940
A Case
of Oral
Lichen
Planus
with
Chronic
Hepatitis
C
Successfully
Treated
by Glycyrrhizin
Yumiko NAGAO'), Michio SATA2), Kyuichi TANIKAWA2)
and Tadamitsu
KAMEYAMA1)
"Department of Oral Surgery, 2'Second Department of Medicine,
Kurume University School of Medicine, Fukuoka, Japan
(Received: April 21, 1995)
(Accepted: June 8, 1995)
Key words: oral lichen planus, chronic hepatitis C, glycyrrhizin
Introduction
Oral lichen planus (OLP) is an inflammatory and intractable disease with a long course associat-ed with chronic hyperkeratosis. Although many causative factors have been mentioned1>-13>, the pathogenesis of OLP is as yet unknown and a treatment for the disease has not been established. Because of reports pointing out the relation between lichen planus and chronic liver disease, we studied the possible relation between OLP and hepatitis B virus (HBV) or hepatitis C virus (HCV) as well as liver dysfunction, and found that patients with OLP were frequently infected with HCV"). This finding implies that HCV infection by itself plays an important role in the development of OLP . We experienced a patient with chronic hepatitis C accompanied by OLP whose oral mucosal lesion was greatly improved by administration of glycyrrhizin (SNMC®) which has been widely used in treatment for liver disease. The patient is interesting for investigating the causes of OLP and therapeutics for OLP.
Case Report Patient: A 49-year-old women.
First medical examination: 23 February 1994.
Chief complaint: Pain in the oral cavity on eating or drinking.
Past history: She had acute hepatitis at the age of 30 years and was treated with therapy for chronic hepatitis non A, non B by a local doctor.
Family history: Her elder sister has chronic hepatitis. Life history: No history of smoking or drinking.
Present illness: From about November 1993 the patient has had white papular lesions from the bilateral lower gingivae to the buccal mucosae causing pain in the oral cavity on eating or drinking .
Because of enlargement of the lesions and exacerbation of subjective symptoms,the patient consulted a local medical doctor, who administrated an external drug and vitamins and observed her course. However, no improvement was seen and the patient was referred to the outpatient of oral surgery clinic.
Physical examination: Among her physical findings, characteristic observations were: reticular type of white papules on her bilateral buccal mucosae, upper and lower gingivae and floor of the mouth; a specific finding of widespread erosions on her buccal mucosae (Fig . 1); and small white
Correspondence to : Yumiko NAGAO, D.D.S.
Department of Oral Surgery, Kurume University School of Medicine, 67 Asahi-machi, Kurume 830 , Japan
Treatment of Lichen Planus in Patient with HCV 941 Fig. 1 Lichen planus of the right buccal mucosa
before SNMC. White lesions of the bilateral buccal mucosa accompanied by erosion.
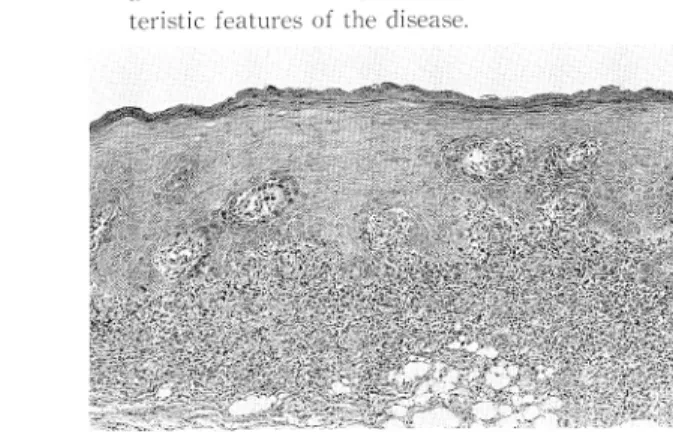
Fig. 2 Photomicrograph illustrating the charac-teristic features of the disease.
papules on the hard palate. All of the lesions caused severe contact pain. These lesions in the oral cavity were similar to those of lichen planus.
Other findings: Blood pressure, 120/80 mmHg; pulse, 60/min; no anemia in the palpable con-juctiva; no jaundice in the bulbus conjunctiva; no findings such as palmar erythema, vascular spider and pitting edema of either leg or foot; no abnormalities in heart and breath sounds; and no distention or fluctuation of the abdomen. The liver was palpable by one finger breadth below the right costal margin, the liver edge was blunt and, smooth, and its consistency was soft. The spleen was not palpable and the area of spleen dullness was widened.
Clinical examination: The results of peripheral blood examination included RBC, 508 x 104(/ mm3); Hb, 14.4 (g/dl); Ht, 43.6 (%); WBC, 7,000 (/mm3) (St, 6%; Seg, 38%; Ba, 1%; Lym, 47%; and Mo, 8%); and platelets, 20.4 x 10' (/mm3). Blood chemical tests on serum showed AST, 53 (IU/1); ALT, 59 (IU/1); y-GTP, 28 (IU/1); LDH, 307 (IU/1); ZTT, 21.1 (U); total bililubin, 0.66 (mg/dl); total protein, 8.8 (g/dl); albumin, 4.3 (g/dl); and y-globulin, 20.9 (%). HCV antibody was positive by the PHA method and serum HCVRNA was detected by the RT-"nested" PCR. The serum HCV RNA level measured by branched DNA signal amplification assay (bDNA, Quantiplex a, Chiron Corp., Emeryville, CA, USA) was 13.0 Meq/ml. The serum was negative for HBsAg and anti-nuclear antibody. The serum levels of IgA, IgM and IgG were 276, 149, and 2658 mg/dl, respectively. Ultrasonographic examination of the abdomen performed in the outpatient clinic revealed a hepatic shape similar to that in chronic hepatitis while no intrahepatic spaceoccupying lesion was observed. The spleen was enlarged. The pathohistological findings in a specimen biopsy of the oral mucosal lesion obtained when she visited outpatient clinic were similar to those of lichen planus (Fig. 2).
Clinical course and treatments: Since patients with chronic hepatitis C in general show only a slightly abnormal ALT level without reduction of liver function, we decided to observe her course without giving any specific treatment. For the OLP, we scaled her teeth and instructed her in tooth brushing. And we prescribed Cepharanthir powder daily at a dose of 20 mg/day in two divided doses after morning and evening meals. Simultaneously, a steroid for external use [Salcoat®] was used to treat the site showing severe inflammation. These treatments were continued for 7 months, resulting in slight improvement of the oral mucosal lesion, recurrence of the erosion, enlargement of the erosion in the bilateral buccal mucosa observed in October 1994, and ingestive disturbance due to the intensive contact pain. Then, considering her chronic hepatitis C, SNMC® was administered daily from October 1994 at a dose of 40 ml/day by intravenous injection. Two months after the therapy, erosion of the bilateral buccal mucosae had almost disappeared, the white papules observed over a
942 Yumilco NAGAO et al
Fig. 3 Lichen planos of the right buccal mucosa after SNMC.The size of the erosion is decreased.
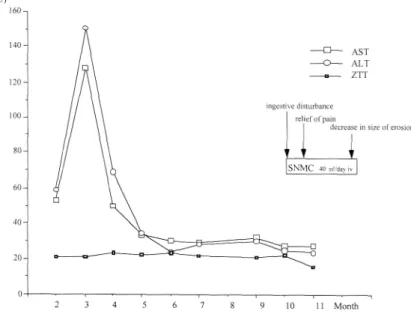
Fig. 4 illustrates the result of liver function tests and the clinical course of the patient.
wide range showed a tendency to disappear , and the pain was relieved (Fig. 3). During this period, no changes were observed in serum levels of AST and ALT from those before SNMC administration .
Discussion
Erosive or bullous types of OLP generally cause intensive contact pains . OLP is generally treated by systemic administration of various vitamins , adrenocortical hormones and tranquilizing agents, or local application of an ointment containing adrenocortical hormones''"' . Howerver, there is no established treatment for OLP at present. Among reports indicating the causes of lichen planus (LP) , a number of them suggest a relationship between LP and chronic hepatitis5)-15) . Recently LP ac-companying HCV infection has been reported at a high incidence14•16'-L8' Furthermore , it has become evident that HCV infection is associated with various immunological disorders , including cryog-lobulinemia, autoimmune thyroiditis and Sjogren syndrome19)
Treatment of Lichen Planus in Patient with HCV 943
patients with OLP will possibly be improved by administrating SNMC® which has been used to treat patients with viral hepatitis.
SNMC(R) containing glycyrrhizin as a main ingredient is a drug to improve liver function and is widely used for treating viral hepatitis. The efficacy of the drug has been established but its activity has not been as yet. It has been reported that the drug has such effects as antiinflamatory activity by glycyrretin, a metabolite of glycyrrhizin; interferon-derived antiviral activity; and activation of natural killer cells. SNMC® was intravenously injected at a daily dose of 40 mg to the present patient. Two weeks after the administration, contact pain at the buccal mucosae had decreased and, two and a half months after the treatment, the extent, color and pain of the OLP lesions were greatly improved as shown in Fig. 3 . Serum levels of AST and ALT, which in the normal range before administration of SNMC®, remained within normal limits during the treatment. This suggests that OLP had improved because of the direct effect of SNMC® on OLP, not because of the secondary effect of improvement in liver function by SNMC®. The results observed in the present study suggest that SNMC® is effective for treatment of OLP associated with HCV infection. The effect of the drug on the pathology should be clarified by further case studies.
References
1) Scully, C.& Kom, E. L.: Lichen planus. review and update on pathogenesis. J. Oral. Pathol. 14: 431-458, 1985. 2) Brody, L.: Electron microscopic demonstration of bacteria in the skin of patients with lichen ruber planus. Nature.
207: 96, 1965.
3) Neumann, J. B., Holmstrup, P.& Pindborg, J. J.: Smoking habits of 611 patiens with oral lichen planus. Oral. Surg. 43: 410, 1977.
4) Jolly, M.: Lichen planus and its association with diabetes mellitus. Med. J. Aust. 1: 990, 1972.
5) Rebora, A., Patri, P., Rampini E., et al.: Erosive lichen planus and cirrhotic hepoatis. It. Gen. Rev. Dermatol. 15: 123-131, 1978.
6) Rebora, A.: Lichen planus and the liver. Lancet. 1: 805, 1981.
7) Rebora, A.& Rongioletti, F.: Lichen planus and chronic active hepatitis. J. Am. Acard. Dermatol. 10: 840-841, 1984.
8) Rebora, A.& Rongioletti, F.: Lichen planus and chronic active hepatitis. Acta. Germ. Venereol. 64: 52-56, 1984. 9) Rebora, A.: Lichen planus and the liver. Acta. Derm. Venereol. 64: 365, 1984.
10) Cottoni, F., Solonas, A., Piga, M. R., Tocco, A., Lissia, M.& Cerimele, D.: Lichen planus, chronic liver disease and immunologic involvement. Arch. Dermatol. Res. 280: 55-60, 1988.
11) Rebora, A.: Lichen planus and the liver. Int. J. Dermatol. 31: 392-395, 1992.
12) Gandolfo, S., Carbone, M., Zulian, P., Brocoletti, R. Carrozzo, M.: Lichen planus orale e patoloia epatica. Parte II-Correlazioni clinico-statistiche tra manifestazioni orali e danno etatico. Minerva. Stomatol. 41: 209-213, 1992. 13) EL, Kabir, M., Sully, C., Porter, S., Porter, K.& Macnamara, E.: Liver function in UK patients with oral lichen
planus. Clin. Exp. Dermatol. 18: 12-16, 1993.
14) Nagao, Y., Sata, M., Tanikawa, K., Itho, K.& Kameyama, T.: Lichen planus and Hepatitis C virus in the Northern Kyushu region of Japan. Eur. J. Clin. (in press)
15) Okamoto, H., Okada, S., Sugiyama, Y., Tanaka, T., Sugai, Y., Akahane, Y., et al.: Detection of hepatitis C virus RNA by a two-stage polymerase chain reaction with two pairs of primers deduced from the 5'-non cording region. Japan. J. Exp. Med. 60: 215-222, 1990.
16) Ferguson, M.M., Simpson, N.B.& Hammersley, N.: The treatment of erosive lichen planus with a retinoid-etretinate. Oral. Surg. 58: 283-287, 1984.
17) Agner, T., Fogh, H.& Weismann, K.: The relation between lichen planus and hepatitis C. A case report. Acta. Derm. Venereol. 72: 380, 1992.
18) Jubert, C., Pawlotsky, J. M., Pouget, F., Andre, C., Deforges, L., Bretagne, S., et al.: Lichen planus and hepatitis C virus-related chronic active hepatitis. Arch. Dermatol. 130: 73-76, 1994.
19) Gandolfo, S., Carbome, M., Carrozzo, M.& Gallo, V.: Oral lichen planus and hepatitis C virus (HCV) infection: is there a relationship? a report of 10 cases. J. Oral. Pathol. Med. 23: 119-122, 1994.
20) Takahara, T., Watanabe, A.& Shiraki, K.: Effects of glycyrrhizin on hepatitis B surface antigen: a biochemical and morphological study. J. Hepatol. 21: 601-609, 1994.
944 Yumiko NAGAO et al グ リ チ ル リ チ ン の 静 注 治 療 が 著 効 を 示 し たC型 慢 性 肝 炎 を 有 す る 口 腔 扁 平 苔 癬 の1例 久留米大学医学部 口腔外科1),第2内 科2) 長 尾 由 実 子1)佐 田 通 夫2)谷 川 久 一2)亀 山 忠 光1) 要 旨 口腔 扁 平 苔 癬(orallichenplanus:OLP)は, 慢 性 の 角 化 異 常 を伴 う難 治 性 の 炎 症 性 疾 患 で あ る が,そ の 経 過 は長 く完 全 治 癒 が 困 難 な疾 患 の 一 つ で あ る.OLPの 発 症 原 因 に つ い て は種 々 の もの が あ る と され て い る が,今 だ 明 らか に され て お らず, 根 治 的 治 療 法 は,確 立 さ れ て い な い.そ こで 今 回, 従 来 慢 性 肝 炎 に対 す る有 効 な治 療 法 の 一 つ と して 広 く使 わ れ て い る グ リチ ル リチ ン(SNMC(R))を, OLP患 者 に投 与 して そ の経 過 を観 察 した. 症 例 は49歳 の 女 性 で,主 訴 は 口腔 内 粘 膜 全 体 の i接触 痛 で あ っ た.既 往 歴 にC型 慢 性 肝 炎 が あ り現 在 経 過 観 察 中 で あ る.現 病 歴 は,1994年11月 頃 よ り両側 下 顎 歯 肉部 か ら頬 粘 膜 にか け て 白斑 を認 め 近 医 で の加 療 を続 けて い た が,改 善 な い た め久 留 米 大 学 医 学 部 口腔 外 科 を受 診 した.扁 平 苔 癬(両 側 頬 粘 膜,全 顎 に及 ぶ 歯 肉 並 び に歯 肉 頬 移 行 部, 口底,口 蓋 粘 膜 部)の 診 断 で,セ フ ァ ラ ンチ ン(R)末 の 内 服 投 与 及 び外 用 ス テ ロ イ ド剤 を使 用 した.同 治 療 を7カ 月 続 け た が,口 腔 粘 膜 病 変 の若 干 の 改 善 と再 発 を繰 り返 す だ けで,同 年10月 に は両 側 頬 粘 膜 の び らん 面 の 拡 大 を認 め,強 い 接 触 痛 の た め に摂 食 障 害 が 出 現 し た.そ こで,軽 度 の血 清AST 値,ALT値 の 異 常 が あ る こ と を考 慮 し,SNMC の連 日投 与(40ml/dayiv)を 行 っ た.治 療 後2カ 月 で 両 側 頬 粘 膜 の び ら ん面 は ほ ぼ消 失 し また 広 範 囲 に認 め られ て い た 白斑 病 変 は消 失 傾 向 を示 し, 疹 痛 も軽 減 した.