Verification of Reliability and Validity of the Development of Growth Motivation Scale for
Nurses
新, 裕紀子
http://hdl.handle.net/2324/4474995
出版情報:九州大学, 2020, 博士(看護学), 課程博士 バージョン:
権利関係:
Verification of Reliability and Validity of the Development of Growth Motivation Scale for Nurses
Authors: Yukiko Arata, MSN, RN1),2), Hisako Nakao, PhD,RN1), Tatsuyuki Kakuma,PhD,MPH3)
1)Department of Health Sciences, Graduate School of Medical Sciences, Kyushu University,
Fukuoka, Japan
2)School of Nursing, Kurume University, Kurume, Japan
3)The Biostatistics Center, Kurume University, Kurume, Japan
Running Title: Development of GMSN
Abstract
Aim: We aimed to verify the reliability and validity of a growth motivation scale developed for nurses.
Methods: We created a 30-item scale derived from the results of qualitative research and implemented a self-administered questionnaire to clinical nurses working in 18 hospitals across Japan. Ultimately, 607 questionnaires were included in the analysis.
Results: In factor analysis, we extracted 24 items and the following 4 factors: “autonomous contribution to the organization”; “personal readiness and abundance of work environment resources”; “self-adjustment with awareness of others”; and “goals originating from regret,” with Cronbach’s αs of 0.90, 0.82, 0.81, and 0.74 respectively, and 0.92 for the overall scale. In the examination of coexistence validity, the scale was significantly correlated with the “Multi-faceted Work Motivations” scale.
Conclusions: The growth motivation scale for nurses was favorable in terms of both reliability and validity and was shown to be an effective scale for measuring growth motivation in nurses. It is necessary to retest the scale and examine its stability in future.
Keywords: growth, motivation, nurses, scale development
Introduction
Nursing professionals are expected to pursue expertise, grow autonomously, and provide high-quality nursing care that fulfills the needs of a changing society1). The development of nurses’ careers is the responsibility of an organization as well as the responsibility of the individuals themselves without depending on management2). In other words, in addition to nurses being expected to continue to grow autonomously, the organization must provide an environment that enables nurses to continue to develop throughout their careers. Furthermore, for nurses, professional development is expected throughout their lives and careers.
So what does the word “growth” signify for a nurse? In previous literature, the growth of nurses is occasionally described using phrases such as “post-traumatic growth” and “professional growth.”
Post-traumatic growth (PTG) refers to the experience of positive change that results from overcoming challenges and crises3). Since nurses are constantly exposed to the psychological pain and distress of patients and their families, they experience PTG, which affects their quality of life in both personal and professional aspects4)5). PTG also has been examined in studies of nurses who provide rescue services in disaster settings6). Overcoming psychological stress while experiencing it is important in the personal growth of nurses in an occupation which involves confronting the illness and death of patients. The Personal Growth Initiative Scale (PGI-S)7)8) is one of the few scales that has been developed to assess growth. Personal Growth Initiative (PGI) is a concept that has two dimensions,
namely cognitive and behavioral, with which individuals proactively intend to achieve personal growth to improve their lives. The concept is also related to overall level of quality of life, which can be described as well-being9)10). However, the PGI-S is not designed to be specifically used for the occupation of nursing. While there are no scales that focus solely on the growth of nurses, one of the six factors of the Misener Nurse Practitioner Job Satisfaction Scale (MNPJSS)11) which measures the job satisfaction of nurses, is related to professional growth. The factor for professional growth is also related to nurse management. The quality of patient care depends on the experience and knowledge of nurses. Any progressive health care organization needs to invest in the professional growth of nurses to survive and provide quality care12). Earlier studies have reported that professional growth is associated with empowerment and job satisfaction13), and that such association has a positive impact on the quality of patient care14). In addition, it has been claimed that the growth of nurses exerts an impact on work continuity15). Moreover, a concept analysis of clinical growth in nursing education found that clinical growth leads to personal growth16). It can be said that personal growth and professional growth are interrelated. Further, similar to Dewey’s17) description of human growth as a sequence in “the continuity of experience,” growth exists on a continuum. Certain studies that have examined the importance of accumulating experiences as well as slow growth suggest that differences in the perception of growth between nurses may affect the degree to which they reconstruct their experiences. From the aforementioned, it is clear that an increasing number of studies have pointed to
the growth of nurses and examined related factors. However, the concept of growth for nurses remains unclear and has been operationally defined in individual studies, like “career advancement and promotions18)” and “changes that take place due to learning and experiencing from interacting with others over the course of nursing practices19).”
Collectively, across multiple studies, definitions of nurse growth include the concept of change through experiences and skill acquisition, and the evolution of interactions and relationships associated with nursing practice. However, a clear and consistent definition has yet to be adopted. Therefore, both the methods used to quantify nurses’ growth and the development of strategies to facilitate growth remain poorly defined.
Currently, the clinical ladder is used as an effective means for facilitating the professional growth of nurses20). The clinical ladder measures the levels of clinical skills of nurses. It aims to offer processes for rewarding nurses in accordance with their clinical skills as well as a means for career progression21). The clinical ladder evaluates nurses’ practical skills in line with their career stages. Most current clinical ladder programs adopt the Novice to Expert model22) by Benner. Various studies on the clinical ladder have been conducted and published in many different countries, and the clinical ladder is adopted in clinical settings23)24). However, to comprehensively evaluate the growth of nurses, it is important to not only evaluate competencies such as clinical skills but also objectively and regularly evaluate the condition of nurses, so that it can be understood to what extent nurses can be proactive in
working on their growth at given time points. A set of processes in which nurses proactively work on their growth can be referred to as motivation.
In psychology, motivation is the process of arousing and sustaining action, as well as regulating and directing behavior25). To date, motivation has been examined from various vantage points such as psychosocial, expectancy, need-based, intrinsic, social goal setting, and self-concept-based perspectives26). The term motivation, is also commonly used in areas of psychology and management27). Recent studies that put forward motivation theories have examined directed motivational currents (DMCs)28) and similar aspects which involve the orientation that facilitates long- term, continuous behavior for achieving goals. DMCs are also considered a strong motivational strategy for tackling indifference and reduced motivation. This motivational concept may help nurses to maintain their motivation as they are expected to engage in self-improvement on a daily basis, and continue to grow.
To date, studies on the motivation of nurses have examined various aspects including the following:
systems of nurse management and care provision29)30); job retention and turnover31); and commitment32). Also, scales that have been used to date in measuring the motivation of nurses include:
the Job Diagnostic Survey29) by Hackman and Oldham33); Intrinsic Job Motivation34) by Warr et al.35); the Motivation at Work Scales32)36) by Gagné et al.37); and Multi-Faced Work Motivation by Ikeda and Morinaga38). These scales were developed in the area of industrial psychology for the purpose of
assessing employees, and were not based on the characteristics of the work of nurses. In recent years, a number of work motivation scales that take into account nurses have also been developed39)40). Increasingly, research that points to occupational characteristics has been conducted. However, as the concept of motivation for work has multi-faceted meanings, the challenge of finding concepts unique to nurses and the need for the development of a scale remain41).
A study involving older nurses found that they wanted to improve the wellbeing and comfort of patients, and that the well-being of nurses can be improved when nurses collaborate with each other in caring for patients42). When nurses develop themselves and continuously grow for the sake of others through interaction with patients and colleagues, it is likely that nurses can benefit patients. It can be said that nurses are a unique group of professionals in that nurses deal directly with the diseases and lives of patients, provide patients with the best care possible, and find meaning in working together with other nurses in the workplace. Researching the growth motivation of nurses should provide important insights to contribute to the well-being of patients and nurses. However, while much research has been done on growth and motivation, no studies have focused on motivation oriented to the subjective and continuous growth of nurses as professionals.
For nurses to grow autonomously, it is necessary to understand the motivation process of nurses, including what they think, how they judge, and how they act as part of their experience toward growth.
Arata et al.43) conducted a qualitative study on the structure of growth motivation of nurses. The results
of the qualitative study showed that the structural model of growth motivation has four continuous hierarchical structures, and each layer has two dimensions: cognitive and behavioral. Their research clarified the state of continuous growth in nurses’ experiences. Therefore, it is possible to create a comprehensive scale that is relevant for participants of various ages. We predict that if a scale of growth motivation for nurses is created, it would be possible to understand their individual motivation states and apply the scale regularly. Moreover, if the mechanism that promotes nurses’ growth could be elucidated and an evaluation tool created, it would contribute to the promotion of career development, improve the quality of patient care, and continuous education.
Therefore, to create a growth motivation scale for nurses (GMSN) which recognizes dynamic changes such as nurses’ growth based on motivational growth studies, the aim of the present study was to create and select questions and items and verify the structural model deduced from the results of a qualitative study43).
Materials and Methods 1.Study Design
The hypothetical structural model used in this study and the items in a tentative scale were referenced and created based on a previous qualitative descriptive study43). We examined the validity of the tentative scale created and refined the items using pretests. Thereafter, we used the refined scale to conduct the main investigation involving hospitals chosen from across the country. Through this
method, we verified the reliability and validity of the scale created.
1) Creation of a tentative GMSN
(1) Definition of nurses’ growth and growth motivation in nurses
It has been suggested that the growth of nurses leads to the demonstration of clinical expertise44) as well as the formation of processes accompanied by changes such as positive psychological changes following the experience of adversities45). Therefore, a consistent definition has yet to be adopted, but definitions of nurses’ growth include changes through experiences such as the acquisition of nursing skills and continuous relationships with others. In this study, we defined nurses’ growth as: “Acquiring the ability to perform highly specialized nursing practices through the experience of overcoming clinical problems, while being supported by people in the workplace, and continuing to develop as a nurse while being aware of one’s own changes as a nurse.”
Growth motivation put forward by Bauer et al.46) is a long-term improvement of eudaimonic well- being in which socio-psychological maturity and subjective happiness are integrated. This concept refers to the desire of individuals to facilitate their growth. In this study, the motivation of nurses toward growth is defined as “a series of processes facilitating the behaviors of nurses that have been recognized while nurses are working toward long-term growth.”
(2) Structural model of growth motivation for nurses
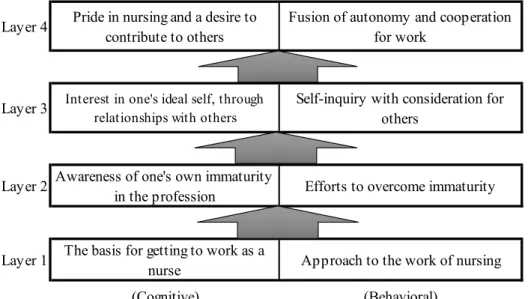
According to Arata et al.43), growth motivation for nurses consists of eight categories. Each category
is divided into four cognitive dimensions and four corresponding behavioral dimensions. Figure 1 shows the hypothetical structural model of motivation in the present study, referring to previous results.
Growth motivation for nurses consists of four layers, and each layer consists of the two dimensions:
cognitive and behavioral.
(3) Creation of items (questions)
In the present study, we created scale items from the main codes to form the categories of growth motivation for nurses based on a previous study43). The codes were short expressions of the raw data, and we endeavored to keep the meaning and content unchanged with the context in mind. We created a 30-item scale by testing each item to determine whether they expressed the constituent elements of each category sufficiently. A five-point Likert scale ranging from 1 (Strongly disagree) to 5 (Strongly agree) was used to evaluate the items.
2)Evaluation of internal validity and pretest
After creation of the tentative scale by the researchers, four university nursing teachers evaluated the internal validity of the items. The teachers have over 10 years of professional clinical experience and have educated nurses as nurse managers in clinical settings. They have expertise in nurse management, and are currently lecturing on nurse management at universities and graduate schools. After identifying the items that corresponded to the definitions of the eight constituent elements, we examined whether the items represent the content of the definitions accurately. Furthermore, as a criterion for making
objective judgments during evaluation, the items were evaluated using a four-point scale in accordance with the content validity index (CVI)47). Polit et al.48) studied literature on CVI related to nurse management and suggested that items for which at least three experts agree that the I-CVI is 0.78 or higher can be considered to have favorable content validity. Also, I-CVI guidelines put forward by Lynn47) state that the range of tolerance varies depending on the number of experts involved. In these guidelines, an I-CVI of at least 1.00 is required when five or less experts are involved. Four experts in addition to the researchers were involved in this study. Although the criterion of 1.00 was not satisfied for three items, it was determined through discussion that the content validity of these items could be ensured if the expressions were changed while maintaining the meanings and contents of the items.
Hence, the expressions of the items were changed to those on which all the four experts agreed.
Additionally, Waltz et al.49) recommend 0.90 for the mean CVI (S-CVI/AVE) of the entire scale. It was 0.92 for this study, which satisfied the recommendation.
After creating the tentative scale, we asked 10 nurses to participate in a pilot study to determine whether the questionnaire content was too difficult for the provision of responses, how understandable the terminology was, and whether any of the items made the respondents feel uncomfortable. We also conducted a pretest involving 50 nurses from three hospitals, who were recruited via convenience sampling. We confirmed the ceiling effect, floor effect, average score, standard deviation, item-total correlation, and presence or absence of missing values for the data, based on the results of 35
respondents in the pretest, and ultimately created a 30-point questionnaire, with responses provided using a 5-point Likert scale.
3) Method of the investigation
(1)Questionnaire composition
① Face sheet
To understand the participants’ characteristics, we asked them to provide details of their sex, age, and number of years of clinical experience.
② GMSN
The GMSN is a 30-item scale with four layers. Each layer consists of cognitive and behavioral items.
Responses are provided using a 5-stage Likert scale.
③ Multi-faceted Work Motivation scale
We used the Multi-faceted Work Motivation (MWM) scale created by Ikeda and Morinaga38) to examine the concurrent validity of the GMSN. Work motivation was used as a concept to represent a dynamic state in which members of an organization act to achieve a goal. The 36-item scale consists of four phases: accomplishment-oriented, competition-oriented, cooperation-oriented, and learning- oriented. Each phase is constructed of items based on three dimensions: direction, persistence, and strength. Responses are provided using a 5-point Likert scale. The scale has shown reproducibility for the four-factor structure and temporal stability upon retesting.
(2) Participant selection and questionnaire distribution
The study involved nurses working at hospitals, regardless of age and sex. Estimating a questionnaire recovery of 30%, we distributed the questionnaire with the aim of receiving 400 effective responses.
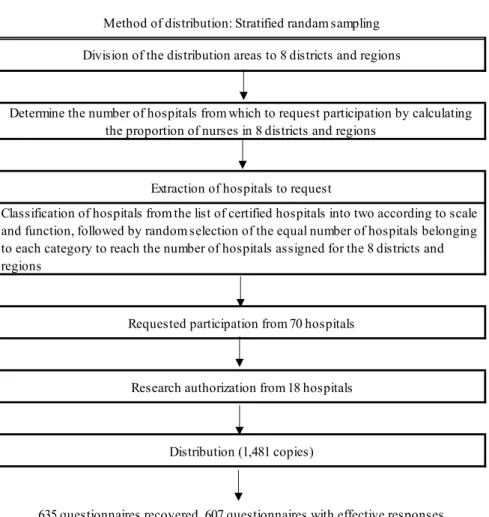
We performed stratified random sampling to conduct a nationwide survey in which the sample reflected the population composition. The proportion of nurses in each of the eight regions of Japan was calculated using data regarding the number of nursing staff relative to the population by prefecture, provided by the Japan Nursing Association50). Furthermore, as the scales and functions of hospitals differed, we searched through the list of certified hospitals at the Japan Council for Quality Health Care51) to identify the scale, function, and name of each hospital. The 2,166 certified hospitals were divided into categories according to type of function and classified as general hospitals (1,030 hospitals), which are key hospitals mainly in relatively large areas providing secondary medical care, and the remaining hospitals were classified as other hospitals (1136 hospitals). The number of certified hospitals approached to participate in the study were assigned according to the proportions of nurses in the eight districts and regions described previously, and we selected general hospitals and other hospitals evenly and randomly, to request participation in each of the eight districts and regions. We approached the head of nursing at the 70 hospitals extracted, in writing and via telephone, and explained the content of the questionnaire, ethical considerations, and method of distribution. Of these hospitals, approval was obtained from 18. The hospitals were located across all the eight regions in
Japan. For the size of the hospitals, eight of the participating hospitals were general hospitals which provide secondary care, and the other 10 were hospitals of different types. Additionally, the number of questionnaire forms to be distributed was adjusted for each hospital depending on the number of nurses based in the region. We then sent a written document containing information concerning the study, with the number of questionnaires corresponding to the number of cooperating participants, with a self-addressed envelope to allow participants to return them to the nursing department at each hospital. In total, 1,481 questionnaires were distributed. The nursing departments were asked to distribute the questionnaires to their nurses, and each nurse was asked to return the completed questionnaires themselves, using the self-addressed envelope, within two weeks of receipt. The study was conducted between February and March 2020, and the respond rate was 43% (n = 635). When forms with missing responses were excluded, the effective response rate was 96% (n = 607; Figure2).
(3) Method of analysis
Construct validity was examined using exploratory factor analysis and criterion-related validity was evaluated by examining concurrent validity via determination of correlations with the MWM scale.
Furthermore, goodness-of-fit for the hypothetical structural model in the study was measured using covariance structure analysis. To examine the reliability of the scale, we checked internal consistency by calculating Cronbach's αs for all factors individually and the overall scale. We calculated descriptive statistics for participants’ sex, age, and number of years of clinical experience and used the
Kruskal-Wallis test to examine the relationship between participants’ age and the GMSN. Statistics that exhibited significant differences were analyzed using Scheffe’s multiple comparison procedure.
We used IBM SPSS for windows v.22.0 and IBM SPSS Amos for Japan v.22.0 to perform the analysis.
2. Ethical considerations
The participants were provided with written explanations regarding the study purpose and methods and anonymity of the data, advised that refusal to participate in the study would not disadvantage them in any way, and informed that returning the questionnaire would imply consent to participate in the study. This study was conducted with approval from Kyushu University Institutional Ethical Review Board for Clinical Research (Approval number: 2019-532).
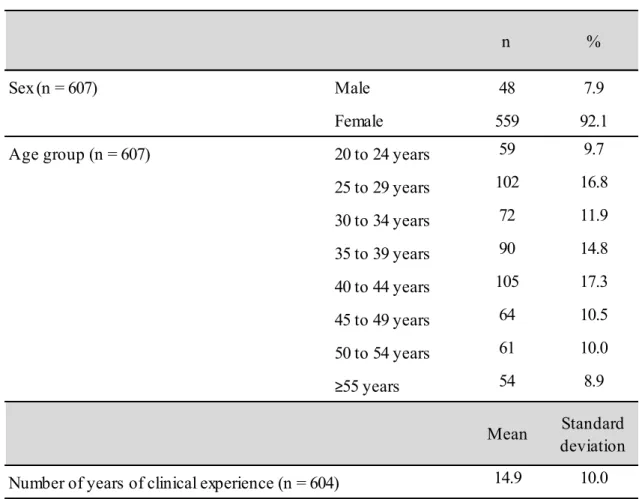
Results 1. Overview of participants (Table 1)
Of the 607 participants, 48 were men (7.9%) and 559 were women (92.1%). The age group trends plotted for every 5 years from age 20 exhibited an M-shaped curve. The mean number of years of clinical experience was 14.9 (SD:10.0).
2. Exploratory factor analysis of the GMSN and goodness-of-fit of the model
The score distribution for the 30 items of the GMSN showed no ceiling or floor effect, and the IT correlations ranged from 0.28 to 0.75. We decided not to exclude any items at this stage and included all questionnaire items in the subsequent analysis.
We then performed a factor analysis of the 30 items using the principal factor method. By referring to the change in the slope of the Scree plot, we conceived that the four-factor structure was valid.
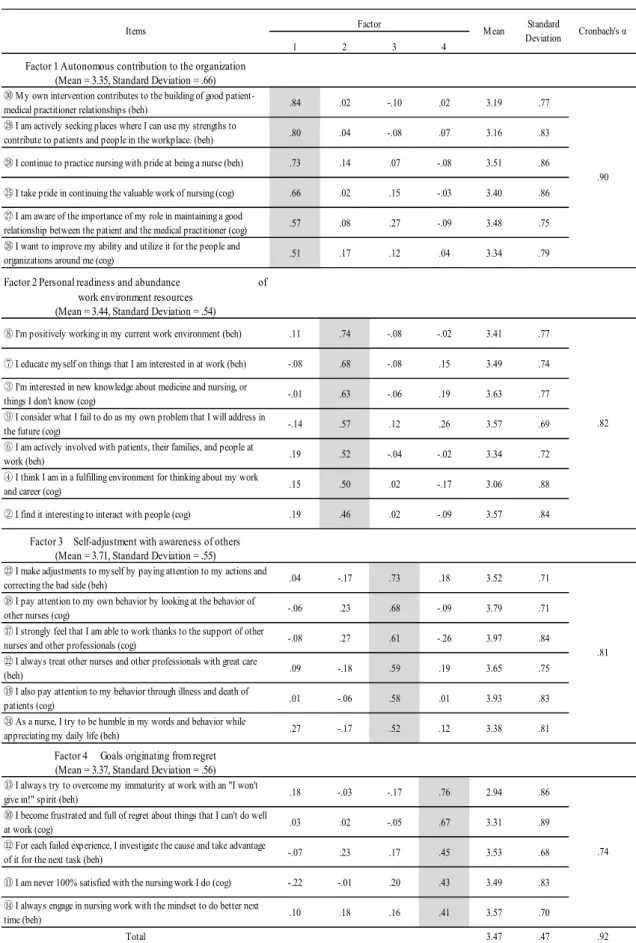
Therefore, we performed a factor analysis with principal factor and Promax rotation assuming a four- factor structure. After excluding six items that did not show sufficient factor loading, we repeated the principal factor and Promax rotation. The total variance explained by the 24 items by 4 factors was 48.69%. Table 2 shows the factor pattern after Promax rotation. The first factor was named
“autonomous contribution to the organization” because of autonomous learning and the wish to contribute to the organization as a whole. This factor is equivalent to “pride in nursing and a desire to contribute to others” and “fusion of autonomy and cooperation for work” in the hypothesis structure model (Fig. 1), which was based on the results of the qualitative research of Layer 4. The second factor was named “personal readiness and abundance of work environment resources” based on nurses’
interests and curiosity about learning and people, and enrichment of the organizational environment that supports individual nurses. This factor is equivalent to “the basis for getting to work as a nurse”
and “approach to the work of nursing” in Layer 1. The third factor was named “self-adjustment with awareness of others,” because nurses deepened their consideration of others and introspection by becoming more aware of their relationships with other staff members and patients. This factor is equivalent to “interest in one’s ideal self, through relations with others” and “self-inquiry with consideration for others” in Layer 3. The fourth factor was named “goals originating from regret”
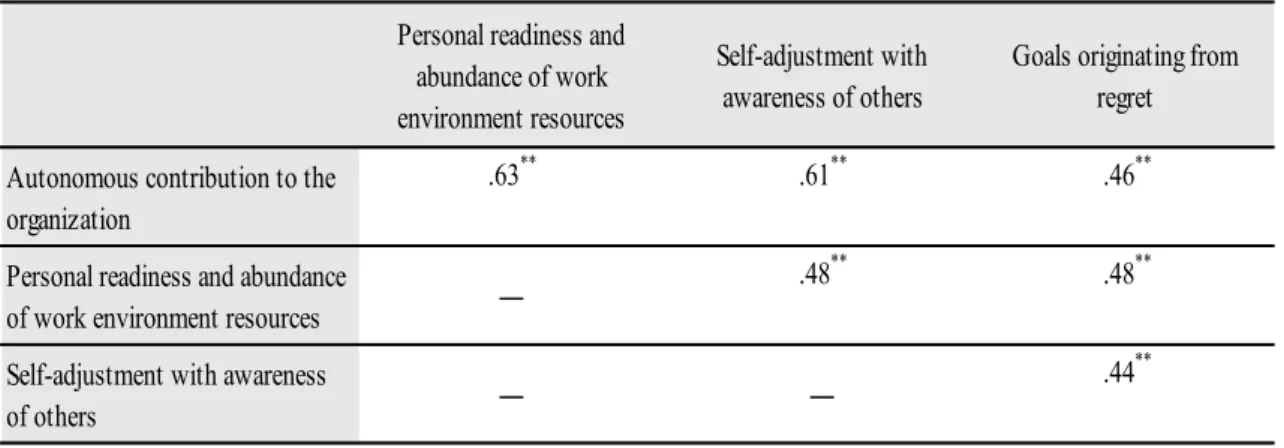
because nurses experienced regret resulting from immaturity and failures and later overcame that regret. This factor is equivalent to “awareness of one’s own immaturity in the profession” and “efforts to overcome immaturity” in Layer 2. Although Item 9 belonged to Factor 4 according to the originally- presumed concept, on this occasion it was part of Factor 2. The other 23 items were classified into their presumed concepts. Cronbach’s αs were as follows: 0.90 for Factor 1, 0.82 for Factor 2, 0.81 for Factor 3, 0.74 for Factor 4 and 0.92 for the overall scale. The correlation coefficients for the relationships between subscales using mean scores for the subscales that represented each factor (hereinafter subscale scores) are shown in Table 3. There were significant correlations ranging from 0.44 to 0.63 between all subscales.
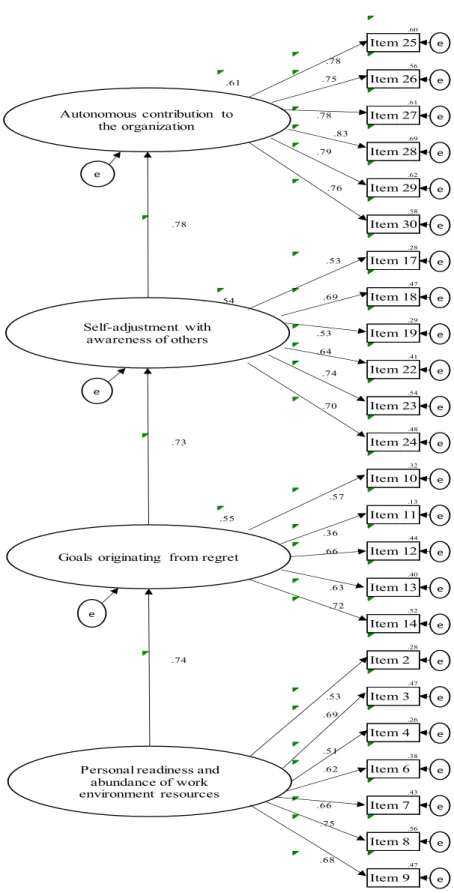
The results of the covariance structure analysis showed that all path coefficients were significant, and the goodness-of-fit indices for the model were goodness-of-fit index = 0.84, adjusted goodness- of-fit index = 0.81, comparative fit index = 0.84 and root mean square error of approximation = 0.08 (Figure 3).
3. Verification of concurrent validity
To verify the coexistence validity of the GMSN, an MWM containing the following four factors was used: accomplishment-oriented, competition-oriented, cooperation-oriented, and learning-oriented.
The Cronbach's α for the MWM scale in this study was 0.96. The results of Spearman’s correlation analysis of correlations between the mean totals for GMSN subscale scores (hereinafter GMSN score)
and MWM subscale scores (hereinafter MWM score) showed significant correlations between all scores, but the correlation between “self-adjustment with awareness of others” in the GMSN and
“competition-oriented” in the MWM scale was low, at 0.18. In contrast, the MWM subscale that was correlated most strongly with “self-adjustment with awareness of others” in the GMSN was
“cooperation-oriented,” at 0.60. “autonomous contribution to the organization” showed strong correlations with “learning-oriented” (0.64) and “accomplishment-oriented” (0.60), while “personal readiness and abundance of work environment resources” showed a strong correlation with “learning- oriented” (0.62; Table 4).
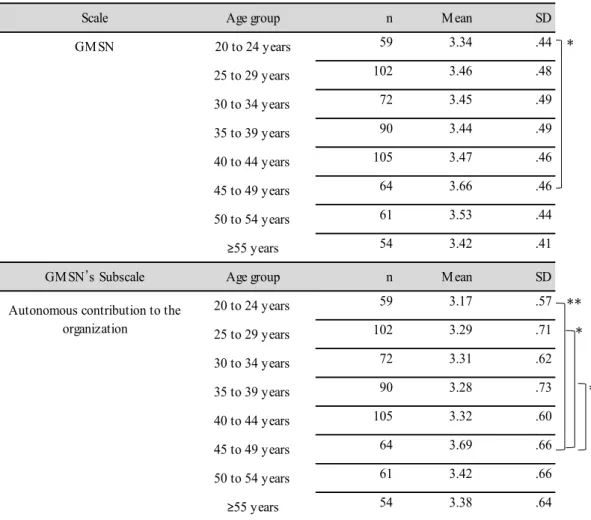
4. Relationship between participant age and GMSN scores
“Total GMSN score” and “autonomous contribution to the organization” differed significantly between age groups. The 45–49 years age group showed the highest total GMSN score, which differed significantly from that observed for the 20–24 years age group, which showed the lowest total GMSN score. Furthermore, the score for “autonomous contribution to the organization” was highest in the 45–49 years age group, which differed significantly from the scores observed in the 20–24, 25–29, and 35–39 years age groups. No significant difference was observed between the other three subscales of GMSN and the age groups (Table 5).
Discussion
We believe that it is important to undertake subjective and continuous evaluation as to whether nurses
progress positively toward their own growth. This study examined the difference between age groups by confirming the reliability and validity of the scale, so that nurses would comprehensively understand the state of their growth motivation. It has been found that there is a weak correlation between age and job satisfaction52). Job satisfaction is a concept which is also related to professional growth. Additionally, certain researchers have pointed out that older employees seek sufficiently challenging and fulfilling tasks to maintain their motivation53). In other words, older employees who maintain motivation for work at a high level may find their tasks sufficiently challenging and be satisfied with their job. Findings from this study suggest that examining the relationship between changes in nurses using age and their growth motivation may help understand their continuous growth, and facilitate further growth.
1.Participant characteristics
In an investigation conducted by the Ministry of Health, Labour and Welfare54), the proportions of men and women working as nurses were 7.8% and 92.2% respectively. The age group composition showed an M-shaped curve, starting from 8.5% of those in the 20–24 age group, dipping slightly in the 30–34 years age group (11.5%), reaching a peak in the 40–44 years age group (15.1%), and decreasing thereafter. Therefore, the male-to-female ratio and the age composition characteristics were in almost complete agreement with the composition of nurses nationwide.
2.Construct validity and internal consistency
The results of exploratory factor analysis of the GMSN, Item 9 “I consider what I fail to do as my own problem that I will address in the future” was the only item that was extracted as a sub-item of
“personal readiness and abundance of work environment resources,” rather than the expected “goals originating from regret.” All other items extracted were categorized into their expected factors, and we confirmed the four-factor structure of the scale. Furthermore, each factor consisted of a cognitive item and its corresponding behavioral item. Item 9 could have been extracted as a part of motivation driven by personal readiness that was cultivated as nursing education up to a certain point, rather than motivation driven by regret. Furthermore, rather than classification of the eight cognitive and behavioral dimensions into independent factors, each factor contained pairs of cognitive and behavioral items. According to the definition of Personal Growth Initiative by Robitschek7), PGI refers to the capabilities of individuals who work toward self-improvement which include both cognitive and behavioral capabilities. Behavioral capabilities supplement cognitive capabilities, and thereby lead to changes in various growth domains. Cognition and behavior are the sequential factors of motivation for growth, and are inseparable from each other. The growth motivation scale developed in this study was based on the growth experiences of individual nurses. The cognitive and behavioral items of the scale were developed in the form of pairs with reference to the experiences of growth in each aspect.
Therefore, it can be considered that compared to generic scale items, those for the process of shifts from cognition to behavior have clearer and stronger linkages between each other. This may explain
why items for cognition were extracted together with corresponding items for behavior, instead of them being extracted separately from each other.
Cronbach’s αs for the overall scale for each factor exceeded 0.74, and there was moderate level of correlation between the subscales, ranging between 0.44 and 0.63. Based on these observations, we believe that distinguishable subscales exist independently in this scale, while the internal consistency of the scale is sufficiently maintained.
The path coefficients of the model created using structural equation modeling were all significant, and the root mean square error of approximation was 0.08. Based on a criterion whereby a coefficient of <0.08 is deemed a reasonable error approximation55) and comprehensive judgment involving other criteria, we concluded that the scale fell within a tolerable range. Based on the above, we are able to confirm a certain level of construct validity for the scale in this study.
3.Verification of coexistence validity
Examination of correlations between the 4 GMSN subscales and 4 MWM subscales showed a weak but significant correlation (0.18) between “self-adjustment with awareness of others” in the GMSN and “competition-oriented” in the MWM. The MWM subscale most strongly correlated with the “self- adjustment with awareness of others,” the GMSN subscale was “cooperation-oriented,” showing a correlation coefficient of 0.60. A study conducted by Ikeda and Morinaga38) showed that the
“competition-oriented” MWM subscale score was lower in nurses relative to that observed in system
engineers. In addition, nurses showed the highest score for cooperation and the lowest score for competition in Ikeda and Morinaga’s38) study. The results were similar in the current study and could be considered to show that nurses place importance on cooperating with others. Moreover, because
“self-adjustment with awareness of others” involves motivating aspects that deepen introspection and consideration for others, it was only weakly correlated with the “competition-oriented” MWM subscale, which is associated with competing with others and wanting to be superior. Furthermore, Yamagishi56) stated, “We exist as individuals, and at the same time live in relationships with others.”
For nurses who work together in teams, engaging in other-directed behaviors such as “self-adjustment with awareness of others” is an important skill in working harmoniously in teams and completing work smoothly, which explains the high correlation of this factor with the “cooperation-oriented” MWM subscale.
The strong correlations between “autonomous contribution to the organization” and the “learning- oriented” and “accomplishment-oriented” MWM subscales could be explained by the fact that
“autonomous contribution to the organization” is a form of motivation for autonomous learning and the desire to contribute to the organization and is therefore closely related to the “learning-oriented”
subscale, whereby nurses learn on their own, and “accomplishment-oriented” subscale whereby they endeavor to achieve challenges. Moreover, “personal readiness and abundance of work environment resources” was strongly correlated with the “learning-oriented” subscale, showing a coefficient of 0.62.
A study conducted by Takahashi et al.57) showed that learning needs tended to be high in work environments that provided learning support for nurses, which highlighted the importance of a workplace environment that promotes willingness to learn. “Personal readiness and abundance of work environment resources” is the motivation that arises from nurses’ interest in nursing science and people and working in an organizational environment providing support to individual nurses; this was ultimately why it was correlated with the “learning-oriented” subscale. Our results were consistent with those of previous studies, and we have confirmed the concurrent validity of GMSN. The GMSN developed in this study is an effective motivational scale with multiple aspects similar to the MWM.
In addition, it is capable of measuring four aspects of individual motivational states and could be used to comprehensively judge the dynamic changes of growth.
4. Relationship between participant age and the GMSN
The GMSN overall and subscale scores were highest in the 45–49 years age group and lowest in the 20–24 years age group. Therefore, we surmised that through years of experience, nurses’ growth elevates higher-order motivation such as “autonomous contribution to the organization” and leads to overall maturity. A study conducted by Lim and Yoneyama58) to examine career development in nurses showed that higher numbers of years of experience as a nurse were associated with higher levels of maturity composed of aspects such as becoming established as a professional and relationships in the workplace with colleagues, which is similar to the current results. The present study shows that nurses’
GMSN scores tend to increase with age, suggesting that it measures maturity in new and experienced nurses. However, scores tend to reduce gradually after the age of 50 years. In the latter stages of the career cycle Schein59) suggests that while using their own skills and talents for the organization, individuals tend to retire from power and responsibility, and centrally shift to more advisory roles for junior staff. At such ages, individuals also tend to accept new roles because of a decline in ability and motivation. The author suggested that the changes in roles that take place with age and maturity tend to reduce the willingness to grow.
5. Limitations of the study and future challenges
As this study involved nurses affiliated with hospitals that had been certified for functional evaluation, sampling bias could have occurred. In addition, although the scale developed in the study had a factor structure that almost satisfied the hypothetical structural model, and the content could be evaluated in terms of reliability and validity, further investigation is required to confirm stability. As the scale was created based on the assumption that it can be used at all ages, it is expected that it will be possible to use it regularly to measure changes in individuals.
The GMSN comprises items that mainly evaluate the intrinsic motivation of nurses. However, nurses can develop intrinsic motivation when they experience external factors (incentives) such as complaints and negative feedback from other nurses and patients. In such situations, nurses may perceive external incentives as issues internal to them, reflect on themselves, and overcome a sense of regret. Future
studies would need to also examine what kind of external factors can increase the intrinsic motivation of nurses and lead to their growth.
Additionally, the GMSN was designed with the expectation that it would be used by staff nurses. It has been pointed out that studies on motivation for work need to navigate between various determinants and potential interventions60) to identify the factors that influence the GMSN. It is necessary to compare nurses’ marital status, department, and other characteristics and to examine the difference in cultural aspects, education systems, and details of work between participants taking into account the possibility that the GMSN may be used regularly. If it is possible to confirm the stability of the scale and score tendencies resulting from nurses’ characteristics, it could be possible to inform support of career development and continuing education that is more suited to individual motivation.
6.Conclusions
We created the GMSN using 30 items deduced from the results of a qualitative study and verified its reliability and validity. In the factor analysis, we extracted 24 items belonging to the following four factors: “autonomous contribution to the organization,” “personal readiness and abundance of work environment resources,” “self-adjustment with awareness of others” and “goals originating from regret.” Cronbach’s αs for the scale maintained high levels of reliability. Examination of coexistence validity identified significant correlations between the GMSN and the MWM scale. Furthermore, the hypothetical structural model was verified, and the GMSN was considered good in terms of both
reliability and validity.
Acknowledgements
We thank the 18 hospitals for assisting us in recruiting for this study, the nurses who completed the survey forms, and the four specialist nursing managers who evaluated the internal validity of items.
References
1)Berg JA, Hicks RW and Roberts ME: Professional growth and development: A lifetime endeavor. J Am Assoc Nurse Pract. 29(8): 429-433, 2017.
2)Sandehang PM, Hariyati RTS and Rachmawati IN: Nurse career mapping: A qualitative case study of a new hospital. BMC Nursing. 18:1-9, 2019.
3)Tedeschi RG and Calhoun LG: Posttraumatic Growth: Conceptual Foundations and Empirical Evidence. Psychol Inq. 15(1):1-18, 2004.
4)Beck CT and Casavant S: Vicarious Posttraumatic Growth in NICU Nurses. Adv Neonatal Care.
20(4):324-332, 2020.
5)Goldblatt H: Caring for abused women: impact on nurses' professional and personal life experiences.
J Adv Nurs. 65(8):1645-1654, 2009.
6)Liao J, Ma X, Gao B, Zhang M, Zhang Y, Liu M, Li, X: Psychological status of nursing survivors in China and its associated factors: 6 years after the 2008 Sichuan earthquake. Neuropsychiatr Dis Treat. 15:2301-2311, 2019.
7)Robitschek C: Personal growth initiative: The construct and its measure. Meas Eval Couns Dev.
30(4):183-198, 1998.
8)Robitschek C, Ashton MW, Spering CC, Geiger N, Byers D, Schotts GC, Thoen, M. A: Development and psychometric evaluation of the Personal Growth Initiative Scale-II. J Couns Psychol. 59(2):274- 287, 2012.
9)Robitschek C: Further validation of the personal growth initiative scale. Meas Eval Couns Dev.
31(4):197-210, 1999.
10)Bhattacharya A and Mehrotra S: Personal Growth Initiative Scale: How does it Perform in Indian Youth Samples? Journal of the Indian Academy of Applied Psychology. 40(1):121-128, 2014 11)Misener TR and Cox DL: Development of the Misener Nurse Practitioner Job Satisfaction Scale.
J Nurs Meas. 9(1):91-108, 2001.
12)Rahimaghaee F, Nayeri ND and Mohammadi E: Managers' roles in the professional growth of Iranian clinical nurses. Nurs Health Sci.12(4):470-476, 2010.
13)O'Keeffe AP, Corry M and Moser DK: Measuring job satisfaction of advanced nurse practitioners and advanced midwife practitioners in the Republic of Ireland: a survey. J Nurs Manag.23(1):107- 117, 2015.
14)García-Sierra R and Fernández-Castro J: Relationships between leadership, structural empowerment, and engagement in nurses. J Adv Nurs. 74(12):2809-2819, 2018.
15) Mizutani N, Hayashi T and Simizu F: Factor to influence a change of organizational Affective commitment in competent nurses. MIE Nursing Journal. 17(1): 53–64,2015. (in Japanese)
16)Barkimer J: Clinical Growth: An Evolutionary Concept Analysis. ANS Adv Nurs Sci.39(3):E28- 39, 2016.
17) Dewey J : Experience and education. 1st ed. pp1-68, The Macmillan Company New York, 1954 (copyright 1938).
18)Parolisi T: Experiences of graduates in Massachusetts of the United States from a RN-to-BSN program. Int J Nurs Sci. 7(2):206-213, 2020.
19)Tanaka I, Higa H and Yamada K: The growth process of new graduate nurses in nursing practice.
The Journal of the Nursing Society of University of Toyama. 15(1): 1–16, 2015. (in Japanese) 20)Pierson MA, Liggett C and Moore KS: Twenty years of experience with a clinical ladder: a tool
for professional growth, evidence-based practice, recruitment, and retention. J Contin Educ Nurs.
41(1): 33-40, 2010.
21)Jones WJ, Jenkins J and Johnson JA: Clinical career ladder development in nursing: concepts and issues. J Health Hum Adm. 10(4):361-377, 1988.
22)Benner P: From Novice to Expert. Am J Nurs. 82(3):402-407, 1982.
23)Buchan J: Evaluating the benefits of a clinical ladder for nursing staff: an international review.
International journal of nursing studies. 36(2):137-144, 1999.
24)Ko YK and Yu S: Clinical ladder program implementation: a project guide. J Nurs Adm.
44(11):612-616, 2014.
25) Young PT: Motivation, In Deutsch A (chief ed) : The Encyclopedia of Mental Health Volume Ⅳ.
1st ed. pp.1256-1266, Franklin Watts. New York, 1963.
26)Barbuto Jr JE and Scholl RW: Motivation sources inventory: Development and validation of new scales to measure an integrative taxonomy of motivation. Psychological Reports. 82(3 PART 1):1011- 1022, 1998.
27)Abu Yahya O, Ismaile S, Allari RS and Hammoudi BM: Correlates of nurses' motivation and their demographic characteristics. Nurs Forum. 54(1):7-15, 2019.
28)Dörnyei Z, Ibrahim Z and Muir C: ‘Directed motivational currents’: Regulating complex dynamic systems through motivational surges. Dörnyei Z et.al.(ed): Motivational Dynamics in Language Learning. pp95-105, UK. 2014.
29)Edgar L: Nurses' motivation and its relationship to the characteristics of nursing care delivery systems: a test of the job characteristics model. Can J Nur Leadersh. 12(1):14-22, 1999.
30)Lohmann J, Souares A, Tiendrebéogo J, Houlfort N, Robyn PJ, Somda SMA and De Allegri, M:
Measuring health workers' motivation composition: Validation of a scale based on Self- Determination Theory in Burkina Faso. Hum Resour Health. 15(1):1-12, 2017.
31)Brewer CS, Kovner CT, Greene W and Cheng Y: Predictors of RNs' intent to work and work
decisions 1 year later in a U.S. national sample. Int J Nurs Stud.46(7):940-56, 2009.
32)Battistelli A, Galletta M, Portoghese I and Vandenberghe C: Mindsets of commitment and motivation: Interrelationships and contribution to work outcomes. J Psychol. 147(1):17-48, 2013.
33)Hackman JR and Oldham GR: Development of the Job Diagnostic Survey. J Appl Psychol. 60(2):
159-170, 1975.
34)van den Berg TIJ, Vrijhoef HJM, Tummers G, Landeweerd JA and van Merode GG: The work setting of diabetes nursing specialists in the Netherlands: A questionnaire survey. Int J Nurs Stud.
45(10):1422-1432, 2008.
35)Warr P, Cook JD and Wall TD: Scales for the measurement of some work attitudes and aspects of psychological well-being. Journal of Occupational Psychology. 52(2):129-148, 1979.
36)Toode K, Routasalo P, Helminen M and Suominen T: Hospital nurses' work motivation. Scand J Caring Sci. 29(2): 248-257, 2015.
37)Gagné M, Forest J, Gilbert MH, Aubé C, Morin E and Malorni A: The motivation at work scale:
Validation evidence in two languages. Educ Psychol Measur. 70(4):628-646, 2010.
38) Ikeda H and Morinaga Y: Developing a measure of multi-faceted work motivations in Japanese organizations. Japanese Association of Industrial/Organizational Psychology Journal. 30(2): 171–
186, 2017. (in Japanese)
39)Engin E and Cam O: Validity and reliability study of the Turkish psychiatric nurses of job
motivation scale. J Psychiatr Ment Health Nurs. 16(5):462-72, 2009.
40)Nishimura N, Dei R, Yamamoto C, Yamaguchi M and Nakajima K: Development of a work motivation scale for nurses. Bulletin of Social Medicine. 34(2):27-34, 2017. (in Japanese)
41)Toode K, Routasalo P and Suominen T: Work motivation of nurses: a literature review. Int J Nurs Stud. 48(2):246-57, 2011.
42)Utriainen K, Kyngäs H and Nikkilä J: Well-being at work among ageing hospital nurses in Northern Finland: a grounded theory study. Int J Circumpolar Health. 68(2):145-157, 2009.
43)Arata Y, Nakao H and Hamada Y: The Structure of Motivation for Growth of Clinical Nurses.
Journal of Japan Academy of Nursing Science. 39:29-37, 2019. (in Japanese)
44) Imai T and Takase M: Support system in the workplace to improve the quality of nursing practice by newly graduated nurses: Analyzing data collected through interviews with nursing managers, using the KJ method. Japanese Journal of Occupational Medicine and Traumatology. 65 (3): 111–
117, 2017. (in Japanese)
45)Vishnevsky T, Quinlan MM, Kilmer RP, Cann A and Danhauer SC: "The Keepers of Stories":
Personal Growth and Wisdom Among Oncology Nurses. J Holist Nurs. 33(4):326-344, 2015.
46)Bauer JJ, Park SW, Montoya RM and Wayment HA: Growth Motivation Toward Two Paths of Eudaimonic Self-Development. J Happiness Stud. 16(1):185-210, 2014.
47)Lynn MR: Determination and quantification of content validity. Nurs Res. 35(6) : 382–385, 1986.
48)Polit DF, Beck CT, and Owen SV: Is the CVI an acceptable indicator of content validity?
Appraisal and recommendations. Res Nurs Health. 30(4): 459–467, 2007.
49)Waltz CF, Strickland OL and Lenz ER: Measurement in nursing and health research (4th edition) Springer Publishing Company, USA, 2010.
50)Japanese Nursing Association: 2017 Nursing related statistics, nursing staff by prefectures,
comparison by population. Available from https://www.nurse.or.jp/home/statistics/pdf/toukei06.pdf (in Japanese)
51) Japan Council for Quality Health Care: 2020 Provision of information on the results of evaluating hospital functions. Available from http://www.report.jcqhc.or.jp/ (Accessed January 16, 2020; in Japanese)
52)O’Brin GE and Dorling P: Age and Job Satisfaction. Aust Psychol.16(1): 49-61,1981.
53)Boumans NP, de Jong AH and Janssen SM: Age-differences in work motivation and job satisfaction.
The influence of age on the relationships between work characteristics and workers' outcomes. Int J Aging Hum Dev. 73(4):331-350, 2011.
54) Ministry of Health, Labour and Welfare: 2018 Summary of reports of sanitation administration (healthcare workers). Available from https://www.mhlw.go.jp/toukei/saikin/hw/eisei/18/dl/kekka1.pdf
(in Japanese)
55) Browne MW and Cudeck R: Alternative ways of assessing model fit, In Bollen KA and Long JS
(eds.): Testing structural equation models. 1st ed. pp. 136–162, SAGE publications London, 1993.
56) Yamagishi A: Self cognition of college students: From the viewpoint of “individual self" and “self in relation to others.” The Journal of Juntendo Medical College of Nursing. 2: 64–73, 1991. (in Japanese)
57) Takahashi K, Kiyomura N, Kajiwara E and Itou N: A study on the personal/environmental factors related to the actual conditions of the learning needs of clinical nurses. Journal of Japan Academy of Nursing Science. 32 (2): 34–43, 2012. (in Japanese)
58) Lim Y and Yoneyama K : Career formation in nurses and factors to effect on it. Journal of Japan Academy of Nursing Science, 28(1): 12–20, 2008. (in Japanese)
59)Schein, EH : Career Dynamics - Career is the human way of life and expression throughout life, (T. Nimura, K. Miyoshi Trans). Hakuto Shobo, Tokyo.1991 (Original work published 1978). (in Japanese)
60)Franco LM, Bennett S, Kanfer R and Stubblebine P: Determinants and consequences of health worker motivation in hospitals in Jordan and Georgia. Soc Sci Med. 58(2):343-355, 2004.
和文抄録
看護師の成長動機づけ尺度開発へ向けた信頼性と妥当性の検証
1)九州大学大学院医学系学府保健学専攻 2)久留米大学医学部看護学科
3)久留米大学バイオ統計センター 新裕紀子1),2),中尾久子1),角間辰之3)
【目的】看護師の成長動機づけ尺度開発へ向けて,尺度の信頼性・妥当性の検証を行うことを目
的とした.
【方法】質的研究結果から導き出された30項目からなる尺度を作成し,全国の病院18施設に勤
務する臨床看護師を対象に自記式質問紙調査を実施した.最終的に607部の質問紙を分析の
対象とした.
【結果】因子分析の結果,24項目4因子が抽出され,それぞれ「自律的組織貢献」「個人のレディ ネスと職場環境資源の豊かさ」「他者を意識した自己調整」「後悔から生じる目標」と命名した.
cronbach’s alphaはそれぞれ.90, .82, .81, .74で,尺度全体としては.92であった.併存妥当性の検 討では「多側面ワークモチベーション尺度」との間に有意な相関関係が認められた.
【結論】看護師の成長動機づけ尺度は,信頼性・妥当性ともに良好であると判断し,看護師の成長
への動機づけの状態を測るための有効な尺度となりうると考えられる.今後は再テストを試み,尺度
の安定性を検討することが必要である.
【キーワード】 成長,動機づけ,看護師,尺度開発
Figure 1. Hypothetical Structural Model of Growth Motivation Scale for Nurses Layer 4 Pride in nursing and a desire to
contribute to others
Fusion of autonomy and cooperation for work
Layer 3 Interest in one's ideal self, through relationships with others
Self-inquiry with consideration for others
Layer 2 Awareness of one's own immaturity
in the profession Efforts to overcome immaturity
Layer 1 The basis for getting to work as a
nurse Approach to the work of nursing
(Cognitive) (Behavioral)
Figure 2. Procedure for distributing questionnaires Method of distribution: Stratified randam sampling Division of the distribution areas to 8 districts and regions
Determine the number of hospitals from which to request participation by calculating the proportion of nurses in 8 districts and regions
Extraction of hospitals to request
Classification of hospitals from the list of certified hospitals into two according to scale and function, followed by random selection of the equal number of hospitals belonging to each category to reach the number of hospitals assigned for the 8 districts and regions
Requested participation from 70 hospitals
Research authorization from 18 hospitals
Distribution (1,481 copies)
635 questionnaires recovered, 607 questionnaires with effective responses
Figure 3. Goodness of fit indices for the structural model
Abbreviations: GFI = goodness-of-fit index; AGFI = adjusted goodness-of-fit index;
CFI = comparative fit index; RMSEA = root mean square error of approximation
.60
Item 25
.78
.56
.61 .75 Item 26
.61
.78 Item 27
.83 .69
.79 Item 28
.62
.76 Item 29
.58
.78 Item 30
.28 .53 Item 17
.47
.54 .69 Item 18
.29
.53 Item 19
.64 .41
.74 Item 22
.54
.70 Item 23
.48
.73 Item 24
.32
Item 10
.57 .13
.55 Item 11
.36 .44
.66 Item 12
.40 .63 Item 13
.72 .52
Item 14
.28
.74 Item 2
.47 .53 Item 3
.69 .26
Item 4
.51
.38
.62 Item 6
.43
.66 Item 7
.75 .56
Item 8
.68
.47
Item 9
GFI: .84 AGFI: .81 CFI: .84 RMSEA: .08 Goals originating from regret
Personal readiness and abundance of work environment resources Autonomous contribution to
the organization
Self-adjustment with awareness of others
e
e
e
e
e
e
e
e
e
e
e
e
e
e
e
e
e
e
e
e
e
e
e
e e
e
e
Table 1. Base attributes
n %
Sex (n = 607) Male 48 7.9
Female 559 92.1
Age group (n = 607) 20 to 24 years 59 9.7
25 to 29 years 102 16.8
30 to 34 years 72 11.9
35 to 39 years 90 14.8
40 to 44 years 105 17.3
45 to 49 years 64 10.5
50 to 54 years 61 10.0
≥55 years 54 8.9
Mean Standard deviation Number of years of clinical experience (n = 604) 14.9 10.0
Table 2. Results of factor analysis of the growth motivation scale for nurses (n=607)
1 2 3 4
Factor 1 Autonomous contribution to the organization (Mean = 3.35, Standard Deviation = .66)
㉚ My own intervention contributes to the building of good patient-
medical practitioner relationships (beh) .84 .02 -.10 .02 3.19 .77
㉙ I am actively seeking places where I can use my strengths to
contribute to patients and people in the workplace. (beh) .80 .04 -.08 .07 3.16 .83
㉘ I continue to practice nursing with pride at being a nurse (beh) .73 .14 .07 -.08 3.51 .86
㉕ I take pride in continuing the valuable work of nursing (cog) .66 .02 .15 -.03 3.40 .86
㉗ I am aware of the importance of my role in maintaining a good
relationship between the patient and the medical practitioner (cog) .57 .08 .27 -.09 3.48 .75
㉖ I want to improve my ability and utilize it for the people and
organizations around me (cog) .51 .17 .12 .04 3.34 .79
Factor 2 Personal readiness and abundance of work environment resources
(Mean = 3.44, Standard Deviation = .54)
⑧ I'm positively working in my current work environment (beh) .11 .74 -.08 -.02 3.41 .77
⑦ I educate myself on things that I am interested in at work (beh) -.08 .68 -.08 .15 3.49 .74
③ I'm interested in new knowledge about medicine and nursing, or
things I don't know (cog) -.01 .63 -.06 .19 3.63 .77
⑨ I consider what I fail to do as my own problem that I will address in
the future (cog) -.14 .57 .12 .26 3.57 .69
⑥ I am actively involved with patients, their families, and people at
work (beh) .19 .52 -.04 -.02 3.34 .72
④ I think I am in a fulfilling environment for thinking about my work
and career (cog) .15 .50 .02 -.17 3.06 .88
② I find it interesting to interact with people (cog) .19 .46 .02 -.09 3.57 .84 Factor 3 Self-adjustment with awareness of others
(Mean = 3.71, Standard Deviation = .55)
㉓ I make adjustments to myself by paying attention to my actions and
correcting the bad side (beh) .04 -.17 .73 .18 3.52 .71
⑱ I pay attention to my own behavior by looking at the behavior of
other nurses (cog) -.06 .23 .68 -.09 3.79 .71
⑰ I strongly feel that I am able to work thanks to the support of other
nurses and other professionals (cog) -.08 .27 .61 -.26 3.97 .84
㉒ I always treat other nurses and other professionals with great care
(beh) .09 -.18 .59 .19 3.65 .75
⑲ I also pay attention to my behavior through illness and death of
patients (cog) .01 -.06 .58 .01 3.93 .83
㉔ As a nurse, I try to be humble in my words and behavior while
appreciating my daily life (beh) .27 -.17 .52 .12 3.38 .81
Factor 4 Goals originating from regret (Mean = 3.37, Standard Deviation = .56)
⑬ I always try to overcome my immaturity at work with an "I won't
give in!" spirit (beh) .18 -.03 -.17 .76 2.94 .86
⑩ I become frustrated and full of regret about things that I can't do well
at work (cog) .03 .02 -.05 .67 3.31 .89
⑫ For each failed experience, I investigate the cause and take advantage
of it for the next task (beh) -.07 .23 .17 .45 3.53 .68
⑪ I am never 100% satisfied with the nursing work I do (cog) -.22 -.01 .20 .43 3.49 .83
⑭ I always engage in nursing work with the mindset to do better next
time (beh) .10 .18 .16 .41 3.57 .70
Total 3.47 .47 .92
.81
.74
Abbreviations: cog = cognitive; beh = behavioral
Items Factor
Cronbach's α
.90
.82 Mean Standard
Deviation
Table 3. Correlation of subscales in the growth motivation scale for nurses Personal readiness and
abundance of work environment resources
Self-adjustment with awareness of others
Goals originating from regret Autonomous contribution to the
organization
.63** .61** .46**
Personal readiness and abundance
of work environment resources ― .48** .48**
Self-adjustment with awareness
of others ― ― .44**
**<.01
Table 4. Correlation of the growth motivation scale for nurses with the Multi-faceted Work Motivation scale and subscales
Competition-oriented Cooperation-oriented Learning-oriented Accomplishment-oriented MWM (M = 2.42, SD = .75) (M = 3.37, SD = .66) (M = 3.15, SD = .65) (M = 3.31, SD = .63) (M = 3.06, SD = .54)
Autonomous contribution to the organization .41** .57** .64** .60** .69**
Personal readiness and abundance of work environment resources
.25** .46** .62** .51** .57**
Self-adjustment with awareness of others .18** .60** .48** .54** .54**
Goals originating from regret .42** .36** .49** .48** .56**
GMSN .39** .63** .71** .67** .74**
**<.01
GMSN = growth motivation scale for nurses; MWM = Multi-faceted Work Motivation scale
Table 5. Relationship between subject age and growth motivation scale for nurses
Age group n Mean SD
20 to 24 years 59 3.34 .44 *
25 to 29 years 102 3.46 .48
30 to 34 years 72 3.45 .49
35 to 39 years 90 3.44 .49
40 to 44 years 105 3.47 .46
45 to 49 years 64 3.66 .46
50 to 54 years 61 3.53 .44
≥55 years 54 3.42 .41
Age group n Mean SD
20 to 24 years 59 3.17 .57 **
25 to 29 years 102 3.29 .71 *
30 to 34 years 72 3.31 .62
35 to 39 years 90 3.28 .73 *
40 to 44 years 105 3.32 .60
45 to 49 years 64 3.69 .66
50 to 54 years 61 3.42 .66
≥55 years 54 3.38 .64
*<.05 **<.01
Abbreviations: GMSN = growth motivation scale for nurses
Scale GMSN
GMSN's Subscale Autonomous contribution to the
organization