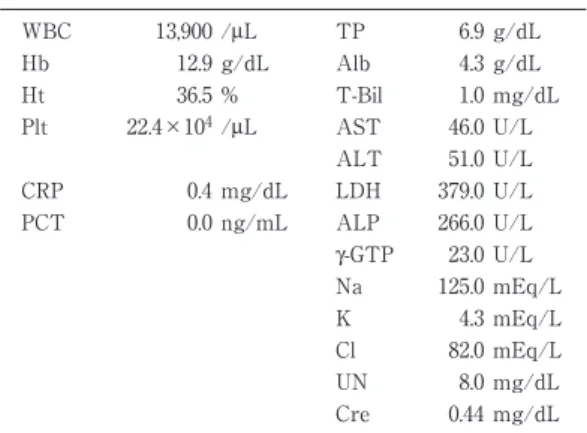
Table 1 Laboratory data on admission
WBC 13,900 /μL TP 6.9 g/dL
Hb 12.9 g/dL Alb 4.3 g/dL
Ht 36.5 % T-Bil 1.0 mg/dL
Plt 22.4×104/μL AST 46.0 U/L ALT 51.0 U/L
CRP 0.4 mg/dL LDH 379.0 U/L
PCT 0.0 ng/mL ALP 266.0 U/L
γ-GTP 23.0 U/L Na 125.0 mEq/L
K 4.3 mEq/L
Cl 82.0 mEq/L
UN 8.0 mg/dL
Cre 0.44 mg/dL
薬剤感受性検査と臨床経過に乖離を認めた Nocardia farcinica による 脳膿瘍の 1 例
1)
千葉大学医学部附属病院呼吸器内科,
2)東京労災病院呼吸器内科
島田(横江)絢子
1)2)高村 智恵
2)河野 正和
2)酒井 俊彦
2)戸島 洋一
2)(平成 27 年 6 月 29 日受付)
(平成 28 年 5 月 26 日受理)
Key words : Nocardia farcinica, brain abscess, sulfamethoxazole-trimethoprim resistance
序 文
ノカルジア感染症は,主として免疫不全者に起こる 日和見感染症として知られている.菌種により性質や 薬剤感受性が異なるため,菌種の同定と薬剤感受性試 験が治療方針の決定において重要である.今回薬剤感 受性試験では sulfamethoxazole-trimethoprim(ST 合 剤)に耐性を示したものの,臨床的に ST 合剤の治療 が効果的であった Nocardia farcinica による脳膿瘍の 1 例を経験したので報告する.
症 例
患者:74 歳女性.
既往歴:自己免疫性肝炎.中枢性尿崩症.
常用薬:プレドニゾロン 16mg/日
現病歴:入院 1 年前に自己免疫性肝炎と診断されプ レドニゾロン 30mg で治療開始し 10mg で肝炎の再燃 を認めたため,再度 30mg に増量し慎重に減量中だっ た.ニューモシスチス肺炎予防の ST 合剤内服はして いなかった.入院 1,2 カ月前より頭痛があり,尿崩 症による多尿として経過観察されていた.頭痛が悪化 したため救急要請し当院に救急搬送された.画像所見 と髄液所見から脳膿瘍,髄膜炎として入院加療とした.
入院時現症:体温 37.8℃,脈拍 76 回/分,血圧 171/
84mmHg,呼吸数 20 回/分,SpO
296%(室内気),意 識:清明,神経学的異常所見なし.他特記所見なし.
入院時検査所見:Table 1に示した.
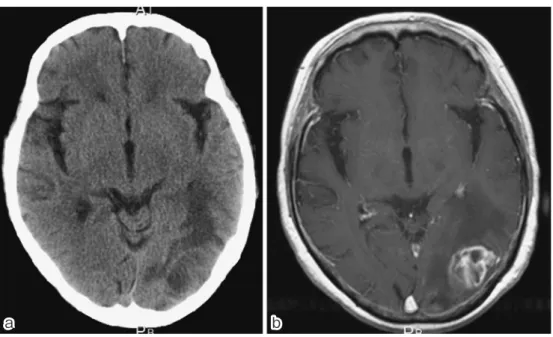
画像検査:胸部 X 線や CT 画像で肺野に異常影を 認めなかった.頭部 CT で左頭頂側頭葉に血管支配領
域と一致しない低吸収域を認めた.頭部造影 MRI で 不均一に造影される膿瘍と周囲に広範な浮腫を認め
(Fig. 1),側脳室内には穿破したと考えられる high density な膿瘍を認めた.
髄液検査:性状は乳白色で混濁しており,多核球優 位の細胞数増多を認めた(Table 2).
入院後経過(Fig. 2):画像所見と髄液所見から脳 膿 瘍 と 髄 膜 炎 の 診 断 で 入 院 と し,ceftriaxone(2g q12h),vancomycin(0.75g q8h),ampicillin(2g q4h)
で抗菌薬の投与を開始した.髄液培養で起炎菌が判明 せず,第 13 病日に膿瘍ドレナージを施行した.膿の グラム染色でグラム陽性の繊維状の桿菌を認め,Kiny- oun 染色陽性であったことから Nocardia による脳膿 瘍と診断し,同日より ST 合 剤(trimethoprim と し て 250mg q8h),amikacin(300mg q12h)の治療に 変更した.amikacin の髄腔内注射も 5mg q24h で 3 日間行った.菌種の同定と感受性検査を専門施設に依
症 例別刷請求先:(〒260―8675)千葉県千葉市中央区亥鼻1―8―1 千葉大学医学部附属病院呼吸器内科
島田 絢子
Fig. 1 (a) Computed tomography (CT) and (b) contrast-enhanced magnetic resonance im- aging (MRI) brain scans show a left tempoparietal lobe nodule with edematous lesions
a
a b b
Table 2 Examination of cerebrospinal fluid
appearance white and turbid
white blood cell count 1,779 /μL polymorphonuclears 1,492 /μL
mononuclears 287 /μL
protein 240 mg/dL
glucose 47 mg/dL
antigen testing for Streptococcus pneumoniae negative gram stain: negative
India ink preparation: negative acid-fast staining: negative cultures: negative
頼し,16SrRNA 遺伝子解析で Nocardia farcinica と同 定された.Clinical and Laboratory Standards Insti- tute(CLSI)の基準に従い実施された感受性試験(微 量液体希釈法)では,ST 合剤に高度の耐性(MIC 152/
8)がみられた(Table 3).当院で施行したディスク 法でも ST 合剤への阻止円形成を認めなかった.感受 性試験の結果の報告をうけて第 32 病日に ST 合剤を 中止し,imipenem-cilastatin と amikacin に変更した.
抗菌薬を変更した後から発熱と頭痛が再燃し,髄液検 査をしたところ細胞数増加がみられた.治療変更前は 比較的症状が落ち着いていたことから,ST 合剤と amikacin の治療に戻したところ,発熱と頭痛の明ら かな改善を認めた.1 カ月の併用療法で ST 合剤の単 剤治療に切り替えて退院とした.徐々に膿瘍の縮小を 認め経過良好である.
考 察
Nocardia は好気性のグラム陽性の分枝状の菌であ
る.Nocardia 属には 80 種類以上の菌種が存在するが,
そのうち人間に感染を起こすものは 33 種程度である.
日本の報告では N. farcinica (27%),N.aseteroides sensu stricto(24%),N.brasiliensis(22%),N.nova(11%),
N.cyriacigeorgica(10%)の順に多いとされる
1).放線 菌に似るが,Kinyoun 染色(特殊抗酸菌染色)で染 まることや,好気性菌であることで鑑別できる.通常 の細菌より培養期間が長く培養が難しい.感染経路と しては皮膚からと,経気道的に肺に感染を起こす経路 がある.これらが播種し菌血症,骨髄炎,脳膿瘍を起 こす場合もある
2).免疫不全者で Nocardia 脳膿瘍を発 症した場合,死亡率は約 30% と予後不良である.特
に N. farcinica は脳への親和性が高く脳膿瘍を形成し
やすいため,中枢神経病変の症状に乏しい場合でも脳 膿瘍の検索を行う必要がある
3).一般に Nocardia 感染 症 の 治 療 の 第 一 選 択 は ST 合 剤 で,重 症 の 場 合 は imipenem-cilastatin や amikacin との併用がすすめら れている.脳膿瘍があれば髄液移行の良い ceftriaxon の使用がすすめられるが N. farcinica の場合は ceftri- axon 耐性であり治療には使えない.ST 合剤が第一選 択肢になる理由として,過去の症例の集積があり,組 織移行性が良好で,内服薬のバイオアベイラビリティ も良好であることが挙げられる.
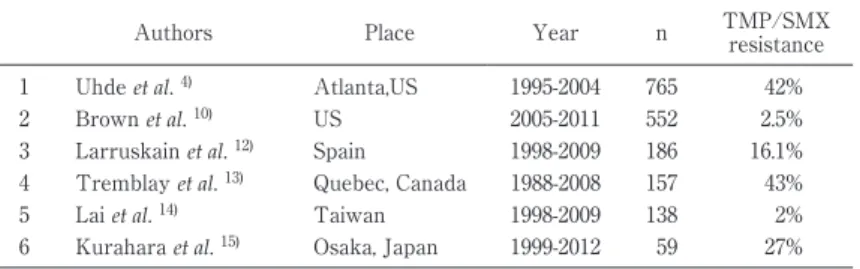
しかし最近 Nocardia の薬剤耐性,とくに ST 合剤へ の耐性が増加していると言われている
4).報告によっ て耐性率には 2〜47% と大きく差がある(Table 4).
その原因として耐性化の地域差や,地域でみられる菌
種の差以外に,感受性試験の方法や解釈が施設により
異なる可能性が指摘されている
5).CLSI ガイドライン
Fig. 2 Clinical course of the patient. After switching from TMP/SMX to IPM/CS, the patientʼs headaches and fever got worsened.
Table 3 Results of susceptibility testing; using the broth mi- crodilution method showing resistance to sulfamethoxazole trimethoprim.
Antibiotics MIC (μg/mL) for category
MIC result Susceptible Intermediate Resistant
AMK ≦8 - ≧16 2
AMPC/CVA ≦8 16/8 ≧32/16 8/4
CTRX ≧8 16-32 ≧64 ≧64
CPFX ≦1 2 ≧4 0.5
IPM ≦4 8 ≧16 2
LZD ≦8 - - 8
MINO ≦1 2-4 ≧8 2
ST ≦38/2 - ≧76/4 >152/8
TOB ≦4 8 ≧16 >16
CTX ≦8 16-32 ≧64 >64
CFPM ≦8 16 ≧32 >32
DOXY ≦1 2-4 ≧8 4
GM ≦4 8 ≧16 >16
ABPC >8
CAM ≦2 4 ≧8 >8
EM >2
Table 4 Resistance to sulfamethoxazole trimethoprim in
Nocardiaspecies in previous reports.
Authors Place Year n TMP/SMX
resistance 1 Uhde et al. 4) Atlanta,US 1995-2004 765 42%
2 Brown et al. 10) US 2005-2011 552 2.5%
3 Larruskain et al. 12) Spain 1998-2009 186 16.1%
4 Tremblay et al. 13) Quebec, Canada 1988-2008 157 43%
5 Lai et al. 14) Taiwan 1998-2009 138 2%
6 Kurahara et al. 15) Osaka, Japan 1999-2012 59 27%
では Nocardia の感受性試験方法としてミューラーヒ
ントン培地を使用した微量液体希釈法を推奨している
が,施行施設や判定者により結果にばらつきが出る可
能性が記載されている
6).Conville らによる Nocardia
の感受性試験結果の再現性に関する多施設共同研究で は,微量液体希釈法で各種 Nocardia の薬剤への Mini- mum inhibitory concentration(MIC)を測定し,そ の結果の一致率を施設間で比較しているが,N. far-
cinica における ST 合剤の感受性結果の再現性が不良
で,MIC(±1 の幅の誤差を含む)の一致率が 68.6%
であった
7).Nocardia はウェルの中で一塊となる性質 があることや,他の菌と異なる生育の特徴をもつこと が,判定が困難な要因ではないかとの記載がある.同 文献ではディスク法の再現性がよいことも報告してお り,微量液体希釈法に併用したほうがよいと述べられ ているが,本症例ではディスク法でも ST 合剤に耐性 の結果であった.
本邦での最近 10 年間の Nocardia による脳膿瘍の症 例報告は,医中誌で 26 例の報告がみられるが,その うち感受性試験の結果が記載されている症例は 9 例で あった.9 例のうち 2 例で ST 合剤に耐性であったが,
1 例は ST 合剤の治療で病勢が悪化し
8),1 例は感受性 結果を得て治療効果判定前に ST 合剤から他薬剤に治 療変更としていた
9).全 26 例のうち ST 合剤を使用し た 22 例の中で 15 例に効果がみられた.これらの結果 から,感受性検査の施行例が少ないこと,また ST 合 剤に対する耐性の結果が出た場合に治療が変更される 場合があると予想され,ST 合剤の効果を臨床的に評 価することが難しいことと考えられる.今回の症例と 同様に,感受性試験では ST 合剤耐性との結果で,臨 床的には効果がみられた症例の報告もあったが,探し 得た限りは 1 例のみであった
10).今回の症例において,
感受性結果が良好であった imipenem-cilastatin で治 療効果が不良だったことも一つ問題点として挙げられ る.通 常 N. farcinica で は imipenem-cilastatin 耐 性 は ほとんどなく,in vitro の多施設比較の薬剤感受性結 果にもばらつきは少なかったとされる
7).今回脳膿瘍 における治療効果不良の原因として,髄液への移行性 が一つの要因として考えられた.imipenem の髄液移 行率は 14%,trimethoprim が 42〜51%,sulfamethoxa- zole が 24〜30% の移行率だとする報告がある
11).
結 語
ステロイド投与下の免疫不全疫患者に Nocardia 脳 膿瘍を発症した症例を経験した.In vitro の感受性検 査では ST 合剤に高度耐性であったが,臨床的には ST 合剤で治療効果がみられた.感受性試験の結果と臨床 的効果は乖離する可能性があり,特に N. farcinica に おける ST 合剤の感受性結果の解釈には注意する必要 がある.現時点では ST 合剤耐性の Nocardia 感染に関 する報告が少なく,実臨床においても感受性試験を積 極的に行い,症例を集積する必要がある.
謝辞:菌の同定,感受性検査に関しまして御指導賜
りました千葉大学真菌医学研究センター 五ノ井透先 生,東邦大学医学部微生物・感染症学講座 石井良和 先生,青木弘太郎先生に深謝申し上げます.
本症例報告は 2014 年 12 月 13 日開催の内科学会関 東地方会にて報告いたしました.
利益相反自己申告:申告すべきものなし
文 献1
)Kageyama A, Yazawa K, Ishikawa J, Hotta K, Nishimura K, Mikami Y:Nocardial infections in Japan from 1992 to 2001, including the first re- port of infection by
Nocardiatransvalensis. Eur J Epidemiol 2004;19(4):383―9.
2
)Lerner PI:Nocardiosis. Clin Infect Dis 1996;
22:891―905.
3
)Mathisen GE, Johnson JP:Brain Abscess. Clin Infect Dis 1997;25:774.
4
)Uhde KB, Pathak S, McCullum I Jr, Jannat- Khah DP, Shadomy SV, Dykewicz CA,
etal.:Antimicrobial-Resistant
NocardiaIsolates, United States, 1995-2004. Clin Infect Dis 2010;51:
1445―8.
5
)Cassir N, Million M, Noudei R, Drancourt M, Brouqui P:Sulfonamide resistance in a dissemi- nated infection caused by
Nocardiawallacei : a case report. J Med Case Rep 2013;7:103.
6
)CLSI:Susceptibility testing of mycobacteria, nocardiae and other aerobic actinomycetes.
CLSI document M24-A. Clinical and Laboratory Standards Institute, Wayne, PA, 2003.
7
)Conveille PS, Brown Elliot BA, Wallace RJ Jr, Witebsky FG, Koziol D, Hall GS,
etal.:MultisiteReproducibility of the Broth Microdilution Method for Susceptibility Testing of
NocardiaSpecies. J Clin Microbiol. 2012;50:1270―80.
8
)高木公暁,山田佳輝,増栄成泰,宇野雅博,藤
木佳則,米田尚生,他:後腹膜膿瘍を契機に発 見された播種性ノカルジア症の 1 例.泌尿器科 紀要 2010;56:691―5.
9
)清水 馨,重田雅代,菅井亮平,吉川眞由美,岡
部英俊,茂籠邦彦,他:脳膿瘍を来した ST 合剤
耐性
Nocardia farcinica感染症の一症例.医学検
査 2010;59:722―6.
10
)Brown Elliott BA, Biehle J, Conveille PS, Cohen S, Saubolle M, Sussland D,
etal.:Sulfonamideresistance in isolates of
Nocardiaspp. from a US multicenter survey. J Clin Microbiol 2012;50:
670.
11
)Roland N, Fritz S, Helmut E:Penetration of Drugs through the Blood-Cerebrospinal Fluid/
Blood-Brain Barrier for Treatment of Central Nervous System Infections. Clin Microbiol Rev 2010;23:858―83.
12
)Larruskain J, Idigoras P, Marimón JM, Pérez- Trallero E:Susceptibility of 186
Nocardiasp.
isolates to 20 antimicrobial agents. Antimicrob
Agents Chemother 2011;55:2995―8.
13
)Tremblay J, Thibert L, Alarie I, Valiquette L, Pépin J:Nocardiosis in Quebec, Canada, 1988- 2008. Clin Microbiol Infect 2011;17:690―6.
14
)Lai CC, Liu WL, Ko WC, Chen YH, Tang HJ, Huang YT,
etal.:Antimicrobial-resistant nocar-dia isolates, Taiwan, 1998-2009. Clin Infect Dis
2011;52:833.
15
)Kurahara Y, Tachibana K, Tsuyuguchi K, Akira M, Suzuki K, Hayashi S:Pulmonary nocardio- sis : a clinical analysis of 59 cases. Respir Inves- tig 2014;52:160―6.
A Case of Brain Abscess Caused by Nocardia farcinica in which the Test Results for Drug Susceptibility Conflicted with the Actual Clinical Course
Ayako SHIMADA (YOKOE)
1)2), Chie KOUMURA
2), Masakazu KOUNO
2), Toshihiko SAKAI
2)& Hirokazu TOJIMA
2)1)
Department of Respiratory Medicine, Chiba University Hospital,
2)