論
文 題 名(注:学 位 論 文 題 名 が 英 語 の 場 合 は 和 訳 をつ け る こ と。)
Effectiveness of neural mobilization for spinal radicular pain: a systematic review with meta-analysis
神 経 根 症 状 に 対 す る神 経 モ ビ ラ イ ゼ ー シ ョ ン の 効 果:
シ ス テ マ テ ィ ッ ク レ ビ ュ ー と メ タ 分 析
(西 暦)2020年 8月 19日 提 出
東 京 都 立 大 学 大 学 院
人 間健康 科 学研 究 科 博 士 前 期 課 程 人 間健 康 科 学 専 攻 理 学療 法 科 学 域 学 修番 号:18895718
氏 名 Wirojwiriyak ul Dherawit
(指導 教 員 名: 山 田 拓 実 )
Effectiveness of neural mobilization for spinal radicular pain: a systematic review with meta-analysis
Wirojwiriyakul Dherawit,Nagahori Hiraku, Takumi Yamada
Abstract
Background: Neural mobilization or neurodynamics is one of the most widely used techniques by physiotherapists to restore the homeostasis of structures both inside and around peripheral nerves and the nervous system. It is especially used to reduce spinal radicular pain. However, the effects of neural mobilization targeting spinal radicular pain symptoms are largely unknown. •
Objective: To determine the effectiveness of neural mobilization for patients with spinal radicular pain.
Study design: Systematic review with meta-analysis
Method: Randomized control trials were included from four databases, namely Cochrane, PubMed, CINHAL, and PEDro, and grey literature, if any form of neural mobilization was performed in patients with spinal radicular pain. The PEDro scale was used to appraise the methodological quality. Using the random effect model, studies were pooled for meta-analysis, and pain score was the primary outcome.
Results: A total of 36 studies were included for full-text analysis, and 6 studies qualified to be included for the assessment of methodological quality. However, 4 studies, involving 213 subjects, that met the predetermined criteria were selected to be pooled for meta-analysis. Overall, the studies had poor to good quality, with an average Pedro score of 4.17 (from 2 to 6). The pooled pain intensity (scale [0-10]:
mean difference, -1.94; 95% CI: -2.98, -0.91; p< .001) decreased following neural mobilization.
Conclusion: The evidence showed beneficial effects of applying neural mobilization to patients with spinal radicular pain. Specifically, neural mobilization techniques can reduce pain among patients with spinal radicular pain. Nonetheless, higher methodological quality and number of studies are essential to confirm the conclusions of this review
Keywords: Neural mobilization, Neurodynamics, Spinal radicular pain, Manual therapy, Physical therapy
Introduction
Spinal radicular pain is usually included as one of the dominated symptoms of spinal radiculopathy, which are multi-factorial nerve root injuries resulting in significant pain, phycological stress, and disability. It has a possibility to occur at any level along the spinal column, with the highest incidence at the lumbar spine, cervical
spine, and rarely in thoracic spine. The treatment for spinal radicular pain can be surgical or non-surgical including manual therapy such as bone mobilization and exercise. While neural mobilization is one of the most widely used
clinical therapy to address the pain generated by spinal radicular pain.
Neural mobilization was initially developed from the neural tension concept. For the first time neural mobilization was used for physical examination and gradually extended to be used for treatment to restore homeostasis for local nerves and the whole nervous system. Recently, neural mobilization technique was also referred to as neurodynamics. Several neural movement techniques have been developed based on neural mobilization concepts such as cervical lateral glide neural mobilization and median nerve neural mobilization
(MNNM). The hypothesized advantageous effects from neural mobilization include facilitation of nerve gliding, reduction of nerve adherence, dispersion of noxious fluids, increased neural vascularity, and improvement of
axoplasmic flow.
As mentioned above, spinal radicular pain radiating to both arms and legs is one of the primary symptoms of patients visiting physical therapy clinic. Although several techniques can be used to address the patient's problem, physical therapists recommended neural mobilization as one of the most useful techniques reducing
radiating pain. However, effectiveness of using neural mobilization among different patients' conditions such as the lower back pain, cervicobrachial pain, and nerve-related neck and arm pain have been extensively documented.
Besides, there are many study designs and results. Some studies with strict methodology assessed the results of using neural mobilization alone, while a few others found the combination effects of using neural mobilization
along with conventional treatment. In addition, some studies showed neural mobilization as one of the beneficial treatments for patients with spinal radicular pain. However, a few others declared neural mobilization may not have satisfying effects in such patients. So, appraising the quality of existing study and pooling the results by
doing systematic review and meta-analysis is the only way to ensure whether neural mobilization for patients with spinal radicular pain is advantageous.
Objectives
The main purpose of this study was to determine the effectiveness of neural mobilization for patients with spinal radicular pain both qualitatively and quantitatively.
1) To appraise the quality of available studies illustrating the effects of neural mobilization among patients with spinal radicular pain by the PEDro scale.
2) To pool the effects of treating patients with spinal radicular pain by neural mobilization and examine its effects in pooled population by meta-analysis.
Methodology
This study aimed to appraise the quality and illustrate the effects of using neural mobilization among patients with spinal radicular pain by systematic review and meta-analysis, respectively. Any neural mobilization methods were included from chosen databases and grey literatures. The methodology was separated into two main processes of systematic review and meta-analysis. The systematic review was conducted by two reviewers who followed a predetermined protocol separately, while meta-analysis was performed by one researcher using Review Manager Computer software.
The research plan was registered at the PROSPERO international prospective register of systematic reviews, University of York, Centre of reviews and dissemination, England.
The registration number was CRD42020140106, and the registration study was published at PROSPERO website on 25 March 2020
(https://www.crd.york.ac.uk/prospero/display record.php?RecordlD=140106)
Searching methodology
The systematic review process was started by the generation of search keywords, including and interpreting by PICO question, and then extended to their synonyms and thesaurus. Next, they were transferred to concept mapping table. Each column of concept mapping was shortened, but the meaning was widened by truncation and free text (MesH term). Next, each column of concept mapping was connected to each other by Boolean operation and was used to generate the searching term for each online database.
PICOS questions for this study were generated following the research questions and hypotheses as patients: patients with radicular pain, intervention: intervention is neural mobilization, control: shame or
conventional treatments, outcome measurement: pain scale, study: Randomized control trial respectively.
Participants/ population
The standard predetermined protocol for inclusion selection was the studies which were control trials and published in English (between 1 March 2010 to 29 February 2020). Besides, the studies must be on humans only.
Moreover, the neural mobilization techniques must have been performed by authentic physical therapy.
Inclusion criteria
• Randomized control trial designed study during the past 10 years (published before March 2020)
• The subject over 18 years old
• The main outcome measurements were pain measurement (NPRS, VAS).
• The aim of each study must be showing the effects of using neural. mobilization techniques compared with any intervention.
Exclusion criteria
• Other kinds of study
• Studies reporting participants who had undergone surgical treatments and systematic diseases
• Not showing effects of neural mobilization and showing mixed effects of neural mobilization and another technique.
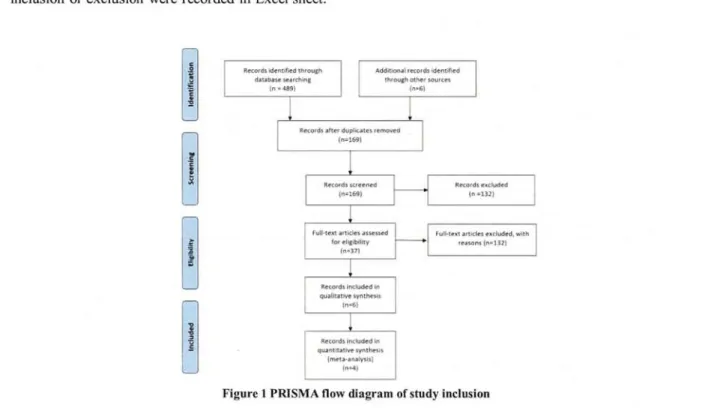
The two reviewers separately read and criticized 169 included studies based on their title and abstract, and finally, 37 studies were included for the next step of reviewing showing in figure 1.
Full text reviewing was done for 37 studies. Both reviewers separately read and collected the data from all 37 studies. Each study was read carefully in detail and the extracted data, identification information, and reason for inclusion or exclusion were recorded in Excel sheet.
c f'
! Records identified through Additional records identified
1 In = 489)(n=6) database searchingthrough other sources
Records after duplicates removed (n=169)
lr---
I
Records screenedRecords excluded
(n=169)in =132)
Full•text articles assessedFull-text articles excluded, with
for eligibility---•reasons (n=1321
3(n=371
I
I Full text articles assessed for eligibility
In=37)
Records included in qualitative synthesis
In=6}
Records Included in quantitative synthesis
{meta analysis)
In=4)
Figure 1 PRISMA flow diagram of study inclusion
For the last steps of reviewing, the collected data from both reviewers were peer read and checked for assembled data. For some studies, discussion was used to finalize whether the studies should be included or excluded. In this process, the opinion of the third reviewer was not necessary because two main reviewers agreed after discussion for all studies.
Finally, six studies were figured out having sufficient quality to be included to appraise in the next step of systematic review, while only 4 studies were homogenous to be pooled and analyzed in meta-analysis process.
The PEDro scale analysis tool was used to evaluate the quality of existence evidences and random effect model in Revman computer program version 5.3 was used to analyze the pooled effects of included studies.
Results
All retrieved 495 studies were screened to exclude duplicate studies. A _ total of 169 studies were roughly checked based on their title, type of study, and abstract, and only 37 studies were included for full text analysis.
Finally, 6 studies were accepted to be included for quality appraisal using the PEDro scale and analyzed for their pooled effected using the random effect model of the meta-analysis method.
The qualified 6 studies were thoroughly reviewed for their methodology and statistical analysis.
Afterwards, all were included for participation in quality appraising process. The table below shows the formation of each study.
Table 1 Description of studies
Stud Title
Patient demoffranhics
Intervention
group Control grou
Outcome
measures Results
David Rodriguez-Sanz et al37
David Rodriguez-Sanz et a138
Effects of Median Nerve Neural Mobilization
in Treating Cervicobrachi al Pain: A Randomized Waiting List—
Controlled Clinical Trial
Cervical Lateral Glide Neural Mobilization Is Effective in Treating Cervicobrachi al Pain: A Randomized Waiting List Controlled Clinical Trial
n=51(21 male, 30 female) age rage 18-45 NRSP at baseline for intervention group is 6.52
? ?0.89 and for control group is 6.39 ? ?o.95
n=52 (26 male, 26 female) Average age for intervention group and control group are 33.3 ??
5.0 32.5 ? ? 4.6 respectively,
<0.53.
n=23 participants with
cervicobrachial pain
median nerve neural mobilization (MNNM) continuously five times for 2 minutes, with 1 minute of rest between applications. The treatment was performed 5 days a week for a total of 6 weeks n=25 participants with
cervicobrachial pain.
two minutes in five consecutive applications, with one minute of rest between each two-minute CLG application five days a week and distributed in a period of six weeks. total of 30 CLG phys- ical
n=28 participants with
cervicobrachial pain
waiting for treatment after the experiment was finished.
n=27 participants with
cervicobrachial pain waiting for treatment after the experiment was finished.
Primary outcome is NRSP was recorded at days 1, 15, and 30. And after treatment 1 hour Seccondary outcome are quick DASH and CROM were recorded at dayl and day30. after treatment 1 hour
Primary outcome is NRSP was recorded at days 1, 15, and 30.
Seccondary outcome are
quick DASH and CROM were recorded
at dayl and day30.
After 30 days and 1 hour of treatment participants in intervention group's pain is 3.08? ?o.83 while control's group is 6.78? ?o.83.
Participants in intervention group reported a decrease of 2.16 NRSP points at the moment of dis- charge, which represents a 35.5% variation improvement.
therapy application days across a six-week period.
Dong-Gyu Kim et a139
Nishant H Nar4°
The effects of neural mobilization on cervical radiculopathy patients' pain, disability, ROM, and deep flexor endurance
Effect of Neural Tissue Mobilization on Pain in Cervical Radiculopathy Patients
n=30 (15 male, 15 female).
Average age for intervention group and
control group are 29.27 (3.34) and 29.33 (3.07) respectively, p=
0.959. NPRS (score) at baseline are
7.00 (0.85) for intervention group and 7.07 (0.80) for control group P=0.826.
n=30 (9 male, 21 female) Average age for
intervention group and control group are 43.93 + 7.05 and 45.06 + 7.46 respectively.
VAS at baseline are 7+1.06 for intervention group and 7.13+0.99 for control group.
n=15 participants with cervical radiculopathy patients neural
mobilization with manual cervical traction (NMCT) + conservative treatments three times per week.
Participants received conservative treatment for 35 minutes and experimental treatment for 10 minutes each time.
n=15 participants with cervical radiculopathy Neural Mobilization + Conventional Therapy
10 days with one session per day (6 days per week)
n=15 participants with cervical radiculopathy patients manual cervical traction (MCT) + conservative treatments three times per week.
Participants received conservative treatment for 35 minutes and experimental treatment for 10 minutes each time.
n=15 participants with cervical radiculopathy conventional thrapy (IF+
cervical traction+isomet ric exercises and advices).
10 days with one session per day (6 days per week)
Outcomes measured at baseline, week 4, and follow- up at week 8.
VAS 1.
2.
3.
4.
NPR S NDI ROM Deep flexor en- duran ce
Intervention group (pre: 7.00 0.85 points, four weeks: 3.93 ± 0.80 points, and eight weeks: 2.13
± 0.92 points; F = 330.74 and P = 0.000) Control group (pre: 7.07 ± 0.80 points, four weeks: 4.93 ± 1.10 points, and eight weeks: 3.20
± 1.26 points; F = 193.70 and P = 0.000).
Mean values of VAS at post treatment in intervention group is 2.06+1.33 and for control group is 3.53+1.12 with value is p < 0.01.
Rohini Gupta and Shallu Shama41
Effectiveness of Median Nerve Slider's Neurodynami cs for managing Pain and Disability in Cevicobrachai 1 Pain syndrome
N=34 (18 male, 16 female) age range from 18- 40 years old.
VAS at pre experiment are 5.15 for intervention group and 5.30 with Z value =
0.58(non- significant)
n=16
Median nerve sliders neurodynamics
five sessions over a period of seven days.
n=18
conventional treatment compraising of neck and shoulder exercise and ergonomic • advice.
five sessions over a period of seven days.
VAS, NDI and CBSQ
Post-intervention Vas for intervention group is 3.30 with z=3.51(Significan t) while for control group is 5.0 with z=2.61 (Significant)
Sahareen Anwar et a142
Effectiveness of
neuromobiliza tion in patients with
N=30 No
demographic information
N=15 Neural
mobilization+
conventional treatment
N=15 Conventional treatment consisted of intermittent cervical
VAS and NDI P=0.46
cervical radiculopathy
traction,hot pack, and
isometric neck exercise.
From 6 studies above, the reviewers had same opinions a the quality of each study was shown in the diagram below.
bout their quality. Using the PEDro scale tool,
Criterion
study 1 2 3 4 5 6 7 8 9 10 11 total
David Rodriguez-Sanz et al David Rodriguez-Sanz et a!38 Dong-Gyu Kim et a139 Nishant H Nar4°
Roluni Gupta and Shallu Shalna41 Sahareen Anwar et a!42
Y Y Y N N Y
Y Y Y Y Y Y
Y Y N N Y N
N N Y N N N
N N N N N N
N N N N N N
Y Y N N N N
Y N Y N N N
N N N N N N
Y Y Y Y Y Y
Y Y Y Y Y N
6 5 5 3 4 2 Note: 1. Eligibility, 2. Random allocation, 3. Concealed allocation, 4. Baseline comparability, 5. Blind subjects, 6. Blind therapists, 7. Blind assessors, 8. Adequate follow-up, 9. Intention-to-treat analysis, 10. Between-group comparisons, 11. Point estimates and variability. Eligibility criteria item does not contribute to total score ; Y, yes ; N, no
Figure 2 Quality of the included studies
Using the PEDro scale assessment tool, the included six studies were appraised for their quality.
of score was 2-6 from poor to high quality. The average score was 4.17, which illustrated fair quality evidences.
The range of existing
Meta-analysis results
For meta-analysis, two studies were excluded from the pooling analysis because they lacked enough homogeneity. Data were collected for the left four studies and reanalyzed to show bigger effects. Revman computer software version 5.3 was used in this process. Effect sizes were compressed by odds ratio for categorical data as well as weighted mean differences for continuous data at 95% confidence intervals (CIs). The standard x2 (Q2) test and inconsistency index (I2) were used to assess heterogeneity. In case the inconsistency index (I2) or x2 test was less than 0.5 or 0.1, the meta-analysis was performed using the random effects model. The diagram below shows the results of meta-analysis.
NMT interventions Control Std. Mean Difference Std. Mean Difference Study or Subgroup Mean SD Total Mean SD Total Weight IV,-Random95% CI EV Random, 95°%CI Kim et al. 20172.13 0 92 15 3.2 1.26 15 25 2% -0 94 F1,70, •0.18] —2—"
Nishant 20142.06 1 33 15 3.53 1.12 15 25 0% -1 16 F1,95, -038]
Rodriguaze-Sanz et al. 2017 (Pedro5) 4.12 1.23 25 6.88 0.97 27 25.4% -2.47 F3.20, -1.731 - Rodnguez-Sanz et al. 20173.08 1.41 23 6.78 0.83 28 24.3% -3.23 1-4.08, -2.38] —*—
Total (95% CI)7885 100.0% -1.941-2.98, -0.91) F
Heterogeneity: Tau'. 0.96; Chr'= 21.07, tlt= 3 (P = 0.0001); P= 86%41—~a
Testtor overall effect Z= 3.68 (P = 0.0002)` Favours 'experimental] Farours[control]
Figure 3 Forest plot showing the results of the meta-analysis of the included studies
The forest plot showed Z value at 3.68 from 163 participants (78 participants received some neural mobilization techniques while 85 participants were in the control group). The graph demonstrated one of the effects of neural mobilization which was improvement in pain at standard mean difference -1.94. Moreover, all the studies favored a decrease in pain measurement after neural mobilization was applied.
Discussion
Neural mobilization is widely used for restoring the homeostasis of nerves and neural tissues by mobilization of the nervous system or structures around it.
Many studies indicated the beneficial effects of applying neural mobilization to wide range of symptoms and disorders affected by neuropathic pain such as lateral epicondylalgia, carpal tunnel syndrome, and tarsal tunnel syndrome.
In the past, neural mobilization concept was used to describe dysfunction of peripheral nervous system called neural tension. Recently, the combination physiological concepts such as structure and function of the nervous system. Neural mobilization or neurodynamic is more accepted in definition of integrated biomechanical, physiological, and morphological functions of the nervous system1-2' 43-46
Spinal radiculopathy is a multifactorial nerve root injury that can generate neuropathic pain, physiological stress, and disability. Although it can occur at any level of spinal column, the highest level is the lumbar spine, cervical spine, and thoracic spine.
Several studies applied neural mobilization aiming to reduce pain and disability in patients with spinal radicular pain. Moreover, many studies showed advantageous effects as well.
This review identified randomized control trials investigating neural mobilization from 4 main physical therapy online electronic databases including a total of 495 studies for screening. Then, 6 studies met the
predetermined inclusion criteria. Analysis of these studies showed improvement in pain intensity after receiving
neural mobilization treatment for a period37'2. These 6 studies demonstrated fair methodological quality with score ranging from 2-6, while average score was 4.17 rated using the PEDRO scale.
Although the quality of existing studies was fair, 2 studies were excluded during the pooling of therapeutic
efficacy of neural mobilization and reassessed by statistical methodology because of lack of homogeneity and the left 4 studies .showed a favorable effect (standard mean difference -1.94).
Due to variable heterogeneity among neural mobilization techniques, this review was designed with the purpose to assess overall beneficial effects of all types of neural mobilization techniques used in physical therapy
clinic. Thus, each randomized control trial has their own specific characteristic. All included studies showed heterogeneity at different pathologies and different types of neural mobilization. David Rodriguez-Sanz et a137 _used median nerve neural mobilization for treating cervicobrachial, while the same group38 had earlier applied cervical lateral glide neural mobilization for treating cervicobrachial pain. Dong-Gyu Kim et a139 examined the effects of neural mobilization along with manual cervical traction (NMCT) and conservative treatments compared with NMCT and conservative treatments. Nishant H Nar40 used standard ULTT 1 combination with conventional therapy, although Rohini Gupta and Shallu Shama41 used median nerve sliders neurodynamics. The last study by Sahareen
Anwar et al42 used neural mobilization along with conventional treatment but the technique was camouflaged.
As mentioned above, the diversity and heterogeneity of neural mobilization techniques is a considerable point for retrieving and assessing the quality of each neural mobilization study. Further study .should focus at one
pathology or one specific type of neural mobilization technique for seeking details about its effectiveness.
Limitation of this study
Due to the strict inclusion criteria of this study, some studies might have been excluded. Besides, only the studies which were published in English were included. However, this study was designed to guarantee inclusion
of wide spectrum of neural mobilization techniques. Nonetheless, due to the evidence limitation and small study samples, conclusion may change over time.
Conflicts of interest
No funding sources and conflicts of interest were reported for this study.
Clinical application
1) Neural mobilization is one of the most useful manual techniques utilized to remove pain and improve disability in wild range of neuromuscular conditions.
2) There are many conservative treatments that can reduce radicular pain originated by neural tissue.
3) Neural mobilization alone and in combination with conventional treatments may improve pain and function in patients with spinal radicular pain. However, individual conditions of patients or other concerning
parameters may limit the effectiveness of neural mobilization techniques.
Conclusion
Neural mobilization techniques including: standard neural mobilization, cervical lateral gliding, neural mobilization along with manual cervical traction and conservative treatments, and standard neural mobilization along with conventional therapy have shown improvement in pain in patients with spinal radicular pain. The finding of the reviews may be used as a guideline to manage patients with cervical radicular pain.
Recommendation for further studies
One of the strengths of this study was its design to examine any kind of neural mobilization technique.
Although the limitations were big problems about definition and techniques of used neural mobilization which may lead to a lack in quality of search research. Moreover, the diversity of neural mobilization techniques may lead to lack of quality of searching methodology. Further studies should focus at similar pathologies and similar neural mobilization techniques.
The hypothesis of using neural mobilization is an attempt to restore balance tension of nervous tissue and interfaces by reducing intrinsic pressure on the neural tissue, facilitation of nerve gliding or reduction of nerve
adherence. Besides, it causes dispersion of noxious fluids, increased neural vascularity, and improvement of
axoplasmic flow. Thus, observing in-vivo measurements of neural movement may be very important for better understanding during physical changes of nerves and its interfaces. Several studies tried to examine the biological effects of neural mobilization techniques via real-time diagnostic ultrasound, while this review focuses at only clinical usage effects. Therefore, future studies can also fmd out whether neural mobilization is more likely to impose mechanical effects or neurophysiological effects on the neural tissue and the
nervous system.
References
1. Anne M.R. Agur, Arthur F. Dailey Il.Grant's atlas of anatomy thirteen edition. Wolthers Kluwer. 2013.
2. David S. Butler. Mobilisation of the nervous system. Churchill livingstone.1991.
3. Inman VT, Sunders J B. the clinic-anatomical aspects of the lumbosacral region. Radiology.1942.
4. Bowsher D. Introduction to the anatomy and physiology of the nervous system, 5th edition. Blackwell Oxford. 1988.
5. Millesi H. The nerve gap: theory and clinical practice. Hand clinics.1986.
6. Brieg A. Adverse mechanical tension in central nervous system. Almqvist& Wiksell, sockholm.1978.
7. Petty N J. Moore A P. Neuromusculoskeletal examination and assessment: A handbook for therapists. Churchill living stone. 2001.
8. A Kummatid, M markrat. Using the Systematic Review to Provide a Complete Summary on a Research Question in Evidence-Based Practice: A 3-Step Method. The Southern College Network Journal of Nursing and Public Health. 2016.
9. Chalmers I, Altman DG, Gotzsche PC. Systematic reviews: BMJ Publishing Group, London; 1995.
10. Murad MH , Montori VM , loannidis JP , Jaeschke R , Devereaux PJ , Prasad K , et al . How to read a systematic review and meta - analysis and apply the results to patient care: users ' guides to the medical literature. JAMA 2014; 312 (2):
171-9.
11. Aromataris E, Pearson A. The systematic review: an overview. Ans J Nurs 2014; 114 (3): 53-8.
12. Shacklock M. Clinical neurodynaics: a new system of musculoskeletal treatment. Elsevier.2005.
13. Nagrale AV , Patil SP , Gandhi RA , Learman K. Effect of slump stretching versus lumbar mobilization with exercise in subjects with non - radicular low back pain : a randomized clinical trial . J Man Manip Ther. 2012: 20:35-42.
https://doi.org/10.1179/20426186114.0000000015.
14. Patel G. To compare the effectiveness of Mulligan bent leg raising and slump stretching in patient with low back pain.
Indian J Physio ther Occup Ther.2014;8:24-28. https://doi.org/10.5958/0973-5674.2014.00350.5.
15. Mahmoud WS. Effect of neural mobilization versus spinal manipulation in patients with radicular chronic low back pain. Eur J Sci Res. 2015: 131: 122-132.
16. Mehta A. Mhatre B. Mote N. Effects of Maitland's joint mobilization versus Shacklock's neurody namic mobilization techniques in low back pain. Indian J Physiother Occup Ther. 2014; 8: 248-255. https://doi.org/10.5958/1.0973-
5674.8.2.094.
17. Kumar S. A prospective randomized controlled trial of neural mobilization and Mackenzie [sic] manipulation in cervical radiculopathy. Indian) Physiother Occup Ther. 2010; 4: 69-75.
18. Nar NH. Effect of neural tissue mobilization on pain in cervical radiculopathy patients. Indian J Physiother Occup Ther.
2014; 8: 144-148. https:// doi.org/10.5958/7.0973-5674.8.1.028.
19. Ragonese J. A randomized trial comparing manual physical therapy to therapeutic exercises, to a combination of therapies, for the treatment of cervical radiculopathy. Orthop Phys Ther Pract. 2009: 21: 71-76.
20. Marks M, Schottker - Koniger T. Probst A. Efficacy of cervical spine mobilization versus peripheral nerve slider techniques in cervicobrachial pain syndrome - a randomized clinical trial. J Phys Ther. 2011: 4: 9-17.
21. Bialosky,JE, Bishop MD, Price DD, Robinson ME, Vincent KR, George SZ. A randomized sham - controlled trial of a neurodynamic technique in the treatment of carpal tunnel syndrome. J Orthop Sports Phys Ther. 2009; 39:709-
723.https://doi.org/10.2519/ jospt.2009.3117.
22. Brininger TL, Rogers JC, Holm MB, Baker NA, Li ZM, Goitz RJ. Efficacy of a fabricated customized splint and tendon and nerve gliding exercises for the treatment of carpal tunnel syndrome: a randomized controlled trial. Arch Phys Med Rehabil. 2007; 88: 1429-1435. https://doi.org/10.1016/j. apmr.2007.07.019.
23. Heebner ML, Roddey TS. The effects of neural mobilization in addition to standard care in per sons with carpal tunnel syndrome from a community hospital. J Hand Ther. 2008; 21: 229-240;quiz241.
https://doi.org/10.1197/j.jht.2007.12.001
24. Horng YS, Hsieh SF, Tu YK, Lin MC, Honig YS, Wang JD. The comparative effectiveness of ten don and nerve gliding exercises in patients with carpal tunnel syndrome: a randomized trial. Am J Phys Med Rehabil. 2011; 90: 435-442.
https://doi.org/10.1097/PRM.0b013e318214eaaf.
25. Oskouei AE, Talebi GA, Shakouri SK, Ghabili K. Effects of neuromobilization maneuver on clinical and electrophysiological measures of patients with carpal tunnel syndrome. J Phys TherSci.2014;26:1017-1022.
https://doi.org/10.1589/ ipts.26.1017.
26. Pinar L, Enhos A, Ada S, Giingor N. Can we use nerve gliding exercises in women with carpal tunnel syndrome? Adv Ther. 2005; 22: 467-475. https://doi.org/10.1007BF02849867.
27. Dabholkar AS, Kalbande VM, Yardi S. Neural tissue mobilisation using ULTT2b and radial head mobilisation v I s exercise programme in lateral epicondylitis. Indian J Physio ther Occup Ther.2013;7:247-252.
https.://doi.org/10.5958/7.0973-5674.7.4.157
28. Vicenzino B, Collins. D, Wright A. The initial effects of a cervical spine manipulative physio therapy treatment on the pain and dysfunction of lateral epicondylalgia. Pain. 1996; 68: 69-74. https`//doi.org/10.1016/S0304-3959(96)03221-6.
29. Kavlak Y, Uygur F. Effects of nerve mobilization exercise as an adjunct to the conservative treat ment for patients with tarsal tunnel syndrome. J Manipulative Physiol Ther. 2011; 34: 441-448. https://doi.org/10.1016/j.jmpt.2011.05.017.
30. Saban 13, Deutscher D, Ziv T. Deep massage to posterior calf muscles in combination with neural mobilization exercises
as a treatment for heel pain: a pilot randomized clinical trial. Man Ther.2014;19:102-108.
https://doi.org/10.1016/j.math.2013.08.001
31. Scrimshaw SV, Maher CG. Randomized control trial of neural mobilization after spinal surgery. Spine (Phila Pa 1976).
2001; 26: 2647-2652.
32. Servernlov B, Larsson M, Rehn K, Adolfsson L. Conservative treatment of the cubital tunnel syndrome. J Hand Surg Eur Vol. 2009; 32: 991-1004.
33. Dabholkar AS , Kalbande VM , Yardi S. Neural tissue mobilisation using ULTT2b and radial head mobilisation v / s exercise programme in lateral epicondylitis . Indian J Physio ther OccupTher.2013;7:247-252. https://doi.org/10.5958 / 7.0973-5674.7.4.157.
34. Vicenzino B, Collins D, Wright A. The initial effects of a cervical spine manipulative physio therapy treatment on the pain and dysfunction of lateral epicondylalgia. Pain. 1996; 68: 69-74. https://doi.org/10.1016/S0304-3959(96)03221-6 35. David RS, Francisco US, Daneil LL et al. effectiveness of median nerve neuralmobilization versus oral ibuprofen
treatment in subjects who suffer from cervicobrachial pain: a randomized clinical trial. Arch Med Sci 2018; 14, 4: 871- 879.
36. Ragonese J. A randomized trial comparing manual physical therapy to therapeutic exercises, to a combination of therapies, for the treatment of cervical radiculopathy. Orthop Prac. 2009; 21 (3): 71-7.
37. David RS, Daniel LL, Francisco US et al. Effects of Median Nerve Neural Mobilization in Treating Cervicobrachial Pain: A Randomized Waiting List—Controlled Clinical Trial. Pain Practice, 2018 431-442. •
38. David RS, Ce sar CL, Francisco US et al. Cervical Lateral Glide Neural Mobilization Is Effective in Treating Cervicobrachial Pain: A Randomized Waiting List Controlled Clinical Trial. Pain Medicine 2017; 18: 2492-2503 doi:
10.1093/pm/pnx011.
39. Kim DG, Chung SH, and Jung HB. The effects of neural mobilization on cervical radiculopathy patients' pain, disability, ROM, and deep flexor endurance. Journal of Back and Musculoskeletal Rehabilitation 30 (2017) 951-959. DOI
10.3233BMR-140191.
40. Nishant H N. Effect of Neural Tissue Mobilization on Pain in Cervical Radiculopathy Patients. Indian Journal of Physiotherapy & Occupational Therapy. 2014:144-149. DOI Number: 10.5958/j.0973-5674.8.1.028
41. Rohini G, Shallu S. Effectiveness of median nerve slider's neurodynamics for managing pain and disability in cervicobrachial pain syndrome. Indian Journal of Physiotherapy & Occupational Therapy. 2012:127-133.
42. Shareen A, Arshad NM, Imran A. Effectiveness of neuromobilization in patients with cervical radiculopathy. Rawal med Jour, 2015: 34-36.
43. Butler DS. The Sensitive Nervous System. Adelaide, Australia: Noi group Publications, 2000.
44. Shacklock MO. Neurodynamics. Physiotherapy 1995; 81: 9-16.
45. Shacklock MO. Clinical applications of neurodynamics. In: Shacklock MO, ed . Moving in on Pain. Chatswood, UK:
Butterworth - Heinemann, 1995: 123-131.
46. Shacklock MO. Clinical Neurodynamics: A Butterworth Heinemann, 2005.
New System of Neuro musculoskeletal Treatment. Oxford, UK: