N
europathic pain caused by a lesion or disease of the somatosensory nervous system presents a sig- nificant burden to individuals and society, as it is typically difficult to obtain sufficient analgesia with phar- macotherapy. The results of several studies of conditionedpain modulation suggest that patients with neuropathic pain have decreased ability to recruit endogenous analgesic mechanisms.1,2 Descending noradrenergic inhibition origi- nates in the locus coeruleus (LC) and suppresses nocicep- tive signals from primary afferents to the spinally projecting neurons.3 Descending noradrenergic inhibition comprises an important element for endogenous analgesia, and is reported to be attenuated over time after nerve injury in a rat neuropathic pain model.4–6
Antidepressants are often used to treat neuropathic pain. In particular, serotonin noradrenaline reuptake inhibi- tors (SNRIs) are considered first-line therapeutics,7 but the mechanisms underlying their analgesic effects are unclear.
Previous studies in a rat nerve injury model demonstrated that a single administration of SNRIs increases the level of noradrenaline in the spinal cord.8,9 This suggests that anti- depressants inhibit neuropathic pain by facilitating the descending noradrenergic inhibitory pathway in the spinal cord. Therefore, we hypothesized that analgesia obtained by repeated SNRI treatment is achieved through reactivation
ANE AAJ
Anesthesia & Analgesia 0003-2999
Lippincott Williams & Wilkins
10.1213/ANE.0000000000002380 AAJ-D-17-02254
Effect of Repeated Duloxetine for Neuropathic Pain
XXXXXXXXX XXX
XXX
00 00
July52017 2017
Anesth Analg
XXX XXX
2017
BACKGROUND: Antidepressants are used to treat neuropathic pain and although the detailed mechanisms of their effects are unclear, the descending noradrenergic inhibitory system might play an important role. We tested our hypothesis that repeated administration of duloxetine sup- presses neuropathic pain by restoring the descending noradrenergic inhibitory system in rats 6 weeks after spinal nerve ligation (SNL).
METHODS: We subcutaneously injected SNL rats with duloxetine (10 mg kg−1 day−1) daily for 3 consecutive days and assessed behavioral hypersensitivity and noxious stimulus–induced analgesia (NSIA) activated by subcutaneous injection of capsaicin. We also performed microdi- alysis studies of the spinal cord, noradrenaline measurements of homogenized lumbar spinal tissue, and immunohistochemistry of the locus coeruleus.
RESULTS: Three daily injections of duloxetine attenuated the mechanical hyperalgesia induced by SNL (SNL treated with vehicle: 88 ± 9.4 g versus SNL treated with duloxetine: 148 ± 13 g, P < .001; estimated treatment effect of duloxetine [95% confidence interval {CI}], 65 [50.6–79.4]; n = 6/group, on day 4) and recovered the decreased NSIA (vehicle: 154 ± 10 g versus duloxetine: 213 ± 33 g, P < .001; 71.3 [57.4–85.2]; n = 6/group, 30 minutes after injection). The noradrenaline content in the dorsal spinal cord increased bilaterally (SNL treated with vehicle: 946.7 ± 203.6 pg/g versus SNL treated with duloxetine: 1593.5 ± 181.4 pg/g, P < .001; 646.79 pg/g [481.61–811.97] on the ipsilateral side; SNL treated with vehicle: 845.0
± 164.7 pg/g versus SNL treated with vehicle: 1557.2 ± 237.4 pg/g, P < .001; 712.17 pg/g [449.31–975.02] on the contralateral side). Intrathecal injection (IT) of the α2-adrenoceptor antagonist idazoxan reversed both the antihyperalgesic effect (before IT: 133 ± 5.7 g versus 30 minutes after IT: 85.8 ± 6.5 g, P < .001, −47 [−39.1 to −54.8], n = 6/group, and NSIA;
vehicle-IT: 219 ± 7.4 g versus idazoxan-IT: 153 ± 10 g, P < .001; −65.8 g [−25.2 to −77.4]
n = 6/group, 30 minutes after forepaw injection of capsaicin). Duloxetine treatment did not alter the noradrenaline release in the spinal cord after capsaicin injection (P = .415), or the frac- tion of nuclei positive for phosphorylated cyclic adenosine monophosphate response element binding protein in the locus coeruleus (P = 1.00 duloxetine versus vehicle 120 minutes after forepaw injection of vehicle and P = 1.00 duloxetine versus vehicle 120 minutes after forepaw injection of capsaicin).
CONCLUSIONS: These findings suggest that 3 daily injections of duloxetine suppressed hyperal- gesia and recovered impaired NSIA in rats 6 weeks after nerve injury. Both effects of duloxetine were reversed by IT of an α2-adrenoceptor antagonist. These findings suggest the inhibitory effects of duloxetine against neuropathic pain depend on recovery of the noradrenergic descend- ing inhibitory system, especially in the spinal cord. (Anesth Analg 2017;XXX:00–00)
AQ4
Jayachitra
Repeated Administration of Duloxetine Suppresses Neuropathic Pain by Accumulating Effects of
Noradrenaline in the Spinal Cord
Sachiko Ito, MD, * Takashi Suto, MD, PhD, * Shigeru Saito, MD, PhD, * and Hideaki Obata, MD, PhD † AQ1
From the *Department of Anesthesiology, Gunma University Graduate School of Medicine, Gunma, Japan; and †Center for Pain Management, Department of Anesthesiology, Fukushima Medical University Hospital, Fukushima Medical University, Fukushima, Japan.
Accepted for publication June 30, 2017.
Funding: The study was supported by Grants-in-Aid for Scientific Research (KAKENHI) from the Ministry of Education, Culture, Sports, Scientific, and Technology of Japan (No. 26670678 to H.O. and 25670664 to S.S.) and research grant from Eli Lilly Japan K.K. (to H.O.).
Conflicts of Interest: See Disclosures at the end of the article.
Reprints will not be available from the authors.
Address correspondence to Hideaki Obata, MD, PhD, Center for Pain Man- agement, Department of Anesthesiology, Fukushima Medical University Hospital, Fukushima Medical University, 1 Hikarigaoka, Fukushima, Fukushima 960–1295, Japan. Address e-mail to [email protected].
Copyright © 2017 International Anesthesia Research Society
AQ3
AQ2
PAIN AND ANALGESIC MECHANISMS
of the descending inhibitory system to recover endogenous analgesia.
In the present study, we subcutaneously administered duloxetine daily for 3 consecutive days to rats 6 weeks after L5 spinal nerve ligation (SNL). To evaluate the change in endogenous analgesia after repeated administration of duloxetine, we used noxious stimulus–induced analgesia (NSIA). NSIA is induced by a nociceptive stimulus, such as a subcutaneous injection of capsaicin, that subsequently produces analgesia at sites remote from the application site of the nociceptive stimulus.10,11 A recent study reported that NSIA is attenuated 6 weeks after nerve injury,6 and we there- fore assessed this time point in the present study. To evalu- ate the effect of repeated administration of duloxetine on SNL-induced hyperalgesia, we measured the withdrawal thresholds over time after injecting duloxetine and inves- tigated the noradrenaline content in homogenized tissue from the dorsal half of the lumbar spinal cord. Furthermore, to determine whether the effect of duloxetine was limited to within the spinal cord or extended to the brainstem source of descending noradrenergic inhibition, we also performed microdialysis in the lumbar spinal cord and immunostain- ing of the LC.
METHODS Animals
All studies were approved by the Animal Care and Use Committee of Gunma University Graduate School of Medicine. Male Sprague-Dawley rats (200–250 g, SLC, Shizuoka, Japan) were used and housed under a 12-hour light–dark cycle with free access to food and water.
SNL was performed as previously described.12 In brief, under anesthesia with isoflurane (2%) in oxygen, the left L5 spinal nerves were identified and cut after tight liga- tion using a 5-0 silk suture. The wound was then closed. We evaluated the rats 6 weeks after SNL for all experiments, as the descending noradrenergic inhibition is weakened at this time point.6,13 Sham operations were performed in the same manner without ligating the nerve.
SNL and sham-operated rats (6 weeks after surgery) were given a subcutaneous injection of duloxetine (10 mg kg−1 day−1) or vehicle (0.5 mL of 50% dimethyl sulfoxide) in their backs daily for 3 consecutive days. Duloxetine was dissolved in 0.5 mL of 50% dimethyl sulfoxide. Adverse behavioral effects, such as sedation or agitation, were care- fully observed and graded as 0 (normal), 1 (moderate), or 2 (severe). Motor function was assessed in terms of the plac- ing reflex and righting reflex with scores of 0 (normal), 1 (impaired), or 2 (absent). To evaluate the placing reflex, the hind limbs of the rat were held and the dorsal surface of the hindpaws was brought into contact with the edge of a table.
The experimenter recorded whether the hindpaws were placed on the surface reflexively. To evaluate the righting reflex, the rat was placed on its back on a flat surface and the experimenter noted whether it immediately assumed the normal upright position.
Assessment of Mechanical Sensitivity and NSIA The withdrawal threshold in response to pressure applied to the hindpaw was measured using an analgesimeter (Ugo
Basile, Comerio, Italy), as previously described.14 Animal training for this test was performed for 3 days before SNL surgery and resumed 1 week after surgery. A cutoff of 250 g was used to avoid tissue injury.
To examine the effects of duloxetine for mechanical hyperalgesia, the withdrawal thresholds to pressure applied to the ipsilateral (left) and contralateral (right) hindpaws were measured at time 0 (before duloxetine injection), and at 120 and 240 minutes after each duloxetine injection. NSIA was assessed according to the previously described proce- dure6,13 by injecting capsaicin (150 μg) into the right forepaw under isoflurane (2.5%) general anesthesia. The withdrawal threshold in response to pressure applied to the contralat- eral (right) hindpaw was measured. Capsaicin injection and NSIA measurements were performed approximately 24 hours after the last duloxetine injection to exclude any acute effects of duloxetine. Capsaicin was initially dissolved in Tween 80 (50%) and ethanol (50%) to a concentration of 50 µg/µL, and then diluted with saline to a concentration of 3 µg/µL; capsaicin was subcutaneously injected at a volume of 50 µL (150 µg) in all experiments.
To evaluate the contribution of noradrenaline in the spi- nal cord to the antihyperalgesic effect and NSIA, we injected the α2-adrenoceptor antagonist idazoxan (30 μg) intrathe- cally after 3 daily injections of duloxetine. The idazoxan doses were selected according to a previous study.15 For intrathecal administration, idazoxan was dissolved in 20 μL saline and injected into the L5-6 intervertebral space using a 30-gauge needle. The investigator measuring the withdrawal thresholds was blinded to the drug treatments.
Studies of the antihyperalgesic effects, NSIA, and idazoxan were performed separately in different groups of rats. After completing the experiments, rats were killed by intraperito- neal injection of an overdose of pentobarbital.
Microdialysis Studies
Microdialysis studies were performed in another group of rats, as previously described.16 Anesthesia was induced with isoflurane (3%) and then maintained with 1% to 1.5%
isoflurane in 100% oxygen through a nose cone. The left femoral vein was cannulated for fluid infusion or drug injections. The rectal temperature was maintained at 37°C to 38°C with a heating pad placed beneath the animal. The L4 to L5 level of the spinal cord was exposed by a thoraco- lumbar laminectomy, and then the rat was placed in a ste- reotaxic apparatus. After opening the dura with a 30-gauge needle, a probe (outer diameter = 0.22 mm, inner diame- ter = 0.20 mm, length = 1 mm; A-I-8-01; Eicom Co, Kyoto, Japan) was inserted from just lateral to the right dorsal root and advanced at an angle of 15° to 30° to a depth of 1 mm using a micromanipulator (model WR-88; Narishige, Tokyo, Japan). The microdialysis probe was perfused with Ringer’s solution (147 mmol/L NaCl, 4 mmol/L KCl, and 2.3 mmol/L CaCl2) at a constant flow rate (1 µL/min) using a microsyringe pump (ESP-64; Eicom Co). After 120 min- utes of constant perfusion, 2 consecutive samples were col- lected to determine the basal noradrenaline concentration in the dialysate (baseline). Then, 15-minute perfusate frac- tions were collected into an auto injector (EAS-20; Eicom Co). The noradrenaline concentrations in the perfusate were
analyzed by high-performance liquid chromatography with electrochemical detection using an HTEC-500 analyzing system (Eicom Co). The chromatographic conditions were as follows. The mobile phase comprised 0.1 mol/L ammo- nium acetate buffer (pH 6.0), 0.05 mol/L sodium sulfonate in methanol (7:3 vol/vol), and 50 mg/L Na2-EDTA. The col- umn was an EICOMPAC CAX (2.0 mm × 200 mm; Eicom Co). The working electrode was glassy carbon (WE-3G, Eicom Co). The flow rate was 0.25 mL/min. The detector voltage was set to 0.45 V. The detector temperature was set to 35.0°C. The retention time for noradrenaline was 5.4 minutes.
Analysis of Homogenized Tissue
We measured the noradrenaline content in the spinal dorsal horn in SNL rats and SNL rats treated with duloxetine using a separate group of rats, as previously described.9 To isolate the dorsal horn of the spinal cord, the portion correspond- ing to segments L4-L6 was divided into 4 constituent quad- rants: dorsal right, dorsal left, ventral right, and ventral left.
The dorsal left (ipsilateral) and dorsal right (contralateral) portions of the spinal cord were weighed and homogenized in 500 μL of 0.2 M perchloric acid containing 0.1 mM EDTA- Na2 and isoproterenol (0.02 mg/mL) as an internal stan- dard, and centrifuged at 20,000g and 0°C for 15 minutes.
The supernatants were adjusted to pH 3.0 by adding 1 M sodium acetate and then filtered through a centrifugal fil- ter with a pore size of 0.45 μm (Millipore, Bedford, MA).
Samples (10 μL) were injected into an HTEC-500 analyzing system (Eicom Co) and the concentration of noradrenaline was analyzed by high-performance liquid chromatography with electrochemical detection. The chromatographic con- ditions were as follows. The mobile phase comprised 0.1 M phosphate buffer (pH 6.0) containing 5 mg/L EDTA-Na2, 190 mg/L sodium 1-octanesulfate acid, and 17% methanol, and the column was an EICOMPAK SC-5ODS (3.0 × 150 mm, Eicom Co). The retention time for noradrenaline was 4.4 minutes.
Immunohistochemistry
Another group of rats was used for immunohistochemistry.
The rats were anesthetized with an intraperitoneal injec- tion of sodium pentobarbital (100 mg/kg), and intracardi- ally perfused with 0.01 M cold phosphate-buffered saline (PBS), followed by 4% paraformaldehyde in 0.1 M phos- phate buffer (pH 7.4) using a peristaltic pump (20 mL/min).
The whole brain was removed and postfixed overnight in 4% paraformaldehyde, followed by immersion in 30%
sucrose at 4°C for 1 week. Transverse brainstem slices con- taining the LC (700-μm thick) were obtained and embed- ded in Optimal Cutting Temperature Compound (4583, Sakura Finetek, Tokyo, Japan) and stored at −80°C. Each segment was cut transversely on a cryostat (CM1850, Leica Biosystems, Tokyo, Japan) at a 20-μm thickness. A rabbit monoclonal antibody against phosphorylated cyclic ade- nosine monophosphate response element binding protein (p-CREB; 1:1000; 06-519; Millipore, Billerica, Massachusetts) was used to assess neural activation, and a mouse monoclo- nal antibody against dopamine-β-hydroxylase (1:500; MAB 308; Millipore) was used to label noradrenergic fibers. To
prevent nonspecific labeling, blocking was performed with 3.0% normal donkey serum and 0.3% Triton X-100 (Sigma- Aldrich, St Louis, Missouri) in PBS. Sections were incu- bated overnight at 4°C in a solution of primary antibodies and blocking serum (1.5% normal donkey serum and 0.1%
Triton X-100 in PBS). Subsequently, the sections were rinsed in PBS and incubated in the appropriate secondary antibody, ie, Cy3-conjugated donkey antirabbit IgG (1:600; 711-165- 152; Millipore) or Cy2-conjugated donkey antimouse IgG (1:200; 715-225-150; Millipore) for 3 hours at room tempera- ture. The sections were washed thoroughly again in PBS and incubated in 4ʹ,6-diaminodino-2-phenylindole, dihy- drochloride (1:40,000; D21490; Molecular Probes, Thermo Fisher Scientific) for 5 minutes. Finally, the sections were dehydrated in ethanol, cleared in xylene, and cover-slipped with DPX mounting medium (Sigma-Aldrich) at room tem- perature. Images of the left and right LC were captured on an Olympus FSX100 microscope (Olympus Co, Tokyo, Japan). The number of p-CREB-positive noradrenergic cells within a defined threshold of staining intensity in the LC was counted using image analysis software (Image J; NIH Image, National Institutes of Health, Bethesda, Maryland).
Data from 8 slices obtained from the left and right LC per rat were averaged.
Statistical Analysis
All data passed normality (Shapiro-Wilk) and equal vari- ance (Levene median) tests. Data are presented as the mean
± SD. For behavioral testing of the antihyperalgesic effect of 3 daily injections of duloxetine, we divided the SNL rats into 2 groups: duloxetine and vehicle. We analyzed the value before SNL surgery, before drug injection (time 0 of days 1–3), 120 minutes after drug injection (days 1–3), 240 minutes after drug injection (days 1–3), and day 4 (~24 hours after day 3 time 0; Figure 1A). We analyzed the group
× day interaction and the group × time interaction within a day separately for each day. To test the effects of intrathecal injection (IT) idazoxan, we analyzed the value at before the idazoxan injection (day 4 time 0 in Figure 1A and time 0 in Figure 2A), and 15 and 30 minutes after the idazoxan injec- tion (Figure 2A). For NSIA testing after 3 daily injections of duloxetine, we analyzed the value before forepaw injec- tion of capsaicin (time 0 of day 4 in Figure 1B and time 0 in Figure 4A) and at the predetermined time points after the capsaicin injection described above. For NSIA testing after pretreatment with idazoxan, we analyzed 30 minutes after the idazoxan injection (time 0 in Figure 4B) and at the prede- termined time points after the capsaicin injection described above. The behavioral testing and time-course data were analyzed using a 2-way repeated-measures analysis of vari- ance (ANOVA) where group and time were considered as independent variables. The data about behavioral testing in naïve rats were analyzed using a 1-way repeated-measures ANOVA. The immunostaining data and noradrenaline con- tent in the homogenized lumbar spinal cord were analyzed using a 2-way ANOVA. When significant differences were observed (P < .05), a priori Student t tests with Bonferroni’s correction for multiple comparisons were performed for between-group comparisons and comparisons at each time point. Statistical analysis was conducted using SigmaPlot
AQ5
AQ6 AQ7
F1
F2
12 (Systat Software Inc, San Jose, California). The P value adjusted with Bonferroni’s correction is reported and P < .05 was considered significant. We performed a power analysis for the primary outcome (mechanical withdrawal threshold in SNL rats) to determine the appropriate sample size, with the assumptions of a mean (±SD) difference of 50 g (±30 g) in the withdrawal threshold in each group according to a previous study.9 We found that 6 rats in each group would result in detection of significant differences with 80% power at a significance level of α = .05.
RESULTS
A total of 158 rats were used, of which 150 rats were ana- lyzed and 8 rats were excluded due to hindlimb paralysis resulting from the SNL surgery. Table 1 shows the results of the 2-way repeated-measures ANOVA (group, time, and group × time interaction). Table 2 shows the estimated
treatment effect (difference between groups) with the 95%
confidence interval.
Antihyperalgesic Effect
Antihyperalgesic Effect of 3 Daily Injections of Duloxetine in SNL Rats. To evaluate the analgesic effects of duloxetine in rats at 6 weeks after SNL, duloxetine (10 mg kg−1 day−1) was administered subcutaneously for 3 consecutive days.
The group × day interaction and group × time interaction within each day were analyzed separately using a 2-way
T1 T2
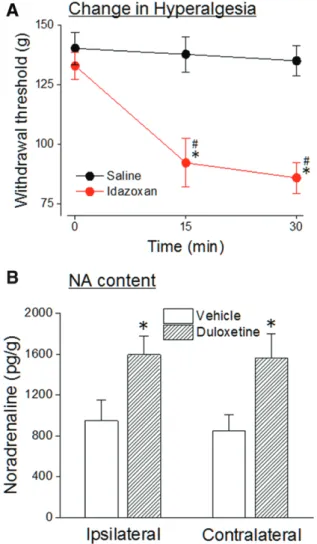
Figure 1. Effects of 3 daily injections of duloxetine on hindpaw withdrawal thresholds ipsilateral (A) or contralateral (B) to the site of the SNL. Rats were administered duloxetine (10 mg kg−1 day−1, subcutaneous injection) or vehicle for 3 consecutive days at 6 wk after SNL. Each day, withdrawal thresholds in both hindpaws were measured at time 0 (before duloxetine injection), and 120 and 240 min after the injection. All data represent the mean ± SD for 6 rats.
Groups were analyzed by 2-way repeated-measures ANOVA followed by Student t test with Bonferroni’s correction. *P < .05 compared with the duloxetine group at time 0 on day 1. $P < .05 compared with the duloxetine group at time 0 each day. #P < .05 compared with the vehicle group at each time point. ANOVA indicates analysis of variance; SNL, spinal nerve ligation.
Figure 2. Effects of intrathecal injection of idazoxan on the anti- hyperalgesic effect provided by duloxetine (A). Rats were treated with duloxetine for 3 consecutive days at 6 wk after SNL and then injected intrathecally with idazoxan (30 μg/20 μL) or vehicle. The antihyperalgesic effect was determined by measuring the withdrawal threshold in the hindpaw ipsilateral (left) to the SNL within 30 min after the intrathecal injection of idazoxan. All data represent the mean ± SD for 6 rats. Groups were analyzed by 2-way repeated- measures ANOVA followed by Student t test with Bonferroni’s cor- rection. #P < .05 compared with the duloxetine group at time 0.
*P < .05 compared with the vehicle group at each time point. NA content in the dorsal half of the lumbar spinal cord (B). Spinal cord tissue from rats injected with duloxetine (10 mg kg−1 day−1) or vehicle for 3 consecutive days at 6 wk after SNL was homogenized, and the noradrenaline content was measured. All data represent the mean
± SD for 6 rats. Groups were analyzed by 2-way ANOVA followed by Student t test with Bonferroni’s correction. *P < .05 compared with vehicle group at each time point. ANOVA indicates analysis of vari- ance; NA, noradrenaline; SNL, spinal nerve ligation.
repeated-measures ANOVA, and all results obtained by 4 daily analyses are shown in Figure 1. The main effects of group and day were significant, and there was a significant group × day interaction on withdrawal threshold in the hindpaw ipsilateral to the SNL site between the
Table 1. Results of 2-Way Repeated-Measures ANOVA
Factor Source of
Variation F Value P
Value Duloxetine-ipsilateral-day
(Figure 1A)
Group F1,40 = 118.351 <.001 Time F4,40 = 111.148 <.001 Group × time
interaction
F4,40 = 31.524 <.001 Duloxetine-ipsilateral-time
within day 1 (Figure 1A)
Group F1,20 = 110.565 <.001 Time F2,20 = 100.834 <.001 Group × time
interaction
F2,20 = 63.194 <.001 Duloxetine-ipsilateral-time
within day 2 (Figure 1A)
Group F1,20 = 154.207 <.001 Time F2,20 = 73.339 <.001 Group × time
interaction
F2,20 = 73.165 <.001 Duloxetine-ipsilateral-time
within day 3 (Figure 1A)
Group F1,20 = 356.000 <.001 Time F2,20 = 84.986 <.001 Group × time
interaction
F2,20 = 60.980 <.001 Duloxetine-contralateral-day
(Figure 1B)
Group F1,40 = 8.601 .015 Time F4,40 = 1.971 .118 Group × time
interaction
F4,40 = 1.647 .181 Duloxetine-contralateral-
time within day 1 (Figure 1B)
Group F1,20 = 11.039 .008 Time F2,20 = 10.004 <.001 Group × time
interaction
F2,20 = 5.425 .013 Duloxetine-contralateral-
time within day 2 (Figure 1B)
Group F1,20 = 13.168 .005 Time F2,20 = 21.108 <.001 Group × time
interaction
F2,20 = 6.778 .006 Duloxetine-contralateral-
time within day 3 (Figure 1B)
Group F1,20 = 92.554 <.001 Time F2,20 = 37.712 <.001 Group × time
interaction
F2,20 = 21.481 <.001 Reverse of antihyperalgesic
effect after duloxetine treatment and idazoxan injection (Figure 2A)
Group F1,20 = 267.302 <.001 Time F2,20 = 38.834 <.001 Group × time
interaction
F2,20 = 26.802 <.001 NSIA-sham and SNL
(Figure 3A)
Group F3,45 = 24.972 <.001 Time F3,45 = 20.096 <.001 Group × time
interaction
F9,45 = 12.169 <.001 Microdialysis-sham and
SNL (Figure 3B)
Group F3,120 = 5.297 .007
Time F6,120 = 1.306 .206
Group × time interaction
F18,120 = 1.522 .094
NSIA after duloxetine treatment (Figure 4A)
Group F1,30 = 11.283 .005 Time F3,30 = 17.635 <.001 Group × time
interaction
F3,30 = 9.072 <.001 NSIA-SNL with duloxetine
treatment and idazoxan injection (Figure 4B)
Group F1,30 = 69.670 <.001 Time F3,30 = 54.063 <.001 Group × time
interaction
F3,30 = 34.547 <.001 Microdialysis after
duloxetine treatment (Figure 5A)
Group F1,60 = 0.722 .415 Time F6,60 = 1.578 .169 Group × time
interaction
F6,60 = 0.352 .906
Abbreviations: ANOVA, analysis of variance; NSIA, noxious stimulus–induced analgesia; SNL, spinal nerve ligation.
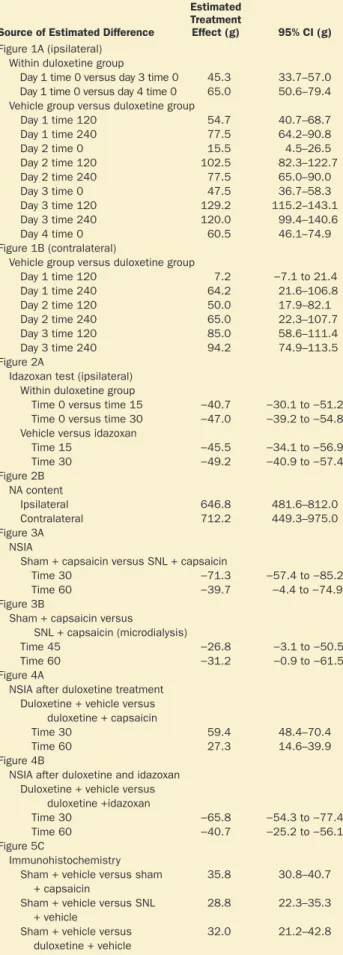
Table 2. Estimated Treatment Effect and 95% CI
Source of Estimated Difference
Estimated Treatment
Effect (g) 95% CI (g) Figure 1A (ipsilateral)
Within duloxetine group
Day 1 time 0 versus day 3 time 0 45.3 33.7–57.0 Day 1 time 0 versus day 4 time 0 65.0 50.6–79.4 Vehicle group versus duloxetine group
Day 1 time 120 54.7 40.7–68.7
Day 1 time 240 77.5 64.2–90.8
Day 2 time 0 15.5 4.5–26.5
Day 2 time 120 102.5 82.3–122.7
Day 2 time 240 77.5 65.0–90.0
Day 3 time 0 47.5 36.7–58.3
Day 3 time 120 129.2 115.2–143.1
Day 3 time 240 120.0 99.4–140.6
Day 4 time 0 60.5 46.1–74.9
Figure 1B (contralateral)
Vehicle group versus duloxetine group
Day 1 time 120 7.2 −7.1 to 21.4
Day 1 time 240 64.2 21.6–106.8
Day 2 time 120 50.0 17.9–82.1
Day 2 time 240 65.0 22.3–107.7
Day 3 time 120 85.0 58.6–111.4
Day 3 time 240 94.2 74.9–113.5
Figure 2A
Idazoxan test (ipsilateral) Within duloxetine group
Time 0 versus time 15 −40.7 −30.1 to −51.2 Time 0 versus time 30 −47.0 −39.2 to −54.8 Vehicle versus idazoxan
Time 15 −45.5 −34.1 to −56.9
Time 30 −49.2 −40.9 to −57.4
Figure 2B NA content
Ipsilateral 646.8 481.6–812.0
Contralateral 712.2 449.3–975.0
Figure 3A NSIA
Sham + capsaicin versus SNL + capsaicin
Time 30 −71.3 −57.4 to −85.2
Time 60 −39.7 −4.4 to −74.9
Figure 3B
Sham + capsaicin versus SNL + capsaicin (microdialysis)
Time 45 −26.8 −3.1 to −50.5
Time 60 −31.2 −0.9 to −61.5
Figure 4A
NSIA after duloxetine treatment Duloxetine + vehicle versus duloxetine + capsaicin
Time 30 59.4 48.4–70.4
Time 60 27.3 14.6–39.9
Figure 4B
NSIA after duloxetine and idazoxan Duloxetine + vehicle versus
duloxetine +idazoxan
Time 30 −65.8 −54.3 to −77.4
Time 60 −40.7 −25.2 to −56.1
Figure 5C
Immunohistochemistry Sham + vehicle versus sham
+ capsaicin
35.8 30.8–40.7
Sham + vehicle versus SNL + vehicle
28.8 22.3–35.3
Sham + vehicle versus duloxetine + vehicle
32.0 21.2–42.8
Abbreviations: 95% CI, 95% confidence interval; NA, noradrenaline; NSIA, noxious stimulus–induced analgesia; SNL, spinal nerve ligation.
duloxetine- and vehicle-injected groups (Figure 1A). SNL rats treated with duloxetine (SNL-duloxetine group) had significantly higher withdrawal thresholds of the ipsilateral hindpaw compared with the SNL-vehicle group on days 2 to 4 (P = .003 on day 2, P < .001 on days 3 and 4), and the SNL-duloxetine group had significantly higher withdrawal thresholds of the ipsilateral hindpaw on days 3 and 4 than on day 1 before injection (P < .001, respectively). To examine the acute effects of duloxetine within 240 minutes after injection, we analyzed the data each day. The main effects of group and time (within day) were significant, and there was a significant group × time interaction on days 1 to 3.
Duloxetine significantly increased the withdrawal threshold of the ipsilateral hindpaw within 240 minutes after injection compared to the vehicle group at each time point. Injection of duloxetine also increased the withdrawal threshold of the ipsilateral hindpaw within 240 minutes after injection compared to before injection (time 0) each day.
In the contralateral hindpaw, the withdrawal thresh- old did not change at time 0 for each day throughout the experiment (Figure 1B). Investigation of the acute effects of duloxetine within 240 minutes after injection revealed a significant main effect of group and time (within day), and a significant group × time interaction on days 1 to 3.
Duloxetine induced the same results as obtained from the ipsilateral hindpaw (Table 2). The results from the contra- lateral hindpaw suggest that duloxetine has acute analgesic effects against nociceptive mechanical stimuli. Therefore, we injected duloxetine into naïve rats using the same proto- col to investigate whether this effect occurs in rats without spinal nerve injury. Duloxetine did not increase the with- drawal threshold in either hindpaw within 240 minutes after injection compared to before injection (time 0) on days 1 to 3 (withdrawal thresholds at 0, 120, and 240 minutes after injection on day 1 were 144 ± 6, 148 ± 13, 148 ± 12 g;
those on day 2 were 141 ± 6, 147 ± 8, 142 ± 8 g; those on day 3 were 145 ± 5, 146 ± 10, 143 ± 12 g); or on the with- drawal threshold on day 4 (142 ± 8 g) compared to day 1 before injection (P = .800 within day 1, P = .469 within day 2, P = .897 within day 3, P = .524 between days [time 0] by 1-way repeated-measures ANOVA). Thus, the acute anal- gesic effect of duloxetine against mechanical stimuli was observed only in SNL rats.
No adverse behavioral effects, such as sedation or agita- tion, were observed, and the placing and righting reflexes were normal (all scores: 0).
Role of α2-Adrenoceptor in the Spinal Cord for Anti- hypersensitivity. To evaluate the contribution of spinal noradrenaline to the duloxetine-induced antihyperalgesic effects, we intrathecally injected the α2-adrenoceptor antagonist idazoxan (30 μg/20 μL) or vehicle (20 μL) on day 4 (Figure 2A). The main effects of group and time were significant, and there was a significant group × time interaction on the withdrawal thresholds in the hindpaw ipsilateral to the SNL between the idazoxan and vehicle groups. Intrathecal idazoxan decreased the withdrawal threshold of the ipsilateral hindpaw at 15 and 30 minutes after injection compared with before injection (P < .001, respectively). Idazoxan also decreased the withdrawal threshold of the ipsilateral hindpaw compared with the
vehicle group at 15 and 30 minutes after injection (P < .001, respectively). These results indicate that α2-adrenoceptors in the spinal cord are involved in the antihyperalgesic effects of duloxetine.
Change in Spinal Noradrenaline Content After 3 Daily Injections of Duloxetine
The noradrenaline content in the dorsal half of the lum- bar spinal cord was measured after 3 daily injections of duloxetine (Figure 2B). In SNL rats treated with duloxetine, there was a significant main effect of group (F1,20 = 70.192;
P < .001), but no main effect of laterality (F1,20 = 0.724;
P = .405) or group × laterality interaction (F1,20 = 0.162;
P = .691). Duloxetine increased the noradrenaline content bilaterally compared with vehicle (P < .001, respectively).
These results are consistent with the result of the idazoxan study described above.
Noxious Stimulus–Induced Analgesia
Effect of SNL on NSIA and Noradrenaline Release in the Spinal Cord. In SNL rats and sham-operated rats, there was a significant main effect of group and time, and there was a significant group × time interaction on withdrawal thresholds in the contralateral hindpaw after forepaw injection of capsaicin (Figure 3A). In sham-operated rats, forepaw injection of capsaicin significantly increased the withdrawal thresholds 30 and 60 minutes after injection compared to vehicle, demonstrating an NSIA effect (P < .001, respectively). This NSIA effect peaked at 30 minutes after capsaicin injection and continued for approximately 60 minutes. SNL rats had a significantly reduced NSIA effect 30 and 60 minutes after capsaicin injection compared with sham-operated rats (P < .001, respectively).
Microdialysis studies of SNL rats and sham-operated rats revealed a significant main effect of group, but no main effect of time, and a significant group × time interaction for capsaicin-evoked noradrenaline release in the right spinal dorsal horn (contralateral to the SNL; Figure 3B). In sham- operated rats, capsaicin injection significantly increased the spinal noradrenaline concentration at 45 and 60 minutes after injection compared with vehicle (P < .001, respec- tively). In SNL rats, however, capsaicin injection did not increase the spinal noradrenaline concentration compared with vehicle (P = 1.000). The basal noradrenaline concen- tration in the right lumbar dorsal horn of SNL rats (0.55 ± 0.16 pg/15 μL) was significantly lower than that in sham- operated rats (0.84 ± 0.38 pg/15 μL; P = .034).
Effect of 3 Daily Injections of Duloxetine on Endogenous Analgesia. We investigated the effects of 3 daily injections of duloxetine on NSIA in SNL rats on day 4. In SNL- duloxetine rats injected into the forepaw with capsaicin or vehicle, there were significant main effects of group and time, and no group × time interaction for withdrawal thresholds in the contralateral hindpaw (Figure 4A).
In SNL rats treated with duloxetine, capsaicin injection significantly increased the withdrawal thresholds of the contralateral hindpaw at 30 and 60 minutes after injection compared with vehicle (P < .001 and P = .012, respectively;
Figure 4A). These findings indicate that NSIA was restored
F3
F4
in SNL rats by repeated administration of duloxetine. Next, to evaluate the contribution of spinal noradrenaline to the restoration of NSIA provided by duloxetine, we injected idazoxan (30 μg/20 μL) or vehicle (20 μL) intrathecally to SNL rats treated with duloxetine. Thirty minutes after idazoxan injection, we injected capsaicin into the forepaw and tested NSIA. After capsaicin injection, there was a significant main effect of group and time, and a significant group × time interaction between the idazoxan- and vehicle-injected groups on withdrawal thresholds in the contralateral hindpaw (Figure 4B). In SNL rats treated with duloxetine, pretreatment with intrathecal idazoxan resulted in a significant reduction of NSIA compared with intrathecal saline (P < .001 at 30 and 60 minutes after
capsaicin injection). This result indicates the importance of spinal noradrenaline provided by repeated administration of duloxetine for restoring NSIA.
Effect of 3 Daily Injections of Duloxetine on Spinal Noradrenaline Release
Microdialysis was performed to investigate whether the enhanced noradrenaline release in the spinal cord after forepaw capsaicin injection was restored by 3 daily injec- tions of duloxetine in SNL rats. After 3 daily injections of duloxetine, the noradrenaline concentration in the spinal Figure 3. Effect of SNL on NSIA and NA release in the spinal cord.
Sham rats or rats 6 wk after SNL were injected subcutaneously with capsaicin (150 μg/50 μL) or vehicle into the right forepaw.
Withdrawal thresholds in the hindpaw contralateral to the SNL (right) were measured over time (A). Changes in the noradrenaline concen- tration from the right lumbar spinal dorsal horn after capsaicin injec- tion (B). After baseline concentrations were determined at 120 min after insertion of the microdialysis probe, capsaicin or vehicle was injected into the right forepaw. Percent change in the noradrenaline concentration over 90 min after forepaw capsaicin injection com- pared to the baseline sample was measured. All data represent the mean ± SD for 6 rats. Data were analyzed by 2-way repeated-mea- sures ANOVA followed by Student t test with Bonferroni’s correction.
*P < .05 compared with the SNL-capsaicin group (A), sham-vehicle group at each time point (B). ANOVA indicates analysis of variance;
NA, noradrenaline; NSIA, noxious stimulus–induced analgesia; SNL, spinal nerve ligation.
Figure 4. Effects of 3 daily injections of duloxetine on NSIA (A). Rats were injected subcutaneously with duloxetine (10 mg kg−1 day−1) for 3 consecutive days at 6 wk after SNL and then injected subcuta- neously with capsaicin or vehicle into the right forepaw. NSIA was determined by measuring withdrawal threshold in the hindpaw con- tralateral (right) to the SNL over time. Effects of intrathecal injection of idazoxan on NSIA provided by duloxetine (B). Rats were treated with duloxetine for 3 consecutive days at 6 wk after SNL and then injected intrathecally with idazoxan (30 μg/20 μL) or vehicle. Thirty minutes after intrathecal injection of idazoxan, the rats were injected into the forepaw with capsaicin (150 μg/50 μL; time 0 in B). All data represent the mean ± SD for 6 rats. Groups were analyzed by 2-way repeated-measures ANOVA followed by Student t test with Bonferroni’s correction. *P < .05 compared with the vehicle (A) or idazoxan (B) group at each time point. ANOVA indicates analysis of variance; NSIA, noxious stimulus–induced analgesia; SNL, spinal nerve ligation.
cord after capsaicin injection was not changed (P = .415;
Figure 5A).
Immunohistochemistry of the LC
We performed immunostaining of p-CREB as a marker of neuronal activation in the LC after 3 daily injections of duloxetine. We determined p-CREB immunoreactivity (IR) in noradrenergic LC neurons in sham-operated rats, SNL rats treated with vehicle (SNL-vehicle group), and SNL rats treated with duloxetine (SNL-duloxetine group;
Figure 5B). Each group of rats was divided into 2 groups and either capsaicin or vehicle was injected into the fore- paw. Noradrenergic neurons were identified by dopamine- β-hydroxylase-IR and 4ʹ,6-diaminodino-2-phenylindole, dihydrochloride staining. For p-CREB-IR in noradrenergic LC neurons, there were significant main effects of group (F2,30 = 11.957; P < .001) and drug (capsaicin or vehicle;
F1,30 = 24.788; P < .001), and a significant group × drug interaction (F2,30 = 20.688; P < .001; Figure 5C). In sham- operated rats, capsaicin increased p-CREB-IR compared
with vehicle (P < .001), and both the SNL-vehicle group and SNL-duloxetine group exhibited higher p-CREB-IR than the sham-operated group (P < .001, respectively). In the SNL- duloxetine group, p-CREB expression was equivalent to that in the SNL-vehicle group (P = 1.000 both forepaw cap- saicin and vehicle-injected group).
DISCUSSION
The results of the present study indicated that 3 daily treat- ments with duloxetine at 6 weeks after SNL produced anti- hyperalgesic effects that were reversed by IT of idazoxan and increased the noradrenaline content in the spinal cord. The 3 daily treatments with duloxetine recovered the impairment of NSIA, and this recovery of NSIA was also reversed by IT of idazoxan. Three daily injections of duloxetine, however, did not alter the p-CREB positive rate in the LC or the nor- adrenaline release in the spinal dorsal horn relative to that observed in SNL rats without duloxetine treatment.
Activation of α2-adrenoceptors in the spinal cord more potently suppresses neuropathic pain than acute
F5
Figure 5. Effects of 3 daily injections of duloxetine on spinal NA release and neuronal activity in the LC. Change in the noradrenaline concentration in the right lumbar dorsal spinal cord measured by microdialysis (A). Rats were injected with duloxetine (10 mg kg−1 day−1) or vehicle for 3 consecutive days at 6 wk after SNL. After determining the baseline concen- tration at 120 min following insertion of the microdialysis probe, capsaicin was injected into the right forepaw. Percent change in the noradrenaline concentration over 90 min after forepaw capsaicin injection compared to the baseline sample. All values represent the mean ± SD for 6 rats and were analyzed by 2-way repeated-measures ANOVA followed by Student t test with Bonferroni’s correction.
Immunostaining for p-CREB in the LC (B).
Photomicrographs of p-CREB immunoreactiv- ity (red) and dopamine-β-hydroxylase immu- noreactivity (green) in the LC were shown.
Rats were injected with duloxetine daily for 3 consecutive days (10 mg kg−1 day−1) at 6 wk after SNL. Sham-operated rats, SNL rats, and SNL rats injected with duloxetine were used.
Each group of rats was perfused and fixed 120 min after injection of capsaicin or vehicle into the right forepaw. Quantification of the ratio of p-CREB-immunoreactive noradrenergic neurons in the LC (C). All data represent the mean ± SD for 6 rats. Groups were analyzed by 2-way repeated-measures ANOVA followed by Student t test with Bonferroni’s correction.
*P < .05 compared with sham-operated rats injected with vehicle. ANOVA indicates analy- sis of variance; LC, locus coeruleus; NA, nor- adrenaline; p-CREB, phosphorylated cyclic adenosine monophosphate response element binding protein; SNL, spinal nerve ligation.
nociceptive pain.17–19 The tone of descending noradren- ergic inhibition decreases over time, however, after nerve injury.5,6,15 A recent study reported that 6 weeks after SNL, increased extracellular glutamate levels caused by down- regulation of the glutamate transporter-1 in the LC reduce noradrenaline release in the spinal cord through autoinhibi- tion of glutamate release in the presynaptic terminals of the LC.13 In the present study, we evaluated the same post-SNL time period used in that recent study, and hypothesized that recovery of descending inhibitory function is an important mechanism underlying the effect of duloxetine against neu- ropathic pain.
The number needed to treat for duloxetine is reported to range from 4.2 to 7.0, which means is clinically useful, and the rate of severe adverse events is also reported to be
low.20–22 The mechanisms underlying the analgesic effects
against neuropathic pain, however, are unclear. In the pres- ent study, the withdrawal threshold of the ipsilateral hind- paw gradually increased after repeated administration of duloxetine. After 3 daily injections of duloxetine, the with- drawal threshold of the ipsilateral hindpaw increased to the same level observed prior to SNL, which was accompanied by an increase in the noradrenaline content in the spinal cord. This antihyperalgesic effect was reversed by IT of the α2-adrenoceptor antagonist idazoxan. These findings sug- gest that the accumulation of spinal noradrenaline has an important role in the analgesic effect of duloxetine in neu- ropathic pain.
We also found that duloxetine has acute antihyperal- gesic effects that continue for at least 240 minutes after the injection. Injection of duloxetine increased withdrawal thresholds not only in the ipsilateral hindpaw but also in the contralateral hindpaw in SNL rats. These effects were not observed in non-SNL control rats. We speculate that this acute analgesic effect in the contralateral hindpaw against mechanical stimuli might be affected by neuronal plasticity, including changes in α2-adrenoceptors after nerve injury to the opposite side, even though the withdrawal thresh- olds after SNL were not changed. In the present study, only mechanical hyperalgesia was measured in the behav- ioral studies and this may not accurately reflect the drug effects against neuropathic pain. Other measures, such as allodynia and thermal hyperalgesia, in combination with a nonstimulation method (eg, conditioned place preference) might be a better way to assess the real effects of duloxetine on neuropathic pain.
We also investigated the effects of repeated administration of duloxetine on endogenous analgesia. A previous study reported reduced NSIA and attenuated LC neural activ- ity in rats 6 weeks after SNL following forepaw injection of capsaicin.13 Three daily treatments with duloxetine reversed the decrease in the NSIA effect at 6 weeks after SNL, and IT of idazoxan attenuated the effect induced by duloxetine.
These results indicate that recovery of NSIA is also medi- ated through α2-adrenoceptors in the spinal cord. Capsaicin- evoked spinal noradrenaline release was not changed in SNL rats treated with duloxetine. Consistent with this, immunos- taining of the LC revealed that the rate of p-CREB positivity in noradrenergic neurons of the LC at 120 minutes after fore- paw capsaicin injection was not changed in SNL rats treated
with duloxetine. These findings suggest that in neuropathic pain, repeated administration of duloxetine reinstates decreased endogenous analgesia, but we could not demon- strate that this is due to the reversal of the dysfunction of the descending noradrenergic inhibitory system. There are sev- eral possible reasons for the discrepancy between behavioral testing and activity of the descending noradrenergic inhibi- tory system. One is that the accumulation of noradrenaline in the spinal cord rather than a change in the descending nor- adrenergic system might play a role even at the beginning of the recovery of NSIA. A previous study demonstrated by extracellular recordings that administration of duloxetine for 7 days restores LC neuronal activity after nerve injury.23 Thus, the possibility that a change in the neuronal activity in the LC becomes apparent after longer-term administra- tion of duloxetine cannot be ruled out. Further studies are needed to systematically examine the duration of duloxetine administration and evaluate neuronal changes in the LC by other means such as neuronal recording or microdialysis.
Another possible mechanism is that the increased level of p-CREB positivity in the LC observed after SNL produced a ceiling effect. Increased noradrenaline by repeated dulox- etine administration might suppress the LC neuronal activity by negative feedback through α2-adrenoceptors in the LC, which might lead to recovery in NSIA. The p-CREB expres- sion, however, did not change. Finally, NSIA is also reported to be mediated by other supraspinal structures such as the nuclei accumbens, periaqueductal gray, and rostroventral medulla.10,11,24 These nuclei might play an important role in NSIA recovery following chronic treatment with duloxetine.
In conclusion, the present study provides new and important information regarding the mechanism by which duloxetine inhibits neuropathic pain. Accumulation of nor- adrenaline in the spinal cord might play an important role in suppressing hyperalgesia and recovering impairment of NSIA provided by 3 daily injections of duloxetine.
E
DISCLOSURES Name: Sachiko Ito, MD.
Contribution: This author helped conduct the study, collect data, analyze the data, and prepare the manuscript.
Conflicts of Interest: None.
Name: Takashi Suto, MD, PhD.
Contribution: This author helped collect data and prepare the manuscript.
Conflicts of Interest: None.
Name: Shigeru Saito, MD, PhD.
Contribution: This author helped design the study and prepare the manuscript.
Conflicts of Interest: None.
Name: Hideaki Obata, MD, PhD.
Contribution: This author helped design and conduct the study, analyze the data, and prepare the manuscript.
Conflicts of Interest: Hideaki Obata has conflict of interest with Eli Lilly Japan K.K.
This manuscript was handled by: Jianren Mao, MD, PhD.
REFERENCES
1. Lewis GN, Rice DA, McNair PJ. Conditioned pain modula- tion in populations with chronic pain: a systematic review and meta-analysis. J Pain. 2012;13:936–944.
2. Yarnitsky D, Granot M, Nahman-Averbuch H, Khamaisi M, Granovsky Y. Conditioned pain modulation predicts duloxetine efficacy in painful diabetic neuropathy. Pain.
2012;153:1193–1198.
3. Fritschy JM, Grzanna R. Demonstration of two separate descending noradrenergic pathways to the rat spinal cord:
evidence for an intragriseal trajectory of locus coeruleus axons in the superficial layers of the dorsal horn. J Comp Neurol.
1990;291:553–582.
4. Howorth PW, Thornton SR, O’Brien V, et al. Retrograde viral vector-mediated inhibition of pontospinal noradrener- gic neurons causes hyperalgesia in rats. J Neurosci. 2009;29:
12855–12864.
5. Hughes SW, Hickey L, Hulse RP, Lumb BM, Pickering AE.
Endogenous analgesic action of the pontospinal noradrenergic system spatially restricts and temporally delays the progres- sion of neuropathic pain following tibial nerve injury. Pain.
2013;154:1680–1690.
6. Matsuoka H, Suto T, Saito S, Obata H. Amitriptyline, but not pregabalin, reverses the attenuation of noxious stimulus- induced analgesia after nerve injury in rats. Anesth Analg.
2016;123:504–510.
7. Finnerup NB, Attal N, Haroutounian S, et al. Pharmacotherapy for neuropathic pain in adults: a systematic review and meta- analysis. Lancet Neurol. 2015;14:162–173.
8. Nakajima K, Obata H, Iriuchijima N, Saito S. An increase in spi- nal cord noradrenaline is a major contributor to the antihyper- algesic effect of antidepressants after peripheral nerve injury in the rat. Pain. 2012;153:990–997.
9. Hoshino H, Obata H, Saito S. Antihyperalgesic effect of dulox- etine and amitriptyline in rats after peripheral nerve injury:
Influence of descending noradrenergic plasticity. Neurosci Lett.
2015;602:62–67.
10. Tambeli CH, Levine JD, Gear RW. Centralization of noxious stimulus-induced analgesia (NSIA) is related to activity at inhibitory synapses in the spinal cord. Pain. 2009;143:228–232.
11. Schmidt BL, Tambeli CH, Levine JD, Gear RW. Adaptations in nucleus accumbens circuitry during opioid withdrawal associ- ated with persistence of noxious stimulus-induced antinocicep- tion in the rat. J Pain. 2003;4:141–147.
12. Kim SH, Chung JM. An experimental model for peripheral neu- ropathy produced by segmental spinal nerve ligation in the rat.
Pain. 1992;50:355–363.
13. Kimura M, Suto T, Morado-Urbina CE, Peters CM, Eisenach JC, Hayashida K. Impaired pain-evoked analgesia after nerve
injury in rats reflects altered glutamate regulation in the locus coeruleus. Anesthesiology. 2015;123:899–908.
14. Randall LO, Selitto JJ. A method for measurement of analge- sic activity on inflamed tissue. Arch Int Pharmacodyn Ther.
1957;111:409–419.
15. Hoshino H, Obata H, Nakajima K, Mieda R, Saito S. The anti- hyperalgesic effects of intrathecal bupropion, a dopamine and noradrenaline reuptake inhibitor, in a rat model of neuropathic pain. Anesth Analg. 2015;120:460–466.
16. Obata H, Kimura M, Nakajima K, Tobe M, Nishikawa K, Saito S. Monoamine-dependent, opioid-independent antihypersensi- tivity effects of intrathecally administered milnacipran, a sero- tonin noradrenaline reuptake inhibitor, in a postoperative pain model in rats. J Pharmacol Exp Ther. 2010;334:1059–1065.
17. Kimura M, Saito S, Obata H. Dexmedetomidine decreases hyperalgesia in neuropathic pain by increasing acetylcholine in the spinal cord. Neurosci Lett. 2012;529:70–74.
18. Paqueron X, Conklin D, Eisenach JC. Plasticity in action of intrathecal clonidine to mechanical but not thermal nociception after peripheral nerve injury. Anesthesiology. 2003;99:199–204.
19. Poree LR, Guo TZ, Kingery WS, Maze M. The analgesic potency of dexmedetomidine is enhanced after nerve injury: a pos- sible role for peripheral alpha2-adrenoceptors. Anesth Analg.
1998;87:941–948.
20. Goldstein DJ, Lu Y, Detke MJ, Lee TC, Iyengar S. Duloxetine vs. placebo in patients with painful diabetic neuropathy. Pain.
2005;116:109–118.
21. Yasuda H, Hotta N, Nakao K, Kasuga M, Kashiwagi A, Kawamori R. Superiority of duloxetine to placebo in improving diabetic neuropathic pain: results of a randomized controlled trial in Japan. J Diabetes Investig. 2011;2:132–139.
22. Raskin J, Pritchett YL, Wang F, et al. A double-blind, random- ized multicenter trial comparing duloxetine with placebo in the management of diabetic peripheral neuropathic pain. Pain Med.
2005;6:346–356.
23. Alba-Delgado C, Mico JA, Sánchez-Blázquez P, Berrocoso E.
Analgesic antidepressants promote the responsiveness of locus coeruleus neurons to noxious stimulation: implications for neu- ropathic pain. Pain. 2012;153:1438–1449.
24. Gear RW, Aley KO, Levine JD. Pain-induced analgesia mediated by mesolimbic reward circuits. J Neurosci. 1999;19:7175–7181.