Hepatocellular carcinoma accompanied by hypersplenism : five cases of simultaneous hepatectomy and laparoscopic
splenectomy
Yasuyuki Nakata, Seiji Haji, Mithuo Yamasaki, Takuya Nakai and
Hajime Ishikawa,
Yoshihumi
Department of Surgery, Kinki University
Osakasayama, Osaka,
Takeyama
Faculuty of
589-8511, Japan
Takeo
Medicine,
Yasuda,
Abstract
Background : We performed simultaneous he- patectomy and laparoscopic splenectomy in a patient with hepatocellular carcinoma ac-
companied by a reduced platelet count caused by hypersplenism.
Methods : We retrospectively studied 5 cases of hepatectomy performed immediately after lapar- oscopic splenectomy at our hospital after July 2006, and evaluated the intraoperative blood loss, need for transfusion during surgery, pos-
toperative complications, and postoperative hos- pital stay. Hematological analysis included the
white blood cell count (WBC), platelet count (Plt), serum alanine transaminase (ALT), total serum bilirubin (T-Bil), prothrombin time (PT)%, and serum albumin (Alb). Analysis was performed on postoperative days (POD) 7, 14, 30,
and 60.
Results : The results showed intraoperative
Introduction
In Japan, the majority of hepatocellular car- cinoma cases are accompanied by chronic viral hepatitis and cirrhosis. When cirrhosis is pres- ent, hypersplenism causes secondary throm- bocytopenia, often making interferon treatment of hepatitis and chemotherapy after the recur- rence of hepatocellular carcinoma difficult. In recent years, many institutions perform splenectomy because of its efficacy in patients with cirrhosis accompanied by throm-
blood loss of 891+523.2 ml (mean+ SD, 35-2, 199), blood transfusion in 3 cases (60%), no complications in all cases, and a postoperative hospital stay of 11.8 (11-13) days. Compared with preoperative levels, WBC and Plt were significantly higher on POD 7, 14, 30, and 60.
while ALT and T-Bil were significantly lower on POD 30. Alb levels were low on all postoper- ative days compared with preoperative levels.
There were no significant changes in PT%.
Conclusions : It was safe to conduct he- patectomy simultaneously with laparoscopic splenectomy. No significant liver dysfunction occurred postoperatively, suggesting a potential reduction in the patient burden.
Key words : patocellular splenectomy
hypersplenism, carcinoma,
cirrhosis, he- hepatectomy,
bocytopenia. When hepatocellular carcinoma and thrombocytopenia due to cirrhosis are pres- ent, splenectomy or partial splenic embolization (PSE) is performed to increase the platelet count prior to hepatectomy or percutaneous radiofre- quency ablation. Because of safety concerns, a relatively small number of simultaneous splenectomy and hepatectomy procedures have been performed, most of which were done in open surgery,7-1° and only a few cases involved laparoscopy.11 The safety of laparoscopic splenectomy has improved in recent years, and
Received May 10, 2011 ; Accepted June 2, 2011
the procedure has fewer complications than open abdominal surgery. With hand-assisted laparos- copy, it is possible to reduce the duration of surgery and intraoperative blood loss. For these reasons, in patients with hepatocellular car- cinoma accompanied by thrombocytopenia, we performed hepatectomy immediately after lapar- oscopic splenectomy. Here, we present a report of 5 cases.
Materials and Methods
Clinical cases and evaluation items
Since July 2006, we have performed simultane- ous hepatectomy and splenectomy by laparos- copy in 5 cases, and have evaluated the efficacy of the procedure as described below. At our institution, the indication for splenectomy is a platelet count of <7>< 10-4 in a patient who requires interferon treatment because of a high hepatitis viral load or who is a candidate for hepatectomy due to the presence of hepatocel- lular carcinoma. Study items were intraoper- ative blood loss, presence or absence of blood transfusion during surgery, postoperative com- plications, and postoperative hospital stay.
Hematological analysis included the white blood cell count (WBC), platelet count (Plt), serum alanine transaminase (ALT), total serum bilir- ubin (T-Bil), prothrombin time (PT)%, and serum albumin (Alb). Analysis was performed on postoperative days (POD) 7, 14, 30, and 60.
Surgical technique
In all cases, 20 units of platelets were adminis- tered before surgery, and splenectomy was perfor- med using laparoscopy on a patient in the semir- ecumbent position to the right. An incision (7 cm) along the midline was made to mount the GelPort® (Applied Medical, CA, USA). A small opening was made in the lower left umbili- cal area for the insertion of a camera, and two openings were made below the left rib cage and in the left abdominal area for a 12-mm port (Fig.
1). We observed the abdominal cavity to ensure the absence of splenculus, opened the omental bursa on the left and separated the gastrosplenic ligament, and made an incision in the proximity of the upper splenic pole. We dissected the splenocolic ligament without processing the short gastric vessels near the upper splenic pole, because they are potential bleeding points.
These blood vessels were transected after the spleen was separated from the retroperitoneum
Solenectomy Open abdominal surgery
Rigfitsemirerun-bent position Supine position
—skin intisbn :port site
Fig. 1 Hepatectomy performed through an extended inci- sion in the supine position after laparoscopic
splenectomy in the right semirecumbent position. In
case 5, liver mobilization was performed by laparos-
copy without extending the original incision.
and mobility improved. Tissues were separated using an ultrasonic coagulation cutting device (Harmonic Scalpel®, Ethicon Endo-Surgery Inc., Tokyo, Japan), LigaSure® (Tyco Healthcare Japan, Tokyo, Japan), and a hook electrocautery probe. The splenic hilum was dissected using a stapler in all cases, and the spleen was placed in a plastic bag and enucleated through the midline incision. The patient was then placed in the supine position and the original incision was extended for hepatectomy (Fig. 1). In cases 1-4, a transverse incision to the right was made from the original incision, resulting in a final inverted L-shaped incision. In case 5, because the loca- tion of the tumor was near the lateral segment of the liver, mobilization of the liver was performed by laparoscopy and resection was made through the original 7-cm incision. In all cases of he- patectomy, the Pringle method was used to per- form inflow occlusion. The hepatic capsule was resected with an ultrasonic coagulation cutting device, and the hepatic parenchyma was resected with a cavitron ultrasonic surgical aspirator and a dissecting sealer (TissueLinkTM monopolar device, TissueLink Medical Inc., NH, USA). In case 1, we also performed radiofrequency abla- tion (Table 1).
Post-discharge follow-up
After discharge, blood sampling and clinical examination were performed on POD 14 and 60.
On POD 30, in addition to blood sampling, computed tomography (CT) angiography was performed to ensure the absence of portal vein thrombosis. In all cases, pneumococcal vaccine was given on POD 30.
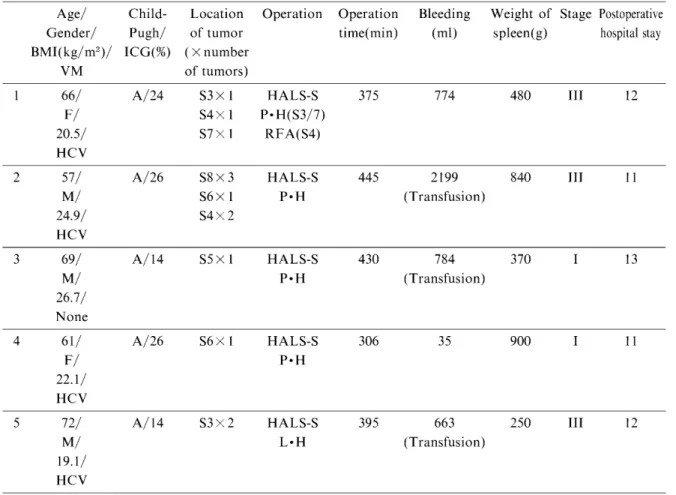
Table 1 Background and progress of patients before and after surgery.
Age/ Child- Location Gender/ Pugh/ of tumor BMI(kg/m2)/ ICG(%) ( X number
VM of tumors)
Operation Operation time(min)
Bleeding Weight of Stage Postoperative (m1) spleen(g) hospital stay
1 66/
F/
20.5/
HCV
A/24 S3 X 1 S4 X 1 S7 X 1
HALS-S P • H(S3/7)
RFA(S4)
375 774 480 TTT 12
2 57/
M/
24.9/
HCV
A/26 S8 X 3 S6 X 1 S4 X 2
HALS-S P•H
445 2199 (Transfusion)
840 III 11
3 69/
M/
26.7/
None
A/14 S5 X 1 HALS-S P•H
430 784 (Transfusion)
370 I 13
4 61/
F/
22.1/
HCV
A/26 S6 X 1 HALS-S
P•H
306 35 900 I 11
5 72/
M/
19.1/
HCV
A/14 S3 X 2 HALS-S L•H
395 663 (Transfusion)
250 ITI 12
VM : Virus Marker ; S : Couinaud's Classification of Splenectomy of Hand assisted Laparoscopic Surgery ; Radio-frequency Ablation.
the liver ; P•Hr : Partial Hepatectomy ; HALS-S : L•Hr : Lateral Segmentectomy of the Liver ; RFA :
Statistics
Statistical analysis was performed using Stu- dent's t-test. The results are expressed as the mean+ SD, and were considered significant when p< 0.05.
Results
The patients were 3 males (60%) and 2 females (40%) aged 65±4.8 (57-72) years old (Table 1).
The average body mass index was 22.66±2.512 (19.1-26.7). Four patients (80%) had chronic hepatitis C, and 1 (20%) was negative for hepati- tis infection. The Child-Pugh classification was A in all cases, and the indocyanine green clear- ance rate was 20.8 ± 5.44 (14-26)%. The average number of tumors per patient was 2.6 (1-6). A tumor was located in both lobes in 2 cases (40%), in the right lobe only in 2 cases (40%), and in the left lobe only in 1 case (20%). Surgery time was 389+48.5 (306-445) min. Blood loss was 891+
523.2 (35-2199) ml, and blood transfusion was
performed in 3 cases (60%). The weight of the spleen was 568± 241.6 (250-900) g. With regard to the degree of tumor progression, 2 patients were Stage I (40%) and 3 were Stage III (60%).
During the postoperative course of all patients, no complications were observed, and the pos- toperative hospital stay was 11.8 (11-13) days (Table 1).
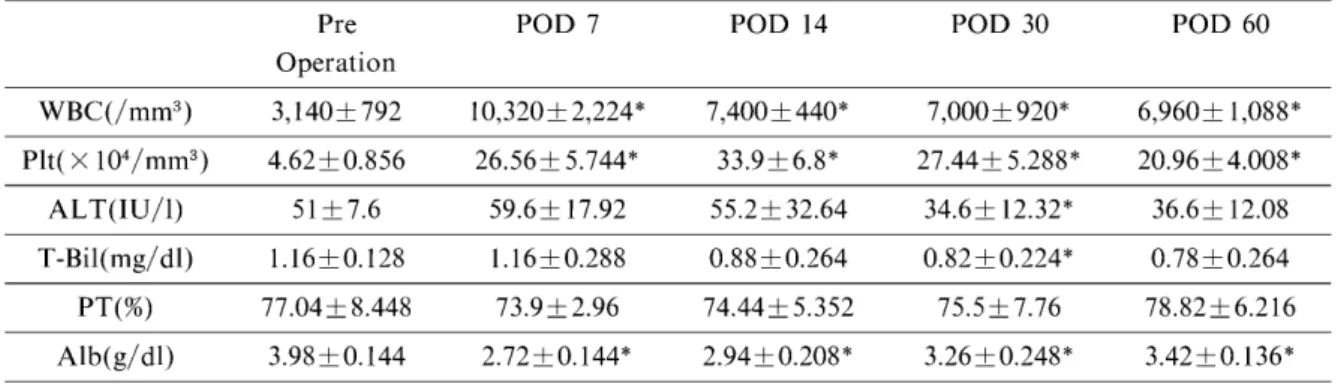
Hematology results showed that the levels of WBC and Plt were significantly higher on POD 7, 14, 30, and 60 compared with preoperative levels (Table 2). ALT levels were significantly lower on POD 30 only. Overall, T-Bil levels were lower than preoperative levels throughout the study period, attaining significance on POD 30. On POD 60, none of the patients had a T-Bil level above the preoperative level. There were no significant differences in PT% between the POD groups. Compared with preoperative levels, Alb levels were significantly lower at all measurement points. In all 5 cases, no portal vein thrombosis was detected by CT angiogra-
Table 2 Hematological analysis results (mean± SD) ; * : P < 0.05 vs . preoperative levels . Pre
Operation
POD 7 POD 14 POD 30 POD 60
WBC(/mm3) 3,140+ 792 10,320+ 2,224* 7,400+ 440* 7,000+ 920* 6,960+ 1,088*
Plt( X 104/mm3) 4.62+0.856 26.56+ 5.744* 33.9+6.8* 27.44+ 5.288* 20.96+4.008*
ALT(IU/1) 51+ 7.6 59.6+ 17.92 55.2+ 32.64 34.6+ 12.32* 36.6+ 12.08
T-Bil(mg/dl) 1.16+0.128 1.16+0.288 0.88+0.264 0.82 + 0.224* 0.78+0.264
PT(%) 77.04+ 8.448 73.9 + 2.96 74.44+ 5.352 75.5 + 7.76 78.82±6.216
Alb(g/dl) 3.98+ 0.144 2.72 + 0.144* 2.94+0.208* 3.26+0.248* 3.42 + 0.136*
phy taken on POD 30.
Discussion
This study aimed to elucidate if hepatectomy can be performed immediately following lapar- oscopic splenectomy in patients with throm- bocytopeni a due to cirrhosis. Besides splenectomy, PSE is performed to increase the platelet count and is easy to perform and less invasive than splenectomy, demonstrating its clinical efficacy.2,3 On the other hand, complica- tions such as high fever, pain, splenic abscess, bacterial peritonitis, hepatic failure, and multi- ple organ failure have been reported. Because the efficacy of PSE lasts approximately 1 year and because it is necessary to perform PSE sev- eral times to obtain its full effect, PSE is current- ly not fully supported.4'5 For this reason, we decided to perform splenectomy because of its reliable end result. In addition, because of improvements in surgical procedures and tech- niques in recent years, resection of the spleen can be achieved safely using a laparoscopic method regardless of the primary disease.L8 Although it was possible to carry out complete laparoscopic splenectomy, we decided to make an inverted L- shaped incision for hepatectomy and performed splenectomy under hand-assisted laparoscopy in all cases. Patients with cirrhosis tend to bleed easily because of an impaired coagulation capac- ity and the presence of portal hypertension that results from the development of collateral circu- lation. Therefore, splenectomy under hand-as- sisted laparoscopy is believed to be safer should manual hemostasis need to be applied to stem bleeding.
In general, splenectomy is performed prior to hepatectomy. According to a study by Shimada et al. on 6 cases of hepatocellular carcinoma in which splenectomy was performed before he-
patectomy,7 a significant increase in WBC and Plt and improvement in the Child-Pugh classifi- cation were observed. In addition, platelet trans- fusion was not necessary prior to hepatectomy, and the amount of bleeding was less compared with cases of hepatectomy without prior splenectomy.7 Our data revealed 891 ± 523.2 (35- 2,199) ml of intraoperative blood loss, 3 cases (60%) of transfusion, no postoperative complica- tions, and 11.8 (11-13) days of postoperative hospital stay. Simultaneous resection of the liver and spleen in open surgery, using the same procedures as those employed in this study, were performed in 12 cases by Takayama et al.,8 35 by Sugawara et al.,' 94 by Chen et al.," and 10 by Shimada et al.' (Table. 3). It may not be appro- priate to compare our data with theirs because of a relatively low sample number in this study ; however, considering the absence of complica- tions and the short hospital stay seen in the present study, we can conclude that the proce- dures used in this study are safe. With regard to transfusion, Chen et al. performed no transfusion in 66 of 94 cases (70.2%)."
The significant increase in WBC and Plt compared with the preoperative levels resulted from the absence of hemolysis after splenectomy.
WBC/Plt levels in previous studies were also significantly increased.7-9 Because there were no significant changes in ALT, T-Bil, and PT%
compared with preoperative levels, it is clear that the liver function is not significantly affected by the procedures used in this study.
The effect of splenectomy on the liver function has been gathering attention in recent years ; however, no consensus has been reached and further studies are needed to elucidate if similar effects can be obtained under stressful conditions such as undergoing simultaneous hepatectomy.
According to Chen et al., the 5-year tumor-free survival rate was extended in patients who under-
Table 3 The reported cases of Simultaneous simultaneous hepatectomy and splenectomy.
Number of cases
Age(Year) (mean± S.D)
Operation Bleeding
(ml)
Complication (%)
Takayame 12 54.0+ 3.0 1,223+ 153 n.d
Sugawara9) 34 58.0+ 1.0 (1) 1,156+159 50.0
Chen'°) 94 44.6+ 10.2 380+ 220 15.9
Shimoda') 10 62.5+6.3 700-6,700
(average 2,451)
n.d
Kitami" 1 63.0 840(g) 0
Own 5 65.0+ 4.8 © 891+523.2 0
n.d
Open simultaneous hepatectomy and splenectomy.
Simultaneous open hepatectomy and laparoscopic splenectomy.
Simultaneous laparoscopic hepatectomy and splenectomy.
: not description
went simultaneous hepatectomy and splenectomy compared with those who under- went hepatectomy only. Interestingly, the ratio of CD4/CD8 (subsets of T cells) increased signif- icantly,10 suggesting the possibility that the removal of the spleen enhances antitumor immu- nity.
Postoperative blood loss, pancreatic fistula, portal vein thrombosis, and overwhelming severe postsplenectomy infection are known complica- tions of splenectomy, among which portal vein thrombosis is known to affect the postoperative liver function. Portal vein thrombosis needs to be seriously considered because it reportedly occurs in 25-68.4% of patients with portal hyper- tension." Accordingly, some studies have repor- ted the use of anticoagulants immediately follow- ing surgery ; however, such treatment may increase the chance of recurrent bleeding from an excision site in the case of simultaneous liver and spleen resection. Prior to this study, we decided to abstain from postoperative anticoagulation therapy and prescribe antiplatelet drugs if throm- bosis was found on CT angiography on POD 30.
It should be noted that there is a report on extensive portal vein thrombosis following simultaneous hepatectomy and splenectomy in open surgery.12 It is necessary to further study the effect of anticoagulant therapy following simultaneous hepatectomy and splenectomy.
Hepatectomy was performed an average of 19 (7-40) days' or 33± 2 days8 after splenectomy in studies that conducted splenectomy and he- patectomy separately. The significance of simul- taneous resection is expected to be high consider- ing the potential progression of disease and
emotional distress of patients during the waiting period between surgery and the increase in medical expense on 2 separate operations.
Conclusion
We encountered 5 cases of hepatocellular car- cinoma accompanied by hypersplenism and con- ducted hepatectomy immediately following laparoscopic splenectomy. The safety of the simultaneous resection procedure was satisfac- tory, and there was no significant decrease in the liver function. Our study clearly suggests the potential alleviation of the burden and pain of patients.
Conflict of interest statement
Yasuyuki Nakata and other co-authors have no conflict of interest.
References
1. Habermalz B, Sauerland S, Decker G, Delaitre B, Gigot JF, Leandros E, Lechner K, Rhodes M, Silecchia G, Szold A, Targarona E, Torelli P, Neugebauer E (2008) Laparoscopic splenectomy : the clinical practice guidelines of the European Association for Endoscopic Surgery (EAES). Surg Endosc 22 : 821-848
2. Han MJ, Zhao HG, Ren K, Zhao DC, Xu K, Zhang XT (1997) Partial splenic embolization for hypers- plenism concomitant with or after arterial embolization of hepatocellular carcinoma in 30 patients. Cardiovasc Intervent Radiol 20: 125-127
3. Shimizu T, Tajiri T, Yoshida H, Yokomuro S, Mamada Y, Taniai N, Kawano Y, Takahashi T, Arima Y, Aramaki T, Kumazaki T (2003) Hand-assisted
laparoscopic hepatectomy after partial splenic embol- ization. Surg Endosc 17 : 1676-1679
4. Palsson B, Hallen M, Forsgerg AM, Almark A (2003) Partial splenic embolization : long-term out- come. Lengenbecks Arch Surg 387: 421-426 5. Murata K, Shiraki K, Takase I, Nakano T, Tameda
Y (1996) Long term follow-up for patients with liver cirrhosis after partial splenic embolization. Hepatogas- troenterology 43: 1212-1217
6. Konstadoulakis MM, Lagoudianakis E, Antonakis PT, Albanopoulos K, Gomatos I, Stamou KM, Lean- dros E, Manouras A (2006) Laparoscopic versus open splenectomy in patients with beta thalassemia major. J Laparoendosc Adv Surg Tech A 16 : 5-8
7. Shimada M, Hashizume M, Shirabe K, Takenaka K, Sugimachi K (2000) A new surgical strategy for cirr- hotic patients with hepatocellular carcinoma and hypersplenism. Performing a hepatectomy after a laparoscopic splenectomy. Surg Endosc 14 : 127-130 8. Takayama T, Makuuchi M, Yamazaki S, Hasegawa H (1987) A role of splenectomy in patients with he- patocellular carcinoma and hypersplenectomy in patients with hepatocellular carcinoma and hypers-
plenism as an aid to hepatectomy (in Japanese with English abstract). J Jpn surg Soc 90 : 1043-1048 9. Sugawara Y, Yamamoto J, Shimada K, Yamasaki S,
Kosuge T, Takayama T, Makuuchi M (2000) Splenectomy in Patients with Hepatocellular Car- cinoma and hypersplenism. J Am Coll Surg 190: 446 -450
10. Chen XP, Wu ZD, Huang ZY, Qiu FZ (2005) Use of hepatectomy and splenectomy to treat hepatocellular carcinoma with cirrhotic hypersplenism. Br J Surg 92 : 334-339
11. Kitami C, Kurosaki I, Yokoyama N, Kobayashi T, Hatakeyama K (2006) Hand-assisted laparoscopic par- tial hepatectomy and splenectomy for hepatocellular carcinoma and hypersplenism (in Japanese with Eng- lish abstract). J Jpn society Endosc Surg 11 : 287-291 12. Inoue S, Shiozawa S, Tsuchiya A, Kim T, Naritaka
Y, Ogawa K (2007) A Case Of Portal Vein Thrombosis After Splenectomy And Hepatectomy Successfully Treated With Thorombolytic Therapy (in Japanese with English abstract). J Jpn Surg Association 68 : 645 -648