Cervical Spine Deformity as a Pathophysiological Cause of
Hirayama Disease
Akira YOKOTE, Shinji OUMA, Hiromu OGUR A, Jun TSUGAWA, Yoshio TSUBOI
Department of Neurology, Faculty of Medicine, Fukuoka University
Abstract
Background: Hirayama disease (HD) is a cervical segmental myelopathy characterized by juvenile onset of muscular atrophy in unilateral upper extremity. In HD, cervical spine deformities may be frequent comorbidities; however, details are unknown. The aim of this study was to quantitatively assess cervical spine deformities in patients with HD.
Methods: We enrolled 16 patients with HD and 55 healthy subjects younger than 30 years who underwent cervical spine magnetic resonance imaging (MRI) between January 2009 and December 2015. We evaluated cervical spine sagittal alignment with the neck in neutral position using the following methods: C2–7 Cobb angle, centroid measurement of cervical lordosis (CCL), absolute rotation angle (ARA), C7 slope (C7S), and Ishihara curvature index (ICI) according to previously established reports.
Results: C2–7 Cobb angle, CCL, ARA, and C7S in HD were significantly less than in controls (mean C2–7 Cobb: −4.28°vs 5.15°, p<0.01; mean CCL: −5.15°vs 7.25°, p<0.01; mean ARA: −3.38°vs 9.21°, p<0.01; C7S: 5.97°vs 15.0°, p<0.01). Additionally, ICI in HD was smaller than in controls (mean ICI: −2.00 vs 8.48, p<0.01). There was no statistically significant difference in stage of disease between progression and stable. Conclusions: This study demonstrates cervical spine deformities in patients with HD using multiple quantitative measurements of cervical spine alignment. These findings also indicate that straight neck or even kyphosis is frequently seen in patients with HD compared with controls. Cervical spine deformities might permanently remain and contribute the pathophysiology of the HD.
Key words: juvenile muscular atrophy, Hirayama disease, magnetic resonance imaging (MRI), cervical spine deformity
Introduction
Hirayama disease (HD) is a cervical segmental myelopathy mostly observed among young adults and is primarily prevalent in male adolescents and young men with an onset at around 16 years of age. Clinical features are characterized by unilateral or asymmetrically bilateral weakness and muscular atrophy of the distal upper extremity 1). It progresses for several years after onset; however, progression ends spontaneously. The most important pathophysiologic change in this condition
is that, when the cervical spine is flexed, the spinal cord around the level of C5-6 shifts forward with the posterior dura mater. Magnetic resonance imaging (MRI) reveals that the spinal cord is flattened between the vertebral body and the posterior wall of the dura mater in the flexed position. Also, stagnation in the venous plexus is depicted as a flow void in the posterior epidural space of the posterior wall of the dura mater (Figure 1)2, 3). These findings suggest circulatory insufficiency of the lower cervical spinal cord under these conditions. Hirayama reported histopathological findings in a patient with this condition revealed a decreased number of anterior
Correspondence to: Yoshio Tsuboi, MD, PhD, Department of Neurology, Faculty of Medicine, Fukuoka University 7 -45-1 Nanakuma, Jonan-ku, Fukuoka, 814-0180, Japan.
a
b
c
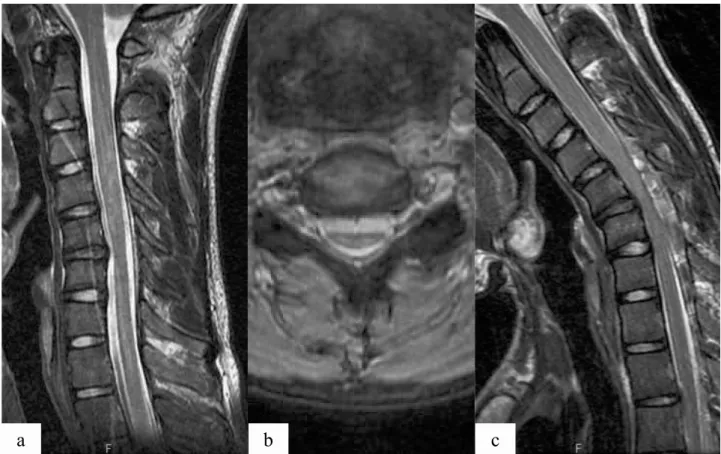
Figure 1. A 17-year-old male adolescent presents with slowly progressive weakness and atrophy of the left upper extremity. His neurological findings are typical features of Hirayama disease.
a: On sagittal T2-weighted cervical magnetic resonance imaging (MRI) in the neutral position, the spinal cord shows marked atrophy at the C5-6 vertebral levels. MRI shows C5-6 disc degeneration. Cervical spine alignment is kyphotic.
b: Axial view of C5-6 shows flattening of the spinal cord.
c: Sagittal T2-weighted cervical MRI in flexion shows expansion of the posterior epidural space and forward displacement of the spinal cord at the C4−6 vertebral levels. Additionally, flow void–like isointensity is seen in the dilated posterior epidural space. — 30 —
horn cells at the lower cervical spinal cord caused by ischemia due to venous congestion 1). It is speculated that this disease process may be caused by an imbalanced development among height, the spinal column, and the dura mater. It has also been reported that the cervical spine deformities tend to co-occur with HD; however, details are unknown. In this study, we have conducted a detailed examination of cervical spine alignment in HD.
Materials and Methods
The subjects of this study were 16 individuals (HD group) who visited our department from January 2009 to December 2015 and were diagnosed with HD based on the clinical course, characteristic neurological symptoms, and MRI (all male subjects; mean age: 19.9 years).
Diagnostic criteria were as follows: ① the onset of symptoms was before the age of 25 years;② the disease progressed gradually, but the progress ended within
several years; ③ unilateral or asymmetrically bilateral distal muscle weakness and atrophy occurred in the upper extremities;④ there was no history of congenital muscle disease, trauma, inflammatory disease, or infectious disease; and ⑤ in the progression stage, cervical MRI showed forward displacement of the posterior wall of the dura mater and expansion of the venous plexus in the epidural space during cervical flexion 4). During the same period, 55 men younger than 30 years who performed cervical MRIs, were included in a control group (age at imaging was between 14 and 30 years, mean age: 22.3 years). MRI was performed for differential diagnosis in the control group, and there were no evidence of cervical spine disorders.
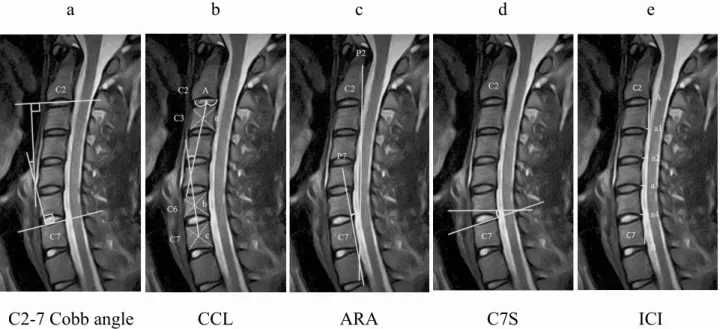
Figure 2. Diagram of cervical spine sagittal magnetic resonance imaging showing five methods of measuring cervical spine alignment. a: C2–7 Cobb angle: The angle between the inferior margin of C2 and the superior margin of C7 is measured.
b: CCL: Vertebral centroid measurement of cervical lordosis.
Points a, b, and c are the centroids of C3, C6, and C7, respectively. Point A is the midpoint of the inferior surface of C2. CCL is estimated from the angle between lines Aa and bc.
c: ARA: Absolute rotation angle.
The posterior margins of C2 and C7 are designated lines P2 and P7, respectively. The angle between P2 and P7 is expressed as the ARA.
d: C7S: C7 slope.
The angle between the superior margin of C7 and horizontal line is measured. e: ICI: Ishihara curvature index.
The posterior inferior corners of C2 and C7 are points A and B. The four distances, a1, a2, a3, and a4, between line AB and the posterior inferior corners of C3–C6, respectively, are measured. ICI is then calculated using the following formula: ICI =(a1 + a2 + a3 + a4)/AB × 100. When posterior inferior points of C3–C6 are behind line CD, the values of a3 to a6 are negative.
angle (ARA), C7 slope (C7S), and Ishihara curvature index (ICI)(Figures. 2a–e)5-10). MRIs were analyzed blinded by two neurologists (S.O., H.O.), and the average values were taken as the results.
Results were analyzed using SPSS version 24 (SPSS, Inc., Chicago, IL), and a significant difference between the two groups was tested using Student’s t-test with p <0.05 taken to be statistically significant.
This study was approved by the Institutional Review Board of Fukuoka University Hospital (Ethical review number 16-2-30).
Results
All individuals in the HD group were male; age at onset was between 13 and 20 years (average 16.3 years); age at imaging was between 14 and 34 years (average 19.9 years); and the period from onset to imaging ranged from 3 months to 19 years (average 2.6 years). In the
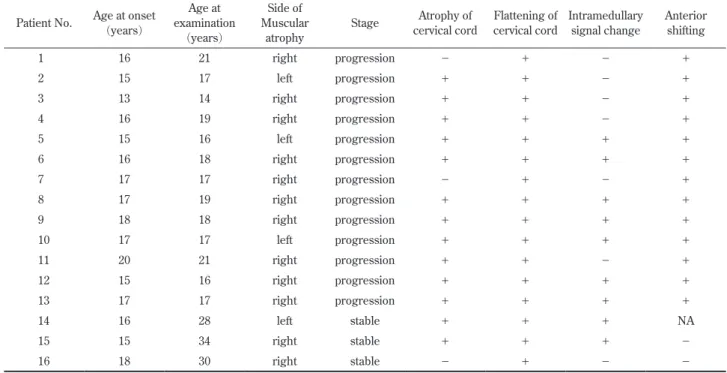
control group, all individuals were male, and the age at imaging was between 14 and 30 years (average age 22.3). There was no statistically significant difference in ages at imaging between the HD and control groups. The right upper extremity was the predominantly affected side in 12 subjects and the left in four subjects. MRI showed 13 subjects to be in the progression stage whereas three were in the stable stage (progression of symptoms had stopped). Cervical MRI in the neutral position revealed spinal cord atrophy in 13 subjects (81.2%), spinal cord flattening in all subjects, and intramedullary high signal intensity on T2-weighted images in nine subjects (56.2%). All subjects, except for one in the stable stage, were evaluated by MRI with the neck flexed; forward displacement of the posterior wall of the dura mater was found in all subjects in the progression stage but was not found in any subject in the stable stage (Table 1).
Table 1. Clinical and neuroradiological characteristics in 16 patients with Hirayama disease.
Patient No. Age at onset (years)
Age at examination
(years)
Side of Muscular
atrophy
Stage Atrophy of cervical cord
Flattening of cervical cord
Intramedullary signal change
Anterior shifting
1 16 21 right progression − + − +
2 15 17 left progression + + − +
3 13 14 right progression + + − +
4 16 19 right progression + + − +
5 15 16 left progression + + + +
6 16 18 right progression + + + +
7 17 17 right progression − + − +
8 17 19 right progression + + + +
9 18 18 right progression + + + +
10 17 17 left progression + + + +
11 20 21 right progression + + − +
12 15 16 right progression + + + +
13 17 17 right progression + + + +
14 16 28 left stable + + + NA
15 15 34 right stable + + + −
16 18 30 right stable − + − −
NA: not applicable
Figure 3. Analysis of cervical spine alignment.
The C2–7 Cobb angle, CCL, ARA, and C7S in Hirayama disease (HD) are significantly reduced compared with controls (mean C2–7 Cobb:−4.28°vs 5.15°, p<0.01; mean CCL:−5.15°vs 7.25°, p<0.01; mean ARA:−3.38°vs 9.21°, p<0.01; C7S: 5.97°vs 15.0°, p<0.01). Additionally, ICI in HD is smaller than in controls (−2.00 vs 8.48, p<0.01).
In HD group, white circle is progression stage and black circle is stable stage. — 32 —
CCL, ARA, and C7S were significantly decreased in the HD group compared to those in the control group (mean C2–7 Cobb:−4.28°vs 5.15°, p<0.01; mean CCL:−5.15° vs 7.25°, p<0.01; mean ARA: −3.38°vs 9.21°, p<0.01; C7S: 5.97 °vs 15.0°, p<0.01). ICI in the HD group was also significantly smaller than that in the control group (− 2.00 vs 8.48, p<0.01). There was no statistically significant difference in stage of disease between progression and
stable.
Discussion
approximately 30% of 333 patients with HD: straight neck in 29 patients, angulation in 30 patients, bony spur in 26 patients, and subluxation in 11 patients. These findings are important auxiliary findings on diagnostic imaging in HD 11). Therefore, for a more quantitative assessment, we used five tests to evaluate abnormalities of cervical spine alignment, and all results indicate that patients with HD tend to have straight neck or kyphosis.
In a previous similar study, Chen et al. assessed cervical spine alignment in 46 patients with HD and in 51 individuals in the control group. They used a different measurement method from ours; they assessed alignment by analyzing the correlation between a line drawn from the dorsocaudal aspect of the C2 vertebral body to the dorsocaudal aspect of the C7 vertebral body and the dorsal aspect of the C3–6 vertebral bodies. Their results indicated that an abnormal cervical curvature is prevalent in patients with HD 12). Xu et al. measured the range of motion of cervical flexion using MRI and plain radiography in 31 patients with HD and in 40 individuals in a control group. They showed that the range of motion was greater in patients with HD 13).
An ethno-specific prevalence of this disease has also been suggested; many cases are reported in Asian countries but few in the United States, France, the Netherlands, and Denmark. Furthermore, cases among siblings have been reported, indicating that some genetic background may be involved in the development of the disease 14). In addition, epidemiological investigation has shown that the onset of HD is consistent with rapid growth in height. However, whether a deformity in the cervical spine, which was revealed in our study, is a reaction to rapid growth in height or is an independent risk factor for the onset of the disease remains inconclusive.
The end of progression of symptoms can be explained by the improvement in cervical instability through the prevention of forward displacement of the dural sac with cervical anterior flexion when growth stops 1). However, some patients eventually develop cervical spondylosis (in adulthood or older adulthood), and this suggests that the deformity of cervical spine becomes more clinically apparent with age.
In this study, by evaluation of its characteristics, we more quantitatively identified the alignment of the cervical spine in HD. However, the number of subjects evaluated in this study is limited, and they were at varying stages of the disease. Additionally, some subjects with HD had normal cervical spine alignment. So cervical
spine deformity in HD is not always seen. We propose that any of the five methods of measurement may be used for screening to promote early detection of HD. Although these measurements are not useful tools for diagnosis, our results suggest that patients with HD tend to cervical spine deformity. To obtain more useful information for elucidating the clinical condition, future large-scale studies are necessary to promote early diagnosis and guide selection of optimal treatments.
Conclusion
In HD, we found that a straight neck or kyphosis is characteristic of the alignment of the cervical spine. These factors may be associated with the pathophysiology of HD, and any of the five methods of measurement that we discussed may be used for screening. However, further investigation is needed before these measurements can be applied to screening protocols and treatment strategies.
References
1) Hirayama K: Juvenile muscular atrophy of distal upper extremity (Hirayama disease). Intern Med 39: 283 -290, 2000.
2) Chen CJ, Chen CM, Wu CL, Ro LS, Chen ST, Lee TH: Hirayama disease: MR diagnosis. Am J Neuroradiol 19: 365-368, 1998.
3) Baba Y, Nakajima M, Utsunomiya H, Tsuboi Y, Fujiki F, Kusuhara T, Yamada T: Magnetic resonance imaging of thoracic epidural venous dilation in Hirayama disease. Neurology 62: 1426-1428, 2004. 4) Hirayama K, Tokumaru Y: Cervical dural sac and
spinal cord in juvenile muscular atrophy of distal upper extremity. Neurology 54: 1922-1926, 2000. 5) Ohara A, Miyamoto K, Naganawa T, Matsumoto K,
Shimizu K. Reliabilities of and correlations among five standard methods of assessing the sagittal alignment of the cervical spine. Spine 31: 2585-2591, 2006. 6) Chen YL. Vertebral centroid measurement of lumbar
lordosis compared with the Cobb technique. Spine 24: 1786-1790, 1999.
7) Harrison DE, Harrison DD, Cailliet R, Troyanovich SJ, Janik TJ, Holland B. Cobb method or Harrison posterior tangent method: which to choose for lateral cervical radiographic analysis. Spine 25: 2072-2078, 2000.
— 34 —
Harrison DE, Holland B: Elliptical modeling of the sagittal lumbar lordosis and segmental rotation angles as a method to discriminate between normal and low back pain subjects. J Spinal Disord 11: 430-9, 1998. 9) Nunez-Pereira S, Hitzl W, Bullmann V, Meier O, Koller
H: Sagittal balance of the cervical spine: an analysis of occipitocervical and spinopelvic interdependence, with C-7 slope as a marker of cervical and spinopelvic alignment. J Neurosurg Spine 23: 16-23, 2015.
10) Ishihara A: Roentgenographic studies on the normal pattern of the cervical curvature. Nippon Seikeigeka Gakkai Zasshi 42: 1033-44, 1968 (in Japanese). 11) Tashiro K, Kikuchi S, Itoyama Y, Tokumaru Y,
Sobue G, Mukai E, Akiguchi I, Nakashima K, Kira J: Nationwide survey of juvenile muscular atropthy of distal upper extremity (Harayama disease) in Japan.
Amyotroph Lateral Scler 7: 38-45, 2006.
12) Chen CJ, Hsu HL, Tseng YC, Lyu RK, Chen CM, Huang YC, Wang LJ, See LC: Hirayama flexion myelopathy: neutral-position MR imaging findings − importance of loss of attachment. Radiology 231: 39 -44, 2004.
13) Xu X, Han H, Gao H, Hou C, Fan D, Fu Y, Sun Y: The increased range of cervical flexed motion detected by radiographs in Hirayama disease. Eur J Radiol 78: 82 -6, 2011.
14) Misra UK, Kalita J, Mishra VN, Kesari A, Mittal B: A clinical, magnetic resonance imaging, and survival motor neuron gene deletion study of Hirayama disease. Arch Neurol 62: 120-3, 2005.