はじめに
椎弓根スクリューの手技での固定術の安全性や 手術成績の安定性が浸透し,脊椎固定術では後方 アプローチが選択されることが多い.Polyaxial 構 造である経皮的椎弓根スクリュー(percutaneous pedicle screw: PPS)の登場にて,instrumentation の 低侵襲化が図れるようになり,出血量や手術時間 の低減が得られるようになった.脊椎破裂骨折の 手術においても,PPS による制動固定術が応用さ れつつある.しかし polyaxial 構造の性質上,椎体 の圧潰が高度でかつ後弯が強い場合の整復矯正は 困難であった.今回,経皮的 uniplanar monoaxial screw システムを用いて加療を行った腰椎破裂骨 折の椎体整復効果を報告する. 症 例 患 者:34 歳,女性 既往歴:うつ病での加療歴あり. 現病歴:アルコール飲酒時に口論となり,3階 福岡記念病院 脳神経外科 [Corresponding author] 隈元真志:〒 814‒8525 福岡市早良区西新1丁目 1‒35
原 著
Neurosurg Emerg 24: 127-132, 2019高度圧潰を伴う腰椎破裂骨折に対する
経皮的 uniplanar monoaxial screw を用いた後方低侵襲手術の
椎体整復効果
隈元真志
1),古市将司
2),溝田新吾
2),大田正流
2),中山大資
3), 口健吾
3),本家秀文
3)福岡記念病院 脊髄脊椎外科
1)福岡記念病院 脳神経外科
2)福岡記念病院 整形外科
3)要旨:経皮的椎弓根スクリュー(percutaneous pedicle screw: PPS)システムを用いた 低侵襲後方脊椎制動固定術は,外傷においても有用な治療選択肢であるが,polyaxial screw では椎体整復操作が困難であった.システムの進歩により椎体整復が可能とな りつつある.当院で加療を行った高度圧潰を伴う腰椎破裂骨折症例の経過を報告する. 症例は 34 歳女性で,高所から転落し救急搬送された.T12 棘突起骨折,L1 破裂骨折 と仙骨骨折,右橈骨骨折,両踵骨骨折を認めた.受傷直後は両下肢がしびれていたが 1日の経過で軽減した.L1 椎体損傷は LSC(load sharing classification)で7点であっ た.手術は Medtronic 社 SOLERA®の PPS である Sagittal Adjusting Screw および Trauma
Instrument Set を用いて,T12‒L2 の後方脊椎制動固定術を行った.骨片占拠率は 60% から 16%に改善した.これまで後方 instrumentation での整復には,従来の開放手技で monoaxial screw を用いていたが,中腔構造をもつ monoaxial screw の登場により,PPS による低侵襲法でも椎体の整復が可能となり,脊柱管に対して ligamentotaxis を用い た間接除圧が可能になった.本症例のように LSC 7点で前方の再建が推奨されるよ うな症例に対しても後方低侵襲法単独で治療できる可能性が示唆された.
Key words: thoracolumbar burst fracture, percutaneous pedicle screw, minimally invasive, monoaxial screw
から転落し当院に救急搬送された.入院時現症: 受傷直後は両下肢全体がしびれていたが下肢麻痺 は認めなかった.膀胱直腸障害は認めなかった. 放射線学的検査:頭部から骨盤までの CT にて T12 棘突起骨折,L1 破裂骨折と仙骨骨折を認めた. 頭部,胸部腹部臓器損傷は認めなかった.MRI で は L1 椎体前縦 帯損傷,T12/L1 棘間 帯,棘上 帯損傷を認めた.さらに後壁骨片突出に伴う脊 柱管狭窄を認めた(Fig. 1).他,右橈骨遠位端骨 折と両踵骨骨折を認めた.両下肢しびれは1日の ベッドレストで軽減した.L1 椎体損傷は LSC (load sharing classification)で7点であった.TLICS (Thoracolumbar Injury Classification and Severity
Score)で5点,新 AO 分類にて B(3)N(1)M(2), Thoraco-Lumbar AOSpine Injury Score で7点と診 断した.
手術方法:多発外傷であり,両踵骨骨折,右橈 骨遠位端骨折の観血的整復術と同日に脊椎固定術 を施行した.手術は SOLERA®の SAS®(Sagittal
Adjusting Screw)お よ び Trauma Instrument Set®
(Medtronic Sofamor Danek)を用いた(Fig. 2a).骨 折椎体上下の one level above, one below の short segment での PSF(pedicle screw fixation)を行い, 脊柱管内に突出した骨片は ligamentotaxis を用い て整復し固定した.整復が不十分で神経症状が出 現あるいは後弯が進行した場合に備えて,二期的 前方アプローチによる椎体置換の可能性を考慮し, L1 骨折椎体には椎体形成や screw 刺入は行わな かった. 術後経過:両踵骨骨折のため免荷が必要であっ たが,脊椎への荷重は翌日から許可し,良好に経 過した.骨片占拠率は術前の 60%から術後9ヵ 月で 16%に改善した.術直後には椎体前壁が 25.8 mm から 35.2 mm に,椎体後壁が 33.6 mm か ら 37.8 mm にそれぞれ整復された.9ヵ月で前壁 は 27.3 mm,後壁は 37.4 mm と矯正損失を認めた が,椎体楔状角は -13.3 度から -10.2 度に維持され ていた(Fig. 3). 考 察 胸腰椎移行部での骨折は全脊椎損傷のうち約 90%を占めるとされ,破裂骨折はその 10∼20% とされる1,3).これほど頻度が高いにも関わらず, 胸腰椎破裂骨折に対する治療法には明確な基準が ない.保存加療および手術加療の選択基準や,手 術アプローチの選択においても前方法か後方法か, あるいは両方からのアプローチか,それならば前 方から先に行うか,後方から行うか,一期的か, Fig. 1 a: Initial sagittal thoraco‒lumbo‒sacral computed tomography
image indicates L1 burst fracture, T12 spinous process fracture, and sacral fracture at the S3 level. b: Initial axial computed tomography image at L1 level reveals severe comminution of the vertebral body and posterior fragments causing spinal canal stenosis. c: Initial short‒T1 inversion recovery magnetic resonance image indicates injuries to the anterior longitudinal ligament at the L1 vertebral body and inter/supra‒spinous ligaments at the T12/L1 levels. Posterior fragments strongly compress the conus medullaris.
二期的か,後方法では固定範囲は short か long か, など未だに controversial である.すなわち,神経 症状の有無,椎体の圧潰・後弯の程度,不安定性 の程度,骨質,手術の侵襲,年齢,全身状態など, さまざまな要素を考慮しながら個々の病態に合わ せて治療法を選択しているのが現状である.神経 脱落症状が無い場合においては,Denis らは胸腰 椎破裂骨折では予防的安定化を推奨している2)が, 一方で不安定性や後彎変形の程度を問わず,神経 症状がない症例は保存加療のほうが治療成績に優 れる12)との報告もあり,見解が未だ定まらない. 後彎変形においては,Shen らや Wang らは後弯変 形をきたした状態で癒合した場合には日常生活に おいて著明な支障が遺残する症例があることを報 告し12,17),また,Wood らも同様に,神経症状がな い症例においても後弯が遺残すると予後不良にな ることを報告18)し,後弯矯正の重要性を示唆した. 骨折後の後彎変形は偽関節や遺残腰痛の問題が発 生すること喚起されており9,15),後弯変形が強い 症例に対しては,保存加療よりも手術加療が行わ Fig. 3 Computed tomography images obtained preoperatively (a),
3 months postoperatively (b), and 9 months postoperatively (C) reveal good reduction of L1 vertebral body and the posterior wall. Fragment occupancy rate for spinal canal has improved from 60% to 16%, finally.
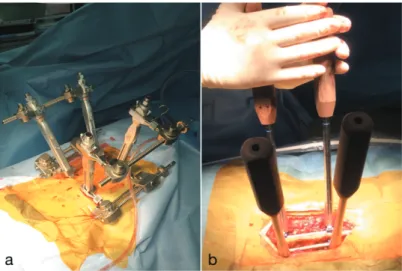
Fig. 2 a: Intraoperative view shows percutaneous uniplanar monoaxial pedicle screws (Sagittal Adjusting Screws®) connected to
the Trauma Instrument Set® (Medtronic Sofamor Danek). This set
appears to be an external fixation used for a long bone. b: The photograph presents conventional open surgery using monoaxial screws (Schantz screw®, DePuy/Shynthes). This procedure requires
れる傾向にある10).
手術アプローチについては,椎体圧潰が高度で, 脊柱管への骨片の突出が強く,後弯変形が強い場 合 は 通 常 は 損 傷 椎 体 の 再 建 が 考 慮 さ れ る. McCormack らは Load sharing classification による 損傷椎体評価の標準化を提唱し,7点以上であれ ば前方支柱再建したほうが臨床成績に優れること を報告した7).近年では後方アプローチによる椎 弓根スクリュー手技での固定術の安全性や手術成 績の安定性が浸透し,後方アプローチが選択され ることが多くなった16).さらにデバイスが進化し, 経皮的な椎弓根スクリュー(percutaneous pedicle screw: PPS)の登場により従来の開放手術に対し て低侵襲法が選択されるようになった10).ただし, PPS は中空での polyaxial スクリューの構造が特徴 である.その構造は経皮的な刺入の簡便性をもた らした代わりに,矯正力がダイレクトに伝わらず, 積極的な椎体の整復操作は困難であった6).よっ て胸腰椎破裂骨折の整復および後弯の矯正を後方 アプローチで行う場合は,従来の開放手技による monoaxial screw を用いた short segment による手術
が有用であり13),著者らも骨粗鬆症を合併しない
若年者に対しては,開放手技で monoaxial screw で ある USS Fracture system®,Schantz screw®(DePuy/
Shynthes)を用いて徒手的に整復し(Fig. 2b), above one,below one での骨移植を用いた2椎間 後方固定を行い,整復が不十分,あるいは矯正損 失を早期に招くようであれば二期的に前方アプロ ーチで前方支柱再建を行う方針としていた.しか し従来の後方開放手技では傍脊柱筋群に対する侵 襲が大きいため医原性筋萎縮を来たす14).医原性 筋萎縮は術後の腰背部遺残の一因である8).PPS シ ステムは従来の開放手術に伴う軟部組織および傍 脊柱筋の損傷なしに,instrumentation を行うこと ができる.今日に至るまで PPS による低侵襲法の 従来法に対する非劣性,あるいは優位性について の多くの議論が行われており,低侵襲法は出血量, 手術時間,術後 痛の低減が得られること,後方 の軟部組織の侵襲が少ないことなどが最大の利点 としてあげられる5).Jiang らは randomized control
study にて PPS 群において痛みの低減と機能のよ りよい改善が得られたことで,傍脊柱筋群への侵 襲が少ないメリットを強調した4).Kumar らは従 来 法 と PPS 法 と を 前 向 き に 検 討 し,Oswestry Disability Index で PPS 群が優位に改善したことを 報告し,低侵襲法での加療を推奨した6). 現在デバイスはさらに進化し,経皮的 monoaxial screw システムにより低侵襲後方アプローチ単独 でも椎体の整復およびアライメント矯正が可能に なりつつある.SAS®はロッド締結部のスライド サドル機構によりロッド締結時に一方向のみスラ イドすることでロッド締結を容易にした uniplanar monoaxial screw の構造をもつ中空の PPS である. Trauma Instrument Set®に接続し,いわば長管骨の
創外固定器具のような感覚で経皮的に骨折椎体の 整復矯正操作が可能である.従来の polyaxial screw が持ち得ない,整復時や矯正時に要する強固な distraction force ならびに前弯形成のための comp-ression force を加えることができる.本症例では, 許容できる椎体整復を得ることができ,かつ脊柱 管の突出骨片を後縦 帯による ligamentotaxis に て整復することが可能であった.本症例のように LSC7点で,前方アプローチによる損傷椎体の再 建が推奨されるような症例に対しても uniplanar monoaxial screw の PPS を用いることで,低侵襲後 方アプローチ単独で治療できる可能性が示唆され た.ただし,術中に想定していた整復が得られな い場合や,術後経過で許容できない矯正損失が生 じることが懸念されるので,二期的前方支柱再建 術の追加が必要となる可能性を念頭に置いた,細 やかな術前の説明と同意を得ることが肝要である. 後方法を選択した場合,固定範囲をいかに判定す るかも論じられる点である.先にも述べたとおり 神経症状の有無,椎体の圧潰・後弯の程度,不安 定性の程度,患者の骨質,手術の侵襲,年齢,全 身状態など多くの要素を熟考しながら決定される. 本症例は活動性の高い若年者ではあったが,骨質 不良なく椎体損傷が一椎体であったため,above one, below one の short segment による PPS 固定を 行った.9ヶ月の経過で矯正損失が生じており, 許容される経過かどうか引き続き慎重なフォロー が重要である.後方 PPS 固定法は椎体間癒合を目 指した手術ではないため,骨折椎体の癒合後にイ ンプラントを抜去することで mobile segment の温
存が可能11)であることもメリットである.一方で, インプラント抜去後に矯正損失が発生あるいはさ らに悪化する可能性があることも今後の課題のひ とつである17).本手技は,損傷椎体の前方支柱再 建を行っていないので implant failure や矯正損失 の発生等,後方固定術後ならびに抜釘後も慎重な 観察が重要であることは論を俟たない. まとめ
経皮的 uniplanar monoaxial screw システムを用 いて加療を行った腰椎破裂骨折の椎体の整復効果 を報告した.LSC7点のような前方手術が推奨さ れる高度圧潰症例でも整復効果は比較的維持され た.経皮的 uniaxial screw あるいは monoaxial screw を用いた破裂骨折の整復効果の報告例は少なく, 今後の症例の蓄積が期待される.
本論文の発表に関して開示する COI はありま せん.
文 献
1) Denis F: The three column spine and its significance in the classification of acute thoracolumbar spinal in-juries. Spine (Phila Pa 1976). 8: 817‒831, 1983. 2) Denis F, Armstrong GW, Matta L, et al: Acute
thora-columbar burst fractures in the absence of neurologic deficit. A comparison between operative and nonop-erative treatment. Clin Orthop Relat Res. (189): 142‒149, 1984.
3) Esses SI, Botsford DJ, Kostuik JP: Evaluation of surgi-cal treatment for burst fractures. Spine (Phila Pa 1976). 15: 667‒673, 1990.
4) Jiang XZ, TianW, Liu B, et al: Comparison of a para-spinal approach with a percutaneous approach in the treatment of thoracolumbar burst fractures with poste-rior ligamentous complex injury: a prospective ran-domized controlled trial. J Int Med Res. 40(4): 1343‒1356, 2012.
5) Kim DY, Lee SH, Lee HY, et al: Comparison of mul-tifidus muscle atrophy and trunk extension muscle strength: percutaneous versus open pedicle screw fixa-tion. Spine (Phila Pa 1976). 30(1): 123‒129, 2005. 6) Kumar A, Aujla R, Lee C. The management of
thora-columbar burst fractures: a prospective study between
conservative management, traditional open spinal sur-gery and minimally interventional spinal sursur-gery. Springer Plus. 4: 204, 2015.
7) McCormack T, Karaikovic E, Gaines RW. The load sharing classification fractures. Spine (Phila Pa 1976). 19(15): 1741‒1744, 1994.
8) Ni WF, Huang YX, Chi YL, et al: Percutaneus pedicle screw fixation for neurologic intact thoracolumbar burst fractures. J Spinal Disord Tech. 23(8): 530‒ 537, 2010.
9) Oda I, Cunningham BW, Buckley RA, et al: Does spinal kyphotic deformity influence the biomechanic characteristics of the adjacent motion segment? An in vivo animal model. Spine (Phila Pa 1976). 24(20): 2139‒46, 1999.
10) Proietti, L. Scaramuzzob L, Tamburrelli FC, et al: Posterior percutaneous reduction and fixation of tho-raco‒lumbar burst fractures. Orthop Traumatol Surg Res. 100(5): 455‒460, 2014.
11) Rahamimov N, Mulla H, Freiman S, et al: Percutaneous augmented instrumentation of unstable thoracolumbar burst fractures. Eur Spine J. 21(5): 850‒854, 2012. 12) Shen WJ, Liu TJ, Shen YS: Nonoperative treatment
versus posterior fixation for thoracolumbar junction burst fractures without neurologic deficit. Spine (Phila Pa 1976). 26(9): 1038‒45, 2001.
13) Steib JP, Charles YP, Aoui M. In situ contouring tech-nique in the treatment of thoracolumbar Fractures. Eur Spine J. 19 (1): S66‒S68, 2010.
14) Styf JR, Willen J. The effects of external compression by three different retractors on pressure in the erector spine muscles during and after posterior lumbar spine surgery in humans. Spine (Phila Pa 1976). 23(3): 354‒358, 1998.
15) Tropiano P, Huang RC, Louis RP, et al: Functional and radiographic outcome of thoracolumbar and lumbar burst fractures managed by closed orthopaedic reduc-tion and casting. Spine (Phila Pa 1976). 28(21): 2459‒65, 2003.
16) Verlaan JJ, Diekerhof CH, Buskens E, et al: Surgical treatment of traumatic fractures of the thoracic and lumbar spine: A systematic review of the literature on techniques, complications, and outcome. Spine (Phila Pa 1976). 29(7): 803‒814, 2004. Review.
17) Wang XY, Dai LY, Chi YL, et al: Kyphosis recurrence after posterior short‒segment fixation in thora columbar fractures. J Neurosurg Spine. 8(3): 246‒ 54, 2008.
18)Wood KB, Buttermann GR, Harris MB, et al: Operative compared with nonoperativetreatment of a thoracolumbar burst fracture without neurological deficit. Aprospective, randomized study. J Bone Joint Surg Am. 97(1): 3‒9, 2015.