原 著
イメージングプレート方式のデジタル口内法エックス線撮影システム
Digora
ⓇOptime II Comfort Occlusal と VistaScan Mini
による咬合法画像の評価
松田 幸子,寺内 庸康,関 健 次
荒木 和之,岡野 友宏
Assessment of Visibility in Occlusal Radiographs Obtained using
the DIGORA
ⓇOptime II Comfort Occlusal System
and VistaScan Mini
Yukiko Matsuda, Hiroyasu Terauchi, Kenji Seki, Kazuyuki Araki and Tomohiro Okano
Purpose: To assess the image quality of digital occlusal radiographic systems.
Materials and methods: Digital occlusal radiographic images were obtained using two kinds of photo-stimulable phosphor sys-tems: Digora Optime II Comfort Occlusal and a VistaScan Mini. Imaging plates (IPs) were used for the Digora system in both verti-cal and horizontal orientations. Images acquired using the digital systems were compared with images acquired using Kodak Insight occlusal films. Occlusal radiographic images were taken using one dry skull. Exposure condition was set at 70kV, 7mA with 0.03, 0.06 and 0.12 seconds. At each exposure time and with each modality, three radiographic images were obtained. The clinical utility of each system was assessed, based on the visibility of the following four anatomical structures and pathologic conditions : (1) maxil-lary bone structure ; (2) anatomical structures such as incisive canals and the median palatine suture; (3) alveolar bone, teeth, and apical regions ; and (4) presence of impacted teeth. Four observers were asked to evaluate each image quality, using the following five point scale : 1=unacceptable; 2=poor; 3=fair; 4=good; and 5=excellent. A one-way ANOVA and Tukey’s test were used for sta-tistical analyses.
Results and conclusions: The average and standard deviation for assessments obtained from film, the Digora system with verti-cal and horizontal IPs, and the VistaScan system, were 4.3±0.59, 4.1±1.01, 3.9±0.66 and 4.2±1.10, respectively. There were no statistically significant differences among the systems, but a statistically significant difference was seen for exposure times, namely, 0.03 second versus 0.06 or 0.12 second. None of the images obtained by the Digora system in conjunction with vertical IPs was rated as unacceptable. These results suggest that the digital systems tested are a viable alternative to an occlusal film system in terms of their clinical utility.
Dental Radiology 2011 ; 51(3): 19-26
Key words:Occlusal radiograph, Direct digital system, Imaging Plate / 咬合法撮影,ダイレクトデジタルシステム,イメージ ングプレート 緒 言 デジタル口内法撮影システムは 1980 年代に実用化され て以来,多くのシステムが開発され臨床に用いられてい る1-5。この X 線検出系には,固体半導体検出器(Charge Coupled Device)を用いる方式と輝尽性蛍光体からなる イメージングプレート(Imaging Plate 以下 IP)を用い
る方式とがあり,それぞれのシステムについてさまざまな 評価が行われている5-10。我々もまた,IP の耐久性につい て検討し,1,000 回の撮影でも同様の信号強度が得られる ことを検証している11。 口内法撮影の中で,咬合法撮影は標準口内法撮影ほど頻 度が高くないが,標準型フィルムでは撮影出来る範囲が狭 いため病変の全貌を診断することができない場合に適応と なる検査である。大学病院などでは,埋伏歯の頬舌的位置, 顎骨の頬舌的膨隆の有無,唾石の有無の把握や顎裂部の精 査,骨移植後の経過観察などに頻繁に用いられている12。 Witcherら13はパノラマ X 線撮影と咬合法撮影とを比較 しているが,前歯部の根吸収の診断や埋伏歯の診断は咬合 法のほうが正確であり,パノラマ X 線撮影では断層域が 狭く,前歯部のスクリーニングの対象にすることは有意義
Received July 15, revision accepted October 25, 2011. 著者所属:昭和大学歯学部歯科放射線医学教室
別刷請求先:〒 145-8515 東京都大田区北千束 2-1-1 昭和大学 歯学部歯科放射線医学教室 松田幸子
From Department of Radiology, School of Dentistry, Showa University, 2-1-1, Kitasenzoku, Ohota-ku, Tokyo, 145-8515, Japan
Address reprint requests to the author, Dr. Y. Matsuda 版権:Ⓒ 2011 日本歯科放射線学会
歯科放射線 51 巻 3 号 松田
ではないと結論付け,咬合法検査の有用性を示唆している。
咬合型フィルム(No.4)は大きさが 57
×
76mmあり,31
×
41mmの標準型口内法フィルムに対して縦も横も 1.5倍以上大きい。DigoraⓇ OptimeII Comfort Occlusalシス
テム(Soredex 社 Tuusula,Finland,日本製品名:ディ ゴラオプティメ II,以下 Digora Occlusal)は従来の標準 型に近い IP を 2 枚使用して咬合法の画像を得ることが可 能である。一方,VistaScan Mini システム(Dürr Dental 社 Bietigheim-Bissingen,Germany,日本製品名:ビス タスキャンミニ,以下 VistaScan)は咬合型フィルムと同 じ大きさの IP をスキャンすることができる。 咬合法撮影は矯正治療でも頻繁に用いられている方法で あるが,撮影対象になるのは口蓋裂や上顎の埋伏歯などを 有する小児が多く,通常の咬合型フィルムでは大きすぎる 場合がある。その際には,標準サイズのフィルムに変更し たり,フィルムの一部を折り曲げるなどの工夫をして撮影 を行っている。Digora Occlusal では 2 枚の IP を連ねると, 大きさが 48
×
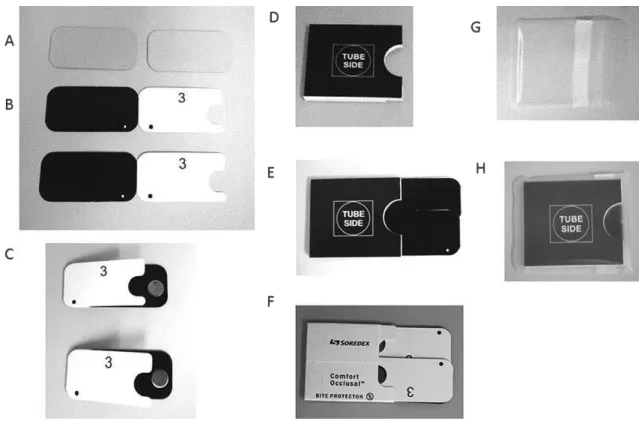
54mmとなり,従来の咬合型フィルムより も小さいことから,口腔内の小さい小児や口蓋裂患者の検 査に有用と考えられる。 本研究では両システムで得られる咬合法デジタル画像の 画質を評価することを目的とした。また,デジタルシステ ムの利点として線量の低減があげられるが,線量の違いに よる画質の違いについても評価を行った。 材料と方法 1.撮影 乾燥頭蓋骨 1 体を被写体とし,上顎前歯部に対して二 等分投影を行った。埋伏歯の代わりに抜去歯を口蓋部に置 いて撮影を行った。 撮影装置には HD-70(朝日レントゲン工業株式会社, 京都)を用い,管電圧 70kV,管電流 7 mA で照射した。 焦 点・ 被 写 体 間 距 離 は 32cm, 照 射 時 間 は 0.03,0.06, 0.12秒の 3 段階とした。撮影はそれぞれ 3 回ずつ行った。 Digora Occlusalシステムでは IP を縦と横に設置した。 2.Digora Occlusal について Digora Occlusal システムの IP および付属するキット を Figure 1 に示す。咬翼法に使用するサイズ 3(27×
54mm)の IP を 2 枚用いる。IP(Figure 1A)を IP のイ メージングプレートカバー(Figure 1B)にはさみ(Fig-ure 1C),IP の長辺を重ね合わせた状態で,咬合法プロテ クタと呼ばれる紙製の咬合法用の器具(Figure 1D)に装 填し(Figure 1E,1F),さらにそれを唾液汚染予防の保 護バッグ(Figure 1G)に入れて(Figure 1H)撮影を行 う。実際に撮影される画像の大きさは 48×
54mmと従来 の咬合型フィルムの大きさ 57×
76mmよりも小さく,ほ ぼ正方形になる。撮影後は IP を順番に取り出してスキャ ナーに入れて読み取りを行う。重複した部分を自動認識し て重ね合わせが行われ,咬合法画像が作成される。読み取 りのピクセルサイズには 60μm と 35μm があるが,本研 究は 35μm で行った。IP の口腔内の挿入方向については, 2枚の IP が前後方向に IP が 2 枚並ぶ方法と近遠心(左 右)方向に並ぶ方法の 2 通りを検討した。 3.VistaScan Mini システムについて VistaScan では咬合型フィルムと同じ大きさの IP を用 いる。Figure 2 に IP(Figure 2A)と保護カバー(Figure 2B)を示す。その右隣に標準型サイズの VistaScan の IP (Figure 2C)と Digora Occlusal の IP(Figure 2D)を横 から見た画像を示す。Digora Occlusal システムの IP は 撮影時のたわみを防ぐために金属板が入っている。そのた め VistaScan よりも厚い。VistaScan の読みとり装置を Figure 2Eに示す。撮影後の IP は保護カバーを付けた状 態で挿入口に設定する。その後,IP をゆっくり押し込む (Figure 2F)。数センチ押し込んだところで装置自体が IP の自動取り込みと読み込みをはじめ,装置下方にある出口 から IP が排出される(Figure 2G)。ピクセルサイズは もっとも細かい 12.5μm で読み取りを行った。Digora Occlusal で 18 画 像,VistaScan で 9 画 像, 計
27のデジタル画像を作成した。いずれも読み取り時のす べての情報が含まれているビット数(Digora Optime は 14ビット,VistaScan は 16 ビット)で画像を出力した。 4.比較対象画像について デジタル画像の比較評価のためにフィルム画像を作成し た。撮影条件はデジタル撮影と同じとした。使用したフィ ル ム は Insight(Eastman Kodak Rochester, NY, USA) で あ る。 撮 影 後 は 自 動 現 像 機 Dent・X(AFP Imaging Co. NY, USA)を用いて通法に従って写真処理を行い,画 像を得た。 5.画像評価方法 デジタル画像は Image J(Ver.1.43)を用いて,1600
×
1200ピクセルのモニタに表示し,評価した。フィルム はシャウカステン上で評価した。 観察者は歯科放射線専門医 3 名,臨床経験が 22 年の一 般開業医 1 名の計 4 名とした。 評価項目は,1.顎骨内の構造,すなわち皮質骨や骨梁 構造を指摘でき,何らかの圧迫性ないし浸潤性の病変に よって膨隆などの変化が認められたときに,その変化を検 出するに足る画質といえるか,2.顎骨内の解剖学的構造 物,すなわち鼻腔切歯管の位置や正中口蓋縫合の連続性を 指摘でき,しかもこの部位が何らかの病変によって侵され たときにその変化を検出するに足る画像といえるか,3. 歯・歯根尖周囲・歯周組織を指摘でき,この部位に透過性 病変,歯根の移動などがみられるときに,その変化を検出 するに足る画像といえるか,4.埋伏歯があった場合,そFigure 1 Digora Optime II Comfort Occlusal 4C start-up kit
A : Size 3 Imaging Plate (IP); B: Protective covers; C: Two IPs covered with a protective cover; D: Comfort OcclusalTM 4C bite protector ; E and F : Slightly overlapped two Comfort OcclusalTM 4C IPs in a bite protector envelope ; G : Hygienic bag ; H : Prepared occlusal kit containing two IPs with protective cover set in a Comfort OcclusalTM 4C bite protector that prevents imaging plate wear and bite damage.
Figure 2 VistaScan Mini system
A : Occlusal size Imaging Plate ; B : Protective bag ; C and D : Comparison of thickness of size 4 imaging plates, used for VistaScan Mini (C) and Digora Optime (D). D is thicker than C.; E : VistaScan Mini scanner ; F : Insertion of exposed IP into the scanner by hand ; and G : Ejection of scanned IP toward the bottom of the scanner.
歯科放射線 51 巻 3 号 松田 の輪郭ならびにその位置を指摘することができ,しかもそ の存在によって周囲の歯や骨梁の構造の変化を判断するの に足る画質といえるか,の 4 項目とした。 評価の基準は 1:不十分である 2:やや不十分である 3:十分である 4:良い 5:優れている の 5 段階評価 とした。さらに,評価 1,2 を合わせて「容認できない」 に,評価 3 を「容認できる」に,評価 4.5 を「良好」の 3段階でも評価した。 6.統計処理 フィルムの評価結果を基準とした。二等分法と軸投影の 撮影法別に,さらに IP を左右に並べて撮影した画像(縦 IP),IP を前後に並べて撮影した画像(横 IP)ごとに撮 影条件の違いによる画質評価への影響について評価した。 統計処理は,一元配置の分散分析を行い,その後の検定は Tukey検定を行った。有意差 5%未満を持って有意差あり と判定した。 結 果 撮影時間 0.03 秒,0.06 秒,0.12 秒で撮影された咬合法 のフィルム画像,Digora Occlusal の縦 IP および横 IP を 用いた画像,VistaScan 画像を Figure 3 に示す。0.03 秒 ではフィルムと VistaScan 画像ではノイズがやや目立つ 傾向があった。 撮影時間別にみた各システムの評価結果を Table 1 に示 した。フィルムによる 0.06 秒の画像は観察者の評価がす べて 5 と一致していた。Digora Occlusal は同じ撮影条件 ではやや低く,縦 IP が 4.6,横 IP が 4.5 であった。統計 学的にはシステム間の違い(film,縦 IP と横 IP,Vis-taScan)による有意差は認めなかったが,撮影時間につ いては 0.03 秒の撮影画像の評価は,0.06 秒および 0.12 秒と比較していずれも危険率 0.0001 未満で有意な差を認 め,いずれのシステムでも線量を減らすことによって評価 が下がる傾向を認めた。 全体としてはフィルム,VistaScan,Digora Occlusal の縦および横 IP との間には有意差を認めなかったのに対 し,撮影時間 0.03 秒の評価だけを同様の統計分析で比較 したところ,フィルム,VistaScan と,Digora Occlusal の縦および横 IP との間には危険率 0.0001 未満で有意な 差を認めた。線量を 0.03 秒に減らした画像ではフィルム と VistaScan の平均の評価が 3 と急激に低くなったのに 対して Digora Occlusal の縦 IP が 4.0,横 IP が 3.8,で あった。 フィルムは 0.06 秒の画像すべてが評価 5 で平均が 5 で あったが,VistaScan は平均 4.2 であった。VistaScan は その倍の時間である 0.12 秒の画像の評価がすべて 5 で あった。撮影時間 0.12 秒の画像の評価の平均をみると, フィルムがやや低い 4.8,Digora Occlusal の縦 IP では 4.5とやや低くなる傾向にあった。さらに横 IP では評価 が 3.6 とさらに低くなる傾向を示した。 同じ撮影条件では Digora Occlusal の縦と横の IP 評価 を比較すると,縦 IP のほうが横 IP よりも評価が高くな る傾向にあった。 評価項目別に “良好”,“容認できる”,“容認できない” の 3 段階に分けて表示したのが Figure 4 である。“容認で きない”という評価が多かったのは,項目 1 の上顎骨の 概形,項目 3 の歯槽骨と根尖部の見えやすさについての 評価であった。さらに,“容認できない”という評価は, フィルムと VistaScan に多く,フィルムではすべての評 価項目に“容認できない”という評価を認めた。 Table 2 にシステムおよび照射時間別に Figure 4 と同 様に評価を 3 段階に分けた結果を示す。各々の撮影条件 と撮影システムで撮影された 3 画像に対し,評価者 4 人 が,4 つの評価項目について評価するため,各システムの 撮影条件ごとに全体で 48 の評価数が得られる。0.06 秒で は,フィルム,縦横 IP の Digora Optime では評価数すべ ての 48 評価が,VistaScan でも 45 評価が“容認できる” という結果であったのにくらべ,線量を半分の 0.03 秒に した場合,Digora Occlusal では縦横 IP ともに“容認で きない”は皆無であったが,フィルムでは 17 評価,Vis-taScanでは 12 評価が“容認できない”であった。また, 線量を倍にした 0.12 秒では,Digora Occlusal の横 IP の 画像以外はすべての評価が容認できるという結果になった。 考 察 Digora Occlusal は IP を 2 枚連ねて撮影するというユ ニークな方法で咬合法撮影を行うシステムである。Vis-taScanは大きな咬合法サイズの IP を用いて撮影するシス テムである。今回我々はこれらの画像についてフィルムと 比較評価することを目的とした。Digora Occlusal では二 等分投影法について,さらに口腔内での IP の置き方によ る診断への影響についても検討を行った。 咬合法撮影に関する研究論文は矯正治療に関連したもの が多い。Sannomiya ら14は咬合法撮影を用いて,外科的 急速拡大装置による正中の口蓋縫線の部分の骨濃度の評価 を, ア ル ミ ニ ウ ム 当 量 を 用 い て 評 価 し て い る。 ま た, Witcherらの研究13では,矯正治療において生じる可能性 のある歯根吸収や,歯列不正の原因となる埋伏歯の有無や その程度を咬合法とパノラマエックス線撮影とで比較し, 前歯部については咬合法のほうが正確であったと報告して おり,被曝線量を減らすためにもパノラマよりも咬合法を 推奨している。 咬合法のデジタル画像についての研究としては,Mas-chtakow PSら15の報告がある。咬合法の撮影で線量が多 い,あるいは少なかった場合に,フィルムをデジタル入力
し,それを画像処理することで診断可能な画像にすること ができるかどうかを評価している。彼らは,診断に最適な 画像が得られた撮影時間は 0.4 秒,それに対して,75%の 0.3秒まで撮影時間を短縮することができたこと,また, 標準の 157.5%の 0.63 秒まで線量を増やして撮影したフィ ルムでも,デジタル処理することで診断できる画像が得ら れたと報告している。この論文では,フィルムをデジタル 処理することで少ない線量でも診断可能な画像が得られる 可能性を示している。 本研究では,フィルムは照射時間 0.06 秒の画像で最も 高い平均評価点の 5 点が得られたが,VistaScan はその倍 の 0.12 秒の画像が最も高い評価点であった。一方,照射 時間が半分になると平均評価点はどちらも 3.0 と急激に落 ち込んだのに対し,Digora Occlusal での縦 IP を用いた 場合の評価点は 4.0,横 IP でも 3.8 であった。このこと から,線量を減らした場合,Digora Occlusal のほうが
Figure 3 Samples of occlusal image obtained by each system
Film and VistaScan Mini images exposed at 0.03 seconds were clearly less dense compared with images exposed at 0.06 seconds. Images obtained by the Digora Optime II Comfort system were less affected by differences in ex-posure time than film images. Images obtained by the VistaScan Mini using an exex-posure of 0.12 seconds had the highest visibility of anatomical structures.
歯科放射線 51 巻 3 号 松田 フィルムや VistaScan よりも高い評価点を得ることがで きたことから,Digora Occlusal は線量による画質への影 響が少ない可能性が示された。同じ IP システムでもこの ような線量による評価の違いが出た理由としては,読み取 りの装置が違うことによる可能性が考えられる。 また,我々の過去の研究で,口内法撮影画像を用いた齲 蝕診断の研究では,D 感度のフィルムの 8 分の 1 までの 線量低減が可能であったが16,咬合法ではそこまでの線量 の低減は困難かもしれない。これは,標準口内法の二等分 法と比べて,咬合法の二等分法は広い範囲が撮影対象とな り,その分だけ範囲内にある構造物のエックス線不透過性 の差が大きくなり,線量を減らすと不透過性の高い部分の 情報量が少なくなるからである。実際に今回の研究でも線 量を減らしてしまうと評価が低くなる傾向にあったが,線
Table 1 Mean and standard deviation (SD) of ratings for each system and exposure time
Time(sec) Film Digora IP(V) Digora IP(H) VistaScan
0.03 0.06 0.12 3.0(1.11) 5.0(0) 4.8(0.41) 4.0(0.58) 4.6(0.50) 4.5(0.50) 3.8(0.43) 4.5(0.50) 3.6(0.67) 3.0(0.89) 4.5(0.63) 5.0(0) A one-way ANOVA test with p<0.05 was used to analyze differences between each modality. No statistically significant differences were seen among the modalities tested. However, statistically significant differences were seen for images exposed at 0.03 seconds versus those exposed at 0.06 and 0.12 seconds. Film of images obtained at 0.06 seconds exposures and the VistaScan Mini images at 0.12 seconds exposure showed higher rates than those at any other exposure time or modality. For images obtained at 0.03 seconds exposure, the average rates of film and VistaScan Mini were clearly lower than for the Digora Optime II system.
Figure 4 Evaluation data for anatomical features and each system
For the Digora Optime II Comfort system, IP (V) and IP (H) mean that IPs positioned vertically and horizon-tally were used, respectively.
Film was rated unacceptable more often than any of the other systems tested. The Digora system with verti-cally oriented IPs was rated good more often than film or the Digora system with horizontal IPs. None of the images obtained by the Digora system with vertical IPs were rated unacceptable. For the film and VistaScan Mini systems, assessments of unacceptable occurred only for the visibility of maxilla outlines, and alveolar and apical regions.
量を減らした画像でも Digora Occlusal の評価値はフィル ムや VistaScan 画像よりも良好な結果が得られていた。 Digora Occlusalは対数応答システムを用いていることか ら,このような解剖学的な厚みの差にも対応することがで きたのではないかと考えられる。 一方,線量が多い場合,有意差は見られなかったが Di-gora Occlusal画像の評価がやや低く,濃度やコントラス ト補正などの画像処理をしても改善されないことが示唆さ れた。これは線量が多い画像では画像処理をしても評価が 変わらなかったという Maschtakow ら15の結果と一致し ていた。線量が多い場合には VistaScan は良好な評価で あった。VistaScan では撮影時間が 0.12 秒の画像では最 も高い評価を得られたが撮影時間が 0.03 秒の画像の評価 は最も低かった。このように VistaScan は少ない線量の 場合,評価が低くなることが示されたが,少ない線量でも 効率よく画像を作成するためには,IP の発光を光電子増 倍管に導く効率,つまり光学効率を上げるための対策が必 要なのかもしれない。 IP の並べ方による画像の評価には統計学的に差はな かったが,一般に縦 IP に比べ横 IP 画像の評価は低くな る傾向にあった。特にこれは,評価 4 の埋伏歯の有無の 診断しやすさを評価するという項目で低くなる傾向にあっ た。縦 IP の画像に比べ,横 IP の場合は,本来の解剖学 的な構造物ではない口蓋縫線や歯に直交する IP の線が見 えてしまうため,診断の妨げとなったのかもしれない。 IPの読み取りは,IP をライトガイドによる読み取り方向 に動かしながら(副走査)レーザー光を IP に平行に当て て(主走査)読み取りを行う。このため,読み取り装置の 読み取り特性はレーザー照射の均一性と光電子増倍管の感 度安定性に影響する。読み取り方向による画像の大きさな どの影響の有無について確認するために以下の検討を行っ た。 厚 さ 0.03mm の 鉛 製 Type14 の エ ッ ク ス 線 テ ス ト チャート(極光株式会社,神奈川)を IP 上に設置して, 撮影を行った。次にテストチャートの向きを 90 度変えて 撮影した画像を作成し,二つの画像のチャートの大きさお よびラインペアの比較を行った。その結果,計測値の違い はわずか数ピクセル,ラインペアはいずれも 10lp/mm で あり,読み取りの方向による影響はほとんどないことを確 認することができた。本研究では,縦 IP に比べて横 IP の評価が低くなる傾向にあったが,この結果も踏まえて考 えると,IP の読み取りの方向による影響はほとんどない こと,IP を横に重ね合わせて撮影した場合,歯および口 蓋縫線と直交する IP の重ね合わせの線という本来の正常 解剖には見られない像ができてしまったことによる視覚的 な影響が大きかったために,評価が低くなった可能性があ る。 以上の結果から,Digora Occlusal システムならびに VistaScanシステムは,線量が同じもしくは多い場合には フィルムと同等の評価が得られた。口蓋縫線と直交するよ うに IP を並べて撮影する場合には,評価が低くなる傾向 にあった。線量による影響は Digora Occlusal のほうが VistaScanよりも小さいと考えられた。VistaScan システ ムの場合にはフィルムと同様に線量が少なくなると評価が 下がる傾向を示した。フィルムと同じ線量では Digora Occlusalシステム,VistaScan システム画像でもほぼす べてが良好という結果が得られ,これらのイメージングプ レートを使った咬合法システムはいずれもフィルムと同等 の評価を得られることが明らかになった。 文 献
1) Ludlow JB, Mol A. Digital imaging. In: White SC, Pharoah MJ, editors. Oral radiology : principles and interpretation. Missouri : Mosby Elsevier ; 2004:p.225-244.
2) Dunn SM, Kantor ML. Digital radiology. Facts and fic-tions. J AmDent Assoc. 1993;124:38-47.
3) Vandre RH, Webber RL. Future trends in dental radiology.
Table 2 Rating frequencies for 4 anatomical features with each system and exposure time
Time (sec.) 0.03 0.06 0.12
System Film Digora
IP(V) DigoraIP(H)VitaScan Film DigoraIP(V) DigoraIP(H) VitaScan Film DigoraIP(V) DigoraIP(H)VitaScan unacceptable fair good 17 10 21 0 8 40 0 12 36 12 24 12 0 0 48 0 0 48 0 0 48 0 3 45 0 0 48 0 0 48 2 18 28 0 0 48 The five ratings used for evaluation were summarized into three categories as follows. 1 : unacceptable and 2 : poor were put together as “unacceptable”; 3: fair was unchanged; and 4: good and 5: excellent were put together as “good”. No images acquired using the Digora with vertical IPs were rated as unacceptable.
Images obtained using film, the Digora system with vertical and horizontal IPs, and the VistaScan Mini system, were almost always rated good when the exposure time was 0.06 seconds. When the exposure time was 0.03 seconds, however, images obtained using film and the VistaScan Mini system were rated fair or unacceptable more often. In fact, more than one quarter of the images acquired using film and the VistaScan Mini system when using an exposure of 0.03 second were rated unacceptable, whereas images acquired by the Digora system were all rated good or fair.
歯科放射線 51 巻 3 号 松田 Oral Surg Oral Med Oral Pathol Oral Radiol Endod.
1995;80:471-478.
4) Kashima I. Computed radiography with photostimulable phosphor in oral and maxillofacial radiology. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1995;80:577-598.
5) Kitagawa H, Farman AG, Scheetz JP, Brown WP, Lewis J, Benefiel M, Kuroyanagi K. Comparison of three intra-oral storage phosphor systems using subjective image quality. Dentomaxillofac Radiol. 2000;29:272-276.
6) Kashima I. Computed radiography with photostimulable phosphor in oral and maxillofacial radiology. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1995;80:577-598.
7) Borg E. Some characteristics of solid-state and photo-stim-ulabl phosphor detectors for intra-oral radiography. Swed Dent J Suppl. 1999;139:1-67.
8) Hildebolt CF, Couture RA, Whiting BR. Dental photostim-ulable phosphor radiography. Dent Clin N Am. 2000;44: 273-297.
9) Wenzel A, Frandsen E, Hintze H. Patient discomfort and crossinfection control in bitewing examination with a stor-age phosphor plate and a CCD-based sensor. J Dent. 1999;27:243-246.
10) Kalathingal SM, Shrout MK, Comer C, Brady C. Rating the extent of surface scratches on photostimulable storage phosphor plates in a dental school environment.
Dento-maxillofac Radiol. 2010;39:179-183.
11) Matsuda Y, Sur J, Arak i K, Okano T. Durability of Digora Optime imaging plates. Oral Radiol. 2011;27:28-34. 12) White SC, Pharaoh MJ. Part IV Imaging principles and
techniques. In : White SC, Pharaoh MJ. ed. Oral Radiolo-gy : Principles and interpretation. 6th ed. St Louis : Mosby Elsevier ; 2009:p.147.
13) Witcher TP, Brand S, Gwilliam JR, McDonald F. Assess-ment of the anterior maxilla in orthodontic patients using upper anterior occlusal radiographs and dental panoramic tomography : a comparison. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010;109:765-774.
14) Sannomiya EK, Macedo MMC, Siqueira DF, Goldenberg FC, Bommarito S. Evaluation of optical density of the midpalatal suture 3 months after surgically assisted rapid maxillary expansion Dentomaxillofac. Radiol. 2007;36: 97-101.
15) Maschtakow PS, Moraes ME, Soares MG, Santos LR, Moraes LC, Castilho JC. Assessment of manipulation ac-curacy of digitized occlusal radiographic images--sub and over exposure. Acta Odontol Latinoam. 2009;22:113-117.
16) Matsuda Y, Okano T, Igeta A, Seki K. Effects of exposure reduction on the accuracy of an intraoral photostimulable-phosphor imaging system in detecting incipient proximal caries. Oral Radiol. 1995;11:11-16.