed
by Kinoshita he doesnot fragmentdatabutemphasizes the importanceof understanding the context and examines theperson's
perception,action and cmotions reflected inthedataas well as related factorsand conditions
(Kinoshita
2003,p.158).
Thisresearch examines the processof changes in
thepaticnt'spsycho]ogyfollowingthe course of time
fromthe onset of herdisease,and itsdiagnosistoher
decision-making regarding preferencesconcerning mechanical venti]ation and itisconsidered that
evuluat-ingtheeffectiveness of
professional
support fromtheviewpoint of the patientispossibleby investigating
whether the outcomes
(changes
inthe patientand herfamily)havebeen obtained as spccialists planncd.as a result of thechanges intheconditions produced bythe
support of specialists.
Inpublicizing thc dataanalysis, the contents were confirmed and approved bythepatientand her family.
111.
Results
Four categories were identifiedas thecause of the perceptualgapintheprocessof decision-making bythe
paticntregarding theuse of mechanical ventilation. As
faras herrelationships with specialists are concerned, there was a gap between the informationwhich the
patientand her family desiredand theinformation
provided by specialists. As for the family,'therewas no sharing of theissuesby the familymembers. There
was also a
perceptual
gap between the patientand herdaughtersarising from theirmother's perceptionof her
disability,which she didnot want to expose to other
people.In addition, thcrewas a pcrceptualgapamong
thethreeparties;thepatient,daughtersand speciulists,
interms of theirperspectivesconcerning the present
and future.The
fo1]owing
isa dctaileddiscussionof theinteraction among thepaticnt,herfamilyand specialists
in
thesefourcategories.-29-1. Informationdesired by the patientlherfamiiy and jnformation
provided
byspecialistsThree yearselapsed until Ms. A was diagnosed as suffering from ALS since she began to feelthat
something was wrong with hertongue,The perceptua]
gap duringthis period between the patientand her
familywas that,while thepatientwas seriously worried
about thesymptom, herfamilydidnot takeitseriously.
InJanuary2001 she saw a neurologist at Hospjta]A
and was hospitalizedinMay formedical examinations.
Her family,who had not taken itvery seriously, was
totallyperplexedwhen the patientwas unexpected]y
diagnosedas suffering froman incurableditiease.They were even more confused becauseoftheway the
physi-cian infonmedthe patientof the disease.Inspite of the
serious matter of lifeor deathforthe
patient,
herphysi-cian gave her a
brief
one-sided businesslikenotice,while ignoringherfamily'sfeelings.Furthermore,the providedinfbrmationwas insufficient,with no specific
detailedexplanation about mechanical ventilation. He only mentioned thathedidnot recommend itbecauseit
involvedmajor burdens.
The patient'sdaughtersgatheredinformationfrom theInternetbecausethey hadno knowledge about the diseaseor the lifeof ventilator-supported patients.They
learnedfrom the Internetabout theapproach toinfbrm patientsof the diseasestep-by-step and asked the physician tofollowthestep fortheirmother. However, the physicianonly offered a choice of either inforrning
herof the
diagnosis
or not. He didnot give a detailedexplanation toMs. A,Afterall, herdaughters explained
to their mother about the diseaseand mechanical
venti]ator support. Almostno informationwas provided
by the physicianeither when Ms. A went to see him
foran examination as an outpatient. Because of the
gap betweentheinformatien providedbythe physician
and the informationwhich theptitientand herfamily wanted, they losttrustinthe physician and began to
look fora goodhospital.They wanted to finda hospital which would providegood emotional care
in
helping
Ms.
A
decide
whether touse a mechanical ventilator ornot.
Followingtheirsearch thefamilymoved Ms. A to HospitalB,which hada goodreputation, Thishospital
providedmedical informationaccording tothepatient's
con-ditionas well as informationon livingwith ALS .When
Ms. A was hospitalizedfor exarninations at Hospital B
hernew physicianfbundtheneed of ventilatory support
forherinthenear futurebecauseof the progression
of bu]barpalsy.He firstconfirmed thefamily's
prefer-ences concerning theuse of mechanical ventilation and
gaveadetailedexplanation tothem and thepatient.The physicianmentioned that he had explained brieflyto
Ms.A about mechanical ventilation and thatherinitial
response was "I do
not want to live
(with
ventilatorysupport)" and "I
can finishnow."
Ms. A'schief
physician
at HospitalB arranged avisit with an ALS patientforMs. A, her husband and
daughterstoprovidethem with informationon living with ALS. The ALS patienthad bronchotomy but refused mechanical ventilatory support, The patient's
fourlimbs were mostly paralyzedand needed total
care. Her husband, who was taking care of hiswife, said inherpresence"I
cannot sleep at al1."This gaye
Ms.A'shusbandan impressionthatthecare would be a
heavyburden.The nurse fromthe IntractableDiseases InformationCentersaid thatMs.A'shusbandprobably
had an image of home ventilation as equal toattending
toal1herpersonalneeds and thathewould not beable
tedo it.One of thedaughtersliyingseparately from
theirparentstook positivelywhat the husband of the patienttheyvisited said. Shefbunditnecessary tohave
a relationship inwhich caregivers can feelfreetosay
anything and accordingly thatthepatient
does
not feelhurtby that.Similarly,regarding theinformation on
the lifeof the patientwith ALS they visited, Ms. A's
husbandhadan impressionofprovidingcare as a heavy
burden, while hisdaughters had a strong impressionof
thefamilywhose relationships were so open thatfamily members could say anything toeach other. Thus, there
was agap intheway theyprocessedthesame
infbrma-tion,
When Ms. A was discharged from Hospital B a
framework which would make ongoing care possible
both at the speciaLty hospitaland herhome was structured. The informationobtained bythe nurse from
theIntractableDiseasesCenter,the visiting nurse and
the healthnurse duringtheirvisittothepatientat home
-30-NII-Electronic Library Service
was deliveredto the patient'schief physicianat the
specialty hospital,and thehospitalinherneighborhood and the specialty hospitalwere collaborating with each other todealwith emergencies. The nurse from the
In-tractable Diseases Centerwas working closely with the patlent'schief physicianat the specialty hospitaland its ward nurse and shared infbrmationalso with home-care
service providers
(Fig.
1). .- -'.---..---L.----..---'1'',1lt,! t. Nursein Charge of"patlent
IntractableDiseasesInformationCenter
N
"
Jxf
]i}xfF
SpecialtyHospitalo
m
VisitingNurse)NNX
Figure1SocialNetworkaround Ms.A 2. Sharingofthe
issue
bythefamily:interventions
in
theproces$of self decision-makingforhomeventilation
Ms. A,who was running a shop with herhusband,
feltuneasy with herfamilywhen she was not able to
work any longer.Shebegan to sleep ina separate room
fromherhusbandbecauseshe didnot want todisturb him when he was tired from the day'swork. During
thatperiodherbulbarpalsyprogressed,making verbal communication almost impossible,and there was a
dangerof choking with phlegm stuck inthe throat. Because herconsideration forthe familymight lead
to an emergency the visiting nurse urged the couple to
sleep within an area inwhich she could reach out her arm togiveherhusbandasignal ifan emergency arose
likechoking with phlegm. The nurse also toldMs. A thatintheevent that aworst situation occurred because
she was not able towake him up, hewould bethe one
who suffered remorse,
Laterwhen Ms. A's swallowing functionbegan to
decline,an accident happened.Her tabletsgotstuck in
herthroat.The visiting nurse asked Ms.A'schief physi-cian atthespecialty hospitaltoconfirm herpreferences
conceming the use of home ventilation topreparefor
emergencies. SinceMs. A's hospitalizationhad been plannedtochange the gastriccannula herchief
physi-
cian at HospitalB decidedto take the time to discuss
the matter with Ms, A whi]e she was hospitalized.
In order to provideher with information regarding the ventilator dependent ]ifehe arranged a visit toa ventilatory supported patientwith ALS beforeMs, A
was hospitalized,
During her firsthospitalizationat HospitalB when she was given an explanation abeut mechanical yentilation, she revealed herpreferencenot touse itfor
the firsttime.Her daughterstoldtheirmother thatthey wanted hertouse it,butshe refused. Sincethen Ms.
A and herfamilystopped ta]king about it.Forsome
time,after she was discharged
from
thehospital,
thetopic was taboo forthe family,However, due tothe in-terventionsmade bythe specialists, thepatientand her
familybegan tothink individuallyabout mechanical
ventilatory support, butdidnot share the issueamong
themselves, Ms. A
did
not confide herworry tothemeither.
The nurse fromtheIntractableDiseasesInformation Center,inspiredby the visiting nurse and the interim
analysis of thisresearch, begantomake interventionsto
helpthepatient make herown decision.To begin with,
she confirmed with Ms.A and herfamilyattheirhome
concerning herpreferenceswith respect tomechanical
ventilation. Her daughterswanted theirmother touse
itand were prepared to support heronce she decidedto
doso.
When thespecialists began to beinvolvedinher decisien-makingprocessMs.A'shusbandshowed more
interestinthe non-use of a ventilator. He asked the followingquestionstothe author infrontof hiswife: "I
want tohearwhat thecaregiver of a patientwith no
venti]atory support hastosay" and "Would
she suffer
more when she isdyingifshe was not supported bythc
ventilator?" When herhusbandwas not with herMs. A said, "My husband does
not want me to use a
ventila-tor."However,herhusbandsaid when hewas not with
her"Maybe,
itwould bebestfbrhertouse it."
Her husband, who had a strong impressionof
heavy care burdenswhen he and hisfamily visited a
patientwith ALS forthe firsttime,was not positive about home ventilation
because
hethought that,basedon herpersonality,hiswife would not need it.He also
said at the beginning that hedid not know much about ventilators. However, basically,hedidnot show much
interestingettinginformationsince hedidnot have much time toread allthematerials hisdaughtersgave
him.Hisknowledge about thediseaseand care was
biased.Therewas a gapinhisperceptionof thedisease
with that of hisfamily,and hehadlittleinterestinit.
The second patientwith ALS, who Ms. A and her
familyvisited, originally didnot want touse mechani-calventilation, butwas persuadedtodoso byher
fam-ily.When Ms.A and herfamilyvisited the firstpatient
beforethispatient,Ms. A'shusbandhada strong image
ef
heavy
care burdens.Therefore,an ALS patient whostM had some mobility was chosen for their second
visit.The caregiver ofthispatientsaid toMs.A and her
familythatitwas goodthatshe decidedtouse a
yen-tilator,and thepatientgave a smile. Ms.A feltthatthe caregiver's attitude must bea bigrelief forthe patient.
As Ms. A's husband's image of ventilatory-life changed
through hisobservation thatthe ventilatory-supported
patientseemed tobemoving forwardwith enthusiasm and thatherfacialexpression lookedbrighterthan the patientwithout such support, hebeganto thinkthathe
would regret itifhe didnot tethiswife use it.
Afterthe visit tothe patientwith ALS, Ms. A's
husbandasked hiswife ifshe wanted touse mechanical
ventilation, butitwas a one-sided question fromhim.
As a resu]t, there was no clear response from her.
However, when herhusband saw a mechanical
ventila-torforthe firsttime hewas encouraged by the nurse
fromthe IntractableDiseasesInfbrmationCentertoask
a question,and hisquestion changed to a more specific
one about her actual ventilator dependent life.The nurse frorntheCenterasked one of her daughtersifshe
had ever imaginedhermother's ventilator dependent
life,after which thedaughteractually beganto have a
clearer imageof the placement of hermother's bedand
furniture.
Ms.A said shehad
notdiscussed
homeven-tilationwith herfo11owingtheir visit to the
ventilatory-supported patientbutsaid thatshe hadheardfromher
husband that theirdaughterswere talkingabout buying acar which could accommodate herwheel chair.
When the specialists began tobe involvedwith the processof Ms. A's decision-makingone of her
-32-NII-Electronic Library Service
daughters,who was livingaway from home, encour-aged hermother toexpress herpreferences regarding
home yentilation. When the familyvisited the first patientwith ALS, the daughterfeltthat herfamily
should shure the issueamong themselves and thought
that the topic shou]d not bespecial so thatthey could
talkfreelyabout it.When she yisited herparentsshe asked Ms. A about home yentilation while they were carrying on an ordinary conversation. At that time the questionwas posedonly fromherside, and there
was no response fromMs.A.However, this ledherto
express herpreferencestoherdaughterwho livedwith
her:"When
she
(daughter
livingseparately) asked me about the ventilator Iwas not able toanswer properly,butIwant to live."Actually,Ms. A decidedtouse
me-chanical vcntilation when thespecialists begantomake
interventionsand her physicalconditions were not as
good as they were beforethefamilyvisited thesecond
ALS patient.Afterheryisit tothe second patientshe
said, "That
was what Ihadimagined.Nothing changed
(in
termsof herfeelings)i'During her second hospitalization her chief
physician at HospitalB met with Ms. A toconfirm her
preferences
concerning mechanical ventilation. Duringthe meeting Ms. A said, "I
want touse the ventilator
as ]ongas Ican remain mobilej' Her
feelings
changedfromthefirsttime she expressed herpreferences,Since Ms.A'sbulbarparalysiswas progressingmore rapidly
than that of her four limbs itwas quitelikelythatshe would use the ventilator while she remained mobile.
However, thequestionremained as towhat should be
donelaterwhen herfourlimbsbecame immobile. Ms. A said the possibilityof using the ventilator would be
fiftypercentifshe became immobile.
Atthemeeting with the specialists and the family,
they triedto share Ms. A'spreferences. However, duringthe interviewat a laterdate itwas found that
Ms. A'sdaughtersand her
husband
didnot confirmherpreferencesdirectlywith her.Also,after the
meet-ing,the nurse from the IntractableDiseases Center received the informationfrem a ward nurse thatMs.
A was doubtfu1regarding what herfamilyhad said. In
order to coordinate with her family,the nurse fromthe Centerobtained permissionfrom Ms. A and confirmed
with herfamily concerning theirpreferencesat home.
Her husband said "I
would regret itifmy wife died without mechanical ventilation, so Iwant herto use
it."Herdaughterwho livedwith them said, "I
want her to continue tolive"becauseshe feltlonelywhen her mother was inhospital.The nurse fromthe Center told
Ms. A thatshe was needed byherfamily.Ms. A held the nurse's hands and cried.
3. Perceptionofdisability
Ms. A'sperceptionof herdisability,which she did
not want exposed to other people, had a major impact on herunderstanding of the disease,and herhusband
had a similar perception.SinceMs.A fbunditdifficult
tocommunicate with other peopleshe hatedtoexpose
herselfto them and didnot want tobetalkedabout. As
a rcsult, she began towithdraw herse]fand said, "If I must d¢pendon a mechanical yentilator Iwant to goto aplacethatnobody willknow" and also said "I
want to
die
(in
obscurity) ]ikean elephant." Her daughters feltambivalent becausethey wished theirmother to live longerand at thesame time were uncertain whether she would be truly happy todependon ventilatory support,
givenherperceptionof disabilityas a disgraceas well as herfeelingsabout continuing to 1ivcwhile remaining
immobile.They ]cftthe decisionto theirmother and
didnot pushhertomake herown decisionconcerning
medical procedures,considering thatshe would not be able tomanage the situation unless she had a wM to
liveand thatthey would accept itifshe decided against
theuse of mechanical ventilation.
There was a gap inthe perceptionof disability
betweenMs. A and herdaughters.Ms.A didnot want
toexpose herselfina wheelchair toother people.while
her daughterswanted herto go out even with
ventila-torysupport. Herdaughtersulso wantcd hertocontinue
tohave contact with thecommunity and wanted her
neighbors to helpherwhen she was on mechanical
ven-tilation.They thought unless she could livepeacefully surrounded by herneighbors her ventilator dependent
lifewouLd bcdepressing.Theywere anxious about their
mother who could not beopen about herself.When the
whole familydiscussedmechanical ventilatory support
hcrdaughterstoldtheirmothcr that they were womied
-33-about herusing theventilator, while beingunwilling to
expose herselftoother people.The daughterwho lived separately said to hermother as she was leavingfor another room while herhusbandwas visiting thehouse,
"There's
no meaning inusing the yentilator ifyou do
not findthe
joy
of watching your grandchild runningaround the room while you are lyinginbed.Thatwill make youfeelworse." However,Ms.A didnot respond
toherdaughter,and itending up as a one-way
com-munication. The nurse from theIntractableDiseases Centerfeltthe distancebetweenMs.A and herfamily.
When Ms. A and her familyvisited the second
patientwith thesame diseaseherhusbandsaidhonestly
tothecaregiver of the patientthathedidnot want to expose hiswife's disabilitytoother people.The patient' s caregiver said that nothing would beginunless they accepted the reality. The nurse from the Intractable DiseasesCenterfeltthatthecaregiver made a differ-ence forMs. A and herhusband,who didnot want
the disabilitytobeexposed. The caregiver's comment
triggered change inMs.A'shusband'sperception.Later
hesaid: L`I
would beopen about thesituation ifmy wife
becamebedridden"and "1
won't beable tomanage this
unless Iletitallout intotheopen ."
Accordingtothe visiting nurse, the facial expres-sion of the daughterlivingwith herparentslooked
gloomy when thenurse began visiting the familyand she would reconfirm several things with the nurse
concerning the medicine prescribedto hermother, but after the meeting herfacetook on a brightlook and she
no longerreconfirmed about the medicine. According
tothe healthnurse, Ms. A used toexpress herselfas a source of troub]e forherfamilyand didnot express
herwish to live,butafterthe meeting she beganto say she wanted to live.Early on, Ms. A'shusbanddidnot
appear himselfeven ifhe passedthe room where the
healthnurse was visiting hiswife, butafter Ms. A's second hospitalization,hechanged and spoke tothe healthnurse asking, "How are things?"
Her husband used tosay, "I
don'tthink my wife will use ventilation;' buthisattitude was differentafter
the meeting when hiswife was hospitalized forthe second time.He said: "I
would regret itifshe didnot
use a ventilator;' and "Nobody
wants todie."However,
hisdaughtersfeltthattheirfatherhad said hewanted
hiswife to use mechanical ventilation becausehewas overwhelmed by hisemotions, while they were still ambivalent about the use of yentilation becauseof their
mother 's
perceptionof disability.
4. A
perspective
focusing on the present and a
perspective
focusing
on thefuture
When Ms. A entered HospitalB forexaminations
thefirsttime,she was recommended byherchief
physi-cian tohave tracheostomy and PEG, butshe refused
to have bothof them. Her familywas still unable
to make their finaldecision concerning mechanical
venti]ation, however,as theysaw herbecoming physi-cally weak and losingweight, thedaughterssuggested
PEG, expecting hertomaintain herenergy byfeeding
nutrition intothe stomach. Thus,they encouraged her
tomake a decision regarding the medical treatment
procedures.However, they didnot pushherto make a
decisionregarding theuse of mechanical venti]ation as
she refused touse it.RightafterMs.A begantoreceive
home care she and herfamilydidnot touch upon me-chanical ventilation. Since she was able to speak and to write she was givenan explanation about an apparatus
forcemmunication, butshe didnot practiceusing a
personalcomputer.
The visiting nurse assumed thattherewas another
barriertotackle concerning the use of home ventilation,
Shethought itwould beimpossibleforMs.A toaccept
herdisabi]itybefbreshe actually facedthereality ofher situation. She considered thatMs. A would overcome the barrierby facingthe reality, and also thatitwas
important forthe familyto wish fbrherto survive by
allmeans and thattheir
feelings
must synchronize withherwish tolivewith herfamily.
IV.
Discussion
1. Issues concerning interactionamong famjly
members
Ms. A'sdaughtersexpressed their willingness
te support theirmother inthe event she chose home ventilation. However, she hadnot beenable toexpress
-34-NII-Electronic Library Service
herwish to
live.
Itissaid thatfamiliesand social va]ues affect the
patients'decision-makingregarding the use of
mechani-cal ventilation. The primary issueforthefamilyinthis research was thatthe family members didnot share the problems resulting fromthepatient'sillnesswith each
other. Despitethe family'scritical situation Ms. A had
not expressed what she hadinmind toherfamily.Her daughterwho livedseparately from herparentsfeltthat unless the familymembers could say openly to each
other what they thought,they would not beable toface thiskindof difficultyand she wanted herparentsto
beopen with each other. She wanted to builda family
relationship, which enabled them totalkabout thiskind
of problemintheirdailyconversations.
The second issuearose from the couple's percep-tion of disability.Both husbandand wife hada strong
feelingthatthey didnot want theirneighbors toknow about herillness.Ms. A said she wanted to
die
(in
obscurity) likean elephant. They were sti]1 influencedbytheold social values thatprevailedinthedayswhen
personswith disabilitieswere not able togoout of the houseoftheir own freewill.
The daughtersleftthe decisiontotheirmother
because they were uncertain whether she would be
happy touse mechanical ventilation considering her
perception
of disabilityand because she didnot wantto be exposed to other people'seyes. Ms. A at first
refused to have PEG butfinallyagreed tohave it with herdaughters'encouragement. However, there was no pushbyherdaughtersabout herpreferences
concerning mechanical ventilation, Itisoften difficult to make a decisionwithout a pushbythefamily.as the patientmust depend on hisfherfamily'scare to live with mechanical ventilatory support. Social values
which impose responsibility on the patientfortheir
selfdecision-rnakingaffect the fami]y,Inthisregard,
Ms. A'sdaughtersmight
feel
thatthey could not take fu11responsibility forthe possibilitythattheirmothermight regret herchoice regarding home ventilation.
Furtherrnore,herhusbanddidnot push hertochoose it either. However,not a few patientshave chosen home ventilation becausetheirspouses took theillness
seri-ously and assumed theinitiative,saying, "This istough
butlet'swork together;'and, "I
want you tolive."Ms. A'shusband thought initialLythathiswife didnot want
touse a ventilator, and hiswife, sensing his
feeling,
thoughtthathedidnot want her touse it.
One of thekeyelements infacilitatingself
decision-making issaid to bethe family.Ms.A'sfamilystrongly
wished
her
tolive.However, since herperceptionof disabilityand not wanting tobeexposed to other
people'seyes didnot change, herdaughters'ambivalent
feelingsremained unchanged.
2. Interventionsby specialists concerning
mation
Itissaid thatphysiciansshould gjvepatients
medi-cal informationina neutral and fairmanner including
themerits and demeritsof using mechanical ventilation
instages as early as possible.Itisalso said thatthey
need to explain to the patientsthatthe care wilL be
provided en a continuing basis,and thatdependingon
their preferencesan explanation rcgarding palliative
care willbenecessary. Ongoingeducation isnecessary
becausepatientswaver emotionally.
The physicianat Hospital A expressed hisopinion that he didnot recommend mechanical ventilation
befbregivinga detai]edexplanation of ittothepatient.
There was a bigdit'ferencebetween hisexplanation
and the informationthepatientand her
family
wanted.The physician'sattitude aroused the family's mistrust
inhim.Afterthe patient and herfamilyreceived an
explanation at Hospital A, her family asked forrnore
informationabout the illnessand other information
which would helpthem to havea clear pictureof her
lifeafter she was puton a mechanical ventilator and
also asked forongoing care. The physician'sattitude in
givingmedical informationand theamount
ofinfbrrna-tionprovidedwere very differentbetweenhospitalsA
and B.Hospita]B arranged a yisit with another patient with the same diseaseforthe purposeof providing
informationabout the patient'slifeathome, and when
thepatientwas goingtobedischargedtheyorganized a
social network or ongoing home care with the specialty
hospitaland the IntractableDiseases Information Center.Itissajd that an explanation concerning pallia-tivecare
is
also necessary inthissituation, butinthese
hospitalsthere was littleinformationon palliativecare
forthepatientswho donot ehoose mechanical ventila-tion, Ms. A'shusbandasked the author about deathin
the event hiswife didnot choose mechanical
ventila-tion.Also,hewanted tohearfromthe caregiver of the
non-ventilatory dependentpatientabout hisfeelings.
Itseems necessary togiveinformationconcerning the
merits and demeritsof using mechanical ventilation as well as itsnon-use fromtheperspectiveof the patient's
family.Particularly,inthe event thatthe patientdoes
not use it,itisquite]ikelythat their familywill regret
it.Itisobvious thatthepatientwill need palliativecare
ifthey refuse mechanical ventilatory support, while at
the same time grieftherapy will benecessary forthe family,
Because each individualhas his/herown sense
of va]ues itisquitenatural thatpeoplehavedifferent perceptionsof thesame information.Afterthefirstvisit
tothepatientwith thesame disease,thedaughterliving
separately from thefamilyappreciated the re]ationshjp
between thecaregiver and the patient inwhich they could say open]y toeach other what was on theirmind,
positiveLy.Ms. A'shusband was struck by the heavy
care burdenand said hedidnot thinkhiswife wou]d
use a ventilator. Ms. A sensed herhusband'sfeelings,
which probably preyented herfromexpressing herwish
tolive,Therewas a small gapbetweenherhusband's
perceptionof the diseaseand thatof the specialists
and hisfamily.However,hisperception of the disease
changed through the interventionsbythe visiting nurse
and thenurse fromtheIntractableDiseasesInformation
Center,buthisand hiswife's perceptionof disability
didnot change. Therefbre,theirdaughterswondered if their mother wou]d bereally happyto havemechanical ventilation, feelingthat she didnot want to expose
herselftoother people'seyes, which was rooted inher
perceptionof disabilities.As a result, the ambivalent
feelingsof herdaughtersremained unresolved. Itis
possible to bridgethe gap inthe perceptions of the
informationgiventothepatientand her familythrough
continuing education by specialists and to solve the problemswhich resu]ted
from
thegap.However, itisnot easy tochange theirvalues.
Itisnecessary to
give
informationwhile takingintoconsideration the relationships among medical care practitioners,patientand family.At the beginning
Ms. A and her family avoided the topic concerning
mechanical ventilation and each of them was worried
about itindividually.The nurse from theIntractable
DiseasesInformationCenterserved as a coordinator
by listeningtowhat Ms. A and herfamilyhad to say
together as well as listeningto them individually.In
addition, arranging visits forMs.A and herfamilyto patientswith the same diseaseand providingthem with opportunities totalkwith thephysicianabout mechani-cal ventilation duringherhospitalization,ledherand
herfamilytoseriously consider itsuse, Dependence on mechanical ventilatory support means imposingcare
burdens on the patient'sfami]y.Itisdifficultforthe patienttomake decisionsifthefamilymembers cannot share the issueswith each other and reach a consensus
even ifinformationhasbeengiventothem individually. Specialistsneed to faeilitateinteractionarnong family members besidesprovidingthem with information,
One of thefactorswhich make the patients'
deci-sion-making regarding mechanical ventilation difficult
isthatthey must decidenot about thepresentsituation
butabout theirfuturecrisis. Particularly,at the stage at which theirdisabilityhas not yetturned worse they find
itdiMculttoaccept the informationthatthey will need ventilatory support inthefuture.They may beable to
absorb itonly when they facethe crisis. Specialistsurge
the patientsto make decisionsbyprovidingthem with
information inadvance inorder to formulate
appropri-ate measures forthe futurecrisis which isinevitable.
There isa major gap between the perspective of
patientsforwhom theirfutureisinconceivable,as they
are so overwhelmed bytheirpresentcondition thatthey
do not want to see what the futureholds,and thatof the
specialists who want tooffer support byfocusingon the future.Forpatientswith ALS, itissaid thatcontinuing
education appropriate foreach
progress
of the disease isnecessary. However,unless support isoffered, whilerecognizing thegapbetweentheseperspectiyes,thegap
of
perceptions
between the patientsand medical carepractitionerswill remain unchanged.
This article hasdiscussedprofessionalsupport
focusingon the
gap
ofperceptions
as itskey words.-36-NII-Electronic Library Service
Sincethisresearch dealswith only one case, theauthor
must be prudent in concluding itsoutcome as the
concept of support forpatientswith ALS ingeneral.In
addition, thisarticle dealswith a patientwho hud little contact with theALS patientssupport group and other
patientswith thesame diseasebutwas mostly involved
with specialists. Therefore,theauthor planstomake comparative case studies of patientswho have more
contact with othcr patientswith thc same diseaseand
patientswho have littlecontact with specialists.
V.
Conclusion
One of the factorswhich makc the patientsiself
decision-making toward mcchanical ventilation
difficultisthe social factorthat the decisiondepends
on the capacity of their familics toprovidecare and that itisa decisionnot ubout thepresentsituation but
about thefuturecrisis.There isa biggapbetweenthe
pcrspectivesof thepatientswho havenot accepted thcir
presentreality or donot want to see what the future
holdsand thosc of specialists who trytosupport them
with a focuson the
future.
Inthisregard, support mustbe providedwhile recegnizing thesegaps.
Educational information and the attitudes of
physiciansplayimportantroles inthe
decision-making
processof patients.Information should be provided
focusingon mechanical ventilation as well as the
merits and demerits of itsuse and non-use. However,it
should begivenbothfromthepcrspectiveof thepatient
and thcirfamily.Sometimes familymembers
do
not share theproblemswith each other even ifeducationalinformationhas been providedtothem and thepatient. Specialistsshould givesupport tofacilitatcinteraction between thepatientand hisfhcrfamilymembers and encourage them to reach a consensus, not simply
provideinforrnation.
Inthe casc of Ms. A some of the problems,which
resulted from the gap of perceptionsconcerning
information,werc so]ved through the continuing
involvement of specialists.Inorder tobeab]e to accept
disability,patientsneed to change their values
(Wright,
1960),butinthisparticularcase ithasnot happened
yet.Because of this the problems arising from the
differentvalues remained unsolved. Exploring an
ap-propriateformof support was the immcdiatechallenge
so thatthepatientwould not regret her decisionto use
mechanical ventilation.
Notes:t)
The IntractableDiseases Information Centerisengaged in
the promotionot'comprehensive home medicul care
ticesinc]udingmedical carc practicesat home,consultation, trainingformedica] care practitionersand researeh, with rhe
main focuson improvement of the patients'care ment through enhancing thecoordination of institutienal
care and homc rnedical care forintractablediseasepatients.
Bibliography
Albert, S.M., Murphy, P.L,and Del Bcne M, L.,et al.(1999), `"A prospectivcstudy of preferencesand actual treatment
choiccs inALS;' Nettrolog.v,53(2),pp.278-83
Anse!m, L.Straussand Juliet.Corbin (1990),Basics of
euaiitativ('Research:Grounded 7:PteorvProceduresand
7bchnique, New York.Sage Pub]ications,Inc.
Felix,P.Biestek,S.J,(1957),The Casework Relationship,
LoyolaUniversity Prcss
Kamo, N,(1998)."Philosophy
of ContcmporaryBioethicsl-1;'
Kato, H. and Kamo, N..eds. Introductionto Bioethics, SekaishisoshaCo.,Ltd.pp.3-13.
Kent, M. A.(]996),'CTheethical arguments concerning the ficialventilation of patientswith motor neurone diseasc;' NursingEthics,3(4),pp.317-28.
Kinoshita,Y, C2003).Grounded 71teor.vAlrproach.Koubundou
PublishersCo,,Ltd.
Kojima, A. (2002),"Who
makes the dccision?:Responsibility
and ambivalence of support providers;'Furukawa, K.,
Iwasaki, S.,Inazawa,K.,et al,7?toughts'on Sociat
port:Lkit{eBase
of
VVkiijlareSociet},,YUhikakuPublishingCo,,Ltd.,pp.209-256,
Mttrk,B. Bromberg and Dallas.A. Forshew, et al. (1996), "Ventilator Dependency inALS: Managemcnt
Disease
Progrcssion and Issuesof Coping,"Jourftaiqf neurotogic' rehabilitation. 10 (3),pp,195-216.
Moss. A,H.,Casey.P.and Stocking,CB., et al, (1993)"Home
ventilation foramyotrophic lateralsclerosis patients: comes, costs, and patient,fami]y, and physician attitudes;' NeLtrology43(2),pp.438-43,
Shimizu,T.,Kitamura.Y.,Tsuchiya,Y.,etal(2001),"Inl'ormation
regarding mechanical ventilatien providedbyphysicians
with ALS patients and reasons for dccision-making," Rct)orton Researchon lnu)roventent
of
eOL.forPatients",ith SPeciji'edDiseases, 2000, pp.196-203.
Smyth.A.,Riedl,M, and Kimura,R,et al.(1997)"End
of life
decisionsinamyotrophic lateralsclcrosis: a cross-cultural perspective;'Journal
of
NeurologicalSciences,p.152.S93-6.
Socjetyof Preventionund CareManagement of Incurable and ChronicalDiseases(2003).Outline
of
PreventionandCare Mdnagement qfIncurahte and ChronicatDiseases, TleilyoBljutsuPrintingCo,,Ltd.
Societas NeurologicaJaponica(2002),Ti'eatmentGuidelinesof
theJopaneseSociety
ofNeurotog.v
jp.orglguideline/,2004.12.1).