Copyright © 1985 by The Johns Hopkins University School of Hygiene and Public Health Printed in U.SA. All rights reserved
THE STANFORD FIVE-CITY PROJECT: DESIGN AND METHODS JOHN W. FARQUHAR,1 STEPHEN P. FORTMANN,1 NATHAN MACCOBY,1 WILLIAM L. HASKELL,1 PAUL T. WILLIAMS,1 JUNE A. FLORA,1 C. BARR TAYLOR,1 BYRON W.
BROWN, JR.,1 DOUGLAS S. SOLOMON,1 AND STEPHEN B. HULLEY3 Farquhar, J. W. (School of Medicine, Stanford U., Stanford, CA 94305), S. P. Fortmann, N. Maccoby, W. L Haskell, P. T. Williams, J. A. Flora, C. B. Taylor, B. W. Brown, Jr., D. S. Solomon, and S. B. Hulley. The Stanford Five-City Project design and methods. Am J Epidemiol 1985; 122:323-34.
The Stanford Five-City Project is a large experimental field study of community health education for the prevention of cardiovascular disease. It will provide data on fundamental questions in cardiovascular disease epidemiology, communica- tion, health education, behavior change, and community organization, and will also test the ability of a potentially cost-effective program to prevent cardiovas- cular disease at the community level. This paper describes the purposes, hy- potheses, design, and methods of the Five-City Project as a reference for future papers describing results. It is hypothesized that a 20% decrease in cardiovas- cular disease risk will lead to a significant decline in cardiovascular disease event rates in two treatment communities compared with three reference com- munities as a result of a six-year intervention program of community-wide health education and organization. Risk factor change will be assessed through four surveys of independent samples and in a repeatedly surveyed cohort Cardio- vascular disease event rates will be assessed through continous community surveillance of fatal and nonfatal myocardial infarction and stroke.
cardiovascular diseases; health education; primary prevention; survey methods
The Stanford Five-City Multifactor Risk of cardiovascular disease epidemiology has Reduction Project is a nine-year field trial been linked to several large, prospective of the community control of cardiovascular longitudinal studies of the distribution and disease. This trial extends the scope and determinants of cardiovascular disease in objectives of the earlier Stanford Three- defined populations. These studies have Community Study (1, 2) through the use of elucidated several consistent and impor- community organization and the inclusion tent pe r 8 O n al characteristics that relate to of independent population surveys and car- i n c r e a s e d r i s k o f subsequent cardiovascular diovascular disease incidence surveillance. ^ ^ T h e s e f a c t o r s i n d u d e elevated a r.
For over three decades, the development terifll b l o o d p r e s s u r e j c i g a r e t t e 8 m o k i n g i el- Receivedfor publication May 30,1984, and in final e V f l t e d
Pl f l S m a
cholesterol, obesity, physical form December 4,1984. inactivity, and Type A behavior (3-7). As
1 Stanford Center for Research in Disease Preven- the associations between these risk factors tion, Stanford University School of Medicine, Stan- j j - i j - u ± u ford, CA 94305. (Reprint requests to Dr. John W. a n d cardiovascular disease became estab- Farquhar.) lished, there was a logical progression from j Apple Computer Inc., Cupertino, CA. observational to experimental studies de-
Department of Epidemiology and International .
Health, School of Medicine, University of California, Signed to Strengthen the causal inferences San Francisco, CA. between identified risk factors and cardio-
J S S Zrrun^
ydBC.
HL
2iS
fNa
r avascular disease and to test the feasibility
tional Institutes of Health. of cardiovascular disease prevention 323
through modifying these risk factors. It has not been possible to conduct experimental trials for all risk factors. For example, the causal relationship between blood pressure and cardiovascular disease is well estab- lished (8-10), but a clinical trial of cigarette smoking would not be ethical and experi- mental tests of the diet-heart theory proved economically infeasible (11). Progress has been made through several recently com- pleted cardiovascular disease prevention trials such as the Lipid Research Clinics Coronary Primary Prevention Trial (12, 13) and the Multiple Risk Factor Interven- tion Trial (14). Begun before these latter studies were completed, the Stanford Five- City Project and sister projects in Minne- sota (15) and Rhode Island (16) comple- ment these other trials. In a search for generalizability of findings, including methods of achieving change, it will be instructive to compare these US commu- nity studies to a number of ongoing or recently completed community-based stud- ies in Europe, Africa, and Australia (17, 18). We have previously compared the de- signs and complementary contributions of the Coronary Primary Prevention Trial, the Multiple Risk Factor Intervention Trial, and the Five-City Project (11).
The Stanford Five-City Project is also a natural outgrowth of the previous work of the Stanford Heart Disease Prevention Program, an interdisciplinary group of medical, communication, and education scientists and professionals. This group was established in 1971 principally to conduct the Stanford Three-Community Study. In the Three-Community Study, the Stanford Heart Disease Prevention Program dem- onstrated the potential for community- wide risk reduction through a program of education carried out principally through mass media in two towns, supplemented by a face-to-face program of intensive instruc- tion for high risk individuals in one of the towns. The third town served as a refer- ence. Although there were limitations in the design of that study, the results suggest
that community health status can be im- proved by an educational program delivered through media and interpersonal channels (1, 2,19-22). Comparable changes occurred in cardiovascular disease risk factors in the similar Finnish North Karelia project, which also began in 1972 and recently re- ported its 10-year follow-up results (17, 23). The Five-City Project differs from the Three-Community Study in that in the for- mer the two communities selected for edu- cation are much larger and more socially complex; the education is more extensive; there are three reference cities rather than one; the education period of the Project will run for six years rather than three; the effects of the intervention will be moni- tored in a wider age range; and the change in cardiovascular disease event rates will be measured. These topics are discussed fur- ther below.
HYPOTHESES
There are two major hypotheses to be tested in the Five-City Project. First, that community-wide education can achieve a lasting reduction in the prevalence of car- diovascular disease risk factors within a general population, leading to a 20 per cent decline in the Framingham multiple logistic measure of risk (24) in representative sam- ples of persons aged 12 to 74. The second hypothesis is that this risk decline will lead to a decline in cardiovascular disease mor- bidity plus mortality in persons aged 30-74 that is significantly greater in the education cities than in reference cities. Given the long preclinical phase of cardiovascular dis- ease, only the risk factor hypothesis is rel- evant to young people.
A test of these hypotheses will require the development of cost-effective and gen- eralizable methods for organizing and edu- cating communities toward prevention and control of chronic diseases. The education program will attempt to achieve a 20 per cent reduction in overall risk in the treat- ment population compared with the refer- ence communities, through a 9 per cent
reduction in cigarettes smoked per day, a 2 per cent change in relative weight, a 7 per cent reduction in systolic blood pressure, and a 4 per cent reduction in total plasma cholesterol. The education program's sec- ondary goal is to create a health promotion structure within the communities that will continue to function after the Project ends. An additional purpose of the Five-City Project is to analyze the secular trends in cardiovascular disease risk factors, morbid- ity, and mortality during a time of declining cardiovascular disease mortality, the cause of which is uncertain. Also, the survey data collected will allow the testing of numerous hypotheses relating to cardiovascular dis- ease epidemiology, behavioral medicine, community organization, physiology, and communication science. Table 1 displays our study's presumed linkage of the inde- pendent variable (the interventions) to the dependent behavioral and physiologic and cardiovascular disease event variables.
DESIGN
Experimental design
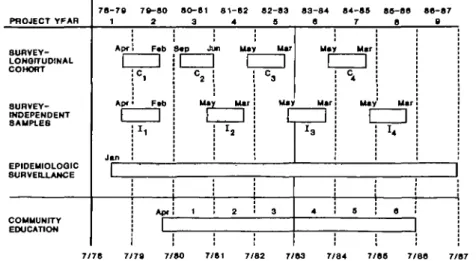
The overall design of the Five-City Proj- ect is illustrated in figure 1. The education program will last six years and was intro- duced after the completion of a baseline population survey. The effect of education
on reducing risk factors will be assessed by comparing the results of the four independ- ent sample surveys in the two treatment communities with the results of these sur- veys in two of the three reference commu- nities. The original independent sample in each community will be resurveyed three times to allow an evaluation of the process of behavior change in this group. Epidemi- ologic surveillance of cardiovascular disease morbidity and mortality occurs in all five cities and will span at least nine years.
City selection
The ideal study design for evaluating the efficacy of comprehensive community- based health education would entail ran- dom assignment of a large number of communities to the treatment and control conditions. The simpler design of five non- randomly assigned cities was chosen be- cause of limited resources and the extensive overlap of media markets in California. The selection of cities was subject to several constraints, including: 1) location in north- ern California, 2) populations exceeding 30,000, 3) total population of the five cities exceeding 300,000 to provide sufficient sta- tistical power to the experiment, 4) reason- able similarity of ethnic, socioeconomic and demographic characteristics, 5) relative
TABLE 1
Goals, intervention topics, and outcome measures of the Stanford Five-City Project Risk category goals Intervention
topics
Behavioral
measures Physiologic measure,. Smoking
Exercise Diet Body weight Blood pressure
Awareness Information Skills training Motivation Maintenance Community
organiza- tion
Attitude Knowledge Diet Exercise Smoking Stress Communica-
tion flow Organizational
behavior
Obesity Plasma choles-
terol Plasma HDL-C Plasma thiocya-
nate Expired air CO Arterial blood
pressure Fitness
Urinary Na+, K+
Total mortality Fatal MI Fatal CHD Nonfatal MI Fatal stroke Nonfatal
stroke
* HDL-C, high density lipoprotein cholesterol; thiocyanate and expired air CO (carbon monoxide) are indirect measures of smoking behavior, urinary Na+ (sodium) and K* (potassium) are measures of dietary intake of these substances.
t MI, myocardial infarction; CHD, coronary heart disease.
PROJECT YFAR
8UHVEY- LONQrrUDINAL COHORT
SURVEY- INDEPENDENT SAMPLES
EPIDEHIOLOQIC SURVEILLANCE
COMMUNITY EDUCATION
7 8 - 7 8 1
Apr
Apr
Jan
1
7 8 - 8 0 2
Fab
C,
Ftt)
Apr 80-81
3
C2
Maj
1
r
81-82 4
m Ma)
c
Mar
h
2
82-83 S
Mar
C3
Mai
r
3
83-84 8
Mai
Mar
J3
4
84-88 7
Mar
C4
May :
88-88 8
Mar
8
88-87 8
1
7/80
FIGURE 1. Design of the nine-year Stanford Five-City Project, 1978-1987. The time sequence of surveys, epidemiologic surveillance and community education is displayed.
independence from other cities (eliminat- ing suburbs of larger metropolitan areas), 6) no shared newspaper or electronic media markets between treatment and control cities, 7) shared media markets between treatment cities (to decrease costs), 8) rel- ative independence of the two treatment cities, despite allowance of some shared media services. We performed a formal se- lection search of all California cities and could not avoid nonrandom selection for our final city choices.
EDUCATION METHODS
In the vernacular of clinical trials, the Community Education Program is the "in- tervention" or "treatment" and is described in this section. However, the Community Education Program has purposes which are independent of its role in the Five-City Project intervention. The education com- ponents are complex and interrelated, and attempts to describe them may result in oversimplification and underemphasis of their interaction. With this caveat, the basic theoretical perspectives are outlined below, followed by a discussion of the media and community programs, and the forma- tive research methods.
Theoretical perspectives
Planning complex community-based studies is assisted by using clear theoretical
guidelines. Many theories of learning are available (25, 26) and a variety of theoret- ical bases for community change also exist (27, 28). The need to reach individuals and to collaborate with (and change) commu- nity institutions requires insights from both sources. We have attempted to com- bine the theoretical foundations for com- munity organizational change with the par- ticular needs of the Project as "community organization for health." Our "health com- munication-behavior change" framework guides the creation of specific educational programs and materials. It is challenging to attempt to link these two widely diver- gent perspectives into a comprehensive community education program and the lit- erature provides little firm guidance. We have recently reported on these theoretical guidelines for community-based health ed- ucation in detail (18).
Media programs
Media programs form a major proportion of the educational effort in the Five-City Project. Education delivered through tele- vision and radio is designed primarily to deliver information that will affect the at- titudes, knowledge, and motivation of in- dividuals within the community. Print me- dia (newspapers, books, pamphlets, etc.)
can provide more information than televi- sion or radio and therefore better skills training. Print media products are distrib- uted through direct mail and through exist- ing organizations, including worksites and medical care providers.
Several continuing television formats were created and will continue in use. These are usually developed in collabora- tion with local television stations. The ed- ucation program began with the airing (in April 1980) of an hour-long "Heart Health Test" which provided general risk reduc- tion information. Some 6-10 additional, shorter programs have been or will be de- veloped. Four of these began as a series of short segments (3-5 minutes) on a local news program and covered smoking cessa- tion, cooking, and exercise and weight con- trol. Another principal use of television is for public service announcements, about 100 of which will be used during the study. The primary use of radio is also for brief announcements and short programs (of five-minute duration). Radio production has concentrated on Spanish-language pro- grams since this is a major information source for Mexican-Americans.
Since considerable complex information must be communicated, print materials are important. A weekly newspaper column in both English and Spanish is a major com- ponent of the print program. In addition, a series of booklets and other print materials are in use or planned. For example, we have developed two "Kits" for smoking cessation and nutrition change that have been shown to be cost-effective (29). By the end of the fourth year of education, every household in the two education communities will have received at least four print products and we will have distributed over 100,000 booklets and pamphlets and larger numbers of less expensive print materials.
Community programs
Some project goals for early extensive impact can be most rapidly achieved through creating media materials and ac-
tivities that rely almost entirely on Stan- ford Heart Disease Prevention Program re- sources. However, as the overall education program matures, an increasing proportion of media products and activities will rely on community resources for collaborative production and distribution. Community programs that involve interpersonal con- tact, such as classes, seminars, and other group interventions, rely more heavily on community resources from the beginning and are essential for achieving the long- term goal of maintenance of behavior change.
Our strategy requires that the design of such programs be interactive, combining theoretical and scientific input from the university with practical input from the community. The general goals, appropriate audience, and content of a program are initially defined by Stanford Heart Disease Prevention Program staff while appropri- ate community resources are sought. A col- laboration is then established that rede- fines the program and establishes its place in the community. After program materials are pretested, implementation begins by re- cruiting and training leaders and then in- troducing the program. Extensive evalua- tion of the early experience leads to refine- ment of the program. Finally, the program is expanded by recruiting additional orga- nizational sponsors, training a director and obtaining financial support. The end result is a locally-controlled program with contin- uing links to the Stanford Heart Disease Prevention Program.
Our community interpersonal programs are delivered through the health depart- ment, community colleges, schools, volun- tary and ad hoc organizations, voluntary health agencies, health professionals, hos- pitals and other nonprofit health service agencies. Some programs can be designed to be delivered in several settings and con- texts (e.g., smoking cessation), while others must be designed specifically for the spon- soring organization (e.g., school curricula and health professional activities).
Formative research methods Formative research (or formative evalu- ation) provides data for designing educa- tional programs and materials to meet specific objectives and for monitoring the progress of the educational program. For example, prior to broadcasting a television program, one must know whether the in- tended audience watches television at the time of the broadcast, whether the content is understandable and relevant, and whether the content is likely to stimulate action. After broadcast, audience size and impact should be evaluated and compared to expectations. The same process is valu- able for planning print materials and com- munity programs where similar questions of audience size, comprehension, retention, and behavior change occur. Health com- munication campaigns have been criticized for a lack of formative research (30), which results in materials and programs that are often unable to meet the campaign objec- tives.
Formative research begins with a clear definition of objectives, including the in- tended audience and the change to be achieved (increased knowledge, use of a new recipe, etc.). The next stage is "concept testing." (For example, do people use cook- books to obtain new recipes or do they obtain them from other sources?) Next, the specific content and format are evaluated for clarity and effectiveness. After mate- rials are introduced, they are "tracked" to see if they reach the intended audience and are effective. We employ a social marketing model (31) to guide our formative research. Formative research uses largely familiar methods for these specific purposes, such as personal and telephone surveys of rep- resentative populations or of small, well- defined subgroups. These methods can rarely provide rigorous data on the effect of various programs on behavior since they must rely largely on self-report. We there- fore supplement them with small-scale con- trolled comparisons of appropriate mate- rials (e.g., different approaches to smoking
cessation) (32). Finally, each educational program is monitored for the number of times it is used, the number of people reached, and the best possible measure of behavior change.
EVALUATION METHODS
Surveys
Population surveys of health behavior and cardiovascular disease risk factors are conducted by full-time Five-City Project staff at permanent survey centers in four of the five cities. Each center is staffed by a nurse/supervisor, an interviewer/abstrac- tor, a laboratory technician, and a medical office assistant. Initial contact is by letter and subsequent telephone call. Home visits are made when necessary for recruitment, but all survey data are collected in the survey center. People who refuse partici- pation are asked to answer by telephone a few questions on age, education, body weight, and smoking status to enable com- parison with the participant groups.
City directories of households published by R. L. Polk were found to provide a relatively complete listing of households in each community (approximately 97 per cent complete) and are revised every two years. All individuals 12 to 74 years of age who reside in randomly selected households at least six months of the year are eligible for the surveys, are invited to participate, and are included in the denominator for calculation of participation rates.
There are two main types of samples included in the surveys: a longitudinal co- hort sample and independent samples. In the initial year of the survey, about 625 people in each community visited the sur- vey centers, comprising the first independ- ent sample. These individuals are invited to participate in subsequent surveys every two years in order to study the process of change in cardiovascular risk and related behaviors over time. Second, third and fourth independent samples will be sur- veyed over the last six years of the project to study cross-sections of the community
329 over time without the potentially confound-
ing effects of repeated measurements. The overall study design can be found in figure 1.
Behavioral measures. The chief sources of data on health-related behaviors are the questionnaires and dietary measures. The core questionnaire consists of the following components: demographic measures; atti- tude and opinion measures; health knowl- edge assessment related to prevention of heart disease and stroke; stress behavior; diet/nutrition and weight behavior; smok- ing behavior, physical activity behavior (33); communication media use and inter- personal communication network analysis; and medical history including medication use. Finally, a random 50 per cent of the participants is given a 24-hour dietary re- call aided by food models to illustrate size, weight or volume of foods.
Physiologic measures. Weight is obtained to the nearest \ lb (0.1 kg) by a balance scale and height to the nearest \ inch (0.6 cm) by metal rule. Nonfasting venous sam- ples are obtained from participants while seated. The refrigerated plasma samples are shipped to Stanford twice each week and are analyzed fresh for lipids and lipo- proteins by long-established methods of the Lipid Research Program (34). Plasma thi- ocyanate is determined on frozen plasma by the procedure of Butts et al. (35). Ex- pired air carbon monoxide, another index of cigarette use, is measured on the Ecoly- zer apparatus (Energetics Science, Inc., New York, NY). A plasma sample is taken in a sealed Wheaton vial for contingency purposes and is stored at —80 C. The frozen samples are shipped to Stanford monthly.
Blood pressure is obtained as indirect brachial artery pressure (systolic and fifth- phase diastolic) on participants sitting at rest for two minutes before the first meas- urement (and before venipuncture). Pres- sures are obtained using a Sphygmetrics Infrasonic Automatic Blood Pressure Re- corder, SR-2 (Puritan-Bennett, Los Ange- les, CA) (36); this is followed by dual meas-
urements of pressure using a standard mer- cury sphygmomanometer and auscultation. The auscultation procedures are reviewed twice yearly and each auscultator is com- pared with a single trainer to maintain reliability.
Urine samples are frozen after collection and shipped monthly to Stanford. Standard laboratory procedures are used for deter- mination of urinary sodium and potassium (flame photometry), and creatinine.
A low-level exercise test, using a Schwinn Electric Brake Stationary Bicycle (Schwinn, Chicago, IL) is performed fol- lowing blood pressure measurement and blood sampling. Measurements are made of pulse rate using a Cardiotachometer (Quin- ton Instrument, Seattle, WA). A proportion of participants is excluded from the test for medical reasons according to conservative criteria. The test is designed to obtain a pulse rate index of relative fitness when a standard work load estimated at 70 per cent of maximum aerobic capacity is performed.
Epidemiologic surveillance The purpose of community epidemiologic surveillance is to allow the calculation of comparable, city-specific rates for total and cardiovascular disease mortality, fatal and nonfatal myocardial infarction, and fatal and nonfatal stroke in each of the five communities included in the study. The mortality rates mentioned are obtainable from vital statistics, but these rely on the unaided interpretation of death certificate diagnoses. The morbidity rates could be determined by repeated examination of a large cohort of individuals, but such cohort studies are expensive. Thus the needed mortality statistics are available inexpen- sively, but their accuracy is suspect, and the morbidity data are not routinely avail- able except at great expense. Community surveillance is designed to obtain accurate mortality statistics and to obtain morbidity statistics at an acceptable cost (37).
Each community is defined with the use of census tracts so that accurate estimates
of the population at risk, and its age/sex structure, can be extrapolated from the 1980 Census. We will also use the 1985 California State special census for these data when available. Detailed address lists were created at the beginning of the project from maps, planning documents, and direct exploration. These lists are used by the field staff to determine eligibility on death cer- tificates and in hospital records.
We monitor only those nonfatal cardio- vascular disease events that result in hos- pitalization. In the United States it is im- practical to rely on physician-reporting for determining the incidence of cardiovascular disease events that do not require hospital- ization (such as the onset of angina or congestive heart failure). Myocardial in- farction and stroke almost always result in hospitalization when they come to medical attention.
In cooperation with other investigators in the United States and Europe, a standard set of criteria was developed for each type of event. These criteria accom- modate variations in physician diagnostic style and they allowed us to obtain com- parable data among different communities. Each case is categorized as definite, possi- ble, or no event. The definite category is rigorous and narrow, and thus highly spe- cific but insensitive. The possible category is quite broad—that is, sensitive but not specific. By examining secular trends in the proportion of total events which are defi- nite, we will be able to estimate the poten- tial for bias from changes in physician diagnostic habits (e.g., completeness of en- zyme determinations in suspected myocar- dial infarction cases). The criteria are avail- able from the authors.
We identify fatal cases through the county death certificate files. Deaths occur- ring both within and outside of California are reported to the decedent's residence county by the state. Thus case finding for fatal cases will be nearly complete. All death certificates are reviewed by a trained abstractor who lists all age- and address-
eligible deaths. Those deaths which are pos- sibly due to cardiovascular disease are fur- ther investigated as detailed below. Non- fatal case identification is performed by reviewing hospital discharge indices for cardiovascular disease and related diag- noses. Again, each age- and address-eligible case is investigated further. Seventeen hos- pitals are involved in this data collection system.
Fatal events are classified as hospital and nonhospital cases, the latter including deaths occurring in emergency rooms. We currently have access to all coroner's rec- ords involved, and obtain copies of all au- topsies performed. All nonhospital deaths, both coroner's cases and others, are further investigated by contacting the decedent's family for the medical history and the cir- cumstances of death. A questionnaire is also sent to the decedent's physician to obtain medical information. Hospitalized deaths are investigated by review of the chart and a family interview is performed only when necessary. All nonfatal cases are investigated by review of the chart, during which an abstract of the case history, lab- oratory data, consultations, and other per- tinent information is made. Electrocardio- grams are photocopied.
All abstracted cases are submitted to the Stanford Five-City Project where they are given an identification number. All per- sonal identification data and any informa- tion that might identify the community are concealed. A computer case file is created and a matching program compares the per- sonal identification data with the data from previous events in order to link all events in the same individual. Next, the computer generates a validation form containing per- tinent medical information but no infor- mation about the community or the indi- vidual (except age and sex). Each event is then reviewed independently by two re- search nurses who have training in cardio- vascular disease diagnosis. These surveil- lance analysts determine whether or not each diagnostic criterion has been met.
331 Each analysis is entered into the computer
file and the criteria are applied automati- cally to obtain a single endpoint determi- nation. If the two endpoints do not match, the case is reviewed by a physician. Confi- dentiality is maintained at all times.
ANALYSES
The nonrandom allocation of the five cities to treatment and control conditions, while necessary for practical reasons, im- poses some uncertainties on the interpre- tation of results (38, 39). Reduction of un- certainty is possible with a multiopera- tional approach to analysis, each approach emphasizing particular aspects of the data and requiring different assumptions. We have discussed these approaches in more detail elsewhere (20, 40).
The principal questions to be addressed in the analysis of the data obtained by the Five-City Project are listed below: a) What is the efficacy of the education program, and which elements appear to be most ef- fective, in reducing cardiovascular disease risk factors? b) Is there a cardiovascular disease morbidity and mortality difference between education and reference cities? c) Given study outcomes, and considering the relevant cost of the research components compared with the education component, what data can be provided to assess the costs of replications of the risk reduction strategy elsewhere?
We will test the efficacy of the education program in reducing cardiovascular disease risk by comparing changes in risk factor levels observed in the independent sample surveys between the treatment and control cities. Two approaches will be considered for evaluating the statistical significance of the treatment versus control group differ- ences. The first evaluates the differences between total samples for treated and con- trol cities at baseline and each follow-up survey by a two-sample t test. Table 2 lists differences in risk factors and in the mul- tiple logistic index of cardiovascular disease risk (24) among independent samples
needed to detect significant changes over time, employing a one-tailed test for signif- icance and assuming an alpha of 0.05 and a beta of 0.1. These detectable changes are comparable to our intended changes (see hypotheses) and are based on the results of the first two independent samples. A major limitation of the independent sample is its inclusion of individuals who have recently migrated into the community and who are sampled without having received full ex- posure to education. In addition, the pro- cess of change within individuals cannot be evaluated from the independent sample. For these reasons, we will also analyze risk change in the members of the original base- line survey who remain in the area through- out the study (the cohort). Table 3 shows the (smaller) changes in outcome variables that will be detectable in the cohort (alpha 0.05, beta 0.1) when individual change scores are contrasted between treatment and control groups. Enhanced power to de- tect change is therefore achieved in the cohort sample by controlling for each indi- vidual's baseline level. It is important to recognize, however, that risk factor changes in longitudinally measured individuals may not parallel changes among individuals not in the cohort due to sensitization from the measurement process itself (especially in the treatment group). Further refinement of the above comparison will be achieved through analysis of covariance to minimize baseline group differences with respect to demographic parameters and other baseline variables.
The above approach based on a two- sample t statistic assumes that individuals are randomly assigned to communities and therefore ignores the between-community variation. However, virtually all of the risk factors exhibit significant variation among communities (even after adjustment for de- mographic characteristics) so that a statis- tical test which uses the individual as the experimental unit may provide overly op- timistic significance levels (41). We will therefore use a second statistical approach
TABLE 2
Baseline mean values and power calculations for changes in cardiovascular risk factors as per cent of baseline between the independent samples of the treatment and control groups (a = 0.05, 0 = 0.10, 1-tailed test): the
Stanford Five-City Project
Systolic pressure (mmHg) Diastolic pressure (mmHg) Plasma total cholesterol (mg/dl) Plasma triglycerides (mg/dl) Plasma HDL-cholesterol§ (mg/dl) Plasma LDL-cholesterol § (mg/dl) Quetelet's index (kg/cm1 X 1,000) Cardiovascular disease risk (12-year
probability)^ Smokers (%)
Cardiovascular health knowledge (32 patients)
Baseline mwint
121.58 74.67 190.57 136.49 53.61 110.63 2.37
0.062 30.00
10.30
Detectable difference* In units as measured
2.98 2.07 7.40 23.25 2.56 6.09 0.071
0.011 8.00
0.84
As % of baseline -2.5 -2.8 -3.9 -17.0 +4.8 -5.5 -3.0 -17.8 -25.3 +8.2
* Assumes a sample size of 1,200 individuals in each group at each survey, 12-74 years old. The detectable difference is 5.86 times the standard error of the mean for a sample of 1,200 individuals estimated from the total baseline sample.
t Baseline mean for all 2,482 individuals with complete data.
t Age- and sex-adjusted risk scores for 1,000 individuals per community, 19 years and older.
§ HDL-cholesterol, high density lipoprotein cholesterol; LDL-cholesterol, low density lipoprotein cholesterol.
TABLE 3
Baseline mean values and power calculations for changes in cardiovascular risk factors as per cent of baseline between the cohort samples of the treatment and the control groups (a = 0.05, 0 «= 0.10, 1-tailed test): the
Stanford Five-City Project
Systolic pressure (mmHg) Diastolic pressure (mmHg) Plasma total cholesterol (mg/dl) Plasma triglycerides (mg/dl) Plasma HDL-cholesterolt (mg/dl) Plasma LDL-cholesterolJ (mg/dl) Quetelet's index (kg/cm* x 1,000) Cardiovascular disease risk (12-year
probability)t Smokers (%)
Cardiovascular health knowledge (32 patients)
BflSClinC mfffln
122.90 75.78 196.18 142.89 54.79 114.26 2.39
0.070 26.68
11.12
Detectable difference* In units as measured
2.51 1.90 4.82 28.00 2.14 4.34 0.032
0.009 4.72
0.65
As % of baseline - 2 . 0 - 2 . 5 - 2 . 5 - 1 9 . 6 +3.9 - 3 . 8 - 1 . 3
-12.9 -17.7
+5.8
* Assumes a cohort sample size of 600 individuals in each group, 12-74 years old, with complete data at baseline and the final follow-up cohort survey. Detectable difference is 2.93 times the standard error for the difference in the change scores between treatment and control groups actually observed between the first and third cohort surveys.
t Assumes a sample size of 500 individuals in each group, 19-74 years old, with complete data at baseline and at the follow-up study.
X HDL-cholesterol, high density lipoprotein cholesterol; LDL-cholesterol, low density lipoprotein cholesterol.
which recognizes the community as the unit of intervention to complement the t tests based on individuals.
The second approach employs a regres- sion analysis of the independent sample data that estimates statistical error from time by town variation. Separate regression lines are fitted to the four means of the independent samples for each community and a test is then performed to determine whether the average of the two treatment city slopes is significantly different from the average of the two control city slopes. This comparison will involve a t test with eight degrees of freedom. The method has been used successfully in analyzing our Three-Community Study results (20). Co- variance adjustment for baseline differ- ences will also be used at this level of anal- ysis.
To assess the effect of education on total cardiovascular disease event rates, we will make age- and sex-adjusted comparisons between event rates in the pooled treat- ment and control site populations, with all five communities contributing data. We will examine age- and sex-specific event rates in the treatment population and the control population using standard binomial or Poisson procedures to determine the ef- fect of treatment on event rates. These procedures will allow us to adjust for de- mographic differences among the treat- ment and control populations. This basic form of analysis will be conducted with pooled populations and combined event rates, as indicated above. But it will also be conducted with total mortality, each sepa- rate kind of cardiovascular disease event, and each different study site. Since our estimates of sample size requirements are based on pooled population and combined events, we expect these supplementary analyses only to suggest ideas about differ- ences between sites or differential effects on certain types of events.
We plan to supplement the above anal- ysis with a comparison of temporal trends in yearly cardiovascular disease event rates
in the treatment and reference sites. Our statistical methods for that time series will be based on regression methods for com- paring slopes based on a relatively small set of points in time as described above for risk factor means in the four survey com- munities. We will also use retrospective data on total (unverified) coronary heart disease death rates in the years preceding this study to examine the degree to which divergence from pre-existing trends are produced in the treatment sites.
So that the results of this research proj- ect will be useful for policy-makers, we are collecting data on the cost of education as well as its effects, allocating the costs to the specific categories of the Project.
REFERENCES
1. Farquhar JW, Maccoby N, Wood PD, et al. Com- munity education for cardiovascular health. Lan- cet 1977;l:1192-5.
2. Maccoby N, Farquhar JW, Wood PD, et al. Re- ducing the risk of cardiovascular disease: effects of a community-based campaign on knowledge and behavior. J Community Health 1977;23:10O- 14.
3. Dawber TR. The Framingham Study—the epide- miology of atherosclerotic disease. Cambridge, MA: Harvard University Press, 1980.
4. The Pooling Project Research Group. Relation- ship of blood pressure, serum cholesterol, smoking habit, relative weight and ECG abnormalities to incidence of major coronary events: final report of the Pooling Project. J Chronic Dis 1978;31:201- 306 (AHA Monograph no. 60).
5. Paffenbarger RS Jr, Hale EW. Work activity and coronary heart mortality. N Engl J Med 1975;292:545-50.
6. Paffenbarger RS Jr, Wing AL, Hyde RT. Physical activity as an index of heart attack risk in college alumni. Am J Epidemiol 1978;108:161-75. 7. Cooper T, Detre T, Weiss SM, et al. Coronary
prone behavior in coronary heart disease: a critical review. Circulation 1981;63:1200-15.
8. Veterans Administration Cooperative Study Group on Antihypertensive Agents. Effects of treatment on morbidity in hypertension. I. Results in patients with diastolic blood pressures averag- ing 115 through 129 mm Hg. JAMA 1967;202:116- 22.
9. Veterans Administration Cooperative Study Group on Antihypertensive Agents. Effects of treatment on morbidity in hypertension. II. Re- sults in patients with diastolic blood pressures averaging 90 through 114 ramHg. JAMA 1970:213:1143-52.
10. Hypertension Detection and Follow-up Program Cooperative Group: Five-year findings of the hy- pertension detection and follow-up program. 1.
FARQUHAR ET AL. Reduction in mortality of persons with high blood
pressure, including mild hypertension. JAMA 1979;242:2562-71.
11. Hulley SB, Fortmann SP. Clinical trials of chang- ing behavior to prevent cardiovascular disease. In: Weiss SM, Herd JA, Fox BH, eds. Perspectives on behavioral medicine. New York, NY: Academic Press, 1981:89-98.
12. Lipid Research Clinics Program. The Lipid Re- search Clinics coronary primary prevention trial results. I. Reduction in incidence of coronary heart disease. JAMA 1984;251:351-64.
13. Lipid Research Clinics Program. The Lipid Re- search Clinics coronary primary prevention trial results. II. The relationship of reduction in inci- dence of coronary heart disease to cholesterol lowering. JAMA 1984;251:365-74.
14. Multiple Risk Factor Intervention Trial Research Group. Multiple Risk Factor Intervention Trial Risk factor changes and mortality results. JAMA 1984;248:1465-77.
15. Blackburn H, Leupker RV, Kline FG, et al. The Minnesota Heart Health Program: a research and demonstration project in cardiovascular disease prevention. In: Matarazzo JD, Miller NE, Weiss SM, et al., eds. Behavioral health: a handbook of health enhancement and disease prevention. Sil- ver Spring, MD: John Wiley, 1984:1171-8. 16. Lasater T, Abrams D, Artz, L, et al. Lay volunteer
delivery of a community-based cardiovascular risk factor change program: The Pawtucket Experi- ment. In: Matarazzo JD, Miller NE, Weiss SM, et al., eds. Behavioral health: a handbook of health enhancement and disease prevention. Silver Spring, MD: John Wiley, 1984:1166-70. 17. Puska P, Tuomilehto J, Salonen JT, et al. Ten
years of the North Karelia Project: results with community-based prevention of coronary heart disease in Finland. Scand J Soc Med 1983;11:65- 8.
18. Farquhar JW, Maccoby N, Wood PD. Education and communication studies. In: Holland WW, Detels R, Knox G, eds. Oxford textbook of public health. London: Oxford Medical Publications (in press).
19. Meyer AJ, Nash JD, McAlister AL, et al. Skills training in a cardiovascular health education cam- paign. J Consult Clin Psychol 1980;48:129-42. 20. Williams PT, Fortmann SP, Farquhar JW, et al.
A comparison of statistical methods for evaluating risk factor changes in community-based studies: an example from the Stanford Three Community Study. J Chronic Dis 1981;34:565-71.
21. Fortmann SP, Williams PT, Hulley SB, et al. Effect of health education on dietary behavior The Stanford Three Community Study. Am J Clin Nutr 1981;34:2030-8.
22. Fortmann SP, Williams PT, Hulley SB, et al. Does dietary health education reach only the priv- ileged? An answer from the Stanford Three Com- munity Study. Circulation 1982;66:77-82. 23. Puska P, Tuomilehto J, Salonen J, et al. The
North Karelia Project: evaluation of a comprehen- sive community programme for control of cardio- vascular diseases in 1972-77 in North Karelia,
Finland. Copenhagen; Public Health in Europe, WHO/EURO Monograph Series, 1981.
24. Truitt J, Cornfield J, Kannel W. Multivariate analysis of the risk of coronary heart disease in Framingham. J Chronic Dis 1967;20:511-24. 25. Bandura A. The self system in reciprocal deter-
minism. Am Psychol 1978;33:344-58.
26. McGuire WF. Theoretical foundations of cam- paigns. In: Rice RE, Paisley WJ, eds. Public com- munication campaigns. Beverly Hills, CA: Sage Publications, 1981:41-70.
27. Rothman J. Three models of community organi- zation practice, their mixing and phasing. In: Cox FM, Erlich JL, Rothman J, et al., eds. Strategies of community organization. 3rd ed. Chicago, IL: FE Peacock Publishers, 1979:25-45.
28. Rogers EM. Diffusion of innovations. 3rd ed. New York, NY: The Free Press, 1983.
29. Sallis JF, Taylor CB, Flora JA, et al. Comparisons of mediated smoking cessation programs for com- munity health education. Presented at American Psychological Association meeting, August 1983. 30. Atkin C. Research evidence on mass mediated
health communication campaigns. In: Nimmo D, ed. Communication Yearbook III. New Bruns- wick, NJ: Transaction Books, 1979.
31. Kotler P, Zaltman G. Social marketing: an ap- proach to planned social change. J Marketing 1971;35:3-12.
32. Sallis JF, Hill RD, Killen JD, et al. An experi- mental evaluation of self-help smoking cessation: The Stanford Quit Kit. (Unpublished manu- script.)
33. Sallis JF, Haskell WL, Wood PD, et al. Physical activity assessment methodology in the Five-City Project. Am J Epidemiol 1985;121:91-106. 34. US Department of Health, Education and Wel-
fare. Lipid Research Clinics manual of laboratory operations. Vol. 1. Lipid and lipoprotein analysis. Washington DC: GPO 1974 (DHEW publication no. (NIH) 75628).
35. Butts WC, Kuehneman M, Widdowson GM. Au- tomated method for determining serum thiocya- nate to distinguish smokers from non-smokers. Clin Chem 1974;20:1344-8.
36. Fortmann SP, Marcuson R, Bitter PH, et al. A comparison of the Sphygmetrics SR-2 automatic blood pressure recorder to the mercury sphygmo- manometer in population studies. Am J Epidemiol 1981;144:836-44.
37. Gillum RF. Community surveillance for cardio- vascular disease. Methods, problems, applica- tions—a review. J Chronic Dis 1978;31:87-94. 38. Campbell DT, Stanley JC. Experimental and
quasi-experimental designs for research. Chicago, IL: Rand McNally, 1963.
39. Cook TD, Campbell DT. The design and conduct of quasi-experiments and true experiments in field settings. In: Dunnette MD, ed. Handbook of in- dustrial and organizational psychology. Chicago, IL: Rand McNally, 1976.
40. Farquhar, JW. The community-based model of life style intervention trials. Am J Epidemiol 1978;108:103-ll.
41. Cornfield J. Randomization by group: a formal analysis. Am J Epidemiol 1978;108:100-2.