185
Longitudinal analysisof HamiltonDepression Rating Scale(HDRS)
scores
北里大学 薬学研究科 松本正入 (MasatoMatsumoto)
CENTERFOR CLINICAL PHARMACY AND
CLINICAL SCIENCES KITASATO UNIVERSITY GRADUTE SCHOOL
ABSTRACT
Antidepressants
are
generally evaluatedon
the basis of the Hamilton Depression Scale Scores ofthesame
patients measuredrepeatedlyover
time.The usual analysis ofthe
scores
measuredat the end of the treatmentperiod alone is,however, inadequate.Toclarify the characteristic features of the test drugs, it is necessary to analyze the
longitudinalpatterns.
In this
paper, we
have analyzed actual clinical trial data in terms of longitudinalchange ofthe
score
ofindividual subjects classified into three patterns (1. No variation,2. Linear improvement, and3. Earlyimprovement). The clinical validity andusefulness
of the analyticalmethod presented
are
alsoexamined.Keywords: antidepressant, evaluationof drugeffect, repeated measurements
INTRODUCTION
For the treatment of depression, TCAs (tricyclic antidepressants) have been
widely used
so
far. In 1999, SSRI (Selective Serotonin Reuptake Inhibitor)was
put onJapanese market. Afterthat, other SSRIs and SNRI (SerotoninNoradrenaline Reuptake Inhibitor)
were
puton
the market. From the many antidepressants,a proper
antidepressant is chosen for each patient. For theproper
choice, it is meaningful tocharacterize the antidepressants. In actual, a lot of meta-analyses (Examples are [1-81.) andthecomparison examinations (Examples
are
[9-12].)havebeen alreadyperformed.The effects of antidepressants
are
generally evaluated using Hamilton Depression Rating Scale (HDRS) introducedby${\rm Max}$Hamiltonin1960
[13-15]. HDRS consists of 17 items and the totalscore
of the17
items is used for themeasure
ofseverity of depression. The maximum and minimum of the total
score
48 points and 0186
point, respectively. In clinical trials, HDRS
scores
are repeatedly measuredon
eachpatient. Adecreaseinthe total indicates the improvementinthe symptoms.
The efficacy ofantidepressant isevaluatedbased onthe
mean
ofthe decrease ofHDRS
scores
at the final measurement point. In the current evaluation, however, thelongirudinal pattern of HDRS
scores
of each patient is not considered. From clinicalviewpoints, the evaluation $\mathrm{i}^{\sigma_{\mathrm{i}}}$ not appropriate. Longitudinal patterns of HDRS
scores
after the administration of
an
antidepressantcan
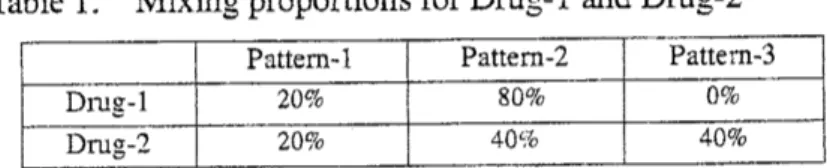
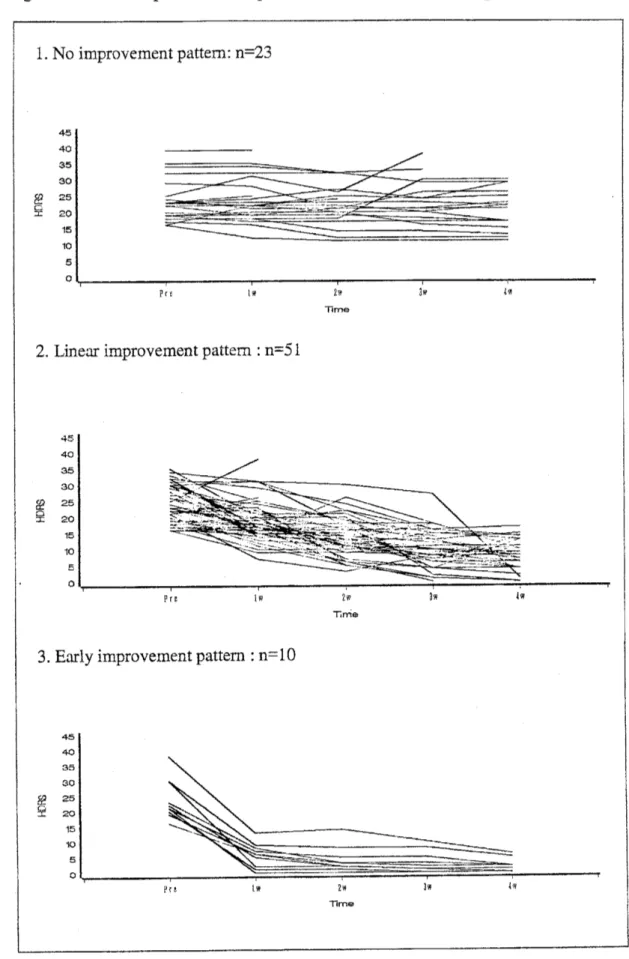
be grouped into the three patternsshown in Figure 1. In Pattern-l, pretreatment
scores
are
maintained. This pattern corresponds to non-responders. Pattem-2 and Pattem-3 correspond to responders. InPattern-2,HDRS scoresdecrease almost Iinearlv. InPattern-3,the
scores
decreasemore
rapidly. The patient population
can
be considered as amixture of patients with the threepatterns. We here
suppose
two drugs, Drug-l and Drug-2, for which the mixingproportionsof the three pattems
are
listedinTable 1.Table 1. Mixingproportions for Drug-l andDrug-2
If the evaluation is made based only on the
mean
of the decrease at the final measurement point, the proportion of responders is 80% in either drug. However, 40%of the patients in Drug-2 show Pattem-3 and respond
more
rapidly. It is clear that Drug-2 is clinically more preferable. Suchan
evaluation can not be made if thelongitudinal patterns of HDRS
scores are
not considered. The efficacy ofantidepressants should be evaluatedbasedonthe longitudinalpatternsofHDRS
scores.
We apply mixture modelsto actual clinicaldata ofHDRS
scores.
Weassume
thefollowing three pattem $\mathrm{s}$ for the longitudinal patterns of HDRS scores, 1. No
improvementpattern,2. Linear improvementpattern,and 3.Early improvementpattem. In applying mixture models, it is
common
toassume
that longitudinal patterns can be described by low-degree polynomials of elapsed time after the beginning oftreatment [16-19]. However, the low-degree polynomial models
are
not necessarilyappropriate for describing the longitudinal patterns ofHDRS
scores.
In Chapter 3 We proposea
model usinga
monotone decreasing function to describe the early187
improvement pattem. Furthermore, $\mathrm{V}\mathrm{Y}^{7}\mathrm{e}$ investigate variance-covariance structures
within a subject. In Chapter 4, YVe conduct simulation studies to evaluate the
performance of the proposed model in Chapter 3. In the chapter of discussion, YVe arrange the resultin this study. We derive the conclusion by present. And YVe refer the
problemof theproposedmethod and theviewofthe future.
MOTIVATING EXAMPLE
The present data
are
HDRSscores
of84
patients ina
randomized, double-blind,comparative study of antidepressants. Thecriteria for selecting the subjects
are
that thetotal
score
forHDRS items 1-17was
16
or
higher and thedepressive moodscore
ofwas
$\underline{0}$orhigher,beforethe start of the treatment. Theantidepressants
were
given for4weeks,following a fixed-flexible regimen. The main item ofevaluation
was
the final general improvement rating (FGIR) $\mathrm{e}\backslash _{t}$aluated by the physicians, taking into account thechanges in the HDRS
scores
and the clinical symptoms. FGIRwas
classified into eightcategories, $\mathrm{i}.\mathrm{e}.$, significant improvement, moderateimprovement, mild improvement,
no
change, slight worsening, worsening, serious worsening andimpossible to evaluate. The
HDRS
scores
were
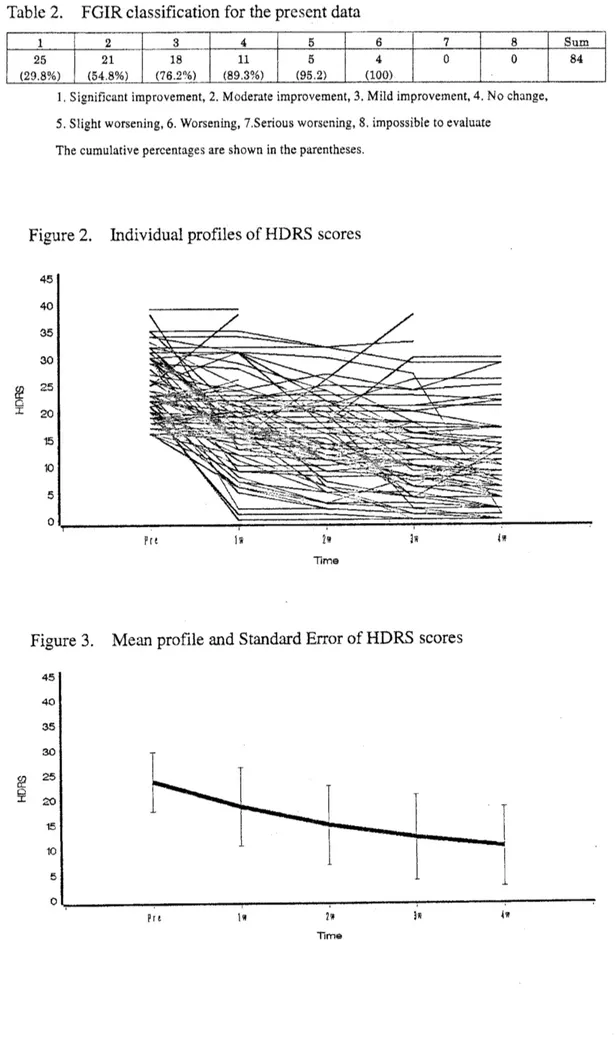
evaluated at five measurement points, i.e., before the treatment and1, 2, 3 and 4 weeks after the beginning of the treatment. The individual and mean profiles of HDRS
scores are
shown in Figure 2 and Figure 3, respectively. FGIR classificationfor thepresent datais shown inTable2.189
Table 2. FGIR classificationforthepresentdata1.Significantimprovement, 2.Moderateimprovement,3.Mild improvement,4,Nochange,
5. Slight worsening, 6.Worsening,7 Serious worsening,S.impossibletoevaluate
The cumulative percentagesareshowninthe parentheses.
Figure2. Individual profiles of HDRS
scores
TIrne
Figure 3. Mean profile and Standard ErrorofHDRS
scores
$[mathring]_{\ddagger \mathrm{Z}}\mathrm{a}\mathrm{e}$
190
MIXTURE DISTRIBUTIONMODELFOR
LONGITUDINAL
DATAMixture distribution models are often applied to the analysis of longitudinal
pattems ofrepeated measurements [16-19].
In this chapter, mixture distribution models
are
applied to HDRSscore
dataobtainedin
an
actual clinical trial of antidepressants.(1) The model
As stated in the first chapter, longitudinal patterns of HDRS
scores
after theadministration of antidepressants
are
grouped into three patterns. We define the threepatterns asfollows.
1. No improvement pattern: the
scores
show no improvement maintaining thepretreatment
scores.
2. Linear improvementpattern: the
scores
show almost linearimprovem $\mathrm{e}\mathrm{n}\mathrm{t}$.3. Earlyimprovementpattern: the
scores
showrapid improvement.These th $\mathrm{e}^{\alpha}$
.
patter $\mathrm{s}$ correspond to the three patterns shown in Figure 1. All of thesubjectsxe assumed tobelong to
one
ofthe $\mathrm{t}\mathrm{h}\mathrm{r}\mathrm{e}^{\Delta}$.
patter $\mathrm{s}$.Let yij denote the HDRS
score
of the patient $\mathrm{i}(\mathrm{i}=1,\cdots, \mathrm{n})$ at the measurementpoint$\mathrm{t}_{\mathrm{j}}$ $(\mathrm{i}=1,\cdots, 5)$. In themixture distribution model, the probability density function
of the observation vector$\mathrm{y}_{\mathrm{i}}=(\mathrm{y}_{\mathrm{i}1},\cdots, \mathrm{y}_{\mathrm{i}5})$ isgiven by
$g$
(
$\mathrm{y}_{\mathrm{i}}$ I$\mathrm{p},8$
)
$= \sum_{m=1}^{3}p_{m}\cdot f_{m}$($\mathrm{y}_{\mathrm{i}}$ I$8_{m}$), (1)where $\mathrm{y}_{i}=(\mathrm{y}_{\mathrm{i}1},\mathrm{y}_{\mathrm{i}2},\mathrm{y}_{13},\mathrm{y}_{\mathrm{i}4},\mathrm{y}_{\mathrm{i}5})^{\mathrm{f}}$ is the measurement vector for the patient
$\mathrm{i}$, $\mathrm{p}=(\mathrm{p}_{1}, \mathrm{p}_{\underline{\gamma}}, \mathrm{p}_{3})$ $(\mathrm{p}_{1}+\mathrm{p}_{-}’\lrcorner_{-}\mathrm{p}_{3}=1)$ isthe vector ofthe mixingproportions ofthethree patterns,$f_{m}$ (
$\cdot$ ) is the
densityfunction forthe m-thpattern$(\mathrm{m}=1,2,3)$, $\mathrm{e}_{\mathrm{m}}$is the vector of theparameters that
defmethe densityfunction$f_{\mathfrak{l}n}$ $($
.
$)$ $(\mathrm{m}=1,2, 3)$,$\mathrm{e}$ $=(8_{1}^{\mathrm{t}}, 8_{2}, {}^{\mathrm{t}}\mathrm{e}_{3}^{\mathrm{t}})^{\mathrm{t}}$denotes the vector of
all the parametersin $6_{1},6_{2}$ and
63.
For the threelongitudinal pattem $\mathrm{s}$statedabove,We
assume
thefollowing model.1. No improvementpattem
I
E1I
$L’)$. Linear improvementpattern
$\mathrm{y}_{ij}=(\alpha_{-},+\mathrm{b}_{2\mathrm{i}})+\beta_{2}\cdot \mathrm{t}+\epsilon_{\mathrm{o}_{1}}\mathrm{i}\sim \mathrm{J}$
3.
Earlyimprovementpattem$y_{ij}=\exp(-(\mathrm{t}_{\mathrm{j}}/\alpha_{3})^{\beta_{\mathrm{j}}})\cdot(\gamma_{3}+\mathrm{b}_{3\mathrm{i}})+\epsilon_{3\mathrm{i}\mathrm{j}}$ ,
Inthis model, it is assumed thatthe pretreatment
scores
a1, a2, and$\mathrm{a}_{3}$are
common
to allthepatients ,$\mathrm{b}_{1\mathrm{i}}$, $\mathrm{b}\underline{\circ}\mathrm{i}$ and$\mathrm{b}_{3\mathrm{i}}$
are
thepatient-specific variations of the pretreatmentscores
normallydistributed
as
$\mathrm{b}_{1\mathrm{i}}\sim \mathrm{N}(0, \mathrm{s}_{\mathrm{b}12})$, $\mathrm{b}_{-:},\sim \mathrm{N}(0, \mathrm{s}\mathrm{b}22)$ and$\mathrm{b}_{3\mathrm{i}}\sim \mathrm{N}(0, \mathrm{s}\mathrm{b}22)$,respectivelyandeiij, $\mathrm{e}_{2\mathrm{i}\mathrm{j}}$ and $\mathrm{s}3\mathrm{i}\mathrm{j}$ is the error term normally distributed with
mean
0 andvariance-covariance matrix $\Sigma_{\mathrm{s}1},\Sigma_{\epsilon^{\underline{\gamma}}}$ and $\Sigma_{\mathrm{s}3}$, respectively. The function of early
improvementpattern
comes
from the following:1–(theWeibulldistributionfunction)$=1-(1-\exp(-(t/\alpha_{3})^{\beta_{3}}))=\exp(-(t/\alpha_{3})^{\beta_{3}})$,
This function is parsimonious and useful for describing monotone decreasing function.
In addition, this function
can
beused for describing thefeature ofHDRSpattern that thevariance for the early improvement pattern becomes smaller
as
the clinical trialadvances. Thedetailsaregivenlater.
(2) The
variance-covariance
within apatientFor the
variance-covariance
matrices of theerror
terms, the following threestruc
rures
are employed: simple variance (SV), first-order autoregressive $(\mathrm{A}\mathrm{R}(1))$, andtoeplitz (TOEP), which are commonlyused in the analysis ofclinical longitudinal data
[20].
When SV is assumed, the
variance-covariance
matrix of the marginal distribution becomes a compound symmetry type in the no improvement pattern andlinearimprovementpattemasfollows:
$\ovalbox{\tt\small REJECT}_{1}^{1}1\ovalbox{\tt\small REJECT} 11^{\cdot}[\sigma_{bm}^{2}]\cdot[1 1 1 1 1]+\{$$\sigma_{\epsilon_{0}0^{m}}^{2}00$
$\sigma_{m}^{2}0000$ $\sigma_{m}^{2}0000$ $\sigma_{m}^{2}0000$ $\sigma_{\epsilon m}000\ovalbox{\tt\small REJECT} 0_{2}$
,$\mathrm{m}=1,2$.
1
EI2
$\ovalbox{\tt\small REJECT}_{\exp(}^{\exp(}\exp\{\exp\langle\exp\langle-\langle 4/\alpha_{3})^{\beta_{3}})-(2/\mathrm{a}_{3})^{p_{3}})-(0/\alpha_{3})^{\beta\underline{\tau}})-(3/\alpha_{3}\}^{\beta 3})-(1/\alpha 3)^{\beta 3})\ovalbox{\tt\small REJECT}$ .
$[_{\sigma_{b3}}2]\ovalbox{\tt\small REJECT}_{\exp\{}^{\exp(}\mathrm{e}\mathrm{x}.\mathrm{p}(\exp(\exp(-(2/\alpha_{3}\rangle^{\beta 3})\ovalbox{\tt\small REJECT}^{t}\wedge(0/\alpha_{3}\rangle^{\beta 3})-(4/\mathrm{a}_{3}\}^{\beta_{3}})-(3/\alpha_{3})^{\beta_{3}})-(1/\alpha_{3})^{\beta 3})+\ovalbox{\tt\small REJECT}$
a
$\epsilon_{0}30002$ $\sigma_{\mathrm{s}_{0}3}000_{\wedge}$
”
$\sigma_{\epsilon_{0}3}0\mathrm{o}_{\wedge}\mathrm{o}_{9}$ $\sigma_{\epsilon_{0}3}0_{2}00$ $\sigma\epsilon 300\ovalbox{\tt\small REJECT} 002$
From this structure, it is found that the variance becomes smaller
as
the clinical trialadvances and that the covariance becomes smaller as the interval between the
measurement points becomes longer.
(3) Results
Table 3 shows the number of theparameters, maximum $10^{\sigma}\underline{\sim}$likelihood andAIC
[21-23] for the three variance-covariance structures, $\mathrm{S}\mathrm{V}$, $\mathrm{A}\mathrm{R}(1)$,
or
TOER The AICsindicate that the
variance-covariance
structure $\mathrm{A}\mathrm{R}(1)$ is the bestamong
the threestructures.
Table
3.
Thenumberofthe parameters, maximum$\log$ likelihoodandAICfor theThe result when $\mathrm{A}\mathrm{R}(1)$ is assumed is shown
as
follows. Table 4 lists themaximum likelihood estimates of the parameters and their standard
errors.
Figure 4163
Table4. Themaximumlikelihood estimates(MLE) and theirstandard
errors
Pattem Parameter MLE $\mathrm{S}.\mathrm{E}$.
$\mathrm{p}1$ 0.298 0.030
$\alpha 1$ 22.4 1.762
1. Noimprovementpattem $\sigma$
$\mathrm{b}$$12$ 8.43 2.639 $\sigma$ $p$ $12$ 40.4 2.349 $p1$ 0.875 o.oos $\mathrm{p}2$ 0.581 0.122 $a\mathrm{z}$ 23.4 0.818
2. Linear improvementpattern
$\mathcal{B}\mathrm{r}$ -4.0 0.285
$\sigma$$\mathrm{b}2^{2}$
o.oo
3.847$\sigma$ $\epsilon$ $2^{2}$ 33.6 3893 $\beta 2$ 0.553 0.066 $\mathrm{p}$a 0.121 $\alpha_{\mathit{3}}$ 0.283 0.053
3. Early improvement pattern
$\beta_{3}$ 0.309 0.070 $\gamma s$ 23.5 3.554 $\sigma$$\mathrm{b}3^{2}$ 31.9 9 $6\hat{0}6$ $\sigma$ $P$ $3^{2}$ 11.5 0477 $\rho s$ 0.859 0.011
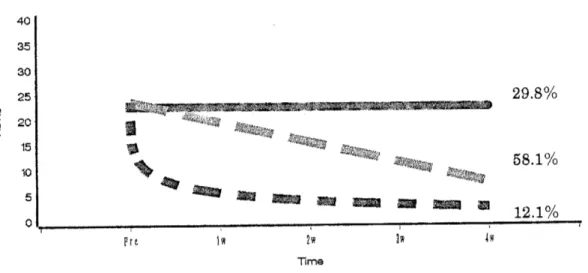
Figure4. Theestimated
mean
profiles of HDRSscores
for the three pattem $\mathrm{s}$$[mathring]_{\mathrm{x}}\not\in$
194
Given the estimatesfor all the parameters, the probabilities that the patient $\mathrm{i}$ with
the data $\mathrm{y}_{\mathrm{i}}$belongs to each of the three patterns
can
be estimated by Bayes theorem[24-26]. By assuming that each patientbelongs to the pattern forwhich the probability
is the largest, thepatientscanbeclassifiedintothethree patterns. Theproportions of the
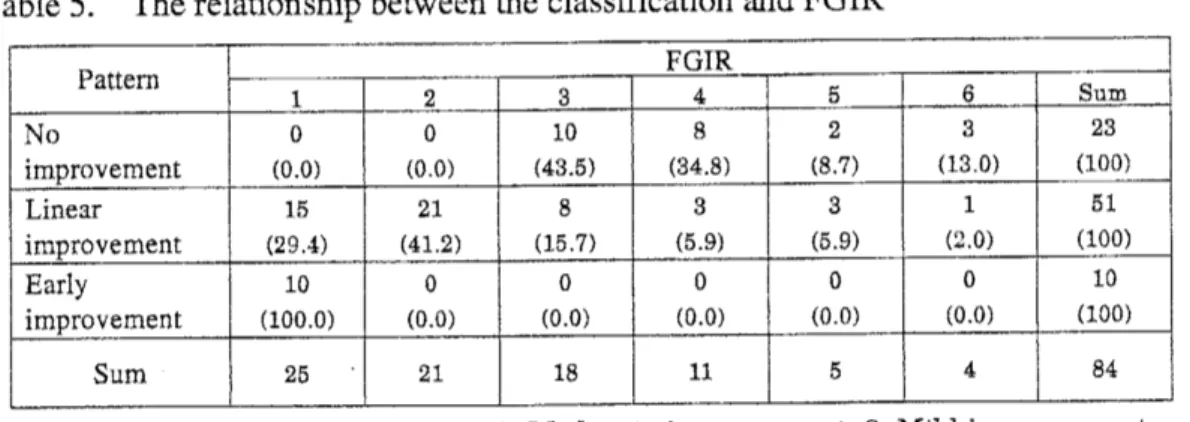
patients classified into the three patterns are 27.4%(23/84: No improvement), 60.7% (51/84: Linear improvement) and 11.9% (10/84: Early improvement). The relationship
between theclassification andFGIR measured in the clinicaltrial is shown in Table 5.
Figure 5 shows theindividual profiles ofthepatientsclassified intothe three patterns.
Table
5.
Therelationshipbetween theclassification and FGIR4.No change,5. Slight worsening,6.Worsening
185
198
From the results assuming the variance-covariance structure $\mathrm{A}\mathrm{R}(1)$, the following
points
can
befound1. The estimated pretreatment
scores are
22.4,23.4
and 23.5 for the noimprovementpattern, linear improvementpattern and earlyimprovementpattem,
respectively. There
seems
tobeno greatdifferencesamongthe three patterns.$\mathrm{i}\mathrm{i}$
.
The estimated mixing proportionsare
29.8%, 58.1%, and 12.1% for the noimprovementpattern, linear improvementpattem, andearly improvement pattem, respectively. About 70% of the patientsbelong to eitherthe linearimprovement
pattern
or
earlyimprovementpattern.$\ddot{\dot{\mathrm{m}}}$. The estimated
scores
at 1 week after thebeginning of the treatmentare 19.4
and5.4 in the linear improvement pattern and early improvement pattern,
respectively. The estimated
scores
at 2 weeksare
15,4 and 3.8 in the linearimprovement pattern and early improvement pattem, respectively. The results
suggest that the HDRS
scores
had been improved clinically well enough at 1week in theearlyimprovementpattern.
$\mathrm{i}\mathrm{v}$
.
The estimatedscores
atthe final measurementpoint(4weeksafter thebeginningof the treatment)
are
22.4,7.4
and 2.4 in theno
improvement pattern, linearimprovement pattern and early improvement pattern, respectively. The HDRS
scores were
improvedinboth the linear andearly improvementpatterns.$\mathrm{v}$. The estimated probabilities that each patient belong to each ofthe three patients
rangefrom
0.504
to 1.000 withmean 0.892.
25,50
and75 percentilesare
0.836,0.966
and0.998,respectively.$\mathrm{v}\mathrm{i}$
.
Theproportionsof thepatients classified into the three patternsare
27,4% (23/84),60.7% (51/84), and 11.9% (10/84) for the
no
improvement pattem, linearimprovement pattem, and early improvement pattern, respectively. These
are
almostthe
same as
theestimatesof themixing proportion.$\mathrm{V}\vec{11}$
.
The relationship between the results of the classificationand FGIR indicates thatall the patients classified into the early improvement pattern showed the significant improvement in FGIR and that about
85
% of the patients classified into the linear improvement pattern showed the mildor
better improvement in FGIR. On the otherhand, thepatientsclassified intotheno
improvement pattern1S7
did not show themoderate
or
betterimprovementin FGIR.SIMULATION
STUDY:DETECTION
OF TRUE VA RIANCE-COVARIANCESTRUCTURE
When repeated measurements of HDRS
scores are
analyzed using the mixture distribution model consisting ofthe three patterns (no improvement, linear improvement,andearlyimprovement)presented in Chapter3, it is importantto examine the influence of the assumption of the within-subject covariance structure on the parameter estimates. In this chapter,the following two simulation studies
are
conductedtoexamine thisissue.Inthe simulation study, We suppose the situation inwhich themodel with thetrue
within-subjectcovariance structureis includedin the appliedmodels. Under this situation,
it is examined whether the selected model
can
detect the true structure of thewithin-subject covariance. In addition, We examine the influence of the mis-specified
within-subjectcovariancestructure
on
the accuracyof the parameterestimates.In this simulation study, thefollowing three structures, $\mathrm{S}\mathrm{Y}$,
$\mathrm{A}\mathrm{R}(1)$, and TOEP are
assumed for the within-subject covariance structure. T.a$\mathrm{b}\mathrm{l}\mathrm{e}$ $6$ shows the true values of the
parameters. Thesevalues
are
determinedby referring to theresultsin Chaper3.Underthe true structure, 100 data sets
are
simulated. Each data setconsistsof thedata of 100 subjects. For each data set, the three mixture distribution models with the
within-subject covariance structure$\mathrm{S}\mathrm{V}$,$\mathrm{A}\mathrm{R}(1)$, and TOEP
are
appliedand the goodness ofeach model isevaluatedbased
on
theAIC[21-23].Table 7 shows the proportions that each mixture distribution model is selected based
on
AIC. The proportion that the true within-subject covariance structure model is selected is about95% for each of the three within-subjectcovariance structure. Thisresultsuggests thattheproposed approach
can
selectthe truewithin-subjectcovariance structureunderthe situation in which the modelwith the true within-subject covariance structureis
includedinthe appliedmodels.
The description of the result is omitted, and the following is confirmed. The
accuracy of the estimates is especially worsened for the following
cases:
SV is assumedwhen the true structure is $\mathrm{A}\mathrm{R}$, and SV
or
$\mathrm{A}\mathrm{R}(1)$ is assumed when the true structure is198
199
DISCUSSION
It is problem from clinical viewpoints that the efficacy of antidepressant is evaluated based
on
themean
ofthe decrease of HDRSscores
at the final measurement point, becausethe longitudinal$\mathrm{p}\mathrm{a}\mathrm{t}\mathrm{t}\frac{-}{}.\mathrm{m}$ofHDRSscores
of eachpatient isnotconsidered.In thepresent study,
we
have evaluated the results on thebasis of$1\mathrm{o}\mathrm{n}_{arrow}\sigma$-itudinalpatterns.Byevaluating the averagechanges ineach pattern and the $\mathrm{m}\dot{\mathrm{L}}\mathrm{X}\mathrm{i}\mathrm{n}_{\underline{arrow}}\sigma$proportions, we could
quantitatively evaluate the early onset of
a
characteristic feature of the drug. Theanalyses at each time point cause the statistical problem ofmultiplicity, and the results
are
difficulttounderstand. Because theobjective ofthe analyses ateachtimepoint istoevaluate
on
the longitudinal patterns,the evaluationispossibleby thismethod.The results ofthis study and the clinical evaluation (FGIR) of the subjects have
acertain level ofagreement. Therefore,
we can
conclude that this method isappropriatefrom theclinical pointofview. Theresults suggest that FGIR isan evaluation inwhich
longitudinalpatterns
are
takeninto account. By classifying the subjects intoone
of thethree patterns,
we can
examine the differences in background factors among subjectshaving these differentpattems.
By applying thismethod, itis possible to execute comparisonbetween drugs by themixtureproportions of the drug. Thenullhypothesis ofcomparisonbetween Drug-l andDrug-2 inthiscaseisasfollows.
$\mathrm{H}_{0\mathrm{P}\mathrm{m},\mathrm{D}\sigma- 1^{=\mathrm{p}_{\mathrm{m},\mathrm{I}\supset \mathrm{r}\mathrm{u}\mathrm{g}-\underline{0}}}}:\mathrm{r}\mathrm{u}_{\mathrm{s}}$ : $\mathrm{m}=1,2,3$,
where$\mathrm{p}_{\mathrm{m}}$ismixingproportionof m-th pattern.
This partwillneed examining inthe future.
One problem with this methodis how to decide
on
the number ofpatterns to beused. This has not been solved in the present study. In this study, the analysis is done
assuming 3 patterns, taking into account the observed data and
an
easiness of clinicalexplanation. When the number of patterns is decided,
we
should decide it in considerationofa
feature ofthe drug andaclinical meaning.In the analysis ofthis study,
we
assumed that all the subjects belonged toone
ofthe three variation pattem $\mathrm{s}$. It is quite possible that data of
some
subjects may beintermediate between twopatterns in fact. Areas tobe studied in the future include the
200
The variance-covariance structure within a patient is actually unknown. It is
necess
ary to investigate the influence of misspecification thevariance-covariance
structure within a patient. In actual analyses, it is quite difficult to specify the correct
variance-covariance
structure withina
subject. It will be desirable touse
a robustestimationmethod against the $\mathrm{m}\mathrm{i}\mathrm{s}$-specification cf
variance-covariance
structure withinasubject.
REFERENCES
1. Bech P. A meta-analysis of the antidepressant properties of serotonin reuptake
inhibitors.International Review ofPsychiatry 1990; 2: 207-211
2. Sitsen$\mathrm{J}_{1}^{\backslash }\cdot \mathrm{I}\mathrm{A}$, ZivkovM. Mirtazapine Clinical Profile. CNS Drugs 1995;$4(1)$:
39-48
3. Grimsley SR, Jann MW Drug Reviews: Paroxetine, sertraline and fluvoxamine:
New selective serotoninreuptake inhibitors. ClinicalPharmacy 1992; 11:930-957 4. Kasper S, Fuger J, Moller HI Comparative Efficacy of Antidepressants. Drugs
1992;43(2): 11-23
5. DavisJM, Wang Z, Janicak PG A Quantitative Analysis ofClinicalDrug Trialsfor
the Treatment of Affective Disorders. Psychopharmacology Bulletin
1993
;29(2):175-181
6. Anderson $\mathrm{I}\mathrm{M}_{\sim}$ Tomenson BM. Treatment discontinuation with selective serotonin
reuptake inhibitors comared with tricyclic antidepressants:
a
meta-analysis BMJ1995; 310(3):
14334438
7. MontgomerySA,Kasper S. Comparisonofcompliancebetween serotonin reuptake
inhibitors and tricyclic antidepressants:
a
meta-analysis. International ClinicalPsychopharmacology 1995;$9(4)$: 33-40
8. Moller HJ, VolzHP. Drug Treatment ofDepression in the
1990s.
Drugs 1996;52:
625-638
9.
AnsseauM,PapartP, Troisfontaines B, etal. Controlled comparison of milnacipranandfluoxetine in major depression. Psychopharmacology 1994; 114: 131-137
10.
Remick RA, Reesal R, Oakander M, et al. Comparison of FLUVOXAMINE andAMITRIPTY LINE in depressed outpatients. Cument Therapeutic Research 1994;
55(3):
243-250
11. Artigas F. Selective $\mathrm{S}\mathrm{e}\mathrm{r}\mathrm{o}\mathrm{t}\mathrm{o}\mathrm{n}\mathrm{i}\mathrm{n}/$ Noradrenaline Reuptake Inhibitors(SNRIs)
Pharmacology andTherapeutic Potentialin the Treatment of Depressive Disorders. CNS Drugs 1995;$4(2)$
: 79-89
201
reuptake inhibitors in major depression. International Clinical Psychophamacology
1996; 11(4): 41-46
13. Hamilton M. A rating scale for depression. J.Neurol.Neurosurg.Psychiat 1960; 23: 56-62
14. Hamilton M. Development of a rating scale for primary depressive illness. Brit.
soc.
din. Psychol 1967; 6:278-296
15. WilliamsJBW.Arch GenPsychiatry 1988;45: 742-747
16. Tango T. A mixturemodeltoclassifyindividualprofilesofrepeated measurements. Data science: classification andrelatedmethods 1998; 247-254
17. Tango T. Mixture models for the analysis of repeated measurements in clinical
traials. JapaneseJournal Applied Statistics 1989; 18: 143-161
18. Skene AM,WhiteSA. Alatent classmodel forrepeatedmeasurements experiments. Statist. Med.1992; 11:2111-2122
19. Pavlic M, Brand RJ, Cummings SR. Estimating probability of
non-response
tobeatmentusingmixture
distributions.
Statist. Med. 2001; 20:1739-1753
20.
Verbeke G, Molenberghs G. Linear Mixed Models for Longitudinal Data;2000:
Springer
21. Akaike H. hfomation theory and an extension of the maximum likelihood principle, $2^{\mathrm{n}\mathrm{d}}$ International Symposium on Information Theory. Akademiai Kiado,
Budapest 1973;
267-281
22.
Sakamoto Y, Ishiguro M, Kitagawa G. Akaike Information Criterion Statistics.Reidel, Dordrecht,
1986
23.
Prazen E, Tanalebe K, Kitagawa G. Selected Papers ofHirotugu Akaike. New York: Springer;1998
24.
Lindsay BG Mixture models: theory,Geometry and Applications: Institute forMathematical Statistics; 1995
25. McLachlanQ Basford KE. Mixture models. NewYork: MarcelDekker; 1988 26. McLachlan G, PeelD. Finite mixture models. NewYork: Wiley;200