■ 原 著
日血外会誌 2012;21:663–668
はじめに 上行弓部から下行大動脈にわたり広範囲に進展した胸部大動 脈瘤の治療は,ステントグラフト(TEVAR)の導入により,より ハイリスク症例への適応が可能となった1).一方,病態や解剖 学的制約のため,こうした低侵襲治療の恩恵を享受できない症 例も多く存在する.今回われわれは,解離による腹部大動脈分 枝の偽腔起始や大動脈の形態と性状がステントグラフトのシー リングに不適切などの理由から TEVAR の適応が困難と判断さ れた症例に対して,正中切開下に long elephant trunk(LET)を pull-through2, 3)させて下行大動脈全長を置換し,良好な結果を得 たので若干の文献的考察を加えて報告する. 手 術(Fig. 1) 麻酔導入後,X 線透視下に大腿動脈(解離症例では真腔)から カテーテルを上行大動脈まで挿入し,留置する.胸骨正中切 開を行い,送血路は右腋窩動脈と上行大動脈または大腿動脈 を選択し,脱血は上下大静脈から行う.人工心肺を確立し, 大動脈を遮断,心停止を得る.脳分離体外循環,中等度低体 温循環停止下に弓部大動脈または弓部の人工血管を切開し, 予め留置しておいたカテーテルを引き出し,LET の先端を把 持しておく.下行大動脈または腹腔動脈上の大動脈への直接 アプローチが必要な場合は,胸部正中切開創から脱転した心 臓の後面で心囊を切開するか,上腹部へ皮膚切開を延長し, 小網を切開して到達した.カテーテルで把持した LET を,解 離症例では真腔内を通し,末梢側の下行大動脈の切開部から 引き出し,中枢・末梢側ともに inclusion 法で吻合する.Inclu-sion法は,フェルト付き 4-0 ポリプロピレン糸を用い大動脈切 開の両端と後壁中央の計 3 カ所で,大動脈後壁と LET をマッ トレス縫合で固定したうえで連続縫合する.前壁は帯状フェ ルト補強下に縫合する.解離症例で偽腔血流を維持する必要 がある場合は,末梢吻合部以下の解離した内膜を可及的に切 除する.LET 留置のみで大動脈瘤の血栓化が期待できる症例 や全身状態が不良な緊急症例では,末梢側の外科的固定は行 わず,留置のみの場合もある.血栓化が得られない時は,二 期的に追加手術を考慮する. 山形大学医学部第二外科(循環器・呼吸器・小児外科学) (Tel: 023-628-5342) 〒 990-2331 山形県山形市飯田西 2-2-2 受付:2011 年 9 月 7 日 受理:2012 年 1 月 5 日 第 39 回日本血管外科学会学術総会(2011 年,沖縄)座長推薦演題広範囲胸部大動脈瘤ハイリスク症例に対する
long elephant trunk を用いた pull-through 法
内田 徹郎 金 哲樹 前川 慶之 大塲 栄一 林 潤 吉村 幸浩 貞弘 光章
要 旨:【目的および方法】当科では胸部大動脈瘤のステントグラフト治療(以下 TEVAR)が困難な広範囲胸部
大動脈瘤に対して,正中切開で下行瘤内に long elephant trunk(以下 LET)を pull-through(以下 PT)させて全下行 置換を行ってきた.本術式の成績,妥当性および問題点について検討した.【結果】症例は 4 例,うち 2 例が破 裂に対する緊急手術,年齢は平均 72 歳であった.A 型解離術後の下行の残存解離腔拡大が 2 例,B 型解離発症 後の下行大動脈拡大が 1 例および弓部から下行へ進展した真性瘤が 1 例であった.本法の適応理由は,左開胸 困難,腹部大動脈分枝の偽腔起始,下行大動脈の高度蛇行および著しく太い下行大動脈であり,TEVAR は困難 と判断した.LET の遠位端は,腹腔動脈直上の大動脈が 1 例,下行大動脈が 3 例であった.固定様式は,解離 内膜の切除と inclusion 法による吻合が 2 例,吻合せず留置のみが 2 例であった.術後に全例で瘤内および解離 腔の血栓化を認め,対麻痺は認めなかった.1 例が消化管出血で死亡したが,他の 3 例は経過良好であった. 手術手技の工夫として,大動脈瘤の蛇行が著しい場合は,人工血管にスティッチを加え過伸展を予防した.中 枢側と末梢側大動脈の口径差が大きい場合は異なるサイズの人工血管を composite graft として PT した.【結論】 広範囲胸部瘤に対する LET による PT 法は,TEVAR が困難なハイリスク症例の手術侵襲の軽減に有効であると 考える.(日血外会誌 2012;21:663–668) 索引用語:Pull-through 法,ロングエレファントトランク,広範囲胸部大動脈瘤
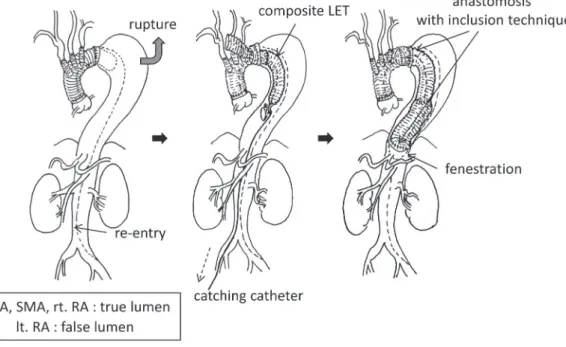
Fig. 1 Schematic drawing of case 1.
Pull-through technique via median sternotomy and laparotomy. Proximal anastomosis was performed with inclu-sion technique. Intimal flap was resected as possible and the distal end of LET was fixed at the abdominal aorta just proximal to the celiac artery.
LET, long elephant trunk; CA, celiac artery; SMA, superior mesenteric artery; RA, renal artery
Fig. 2 Modification of LET for pull-through technique. Composite LET consisted of two different sizes of graft was made prior to operation. Longitudinal
stitch was placed onto the lesser curvature of the graft. A: Composite LET. B: Reversed composite LET. LET, long elephant trunk
症例および結果 胸骨正中切開アプローチで LET を下行大動脈瘤内に pull-throughさせて治療を行った症例は 4 例であった. 症例 1(Fig. 1):77 歳,女性.A 型大動脈解離に対する上行 弓部置換術後に下行大動脈の解離腔が拡大したため,左開胸に よる手術を試みた.しかし高度の肺癒着のため,剝離に伴う肺 出血による播種性血管内凝固症候群を来し手術を断念した.10 年後に瘤破裂による喀血を認め,緊急手術を行った.下行置換 が必要だが,左開胸アプローチは不可能なため再胸骨正中切開 と上腹部切開下に,pull-through 法による手術を計画した.中 枢側は弓部の人工血管に inclusion 法で吻合し,末梢側は腹部切 開から小網を経由して,腹腔動脈直上の腹部大動脈の解離内膜 を 切 除 し た う え で,inclusion 法 で 吻 合 し た.LET を pull-throughさせる際,中枢と末梢で吻合部の口径差が大きいた め,24 mm と 30 mm の太さの異なる 2 本の人工血管を吻合 し,composite LET を作製した(Fig. 2A).
665 2012年 8 月 内田ほか:広範囲胸部瘤に対する pull-through 法 術後に下行の残存解離腔拡大を認めた.下行大動脈は高度に蛇 行,屈曲し,右胸腔を走行していた.手術は,下大静脈の右側 で心囊を切開し,下行大動脈内を pull-through させた LET の遠 位端で解離内膜を可及的に切除して,inclusion 法で吻合した. 症例 3(Fig. 4):65 歳,女性.最大径 10 cm の遠位弓部大動脈 瘤に対する上行弓部および下行置換術を施行した.高度の肺気 腫を認めたため,左開胸の手術を回避し,正中切開で手術を 行った.弓部と下行大動脈の口径差が大きいため,30 mm と 22 mmの 2 本の人工血管で作製した composite LET を pull-through させた(Fig. 2B).LET の遠位端の外科的な固定は行わなかった. 症例 4(Fig. 5):62 歳,男性.B 型慢性解離の経過観察中に解 離性大動脈瘤破裂を来した.前医で挿入された両側の胸腔ド
Fig. 3 Schematic drawing of case 2.
The LET was pulled down the descending aorta. Both proximal and distal end of the LET were anastomosed with inclusion technique. Distal anastomosis was performed through the posterior pericardium with fenestration.
LET, long elephant trunk; CA, celiac artery; SMA, superior mesenteric artery; RA, renal artery
Fig. 4 Schematic drawing of case 3.
Complete aneurysmal thrombosis around the LET was achieved without distal anastomosis of the LET.
レーンから大量の出血を認めた.血圧が測定不能な高度の ショック状態であり,まず正中切開で長さ 15 cm の LET を用い た上行弓部置換を行い,血栓化による破裂部位のコントロール が得られなかった場合は二期的に下行大動脈への手術を考慮す る方針とした.手術翌日の CT で,破裂した偽腔は完全に血栓 化していた. LET を用いた pull-through 法の適応理由は,腹部大動脈分枝 の偽腔起始,下行大動脈の高度蛇行および屈曲,著しく大きな 下行大動脈径であり,TEVAR は困難と考えられた.症例 3 は,LET を使用せずとも段階的手術として TEVAR の適応が可 能であったと考える.LET の遠位端の位置は,腹腔動脈直上の 腹部大動脈が 1 例,下行大動脈が 3 例であった.遠位端の固定 様式は,解離内膜の末梢方向への切除を加えた inclusion 法によ る吻合が 2 例,吻合せず留置のみが 2 例であった.術後に全例 で瘤内および解離腔の血栓化を認め,対麻痺は認めなかった.1 例(症例 1)が 2 カ月後に突然の消化管出血で死亡したが,他の 3 例は経過良好であった. 考 察 広範囲胸部大動脈瘤の治療は,一期的もしくは段階的手術が 考慮される.一期的手術は手術侵襲が大きく,重篤な術後合併 症が危惧される4).一方,段階的手術は複数回の手術リスクお よび待機中の破裂の可能性がある5, 6).最近の TEVAR の発達に 伴い,初回手術は ET を用いた上行弓部置換術を胸骨正中切開 で行い,第二期手術は下行大動脈へ TEVAR を施行する低侵襲 な治療体系が確立してきた1). 腹部大動脈の分枝が偽腔から起始する解離症例や末梢側の大 動脈がステントグラフトのシーリングに不適切な場合,TEVAR は困難である.左開胸下の手術が考慮されるが,可及的に開胸 操作を回避したいハイリスク症例では異なった治療計画が必要 である.今回われわれは,正中切開アプローチのみで,LET を pull-throughさせて全下行大動脈置換術を施行した. Pull-through 法の概念は新しいものではなく,問題点として, 対麻痺,瘤内でのグラフト屈曲による灌流不全および瘤内の血 流残存による不十分な exclusion 効果が指摘されている. LET を用いた弓部置換術は 2000 年に Kuki らが報告してい る7).最近の報告8, 9)では,グラフト周囲の血栓化が約 80%の症 例で認められるため,現在は LET の遠位端の吻合は行わない方 針としている.われわれも,LET と大動脈の口径差がなく血栓 化が期待できる場合や緊急手術では末梢側の外科的固定は行わ ず,留置のみとすることを考慮する.一方,解離症例で大動脈 の主要分枝が偽腔起始の場合は,末梢側吻合部における解離内 膜切除が必要である. LET を用いた pull-through 法の導入にあたり,いくつかの手 術手技の工夫を加えた.Pull-through 時には人工血管の折れやね じれによる閉塞が危惧される.対策として,X 線透視下にカ
Fig. 5 Schematic drawing of case 4.
Graft replacement of total arch and entire descending aorta was performed via median sternotomy. The LET pulled through the true lumen was placed without dis-tal anastomosis. Bleeding was stopped and false lumen was thrombosed completely. LET, long elephant trunk; CA, celiac artery; SMA, superior mesenteric artery; RA, renal artery
667 2012年 8 月 内田ほか:広範囲胸部瘤に対する pull-through 法 テーテルを大腿動脈から上行大動脈に進め,人工血管を把持 し,金属クリップによるマーキングをガイドに瘤内を誘導,留 置した.大動脈の蛇行が高度な場合は,小弯側の屈曲に合わせ て 2-0 糸によるスティッチを人工血管の長軸方向に加えること で自然なカーブをつけた.また LET を適用する中枢と末梢の大 動脈径が大きく異なる場合があり,今回の 2 症例でも 10 mm 以 上の口径差があった.これに対して,2 種類の異なるサイズの 人工血管を予め吻合して composite graft とした.Composite LET と人工血管の小弯のスティッチにより,大動脈壁との密着によ る肋間動脈のカバーひいては速やかな瘤内の血栓化が得られる と考える.上記の工夫を行わなかった 2 症例でも血栓化を認め たが,LET と大動脈壁との口径差が小さく,長い範囲での密着 が可能であったためと考えられる. 今回の検討症例では幸いにも術後に対麻痺を認めなかった が,本術式における対麻痺発生の可能性の問題は依然として解 決されていない.しかし,広範囲胸部瘤の治療体系における LETによる pull-through 法は,TEVAR が困難なハイリスク症例 の手術侵襲の軽減に有効な選択肢のひとつであると考える. 結 語 TEVAR が困難な広範囲胸部大動脈瘤を有するハイリスク症 例に対して,正中切開アプローチによる pull-through 法を応用し て手術を施行し,良好な結果を得た.術後の対麻痺を認めず, 全例において LET 周囲の血栓化が得られた.対麻痺予防の問題 は未解決だが,広範囲胸部瘤に対する LET による pull-through 法は,ハイリスク症例に有用であると考える. 本論文の要旨は,第 39 回日本血管外科学会学術総会(2011 年 4 月,沖 縄)で発表した. 文 献
1) Greenberg RK, Haddad F, Svensson L, et al. Hybrid approaches to thoracic aortic aneurysms: the role of endovascular elephant trunk completion. Circulation 2005;112:2619-2626.
2) 岩田圭司,島崎靖久,阪本朋彦.広範囲胸部大動脈瘤に対する 大動脈内 pull-through 法による一期的弓部・下行置換術.胸部 外科 2009;62: 369-372.
3) Koizumi K, Ueda T, Shimizu H, et al. Pull-through technique for entire thoracic aortic dissection without additional left thoracotomy. Interact Cardiovasc Thorac Surg 2011;12: 339-340.
4) Kouchoukos NT, Mauney MC, Masetti P, et al. Optimization of aor-tic arch replacement with a one-stage approach. Ann Thorac Surg 2007;83:S811-S814; discussion S824-S831.
5) Borst HG, Frank G, Schaps D. Treatment of extensive aortic aneu-rysms by a new multiple-stage approach. J Thorac Cardiovasc Surg 1988;95:11-13.
6) Safi HJ, Miller CC, Estrera AL, et al. Optimization of aortic arch replacement: two-stage approach. Ann Thorac Surg 2007;83:S815- S818; discussion S824-S831.
7) Kuki S, Taniguchi K, Masai T, et al. A novel modification of elephant trunk technique using a single four-branched arch graft for extensive thoracic aortic aneurysm. Eur J Cardiothorac Surg 2000;18:246-248. 8) Toda K, Taniguchi K, Masai T, et al. Arch aneurysm repair with long
elephant trunk: a 10-year experience in 111 patients. Ann Thorac Surg 2009;88:16-22.
9) Hata H, Toda K, Shudo Y, et al. Repair for acute type A aortic dissec-tion with a long elephant trunk technique. J Thorac Cardiovasc Surg 2009;137:777-778.
The Pull-through Technique Using the Long Elephant Trunk for Extensive Thoracic
Aortic Aneurysm
Tetsuro Uchida, Cholsu Kim, Yoshiyuki Maekawa, Eiichi Oba, Jun Hayashi, Yukihiro Yoshimura
and Mitsuaki Sadahiro
Second Department of Surgery, Yamagata University Faculty of Medicine
Key words: Pull-through technique, Extensive thoracic aortic aneurysm, Long elephant trunk
Objectives and methods: We performed graft replacement of the entire descending thoracic aorta using the pull-through technique in patients with high mortality and morbidity who were unsuitable for endovascular repair. The purpose of this study was to determine the surgical outcomes, feasibility and problems concerning this method. Results: A total of 4 patients (1 man and 3 women, mean age, 72 years) with extensive thoracic aortic aneurysm underwent surgical repair using the long elephant trunk (LET) via a median sternotomy, but without an additional left thoracotomy. Two patients who had previously undergone total arch replacement for aortic dissection showed enlargement of the false lumen of the entire downstream descending aorta. One patient presented with rupture of a dissecting aneurysm of the descending aorta and another had an extensive atherosclerotic thoracic aortic aneurysm. The current technique was employed because of the difficulty in performing a left thoracotomy, due to abdominal vessels arising from the false lumen but without significant fenestration, and an unfavorable anchoring site of the endovascular stent graft. The distal end of the LET was fixed at the abdominal aorta just proximal to the celiac artery in 1 patient and the descending aorta in 3 patients. Distal anastomosis was performed in 2 patients in a double-barrel fashion. Subsequent distal anastomosis was not required in the other 2 patients. Complete aneurysmal thrombosis around the LET was achieved in all patients and no further procedures were required. Although the intercostal artery was not reconstructed in any case, paraplegia was not observed. The postoperative courses were uneventful except for 1 patient who died of gastrointestinal bleeding. In 1 case with a highly elongated aorta, we sutured the lesser curvature of the LET in order to fix its length and prevent over-stretching when the LET was pulled to the downstream aorta. However, if the size discrepancy between the proximal and distal aorta was too large, a composite LET which consisted of 2 different sizes of graft was pulled through the descending aorta. Conclusion: We recommend the pull-through technique as a less invasive alternative to a conventional left thoracotomy and endovascular aortic repair in selected high-risk patients.