日本血管外科学会雑誌 2021; 30: 183–186 183
巨大上腸間膜動脈瘤に対する1 手術例
古山 和憲 *,池田 真浩
要 旨: 症例は 65 歳女性.定期健診のため近医を受診した際に上腹部に拍動性腫瘤を指摘され当科紹介.CT 検査にて最大径 70 mm 大の巨大上腸間膜動脈瘤と診断.血管造影検査では右肝動脈が瘤から分岐する破格と瘤の 末梢から小腸領域および結腸へ灌流する 2 本の分枝を認めた.手術は開腹下で上腸間膜動脈と右肝動脈は直接吻 合し,瘤の末梢から出ていた 2 本の分枝は大伏在静脈グラフトを介して腹部大動脈と吻合した.術後経過は腸管 虚血や肝障害もなく良好であった.上腸間膜動脈瘤の頻度は内臓動脈瘤でも 5–8% 程度と比較的稀であり,手術 術式についても一定の見解は得られていない.今回われわれは,巨大上腸間膜動脈瘤に対する 1 手術例を経験し たので文献的考察を踏まえて報告する. (日血外会誌 2021; 30: 183–186) 索引用語: 上腸間膜動脈瘤,血行再建,大伏在静脈背
景
腹部内臓動脈瘤は比較的稀な疾患であるが,その中 でも上腸間膜動脈瘤の発生頻度は 5–8% とさらに少な い1–4).多くは破裂により初めて診断されるが,偶発的 に CT 検査などの画像検査で見つかる場合もある.今回 われわれは上腹部拍動性腫瘤を契機に発見された巨大上 腸間膜動脈瘤の 1 例を経験したため,文献的考察を踏ま えて報告する.症
例
患 者:65 歳,女性 主 訴:上腹部拍動性腫瘤 既往歴:慢性胃炎 現病歴:定期検診で近医を受診したところ,上腹部に 拍動性腫瘤を触知したため腹部大動脈瘤疑いにて当科紹 介.40 代頃から拍動性腫瘤を自覚していた. 既往歴:特記事項なし 喫煙歴:7 本/日(45 年間) 入 院 時 現 症: 身 長 162 cm, 体 重 47 kg, 体 温 36.4°C, 血圧 130/80 mmHg,脈拍 65 回/分,腹部は平坦軟,心窩 部に拍動性腫瘤を触知,自発痛や圧痛なし.血液検査所 見,心電図検査および胸腹部レントゲン検査では明らか な異常所見は認めなかった. 腹 部 造 影 CT 検 査: 最 大 短 径 70 mm の 上 腸 間 膜 動 脈 瘤を認める(Fig. 1a).瘤から右肝動脈が分岐している (Fig. 1b). 上腸間膜動脈造影検査:右肝動脈は上腸間膜動脈瘤の 根部より分岐しており,瘤の末梢側から分枝を 2 本認め る(Fig. 2). 手術所見:腹部正中切開で開腹.上腸間膜動脈瘤は 腹側に膵臓を持ち上げる形で認めた.上腸間膜動脈本 幹(径約 6 mm)と右肝動脈(径約 3.5 mm)は巨大な瘤 に接するように存在していたため剝離に難渋し,かつ瘤 を膵臓が覆っており視野の確保に難渋した.腸間膜内 の上腸間膜動脈瘤末梢の 2 本の分枝(径約 3 mm)も剝 離.全身ヘパリン化ののち,上腸間膜動脈本幹・右肝動 脈・上腸間膜動脈瘤末梢の分枝 2 本を遮断後,瘤を切開 した.上腸間膜動脈本幹と右肝動脈は断端が近いため, 6-0 PROLENE 連続の端々吻合で再建した.次いで,腹 部大動脈を下腸間膜動脈直下と bifurcation 直上で完全遮 断し,腹部大動脈に puncher で 2 カ所吻合口を作成した 後,6-0 PROLENE 連続の端側吻合で大伏在静脈グラフト (径約 4 mm)2 本と腹部大動脈の吻合を行った.その後, この大伏在静脈グラフト 2 本と上腸間膜動脈末梢の 2 本 の分枝を 7-0 PROLENE 連続の端々吻合で各々再建した (Fig. 3). 術後経過:術後 4 日目に経口摂取を開始.その後腸管 虚血症状を認めず,腹部造影 CT 検査で開存も確認でき 富山赤十字病院心臓血管・呼吸器外科 〒930–0859 富山県富山市牛島本町2丁目1–58 * E-mail: [email protected] 受付:2021年2月12日 受理:2021年4月8日 doi: 10.11401/jsvs.21-00013■ 症
例
184 日本血管外科学会雑誌 第30巻 第3号(2021) たため,術後 14 日目に独歩退院した.術後 2 年目の CT 検査ではグラフトおよび腸管等血流に問題を認めなかっ た(Fig. 4).術後 5 年を経過した現在も問題なく他院通 院中である.
考
察
腹 部 内 臓 動 脈 瘤 は 全 人 口 の 1% 程 度, 剖 検 例 で は 0.01–0.2% にしか見られない比較的稀な疾患である5, 6). その中でも上腸間膜動脈瘤の頻度は,全内臓動脈瘤の うち 5–8% とさらに稀であるが1–4),脾動脈瘤 31.6–60%, 肝動脈瘤 20–24.8% に次いで 3 番目に多いとも言われて いる1, 4, 7).原因としては動脈硬化,先天性の血管異常, 感染,血管炎,膵炎,外傷性,医原性などさまざまで あり,また,以前は真菌感染によるものが 60% と多かっ た8, 9).しかし,最近は分節状動脈中膜融解や線維筋性 異形成による報告も散見される1, 10).本症例は高血圧の 既往はないものの,喫煙者であり動脈硬化性によるもの が考えられたが,40 代頃から拍動性腫瘤を自覚してい たため先天性に存在し,徐々に増大していた可能性も否 定はできない.症状としては本症例のように拍動性腫瘤 を触知する場合や,瘤増大による臓器の圧迫症状を認め ることがあるが,無症状のことも多く,人間ドックや健 康診断などで偶然発見される場合や,破裂するまで気づ かれない例も少なくない3). CT 検査等で上腸間膜動脈瘤と診断がついた場合,血 管造影検査によって瘤の形態や血管の分岐,側副血行路 の有無などより詳細な情報を把握し,術式を決定しなけ ればならない. 治療については瘤の局在や大きさにより,開腹手術や コイル塞栓術,ステント治療などさまざまであり2),治 療適応についても施設により多様である.一般的には, 破裂症例はもちろん瘤径の急速な拡大を伴うもの,仮性 瘤,出産適齢期の女性,妊婦については治療適応がある と考えられるが,瘤径については破裂の可能性との関連 を示唆するデータが少なく,一定の見解は得られていな い6).上腸間膜動脈は小腸および右半結腸を灌流してい ることから上腸間膜動脈瘤の治療法については慎重を期 する必要がある.瘤が下膵十二指腸動脈や中結腸動脈よ り中枢側にあり,腹腔動脈や下腸間膜動脈からの側副血 行路を介して小腸や右半結腸に灌流される場合,血行再 建は不要でコイル塞栓や瘤の単純結紮で十分であること が多い7, 9).しかし,瘤が末梢側にある場合や側副血行Fig. 1 a; Enhanced computed tomography showed the superior mesenteric artery aneurysm (arrow). b; Enhanced three-dimensional computed tomog-raphy showed the superior mesenteric artery aneurysm. The right hepatic artery branched from the aneurysm (arrowhead).
Fig. 2 Preoperative angiography of the superior mesenteric artery showed the right hepatic artery branching from the aneurysm (arrow) and two branches from the distal part of the aneurysm (arrowhead).
185 古山ほか: 巨大上腸間膜動脈瘤の1例 路の発達がない場合は血行再建を行わないと腸管虚血を 来してしまう1, 2).本症例では術前の血管造影検査で右 肝動脈が瘤から分岐していること,瘤の 2 本の末梢枝が 小腸・結腸を灌流していると考えられたことから,これ らの分枝の血行再建が必要であり,その大きさからして も開腹手術以外の選択肢はなかった.右肝動脈は上腸間 膜動脈本幹と近く,直接吻合が可能であったため端々吻 合で再建を行った.2 本の末梢枝については in flow とす る腹部大動脈と距離があったため大伏在静脈グラフトを 介して再建を行った.自然なグラフト走行デザインが想 像しづらかったので,グラフトを長めにして長さに余裕 をもたせた.使用するグラフトについては大伏在静脈の 他に,人工血管や脾動脈,内腸骨動脈を使用した報告 があり2, 3),McMillan らは 3 年で大伏在静脈の開存率は 95%,polytetrafluoroethylene(PTFE)は 89% と報告してい る11).また,島田らは静脈グラフトが動脈系へ移植さ れるとその高い血圧と浸透圧によって静脈壁が肥厚し静 脈の動脈化が起こり,場合によっては再手術の原因とも なることから動脈グラフトを選択している3).上腸間膜 動脈瘤の経過については適切な治療が行われれば予後は 比較的良好であり,本症例も術後 5 年経過した現在も問 題は起こっていない. 近年血管内治療の発展に伴い,上腸間膜動脈瘤に限 らず腹部内臓動脈瘤の治療において血管内治療の適応 が拡大しつつある6).とくに解離性上腸間膜動脈瘤や外 傷,もしくは消化器外科術後の上腸間膜動脈仮性瘤に対 しては,コイル塞栓術やステント挿入術のみならず,最 近ではステントグラフトの使用や12–17),ハイブリッドで 行った報告も散見される18, 19).Jiang らはその適応にお いて,(1)ステントグラフトにより腸管へ流入する分枝 が閉塞されないこと,(2)瘤が大きすぎず,適切なラン ディングゾーンが確保できること,(3)感染性でないこ と,を述べているが20),本症例のように上記に当ては まらない場合においてはやはり外科的治療が必要であ り,上腸間膜動脈瘤はその性状や局在から,術式や血行 再建の有無について慎重に判断を行う必要がある.
利益相反
本論文について申告する利益相反はない.文
献
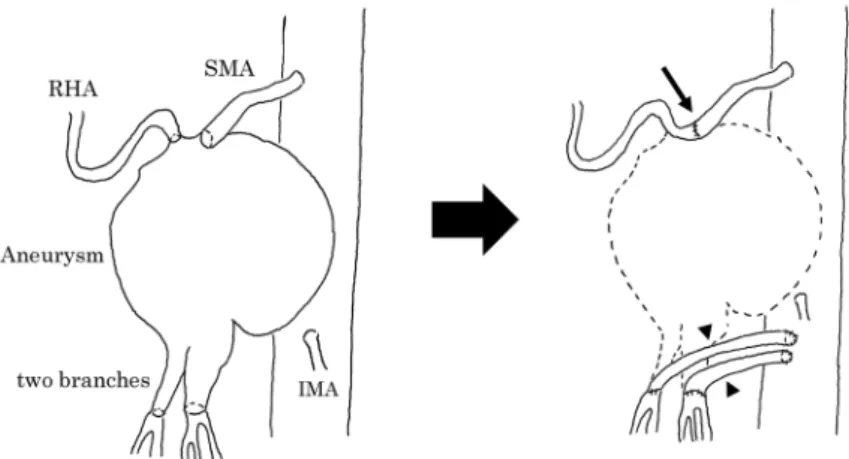
1) 小野裕國, 阿部裕之, 北中陽介, 他. 背部痛を契機に 診断された巨大上腸間膜動脈瘤の 1 治験例.日血外会誌 2013; 22: 53–56. 2) 片山桂次郎, 野村文一, 泉谷裕則, 他. 巨大上腸間膜 動脈瘤に対し瘤切除分枝再建を行った一例.日血外会誌 Fig. 3 Shema of reconstruction design. The SMA was directly anastomosed to the RHA (arrow). Two branches of the SMA aneurysm were anasto-mosed to the abdominal aorta with the saphenous vein grafts individually interposed (arrowhead). SMA; superior mesenteric artery, RHA; right hepatic artery, IMA; inferior mesenteric artery.Fig. 4 Enhanced three-dimensional computed tomography image (arrow; blood vessel graft, arrowhead; SMA-RHA bypass).
186 日本血管外科学会雑誌 第30巻 第3号(2021) 2005; 14: 23–26. 3) 島田順一,河内秀幸,塚本賢治,他.上腸間膜動脈瘤に 対して内腸骨動脈グラフトを用いて血行再建を行った 1 例.日消外会誌 1991; 24 :1061–1065. 4) 下江安司,金香充範,安田 理.腸骨動脈瘤と多発腹部 内臓動脈瘤に対する同時手術の 1 例.日臨外会誌 2010; 71: 1980–1984.
5) Panayiotopoulos YP, Assadourian R, Taylor PR. Aneurysms of the visceral and renal arteries. Ann R Coll Surg Engl 1996; 78: 412–419.
6) 高橋直子,布川雅雄,今村健太郎,他.腹部内臓動脈瘤 の治療検討.日血外会誌 2010; 19: 487–493.
7) Stone WM, Abbas M, Cherry KJ, et al. Superior mesenteric artery aneurysms: is presence an indication for intervention? J Vasc Surg 2002; 36: 234–237.
8) 石川 健,山本 寛,古川 顕,他.解離を伴った上腸 間膜動脈瘤破裂の 1 例.日臨外会誌 2005; 66: 493–496. 9) Shanley CJ, Shah NL, Messina LM. Uncommon splanchnic artery
aneurysms: pancreaticoduodenal, gastroduodenal, superior mes-enteric, inferior mesmes-enteric, and colic. Ann Vasc Surg 1996; 10: 506–515.
10) Kimura K, Ohtake H, Kato H, et al. Multivisceral fibromuscular dysplasia: an unusual case of renal and superior mesenteric in-volvement. Ann Vasc Dis 2010; 3: 152–156.
11) McMillan WD, McCarthy WJ, Bresticker MR, et al. Mesenteric artery bypass: objective patency determination. J Vasc Surg 1995; 21: 729–740.
12) Drescher R, Köster O, von Rothenburg T. Superior mesenteric artery aneurysm stent graft. Abdom Imaging 2006; 31: 113–116. 13) Ishida M, Kato N, Hirano T, et al. Dissecting aneurysm of the
superior mesenteric artery successfully treated by endovascular stent-graft placement. Cardiovasc Intervent Radiol 2003; 26: 403–406.
14) Patelis N, Doukas P, Dodos I, et al. Endovascular repair of a complex isolated dissecting aneurysm of the superior mesenteric artery. EJVES Short Reports 2019; 44: 5–8.
15) Shrikhande GV, Khan SZ, Gallagher K, et al. Endovascular man-agement of superior mesenteric artery pseudoaneurysm. J Vasc Surg 2011; 53: 209–211.
16) Boufi M, Belmir H, Hartung O, et al. Emergency stent graft im-plantation for ruptured visceral artery pseudoaneurysm. J Vasc Surg 2011; 53: 1625–1631.
17) Rocek M, Peregrin JH, Dutka J, et al. Percutaneous treatment of a superior mesenteric artery pseudoaneurysm using a stent-graft. AJR 2002; 178: 1459–1461.
18) Cumbie TA, Kedora JC, Pearl GJ, et al. A hybrid repair of a supe-rior mesenteric artery pseudoaneurysm using open mesenteric by-pass and endovascular exclusion. Proc Bayl Univ Med Cent 2015; 28: 355–357.
19) Nomura Y, Yamaguchi M, Kitagawa A, et al. Hybrid management of ruptured isolated superior mesenteric artery dissecting aneu-rysm. J Vasc Surg 2011; 54: 1808–1811.
20) Jiang J, Ding X, Su Q, et al. Therapeutic management of superior mesenteric artery aneurysms. J Vasc Surg 2011; 53: 1619–1624.
A Case of a Giant Superior Mesenteric Artery Aneurysm
Kazunori Koyama and Masahiro Ikeda
Department of Cardiovascular and Chest Surgery, Toyama Red Cross Hospital
Key words: superior mesenteric artery aneurysm, reconstruction of superior mesenteric artery, saphenous vein graft We herein report a case of a giant superior mesenteric artery (SMA) aneurysm. A 65-year-old woman was admitted to our hospital because of a pulsatile upper abdominal mass. She was diagnosed of a giant aneurysm of the SMA (maximum diameter of 70 mm) by enhanced computed tomography (CT). In the preoperative angiography, the right hepatic artery was branched from the aneurysm, and two branches from the distal part of the aneurysm provided blood inflow to the small bowel and colon respectively. Aneurysmectomy with recon-struction of the SMA branches was performed. The SMA trunk was anastomosed to the right hepatic artery. Two branches of the SMA aneurysm were anastomosed to the abdominal aorta with the saphenous vein grafts individually interposed. The postoperative course was uneventful, and no abdominal complications occurred.