Posted at the Institutional Resources for Unique Collection and Academic Archives at Tokyo Dental College, Available from http://ir.tdc.ac.jp/
Author(s)
Alternative Terakawa, Y; Ichinohe, T; Kaneko, Y
Journal Regional anesthesia and pain medicine, 34(6): 553-556
URL http://hdl.handle.net/10130/2185
Right
This is a non-final version of an article published in final form in Reg Anesth Pain Med. 2009 Nov-Dec;34(6):553-6
Title Page
Redistribution of tissue blood flow after stellate ganglion block in the rabbit
Yui Terakawa, DDS* Tatsuya Ichinohe, DDS, PhD† Yuzuru Kaneko, DDS, PhD ‡
*Postgraduate student
†Professor and Chairman ‡Professor
Department of Dental Anesthesiology, Tokyo Dental College
Address correspondence to; Yui Terakawa, DDS
Department of Dental Anesthesiology, Tokyo Dental College
1-2-2, Masago, Mihama-ku, Chiba 261-8502, Japan
Telephone number: +81-43-270-3970
Fax number: +81-43-270-3971
Financial source: n.a
Meetings: The 283th Annual meeting of Tokyo Dental College Society
The 36th Annual meeting of Japanese Dental Society of Anesthesiology
Abstract
Background and Objectives: The goal of this study was to compare tissue blood flow at
various sites before and after stellate ganglion block (SGB), and discuss the redistribution of
tissue blood flow after SGB.
Methods: We utilized 16 male Japan White rabbits. For SGB, the tip of the 26-gauge needle
was placed on the left transverse process of the cervical vertebra, 1-2 mm caudal to the cricoid
cartilage. Either 0.2 ml of 1 % lidocaine (Lidocaine group) or normal saline solution (Saline
group) was injected. In Lidocaine group, data were recorded immediately before SGB and at
the time when the maximal change in common carotid artery blood flow (CCBF) was observed
after SGB. In Saline group, data were recorded immediately before SGB and 3 minutes after
SGB. Observed variables were blood pressure, heart rate, CCBF, tongue mucosal blood flow
(TMBF), mandibular bone marrow blood flow (BBF), masseter muscle blood flow (MBF),
quadriceps muscle blood flow (QBF), liver blood flow (LBF) and renal blood flow (RBF).
Results: CCBF, TMBF, BBF and MBF on the block side were increased whereas BBF and
MBF on the non-block side, QBF, LBF and RBF were decreased after SGB in Lidocaine
group.
flow on the non-block side are redistributed to the block side after SGB. In addition,
redistribution from peripheral tissue may have more important role than that of visceral blood
flow after SGB.
Key Words: Stellate ganglion block - Redistribution of tissue blood flow - Face - Lower limb
Introduction
Stellate ganglion block (SGB) increases regional tissue blood flow in head, face, neck and
upper limb depending on its sympatholytic effects.1 SGB is useful for the treatment of several
disorders such as orofacial pain including postherpetic neuralgia. 2,3
It has been reported that an increase in regional tissue blood flow on the block side is
attributable to the redistribution of that on the non-block side.4,5 Cerebral blood flow,4 and
common carotid arterial blood flow (CCBF) and brachial arterial and venous blood flow5 were
increased after SGB whereas those on the non-block side were decreased.4,5 Meanwhile, there
is a report that facial skin blood flow was bilaterally increased after SGB.6 In addition, blood
flow of celiac artery, which is not innervated by the cervical sympathetic fibers, was increased
after SGB.7 It is assumed that there should be a region where tissue blood flow decreases to
balance with increased blood flow on the block side after SGB because circulating blood
volume is constant. This blood flow decrease might result in inadequate tissue oxygenation at
these sites. However, the change of tissue blood flow distribution before and after SGB
remains unknown.
In this study, therefore, we compared tissue blood flow before and after SGB, and
tongue mucosal blood flow (TMBF), mandibular bone marrow blood flow (BBF), masseter
muscle blood flow (MBF), quadriceps muscle blood flow (QBF), liver blood flow (LBF) and
Methods
Sixteen male Japan White rabbits (2.2-2.7kg) were utilized. Rabbits were purchased from
Sankyo Labo Company, Tokyo. This study was performed according to The Guidelines for the
Treatment of Experimental Animals in Tokyo Dental College. All animals were allowed food
and water ad libitum until the morning of the experiment. The animals were randomly
allocated in two groups: Lidocaine group (n=8) and Saline group (n=8).
Anesthesia was induced by inhalation of 4.0% isoflurane in oxygen delivered using
a mask. Before skin incisions for each of the experimental procedures, appropriate doses of
lidocaine were injected into the surgical field. A #20 Fr non-cuffed pediatric tracheal tube was
inserted into the trachea through tracheostomy. The left auricular marginal vein and right
femoral artery were cannulated with 22- and 20-gauge Teflon indwelling catheters,
respectively. After intravenous acetated Ringer’s solution was started at 10 ml/kg/hr, the
animals were paralyzed with 14 mcg/kg/min rocuronium bromide (Eslax, Schering-Plough,
Tokyo) and mechanically ventilated. End-tidal partial pressure of carbon dioxide (ETCO2) was
maintained at about 35mmHg. Femoral artery blood pressure was continuously monitored with
a pressure transducer (P231D; Gould, Oxnard, California). Heart rate (HR) was recorded by a
flowmeter (T108; Transonic, Ithaca NY). A flow probe (type 3SB) was applied to the isolated
left common carotid artery. TMBF was measured with a laser Doppler flowmeter (ALF21;
Unique Medical, Tokyo). A contact-type probe (type C; Unique Medical) for TMBF
measurement was placed at the anterior third of the left dorsal surface of the tongue. Care was
taken to minimize the contact pressure of the probe to prevent blood flow disturbance in the
tongue mucosa. Systolic blood pressure (SBP), diastolic blood pressure (DBP), mean arterial
pressure (MAP), HR, CCBF and TMBF were continuously recorded on a polygraph
(Series360 NEC; Sanei, Tokyo).
After the skin incision along both left and right lower margins of the mandible
without local anesthesia, the periosteum of the mandibular body was exposed. The periosteum
was detached to expose the surface of the mandibular body on both side. Two small holes
(approximately 1 mm in diameter, one in the left side and the other in the right side)
perforating into the bone marrow through the cortical bone were drilled with a round bar (ISO.
008, Morita, Japan). Needle probes of a hydrogen clearance tissue blood flowmeter (UHE-100,
Unique Medical, Japan) were inserted 3mm deep into the left and right bone marrow to
measure both left BBF (L-BBF) and right BBF (R-BBF), respectively. In addition, the fascia of
probes of the hydrogen clearance tissue blood flowmeter were inserted 3mm deep into the left
and right masseter muscle to measure left MBF (L-MBF) and right MBF (R-MBF),
respectively. Then, after the skin incision along the left femoral region without local anesthesia,
the quadriceps muscle was exposed. A needle probe of the hydrogen clearance tissue blood
flowmeter was inserted 5mm deep into the center of the left quadriceps muscle to measure
QBF. Furthermore, after midline laparotomy, two needle probes of the hydrogen clearance
tissue blood flowmeter were inserted 5mm and 2mm deep into the right lobe of the liver just
below xiphoid process of the sternum and the left renal cortex to measure LBF and RBF,
respectively.
After completion of experimental preparations, isoflurane inhalation was
discontinued. Then, inhalation of sevoflurane was started at 1.8% of end-tidal concentration
and maintained at that level for more than 60 min to stabilize the hemodynamic and respiratory
parameters. Sevoflurane concentration was continuously monitored with an anesthetic gas
monitor (Capnmac; Datex, Helsinki). Body temperature was continuously monitored with a
rectal probe and maintained between 39.0 and 39.5℃ with the aid of a heating lamp.
For SGB, the tip of the needle was placed on the left transverse process of the
ml disposable syringe was used.8 After confirming contact of the tip of the needle with the left
transverse process, either 0.2 ml of 1 % lidocaine (Lidocaine group) or 0.2 ml of normal saline
solution (Saline group) was injected. In Lidocaine group, data were recorded immediately
before SGB (Pre) and at the time when the maximal change in CCBF was observed after SGB
(Post). In Saline group, data were recorded immediately before SGB (Pre) and 3 minutes after
SGB (Post).
In this study, data were expressed as the mean ± standard deviation. The paired t-test
was used for within-group comparisons and the unpaired t-test for between-group comparisons.
P values less than 0.05 were considered statistically significant. All blood flow data in
Results
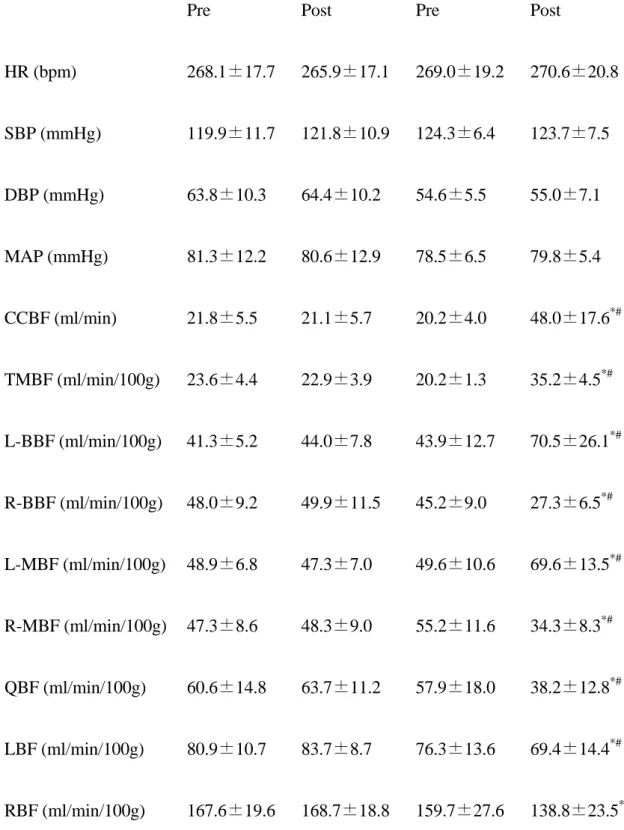
Time for the maximal effect was 2.6 ± 0.2 min in Lidocaine group. There were no
differences in respective Pre values between two groups. In Saline group, there were no
differences between Pre and Post values for all observed variables. In contrast, in Lidocaine
group, significant changes from Pre to Post values were observed in CCBF, TMBF, BBF, MBF,
QBF, LBF and RBF. In addition, there were significant differences in respective Post values
between two groups. (Table 1)
In Lidocaine group, Post values for CCBF, TMBF, L-BBF and L-MBF were
significantly increased by 138%, 75%, 60% and 40% in comparison with Pre values,
respectively. In contrast, Post values for R-BBF, R-MBF, QBF, LBF and RBF were
significantly decreased by 40%, 38%, 34%, 9% and 13% in comparison with Pre values,
Discussion
This study showed that CCBF, TMBF, L-BBF and L-MBF were increased whereas R-BBF,
R-MBF, QBF, LBF and RBF were decreased in Lidocaine group after SGB.
Stellate ganglion was confirmed by exposing cervical sympathetic nerve trunk in our
preliminary study. When SGB was performed based on these results, CCBF was increased
immediately after SGB in a reproducible manner. Consequently, SGB was performed by the
technique written in the method session in this study.
In a previous study, minimum alveolar concentration (MAC) of sevoflurane is 1.5 to
1.8 times as high as that of isoflurane. 9 Therefore, isoflurane was used for induction of
anesthesia and experimental preparations in this study because isoflurane was able to induce
anesthesia more smoothly than sevoflurane. Anesthesia was maintained with 1.8% sevoflurane
throughout experiment. This concentration was equal to almost 0.5 MAC of sevoflurane in the
rabbit.9-12 Sevoflurane has less sympatholytic effects than isofluraneand these effects occur at
the level higher than 0.75 MAC of sevoflurane. 13 Therefore, sevoflurane might minimally
modify the sympatholytic effects of SGB.
In our pilot study, infusion rate of rocuronium bromide which provided stable
based on a previous study8 and the results of our pilot study, Post values in Saline group were
recorded 3 minutes after SGB. This was almost equal to the time for the maximal change in
CCBF in Lidocaine group. Blood flow in the internal carotid artery (ICA) was increased after
SGB with 2% lidocaine.14 In cases of facial palsy, CCBF and blood flow of the facial nerve
were increased after SGB with 1% mepivacaine.15 CCBF and TMBF were significantly
increased after SGB with 1% lidocaine.8 Based on these reports, it is suggested that the
significant increase in CCBF in this study was caused by the effect of SGB.
An increase in CCBF is dependent on an increase in cardiac output (CO). Increase in CO
is supplied by an afterload (total peripheral resistance) reduction and increases in HR, cardiac
contractility and/or preload (venous return). In this study, no change in HR was observed. In
addition, cardiac contractility and venous return should not increase after SGB because of its
sympatholytic effect. Therefore, it is suggested that significant increase in CCBF was
attributable to CO increase through afterload reduction (vasodilatation). Although afterload
decrease may induce hypotension, blood pressure was unchanged after SGB in this study.
Tissue blood flow in the block side was increased because peripheral vascular resistance at head,
neck and upper limb was decreased after SGB. In contrast, it was speculated that peripheral
and lower limb were decreased. Therefore, total peripheral resistance might minimally change
in this study. As a result, blood pressure should be unchanged throughout the experiment. This
means that afterload decrease observed in this study was a regional phenomenon based on the
effect of SGB.
Although changes in CCBF result from changes in the blood flow in both ICA and
external carotid artery (ECA), ICA blood flow under normal condition should minimally
change because of the autoregulatory mechanisms of cerebral blood flow. In contrast, ECA
blood flow may change depending on the degree of activations of alpha- and beta-adrenergic
receptors, which innervate blood vessels of skin and mucosa (alpha-adrenergic receptors
dominant) and skeletal muscles (beta-adrenergic receptors dominant).16 Bone marrow blood
flow may change depending on blood pressure. It is suggested that the increases in BBF, MBF
and TMBF on the block side in Lidocaine group resulted from afterload reduction caused by
the sympatholytic effects of SGB. In this study, TMBF and L-MBF were significantly
increased by 75% and 40% in comparison with respective Pre values in Lidocaine group.
Since alpha-adrenergic receptors dominantly exist in the vasculature in head and neck area16, it
may be reasonable that the increase in TMBF was more than that in L-MBF in this study.
redistribution of that on the non-block side.4,5 However, in this study, QBF, LBF and RBF,
which are out of the sympatholytic effects of SGB, as well as R-BBF and R-MBF on the
non-block side were decreased. Therefore, it is suggested that the increase in blood flow on the
block side is redistributed from not only the non-block side but also lower limb and viscera.
The blood flow of quadriceps muscle, well-vascularized liver and renal cortex17 were adopted
as indicators that were not affected by the sympatholytic effects of SGB in this study.
Quadriceps muscle can be a good indicator for the blood flow of muscular tissue like the
masseter muscle. Similarly, liver and renal cortex can be good indicators for the blood flow of
visceral organ. Biceps brachii muscle blood flow was decreased by 40% whereas liver and
renal blood flow were decreased by 25% to 30% during deliberate hypotention with
trinitroglycerine.18 Hindlimb blood flow was decreased by 60% whereas cerebral blood flow
remained unchanged during deliberate hypotention with sodium nitroprusside.19 When the
circulating blood volume is constant, there is a fundamental mechanism to control tissue blood
flow in vital and non-vital organs as needed through the change of the vascular bed. 20
However, the mechanism of blood flow redistribution is still unclear and to be investigated in
future. Therefore, it is suggested that peripheral tissue blood flow decreased in a compensatory
were less decreased in comparison with peripheral MBF, TMBF and QBF in this study. Renal
blood flow was decreased by 40% during deliberate hypotention whereas this decrease never
reached the critical level.21 Additionally, there are no reports of impaired liver function during
deliberate hytotention in patients with nomal liver function. 22 In this study, changes in visceral
blood flow after SGB might be of no clinical significance because the decrease in LBF and
RBF were slight and blood pressure showed no major change. Based on the previous studies
and the results of this study, it is suggested that blood flow in peripheral tissue such as lower
limb has more important role on the increase in tissue blood flow after SGB in comparison
with visceral blood flow.
In clinical situations, palm skin temperature at the block side was elevated while that
at the non-block side was lowered following upper thoracic sympathetic ganglion block. 23 In
addition, when lumbar sympathetic ganglion block was performed to the patients with
arteriosclerosis obliterans of lower limbs, blood flow on the non-block side was decreased.24
Therefore, it is suggested that blood flow redistribution to the block side from the non-block
side and the other parts of the body after unilateral sympathetic ganglion block might cause
“steal” phenomenon. Attention should be paid to patients undergoing SGB who have bilateral
There are some reports focusing on the effect of SGB on coronary hemodynamics.
It is reported that SGB has deteriorative effects on the myocardial oxygen supply-demand
relationship with normal coronary circulation in the dog. 25 In that study, coronary artery blood
flow was measured whereas myocardial oxygen consumption and oxygen extraction ratio were
calculated. In addition, myocardial blood flow and tissue oxygen tension were not measured.25
Therefore, the effect of SGB on coronary hemodynamics still remains controversial and is to
be investigated.
In conclusion, it is suggested that lower limb and visceral blood flow as well as the
non-block side are redistributed to the block side after SGB. Peripheral tissue blood flow has
References
1) Barash PG, Cullen BF, Stoelting RK. Peripheral nerve blockade. In: Mulroy MF. Clinical
Anesthesia. 2nd ed, Philadelphia, PA: Lippincott, 1992.
2) Milligan NS, Nash TP: Treatment of post-herpetic neuralgia. A review of 77 consecutive
cases. Pain 1985; 23: 381-386.
3) Salvaggio I, Adducci E, Dell’vAquila L et al: Facial pain: a possible therapy with stellate
ganglion block. Pain Med 2008; 9: 958-962.
4) Yamazaki Y, Mimura T, Iwasaki F, Namiki A: Regional cerebral blood flow and
oxygenation following cervicothoracic sympathetic block. Masui 1998; 47: 1233-1236.
5) Okuda Y, Kitajima T: Influence of stellate ganglion block on bilateral cervicobrachial
arterial and venous blood flow. Masui 1994; 43: 1201-1206.
6) Kakuyama M, Toda H, Osawa M, Fukuda K. The bilateral effect on stellate ganglion block
on the facial skin blood flow. Reg Anesth Pain Med 2000; 25: 389-392.
7) Mineta M, Takeda Y, Matoba M et al: Change of the blood flow in celiac artery and superior
mesenteric artery after stellate ganglion block. Masui 1993; 42: 1808-1812.
8) Terakawa Y, Handa M, Ichinohe T, Kaneko Y: Epinephrine in local anesthetic cancels
Coll 2007; 48: 37-42.
9) Scheller MS, Saidman LJ, Brian L: MAC of sevoflurane in humans and the New Zealand
White rabbit. Can J Anaesh 1988; 35: 153-156.
10) Ichinohe T, Homma Y, Kaneko Y: Mucosal blood flow during various intravenous and
inhalational anesthetics in the rabbit. Oral Surg Oral Med Oral Pathol Oral Radiol Endod
1998; 85: 268-271.
11) Kemmochi M, Ichinohe T, Kaneko Y: Remifentanil decreases mandibular bone marrow
blood flow during propofol and sevoflurane anesthesia in rabbits. J Oral Maxillofac Surg
2009; in press.
12) Handa M, Ichinohe T, Kaneko Y: Changes in partial pressure of arterial carbon dioxide
induces redistribution oral tissue blood flow in the rabbit. J Oral Maxillofac Surg 2008; 66:
1820-1825.
13) Akata T, Kobama K, Takahashi S: Volatile anesthetic action on norepinephrine-induced
contraction of small splanchnic resistance arteries. Can J Anesth 1995; 42: 1040-1050.
14) Liu F, Xu G, Liu Z, Zhao Y, Lv X, Wang J: The effects of stellate ganglion block on visual
evoked potential and blood flow of the ophthalmic and internal carotid arteries in patients with
15) Murakawa K: Changes in microcirculation in the facial nerve with electrical stimulation
and chemical blockade of cervical sympathetic trunks. Masui 1993; 42: 646-652.
16) Thomas CW, David PW. Neurotransmission. In: Westfall TC, Westfall DP. Goodman &
Gilman’s The Pharmacological Basis of Therapeutics. 11th ed. New York, NY: Lippincott
Brunton LL, Lazo JS, Parker KL, 2006.
17) Brezis M, Rosen S. Hypoxia of the renal medulla -its implications for disease. N Engl J
Med 1995; 332: 647-655.
18) Kobori M, Negishi H, Hosoyamada A. Influence of hypotensive anesthesia on the organ
blood flow –Comparison of trinitoroglycerine and nicardipine-. Masui 1995; 44: 956-962.
19) Chang CL, Yeh FC, Ho W, Chen HI. Effects of sodium nitropurusside-induced hypotention
on the cerebral and hindlimb blood flow in dogs. Proc Natl Sci Counc Repub China B 1985; 9:
202-207.
20) DeBakey ME, Burch G, Ray T et al: The borrowing- lending hemodynamic phenomenon
(Hemometakinesia) and its therapeutic application in peripheral vascular disturbances. Ann
Surg 1947; 126:850-865.
21) Kick O, Aken HV, Wouters PF, Verbesselt K, Hemelrijck JV. Vital organ blood flow during
22) Rodrigo C. Induced hypotention during anesthesia, with special reference to orthognathic
surgery. Anesth Prog 1995; 42: 41-58.
23) Hashizume K, Yamagami A, Yoshikawa M, Furuya J. Clinical evaluation of “borrowing-
lending” phenomenon in the upper limbs following upper thoracic sympathetic ganglion block.
Pain Clinic 1996; 17: 389-392. (In Japanese)
24) Baron HC, Hiesiger E, Sabri M. Undesirable effects of hemometakinesia induced vascular
reconstruction. Surg Gynecol Obstet 1979; 148: 534-538.
25) Sasaki I, Kaneko T, Iwatsuki N, Hashimoto Y. Effects of stellate ganglion block on
Tables
Table 1 Hemodynamic variables and blood flow data
Saline group Lidocaine group
Pre Post Pre Post
HR (bpm) 268.1±17.7 265.9±17.1 269.0±19.2 270.6±20.8 SBP (mmHg) 119.9±11.7 121.8±10.9 124.3±6.4 123.7±7.5 DBP (mmHg) 63.8±10.3 64.4±10.2 54.6±5.5 55.0±7.1 MAP (mmHg) 81.3±12.2 80.6±12.9 78.5±6.5 79.8±5.4 CCBF (ml/min) 21.8±5.5 21.1±5.7 20.2±4.0 48.0±17.6*# TMBF (ml/min/100g) 23.6±4.4 22.9±3.9 20.2±1.3 35.2±4.5*# L-BBF (ml/min/100g) 41.3±5.2 44.0±7.8 43.9±12.7 70.5±26.1*# R-BBF (ml/min/100g) 48.0±9.2 49.9±11.5 45.2±9.0 27.3±6.5*# L-MBF (ml/min/100g) 48.9±6.8 47.3±7.0 49.6±10.6 69.6±13.5*# R-MBF (ml/min/100g) 47.3±8.6 48.3±9.0 55.2±11.6 34.3±8.3*# QBF (ml/min/100g) 60.6±14.8 63.7±11.2 57.9±18.0 38.2±12.8*# LBF (ml/min/100g) 80.9±10.7 83.7±8.7 76.3±13.6 69.4±14.4*# RBF (ml/min/100g) 167.6±19.6 168.7±18.8 159.7±27.6 138.8±23.5*#
HR: heart rate; SBP: systolic blood pressure; DBP: diastolic blood pressure; MAP: mean
arterial pressure; CCBF: common carotid artery blood flow; TMBF: tongue mucosal blood
flow; BBF: mandibular bone marrow blood flow; MBF: masseter muscle blood flow; QBF:
quadriceps muscle blood flow; LBF: liver blood flow; RBF: renal blood flow
L: left side; R: right side
Pre: immediately before SGB
Post: at the time when maximal change in CCBF was observed after SGB (Lidocaine group) or
3 minutes after SGB (Saline group)
mean ± standard deviation (n=8)
*p<0.05 vs Pre
#
Legends for figures
Fig. 1 Changes in tissue blood flow in the Lidocaine group.
Data were expressed as the percentage of respective Pre value in the Lidocaine group.
CCBF: common carotid artery blood flow; TMBF: tongue mucosal blood flow; BBF:
mandibular bone marrow blood flow; MBF: masseter muscle blood flow; QBF: quadriceps
muscle blood flow; LBF: liver blood flow; RBF: renal blood flow
L: left side; R: right side
Pre: immediately before SGB
Post: at the time when maximal change in CCBF was observed after SGB (Lidocaine group) or
3 minutes after SGB (Saline group)