連絡先:篠田 淳,〒505−0034 美濃加茂市古井町下古井 630 木沢記念病院・中部療護センター
Address reprint requests to:Jun Shinoda, M.D., Ph.D., F.R.C.S.Ed., Chubu Medical Center for Prolonged Traumatic Brain Dysfunc-tion, Kizawa Memorial Hospital, 630 Shimo−kobi, Kobi−cho, Minokamo−shi, Gifu 505−0034, Japan
高次脳機能障害を引き起こす外傷性脳損傷の画像評価
―特にびまん性脳損傷慢性期の画像について―
篠田 淳
1)2),浅野 好孝
1)2)1)木沢記念病院・中部療護センター,2)岐阜大学連携大学院医学系研究科神経統御学講座脳病態解析学分野
Neuroimaging of Patients with Impairments of Executive Brain
Func-tion Due to Traumatic Brain Injury
Jun Shinoda, M.D., Ph.D., F.R.C.S.Ed.1)2), and Yoshitaka Asano, M.D., D.M.Sc.1)2)
1)Chubu Medical Center for Prolonged Traumatic Brain Dysfunction, Kizawa Memorial Hospital, 2)Department of Clinical Brain Sci-ences, Gifu University Graduate School of Medicine
After suffering traumatic brain injury(TBI), there may be a substantial number of disabled people whose impairment is not recognized socially because their disabilities are limited to cognitive, emotional and behavioral domains, with no obvious physical deficits. The Japanese Government has provided medico−social services for such patients diagnosed with impairments of executive brain function(IEBF), since 2006. One of the administra-tive criteria for diagnosis of IEBF to receive medico−social services is the confirmation of organic injured lesions in the brain by neuroimaging modalities. Consequently, some people with chronic stage TBI have been excluded from receiving services because no lesions were apparent on conventional CT or MRI. Recent development of SPECT, PET and new MRI neuroimaging modalities make it possible to detect regions of metabolic dysfunction where organic injured lesions may be absent or have not been detected on conventional CT or MRI.
One of the most crucial diagnostic findings of diffuse TBI in the chronic stage on conventional CT or MRI is diffuse brain atrophy. T2* weighted imaging(WI)and susceptibility WI(SWI)are extremely sensitive methods
to detect hemosiderin−lading lesions even in the chronic stage. Another method, diffusion tensor imaging(DTI), permits the evaluation of white matter structural integrity in the brain. One index used in DTI is the fractional anisotropy(FA)value. A region of interest(ROI)study of FA values in patients with diffuse TBI revealed signifi-cant decreases in the corpus callosum, coronal radiation, centrum semiovale, cingulated gyrus. Tractogram derived by fiber tracking on FA map is an innovative neuroimaging technique, which reveals axonal deficits visually. Another innovative neuroimaging tool derived from DTI is the FA−SPM image. This permits the detec-tion of lesions with significantly decreased FA values objectively and over the whole brain. Alternatively, FDG− PET and ECD−SPECT are functional neuroimaging modalities which can uncover the regions with metabolic dys-function in the brain. In patients with diffuse TBI, metabolic dysdys-function is characteristically shown in the medial part of the prefrontal region and the base of the bilateral frontal lobes, the bilateral cingulated gyri, and the bilat-eral thalami, in the chronic stage.
The findings suggesting the existence of minute lesions due to TBI on these new neuroimaging modalities may be useful evidence for diagnosing IEBF administratively, and also serve as a tool for elucidating the mecha-nisms of IEBF after TBI.
(Received May 15, 2013;accepted May 17, 2013)
Key words:traumatic brain injury, executive brain function, MRI, diffusion tensor imaging, tractography, frac-tional anisotropy, FDG−PET, ECD−SPECT
Jpn J Neurosurg(Tokyo)22:842−848, 2013
はじめに
救急医療の進歩により多くの交通事故による重傷頭部 外傷患者の救命が可能となった.一方,急性期の危機を 乗り切ったこれらの人たちの中には障害を後遺し生活制 限を余儀なくされている人たちも多い.従来,意識の障 害,身体の障害など一見してその存在が理解される障害 は社会的に注目されてきたが,記憶・記銘力障害,注意 障害,遂行機能障害,社会的行動障害などの「見えない 障害」を後遺し社会に適応できない人たちの存在は十分 理解されてこなかった.日本政府は 2006 年から彼らに 「高次脳機能障害」という傷病名をつけ,障害者として行 政支援の対象とすることにより,自立と社会参加へ向け 包括的な取り組みを開始した10). 2001 年度から始まった高次脳機能障害支援モデル事 業で定められた高次脳機能障害診断基準では,本障害の 診断に際し上記臨床症状が存在することのほか,com-puted tomography(CT),magnetic resonance image(MRI) 等で脳の器質的疾患が確認されることが必要とされ る6)7).脳挫傷や重度のびまん性脳外傷は慢性期において も従来の CT,MRI で脳の器質的異常を比較的容易に捉 えることができる.また,慢性期の画像で脳に器質的損 傷が確認できなくても急性期の画像で外傷性くも膜下出 血,脳室内出血,白質内の微小出血等がみられれば診断 は可能である.急性期の画像に異常がない場合でも受傷 直後の意識障害(6 時間以上の昏睡)があれば診断基準 を満たすと解釈される.しかし,臨床症状が存在しても 急性期の画像で異常が認められず,かつ受傷時意識障害 も軽度であった症例は診断に苦慮する.近年,MRI の新しい撮像法の開発,single photon emis-sion computed tomography(SPECT)や positron emisemis-sion tomography(PET)による脳代謝検査の普及はめざまし く,従来の画像では確認できなかった脳の器質的損傷を 捉える画像を作成することが可能となった.これらの画 像の進歩は従来「見えない障害」と呼ばれてきた高次脳 機能障害を「見える障害」へ移行させつつある.以下, 当施設で使用する最新の神経画像を中心に,外傷性脳損 傷,特にびまん性脳損傷慢性期の画像診断と画像所見か ら推測できる高次脳機能障害のメカニズムについて述べ る.
MRI
□1 Structural MRI 国内に広く普及している MRI 装置で撮像可能な T1強調画像(T1WI),T2 強調画像(T2WI),fluid attenuated inversion recovery(FLAIR)等でも外傷による脳の器質的 変化は十分観察できる.びまん性脳損傷慢性期で最もよ くみられる所見はびまん性脳萎縮である.脳溝の拡大, 脳室の拡大でその存在が確認できる(Fig. 1).一般に外 傷の重症度に従い脳の萎縮も著しいとされる.また,び まん性脳損傷で損傷を受けやすい脳梁,脳弓,脳幹の萎 縮も本症慢性期の特徴である.脳萎縮の状態は年齢,既 往症に影響を受けやすく,さらには同年齢でもしばしば 個人差があることから,受傷急性期に撮られた画像と比 較して評価を下すことが肝要である. 受傷急性期にみられた少量の頭蓋内出血を慢性期に画 像で確認することは困難である.T2*強調画像(T2*WI)
や susceptibility weighted image(SWI)は慢性期に残存 する微小出血後のヘモジデリンを鋭敏に捉えることがで きる(Fig. 2)9)16).びまん性脳損傷では脳梁,大脳基底
核部,大脳半球深部白質でヘモジデリンを捉えやすい.
□2
Diffusion tensor image(DTI)
DTI により神経線維の周囲に存在する水の異方性の 強さを表す fractional anisotropy(FA)を画像化した FA map を作成し,関心領域の FA 値を計測することにより FA 値の低下している部位を器質的な神経軸索損傷部位 として評価可能となった.びまん性脳損傷では脳梁,脳 弓,放線冠,半卵円中心,帯状回などで有意な FA 値の 低下をみる11).また,皮質脊髄路における FA 値の低下は 磁気刺激による運動誘発電位の出現しにくさと相関して おり,FA 値は脳の形態的変化の評価のみならず機能的
Fig. 1 Fluid attenuated inversion recovery
image of a 23−year−old man with
chronic diffuse and focal brain injury
Severe and diffuse atrophy can be seen in the brain stem and bilateral cerebral hemisphere with contusional brain damages in the left frontal and temporal lobes.
変化の評価にも使用できる可能性が示唆されている17).
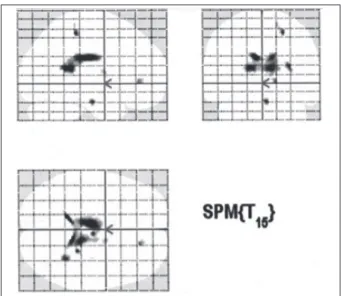
FA map から線維追跡によって得られる tractogram は 関心領域を通過する神経軸索の三次元的観察を可能に し,損傷部位を解剖学的に捉えやすい.脳梁,帯状束, 上縦束,皮質脊髄路,視放線を通過する線維は手技的に 描出しやすく,健常者または患者の健常側の tractogram と比較し線維が疎である領域では,軸索損傷により線維 追跡が途切れたものと判断される(Fig. 3). しかし,このような関心領域を標的とした解析は関心 領域の設定や FA 値のしきい値の設定に恣意が入るこ と,関心領域以外の部位を評価できないことといった弱 点がある.これを補う目的で全脳を対象として statisti-cal parametric mapping(SPM,統計学的画像解析)によ る有意な FA 値低下領域(健常者と比較し)の評価が行わ れる.健常者群と患者群の比較による群間解析では患者 群では脳梁,脳弓において有意に FA 値が低下している ことが明らかとなった.これらの部位はびまん性脳損傷 で最も器質的損傷を受けやすい部位と考えられる.最近 では群間解析のみならず個別解析(FA−SPM image)も可 能となった(Fig. 4).軽度∼中等度の外傷性脳損傷患者 を対象とした場合,T2*WI で異常信号を捉えることがで きなかった症例においても FA−SPM image で有意に FA 値が低下する部位を確認できる1).FA−SPM image は 通常の MRI では確認できないきわめて微細な脳損傷を も捉えることができる優れた画像といえる. DTI における軸索損傷のもう 1 つの指標として,神経 線維の周囲に存在する水の拡散の程度を表す mean dif-fusivity(MD)も用いられる.一部の軸索に損傷が起こっ ても,軸索束はいまだ存在しており水の異方性が保たれ ている状態(FA 値に変化がない状態)でも損傷された軸 索周囲の水の拡散が大きい状態であれば MD 値は増加 する.一般に外傷性脳損傷では FA 値は重度損傷を,MD 値は軽度損傷を捉える際に鋭敏であるとされる2).また, 軽度外傷性脳損傷では MD 値は FA 値に比べ脳震盪症候 群を呈する患者で異常値が出やすい傾向にある8).
Fig. 3 Tractography of the corpus callosum The number of fibers is decreased in the posterior part of the body of the corpus callosum in patients with chronic diffuse brain injury (B) compared to the normal control(A).
A B
Fig. 4 FA−SPM image of a 29−year−old woman
with chronic diffuse brain injury
Regions with significantly decreased FA value compared to that of the normal control can be seen in the corpus callosum as black shadows in the glass brain.
Fig. 2 T2* weighted image of a 29−year−old
man with chronic diffuse brain injury
Several abnormal low intensity lesions which mean precipitation of hemosiderin can be seen in the bilateral basal ganglia and corpus callosum.
□3 Functional MRI(fMRI) 薬剤を使用しない脳機能画像としてさまざまな作業課 題による fMRI が行われている.一般に,びまん性脳外 傷の軽症例では容易な作業課題に対しては健常者と同様 に大脳皮質の比較的広い領域で活動性が高まるが,作業 課題が難しくなるほど健常者と異なり大脳皮質の活動部 位が狭くなり散逸する.この傾向は中等症例,重症例で 顕著となる.また,高次脳機能障害患者では健常者に比 べ,注意力を惹起する stroop test で前部帯状回近傍の賦 活低下がみられる14). □4 MR spectroscopy(MRS) 急性期では,びまん性脳損傷軽症例でも健常者に比べ 大脳半球深部白質,脳梁膨大部で cho/creatine 比の増加, N−acetyl aspartate 値の低下,lactate/creatine 比の増加が みられることが報告されている3).慢性期では軽症例で
これらの異常所見を捉えることは難しいが,中等症∼重 症例では臨床症状の重症度に相関して全脳で N−acetyl aspartate 値の低下,lactate の出現,白質で creatine,myoi-nositol の上昇,choline/creatine 比の上昇がみられる5).
Fig. 5 FDG−PET of a patient with chronic diffuse brain injury Regions with significantly decreased glucose metabolism compared to that of the normal control can be seen bilaterally in the corpus callosum (a), medial prefrontal region(b), fronto−basal region(c), and thalamus (d)
as red colored areas in the brain.
a b
c d
Fig. 6 ECD−SPECT of patients with chronic diffuse brain injury
In the group of patients with MRI abnormalities, regions with significantly decreased cerebral blood flow compared to that of the group without MRI abnormalities can be seen bilaterally in the anterior cingulated, medial prefrontal region, thalamus as black shadows in the brain(A). In the group of patients without MRI abnormalities, however, regions with significantly decreased cerebral blood flow compared to that of the group with MRI abnormalities can be seen bilaterally in the parito−occipital convexity as black shadows in the brain(B).
18
F
−
fluorodeoxyglucose
(
FDG
)−
PET
SPM 統計学的画像解析を用いることにより,慢性期び まん性脳損傷群の脳代謝機能が健常者に比べ有意に低下 している領域が FDG−PET 画像上で視覚的に捉えやす くなった.群間解析では健常者群と比較し,慢性期びま ん性脳損傷群では両側性に帯状回,前頭前野内側,前頭 葉底面,視床で有意な脳代謝機能の低下が観察される. これらの領域は高次脳機能障害例,最小意識状態例,植 物状態例で共通して脳代謝機能が低下しており認知機能 障害,意識障害が重度になるに従いその機能低下範囲が 広がる(Fig. 5)12). 個々の患者の脳糖代謝機能を評価する場合は,同じく 統計画像解析である easy Z score imaging system(eZIS) 解析がわが国では臨床の場で広く用いられる.このよう な個別解析でも,びまん性脳損傷例では両側前頭前野内 側部から底部,両側帯状回で代謝機能の低下が頻繁に観 察され,この機能低下パターンがびまん性脳損傷例の特 徴所見と考えられる.Posttraumatic stress disorder(PTSD)や外傷後抑うつ 状態等の機能的病態でもしばしばこれらの部位の血流低 下は観察されるが,これらの機能的病態では帯状回,前 頭前野内側,前頭葉底面,視床に血流低下域が限局する よりむしろ脳の器質的損傷例に比べ両側大脳半球円蓋部 に比較的広範に軽度の血流低下域が散在することが特徴 である.
99m
Tc
−
ethyl
−
cysteinate dimer
(
ECD
)−
SPECT
器質的脳損傷を有するびまん性脳損傷後高次脳機能障 害患者は,ECD−SPECT 統計画像解析でも FDG−PET で 脳糖代謝機能低下部位として観察される帯状回,前頭前 野内側,前頭葉底面,視床に一致して両側性に比較的限 局して脳血流低下部位を捉えることができる. FDG−PET 同様,PTSD や外傷後抑うつ状態等の機能 的病態でもしばしばこれらの部位の血流低下は観察され るが,これらの機能的病態では帯状回,前頭前野内側, 前頭葉底面,視床に血流低下域が限局するよりむしろ脳 の器質的損傷例に比べ両側大脳半球円蓋部に比較的広範 に軽度の血流低下域が散在することが特徴である(Fig. 6)4)15).高次機能障害出現のメカニズム
Structural MRI,DTI などの形態画像,MRS に代表さ れる代謝物質組成解析画像では,びまん性脳外傷による 脳損傷器質的病巣が脳梁,脳弓,大脳基底核部,大脳半 球深部白質に存在することが示唆された.有限要素頭部Fig. 7 Shear stress distribution of the brain by
traumatic rotational impact using a finite element brain model
The central structures of the brain, including the corpus callosum, fornix, basal ganglia, diencephalon, and brain stem, are predisposed to shear stress injury by traumatic rotational impact from any directions. Especially, the splenium is susceptible by impacts from any directions, and the genu of the corpus callosum and thalamus are susceptible by sagittal impact.(These figures were cited from Ref. 13. with permission of the authors.)
Sagittal Lateral Vertical Lateral Sagittal Vertical
コンピューターモデルを用いた頭部への衝撃実験では, 前後方向回転衝撃,左右方向回転衝撃,水平回転衝撃の いずれの衝撃においても脳幹と脳梁を中心としたその近 傍(帯状回,脳弓,視床,大脳半球深部白質)に最大の 応力が生じる.特に,前後方向回転衝撃では脳梁膝部, 脳梁膨大部,視床,左右方向回転衝撃では脳梁膨大部, 脳幹,水平回転衝撃では脳梁膨大部に大きな応力が生じ るとされる(Fig. 7)13).これらの結果は structural MRI,
DTI で示された病変部位ときわめて近似した領域で軸 索損傷が生じやすいことを示しており,structural MRI, DTI で示された病変は脳内に実際に存在する器質的病 変である可能性を強く裏づけている. 厚生労働省基準で定められた高次脳機能障害の病態か ら想定される「高次脳機能」とは,五感(視覚,聴覚, 味覚,嗅覚,触覚)から得られた情報を過去に蓄えられ た情報(記憶)を基に解析,処理し,感情や情動をうま く抑制しながら目的に到達するまでの適切な行動を含む 一連の脳認知機能と解釈すると理解しやすい.すなわち, 「高次脳機能」とは大脳新皮質,大脳基底核,大脳辺縁系 それぞれと,それら相互の情報伝達回路(ネットワーク) の統合された機能を指すと考えられる. びまん性脳損傷の本質は剪断力による軸索損傷と考え られるので,大脳新皮質,大脳基底核部,大脳辺縁系に おける相互の情報伝達回路がこれらの部位の軸索損傷に より破綻することによって高次脳機能障害が出現する. 一方,びまん性脳損傷による高次脳機能障害患者を対象 とした FDG−PET,ECD−SPECT,fMRI といった機能画 像は structural MRI,DTI などの形態画像でみられる器 質的病巣と解剖学的部位がやや異なり,一様に帯状回, 前頭前野内側部で脳機能低下を示す.これらの部位の障 害は一次的損傷によるものも存在するが,むしろ他部位 の器質的損傷によって引き起こされる神経伝達・伝導の 障害により二次的に生じた機能障害と考えるほうが理解 しやすい.このような最新の画像所見から推論すると, びまん性脳損傷後に出現する高次脳機能障害は外傷時に 脳に加わる煎断力で器質的損傷を受けた一次的損傷部位 の機能障害,すなわち一次的損傷で損傷された軸索が 担っていた情報伝達回路の機能障害,さらにそれら軸索 損傷に起因する神経伝達・伝導障害によって生じた二次 的損傷部の機能障害が合わさった障害と考えられる. 文 献
1)Asano Y, Shinoda J, Okumura A, Aki T, Takenaka S, Miwa K, Yamada M, Ito T, Yokoyama K:Utility of fractional ani-sotropy imaging analyzed by statistical parametric
map-ping for detecting minute brain lesions in chronic−stage patients who had mild or moderate traumatic brain injury. Neurol Med Chir(Tokyo) 52:31−40, 2012.
2)Cubon VA, Putukian M, Boyer C, Dettwiler A:A diffusion tensor imaging study on the white matter skeleton in indi-viduals with sports−related concussion. J Neurotrauma
28:189−201, 2011.
3)Garnett MR, Blamire AM, Rajagopalan B, Styles P, Cadoux−Hudson TA:Evidence for cellular damage in nor-mal−appearing white matter correlates with injury sever-ity in patients following traumatic brain injury:A mag-netic resonance spectroscopy study. Brain 123:1403− 1409, 2000. 4)後藤杏里,粳間 剛,安保雅博:リハ患者の意欲が乏し い.リハ医のモヤモヤ解決!こんなときどうする? 臨 床リハ 19:393−397,2010. 5)糟谷幸徳,田野倉亮,福山誠介,浅野好孝,篠田 淳: MR spectroscopy(MRS)による遷延性意識障害患者の評 価.第 19 回日本意識障害学会プログラム・抄録集.意 識障害の医療―深遠にある科学―.p.34,2010. 6)国立身体障害者リハビリテーションセンター:高次脳機 能障害支援モデル事業報告書―平成 13 年度∼平成 15 年度のまとめ―.2004. 7)厚生労働省社会・援護局障害保健福祉部,国立身体障害 者リハビリテーションセンター:高次脳機能障害者支援 の手引き.2006.
8)Messé A, Caplain S, Pélégrini−Issac M, Blancho S, Montreuil M, Lévy R, Lehéricy S, Benali H:Structural integrity and postconcussion syndrome in mild traumatic brain injury patients. Brain Imaging Behav 6:283−292, 2012.
9)Metting Z, Rödiger LA, De Keyser J, van der Naalt J: Structural and functional neuroimaging in mild−to−moder-ate head injury. Lancet Neurol 6:699−710, 2007. 10)中島八十一:厚生労働省科学研究費補助金こころの健康
科学研究事業.高次脳機能障害者に対する地域支援ネッ トワークの構築に関する研究―平成 18 年度∼平成 20 年度総合研究報告書―.2009.
11)Nakayama N, Okumura A, Shinoda J, Yasokawa YT, Miwa K, Yoshimura S, Iwama T:Evidence for white matter dis-ruption in traumatic brain injury without macroscopic lesions. J Neurol Neurosurg Psychiatry 77:850−855, 2006.
12)Nakayama N, Okumura A, Shinoda J, Nakashima T, Iwama T:Relationship between regional cerebral metabolism and consciousness disturbance in traumatic diffuse brain injury without large focal lesions:an FDG−PET study with statistical parametric mapping analysis. J Neurol Neu-rosurg Psychiatry 77:856−862, 2006.
13)大西壮馬,平林智子,田中栄一:回転衝撃負荷における 脳の力学応答.(personal communication).
14)Soeda A, Nakashima T, Okumura A, Kuwata K, Shinoda J, Iwama T:Cognitive impairment after traumatic brain inju-ry:a functional magnetic resonance imaging study using the Stroop task. Neuroradiology 47:501−506, 2005. 15)竹中俊介,篠田 淳,浅野好孝,秋 達樹,三輪和弘,
岩間 亨:頭部外傷後遺症・高次脳機能障害の核医学診 断.第 2 回日本ニューロリハビリテーション学会学術集 会プログラム・抄録集.p.68, 2011.
16)Van Boven RW, Harrington GS, Hackney DB, Ebel A, Gauger G, Bremner JD, D’Esposito M, Detre JA, Haacke EM, Jack CR Jr, Jagust WJ, Le Bihan D, Mathis CA,
Muel-ler S, Mukherjee P, Schuff N, Chen A, Weiner MW: Advances in neuroimaging of traumatic brain injury and posttraumatic stress disorder. J Rehabil Res Dev 46: 717−757, 2009.
17)Yasokawa YT, Shinoda J, Okumura A, Nakayama N, Miwa
K, Iwama T:Correlation between diffusion−tensor mag-netic resonance imaging and motor−evoked potential in chronic severe diffuse axonal injury. J Neurotrauma 24: 163−173, 2007. 高次脳機能障害を引き起こす外傷性脳損傷の画像評価 ―特にびまん性脳損傷慢性期の画像について― 篠田 淳 浅野 好孝 従来,頭部外傷後に記憶・記銘力障害,注意障害,遂行機能障害,社会的行動障害を後遺し社会に 適応できない人たちの存在は十分理解されなかった.国は彼らに「高次脳機能障害」という傷病名を つけ障害者として行政支援の対象とすることにした.本障害診断基準では画像で脳の器質的疾患が確 認されることが必要とされる.近年,MRI の新しい撮像法,SPECT や PET は従来の画像では確認で きなかった脳の損傷を捉えることを可能にした.これらの画像は従来「見えない障害」と呼ばれてき た高次脳機能障害を「見える障害」へ移行させつつある.びまん性脳損傷慢性期の画像診断と画像所 見から推測できる本障害のメカニズムについて述べる.
脳外誌 22:842−848,2013